
Abstract
Background
Adults with ADHD and/or autism often face substantial challenges in working life. Although society offers support, interventions often fail to meet individual needs.
Aim
To explore, in adults aged 25–40 with ADHD and/or autism, what characterizes support perceived as essential, including how, when, and by whom it should be delivered.
Method
A qualitative survey explored desired forms of support in working life in Sweden. In total, 531 participants responded (24.5% response rate). Qualitative analysis of open-ended responses was performed to identify key patterns regarding support needs and expectations.
Results
Respondents consistently emphasized the need for person-centered, flexible, and sustainable support, noting that timing, delivery approach, and relational attitudes were as critical as the content of any intervention. They described comprehensive, coherent assistance tailored to individual circumstances as essential. However, participants reported that, in reality, the support they had received was fragmented and fell short of these expectations, revealing a discrepancy between desired and actual provision.
Conclusions
Effective support must be person-centered. Not only in what is provided but also in how, when, and for how long it is delivered. Embedding flexibility and responsiveness into workplace practices is essential for promoting long-term employability and well-being.
Lay Abstract
Many autistic and ADHD adults face challenges at work. Support exists, but it often does not match individual needs. Previous research shows that workplace adjustments can help, but they are not always provided in ways that work for the person. This study asked over 500 adults in Sweden with autism and/or ADHD what support they find most helpful and how they experience the help they receive. People shared their views in both structured questions and open comments, giving a rich picture of real-life experiences and what truly matters to them. The findings show a clear gap between what people need and what they get. Participants stressed that support should be flexible and person-centered. It is not only about what is offered but also how, when, and for how long. Attitudes and relationships at work matter as much as practical changes. Many described support as fragmented and short-term, which made it harder to stay in work or return after unemployment. They also highlighted that unclear communication and a lack of understanding from managers often created stress. To make workplaces more inclusive, support must be tailored and adaptable over time. Employers, service providers, and policymakers need to work together to create sustainable solutions. Open communication, willingness to adjust, and long-term planning are key. These steps can help more neurodivergent adults find and keep jobs while maintaining well-being and contributing strength to society. When support works well, it benefits not only the individual but also teams, organizations, and the wider community.
Keywords
Introduction
Many adults with ADHD and/or autism face significant challenges related to work, such as obtaining employment, maintaining it, and preserving their health throughout the process (Davies et al., 2023; FitzGerald et al., 2021; Högstedt et al., 2022). To promote labor market participation, the Swedish system offers various support structures in collaboration with healthcare services, the Swedish Social Insurance Agency, municipalities, and the Swedish Public Employment Service. Under the Act concerning Support and Service for Persons with Certain Functional Impairments (LSS), autistic