
Abstract
Background and objective:
In low- and middle-income countries, pharmaceutical compounding is vital to provide high-quality healthcare service. Accordingly, this study aimed to investigate the extent status of practice and barriers to compounding services in hospital and community pharmacies of Southwest Ethiopia.
Methods:
A healthcare institution-based cross-sectional study was conducted from 15 September 2021 to 25 January 2022. Data were collected from 104 pharmacists using a self-administered questionnaire. The responding pharmacists were selected by purposive sampling technique. Finally, descriptive statistical methods were used for data analysis with the help of IBM SPSS Statistics V21.0.
Results:
A total of 104 pharmacists (27 hospital pharmacists and 77 community pharmacists) responded (response rate: 0.945). Besides providing other routine essential pharmacy services, around 93.3% of contacted pharmacies have a history of practicing compounding services. The most common practices were granule or powder reconstitution to suspensions or solutions (98.97%) and crushing tablets into smaller forms (92.8%). Commonly, compounding was requested and practiced for preparing pediatrics (97.9%) and geriatrics (96.9%) doses from adult doses, unavailable dosage forms (88.7%), and solving therapeutic gaps (86.6%). All compounding pharmacies participated in compounding antimicrobial medications. They often cited lacking skills or training (76.3%) and insufficient equipment and supplies needed for compounding (99%) as the main barriers.
Conclusion and recommendation:
With many facilitators, challenges, and limitations, medication compounding services remain one of the core healthcare services. Areas needing improvement include strengthening comprehensive and continuous professional development for pharmacists on compounding standards.
Background
The healthcare industry is one of the main contributors to the advancement of social, economic, and environmental conditions around the globe. Through a structured system, it provides services that improve, maintain, and restore the health status of individuals in a favorable environment. However, in low- and middle-income countries (LMICs), regular access to adequate health system building blocks to provide effective services is the main challenge. Especially, ensuring access to essential medicines with controlled quality has been a common obstacle.1–4
Pharmaceutical compounding is a vital component of pharmacy practice. Despite its low prevalence, it can ensure access to some essential medicines and be a good alternative for access to commercially unavailable products. It involves combining, mixing, or altering pharmaceutical ingredients to create a customized medication for practicing individualized therapy. The procedures are as simple as crushing tablets and as complex as compounding sterile products in an aseptic environment. Accordingly, it can be performed in pharmacies, hospital wards, outpatient clinics, and outsourcing to US Food & Drug Administration (FDA)-regulated facilities.5–11
Prescribing compounded medications and developing compounding plans should be based on the practitioner-patient-pharmacist (triad) relationship. Moreover, compounding should be performed or supervised by licensed pharmacy professionals. The compounder collects active ingredients which can exist as pure chemicals or derives from commercially available medication and selects appropriate compounding formulae and facilities. Then, following validated standard operating procedures, the product is prepared, documented, and dispensed to the patient.11–15
Different studies conducted in the LMICs revealed that compounding practice and adherence to good compounding practice remain the main challenges. Especially, scarcities of raw materials, trained staff, facilities, and attitudes of prescribers, compounders, and users have been common barriers to the practice in health facilities. Moreover, before marketing compounded medications, FDA does not ensure their safety, effectiveness, and quality as FDA-approved drugs.7,16–19
However, in LMICs such as Ethiopia, data regarding pharmaceutical compounding are limited. Therefore, investigating the status of pharmaceutical compounding and potentially related factors to the practice is essential for resource planning and strengthening compounding services. Accordingly, this study aimed to reveal the current practice of pharmaceutical compounding and barriers in hospital and community pharmacies of Southwest Ethiopia.
Methods
Study setting, design, and participants
A healthcare institution-based descriptive cross-sectional survey was conducted in Southwest Ethiopia from 15 September 2021 to 25 January 2022. The study population was pharmacy professionals working in hospital and community pharmacies. They provide pharmaceutical services such as ensuring access to medications and drug information for communities in Jimma Town and Mettu City.
Jimma Town and Mettu City have located 346 km and 600 km in the southwest direction of Addis Ababa (the capital city of Ethiopia), respectively. In the study area, there are hospital pharmacies of public hospitals (Jimma University Medical Center, Shenen Gibe Hospital) and private hospitals (Fromsis Primary Hospital, Oda Hulle Primary Hospital, and Awetu Primary Hospital) in Jimma Town during the study period.
Conceptual framework

Sample size determination and sampling technique
Considering client number per day, years of working experience, available resources, and extent of pharmaceutical services per day, the study pharmacies were selected. Accordingly, 110 pharmacies were selected and contacted. A total of 104 agreed to complete the questionnaires (the response rate is 0.945). Only one experienced and voluntary pharmacy professional working in each study pharmacy participated.
Considering the influence of the number and resources of pharmacies in the study area, response rate, and heterogeneity of study variables, a purposive sampling technique was used. Generally, 27 respondents from hospital pharmacies and 55 from community pharmacies were from Jimma Town. A total of 22 community pharmacies were from Mettu City.
Inclusion criteria
Considering the work characteristics, pharmacist’s workload, study site, almost only face-to-face means of interaction, and professional responsibilities, study pharmacies providing pharmaceutical services for at least 50 clients per day were considered in the study.
A voluntary pharmacy professional with at least 2 years of working experience in the study pharmacy was considered in the study.
Exclusion criteria
Involuntary study pharmacies were excluded.
Pharmacies providing a few numbers of pharmaceutical services and serving less than 50 clients per day were excluded.
Data collection tool and process
A pretested and semi-structured questionnaire was used for data collection. The questionnaire was developed using an intensive review of related literature14,16–20 Moreover, comments from the experts during the pilot study were considered to finalize the questionnaire and enhance its validity. It had two sections. The first section asked about the selected pharmacies and prescribing, compounding, and dispensing practices of compounded medications. The second section asked about the main reasons for providing pharmaceutical compounding services, challenges, and documentation.
Data collectors were five healthcare practitioners. A principal investigator gave them a short training on the study aim, questionnaire, and data collection procedure. During data collection, data collectors introduced the study objective to the participants, obtained verbal consent, and distributed questionnaires to the volunteers. Finally, the confidentiality of the collected filled questionnaire was maintained.
Pilot study
A pilot study was conducted using randomly selected 10 study respondents from 3 community pharmacies and 2 hospital pharmacies. Finally, recommendations from the respondents during a pilot study were considered in the final questionnaire. However, data collected during the pilot study were not included in the analysis and presentation of the final results.
Data quality, analysis, and presentation
Following the pilot study, the questionnaire was revised for clarity, completeness, and consistency. In addition, after data collection, each filled questionnaire was checked for completeness and kept secure.
Descriptive statistics were used to describe the features of collected data using IBM SPSS Statistics V21.0. Finally, the analyzed data were presented using frequency distribution.
Operational definition
Pharmaceutical compounding service is preparing unlicensed or personalized medication by mixing, reconstituting, crushing, or repackaging following recommended compounding formula and procedure in pharmacy, ward, or other settings.8,14,21–23
Medication reconstitution is a process of preparing a specific concentration of liquid medication formulation by mixing it with liquid diluent.
Results
Of 110 pharmacists contacted, 104 agreed and completed the questionnaire. A total of 97 (93.3%) pharmacies had the experience of providing compounding services for the community (Table 1).
Basic description of medication compounding services in hospital and community pharmacies (N = 104).

Only one answer was recommended for the question asking for the requested medication name, dispensing practice, compounding formula, and source of compounding formula. It was planned to know the most.
According to the current study, 97 pharmacies participated in antimicrobial medication compounding. They were commonly requested for dermatological, gastrointestinal tract, and metabolic disorders (Table 2).
Compounding practices and compounded medications in hospital and community pharmacies (N = 97).

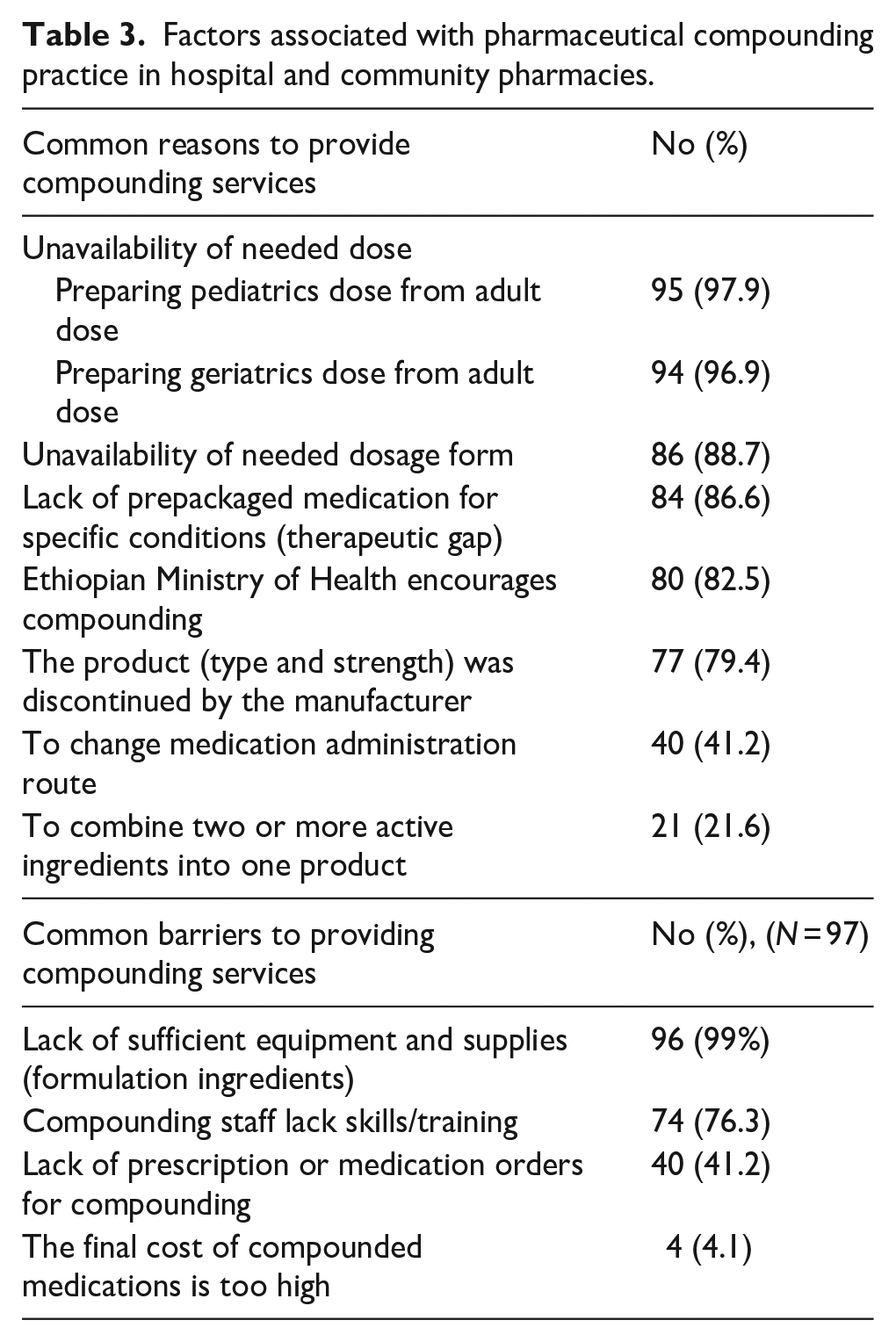
This study indicated the presence of many reasons for requesting compounding services and challenges (Table 3).
Factors associated with pharmaceutical compounding practice in hospital and community pharmacies.
Discussion
Globally, ensuring access to essential medicines with controlled quality is one of the building blocks of the health system. As a fundamental component of realizing the right to health, manufacturing medication in the pharmaceutical industry and locally compounding in a health facility play a vital role. In LMICs, pharmaceutical industries are limited in number and advancement. Therefore, compounding services, as an integral part of pharmacy practice, contribute to ensuring access to quality essential medicines.5,6,9,10,24 Similarly, this study showed the availability and necessity of compounding services in almost all pharmacies at different levels in the study area (Table 1). It can be associated with poor access to essential medicines of required dosage regimens and less prevalence of pharmaceutical industries in the study area (low-income country).
The approach that “one-size-fits-all” does not work for medications is a challenge to access essential medicines, especially for vulnerable populations and patients with rare diseases. Compounding practice becomes a critical solution.9,10,24 In the same way, the current study showed the unavailability of needed dosage regimens for pediatrics and geriatrics and prepackaged medication for specific conditions as the most common reasons for compounding practice (Table 3). The service might be related to the economic inefficiency of manufacturing and marketing all needed medication dosage regimens for individualized therapy, particularly in LMICs. They make compounding the primarily safe and recommended solution.
Furthermore, compounding service facilitates easy administration and prevents unnecessary medication overdosing.25,26 According to the current study, compounding was used to combine two or more active ingredients into a single product and change the route of administration. It might be linked to the advantages of safe medication administration, which contributes to patient compliance and medication effectiveness.
The current study showed the common practice of antimicrobial medication compounding using techniques such as crushing tablets into smaller forms and granule or powder reconstitution (Table 2). These findings have similarities with data reported by a study conducted in Jordanian pharmacies (2019). 18 Their dominance was related to the short stability period of some medications in liquid form and frequent requests for altering medication dosage regimens for individualized therapy. Moreover, these compounding techniques did not need a large premise and complex procedures for compounding.
Poor compounding practices and unverified safety, effectiveness, or quality of compounded medication before marketing by the FDA can cause user exposure to potentially serious health risks.19,27 Therefore, compounding pharmacists should have deep knowledge and skill, significant training time, quality raw materials, and facilities for compounding. Even though technology has been advancing over the last few decades and compounding is re-emerging, these requirements are still barriers.7,14,26,28 This study also indicated scarcity of sufficient compounding equipment and supplies and lack of training and skill as the main challenges to fully providing compounding services (Table 3). These challenges should be associated with scarcity of readiness, such as limited pharmacist role in clinical patient care in LMICs, and challenges of getting resources in the local pharmacies.
The compounding process should be well documented and kept safe. The content should include drug dosage regimen, master formulation record, log of compounded items, compounder name, date, prescription number, labeling, quality control procedures, and results. They are used to evaluate and replicate the compounding process.7,29 This study also indicated the practice of documentation which is similar to the finding by AlKhatib et al. 18 Most of the study institutes keep handwritten records. The easy accessibility and favorability of most professionals make handwritten documentation commonly used.
Limitations of the study
Even though efforts were made to reduce potential bias by selecting the study pharmacies in the selected study areas, it did not achieve national coverage. Moreover, the study did not evaluate the attitude of healthcare practitioners and users toward the safety, quality, and efficacy of compounded medications.
Conclusion
Most of the community and hospital pharmacies had experience in providing compounding services. Commonly, crushing tablets and reconstitution to prepare suspensions or solutions were the most compounding practices to provide customized medications. They used to prepare commercially unavailable pediatric and geriatric doses from adult doses and dosage forms. Also, they can solve therapeutic gaps. However, the practice is inadequate due to a lack or scarcity of trained compounding staff, equipment, supplies, and other facilities. They were perceived as the main barriers by the compounding pharmacists.
Recommendation
Re-emphasizing the advancement and regulation of compounding services needs consideration to enhance the quality of health services while reducing potential health risks. Therefore, strengthening comprehensive and continuous professional development for pharmacists on compounding standards, funding to fulfill compounding equipment and supplies, and proper vigilance for members of vulnerable populations taking care will contribute to the effectiveness of the services.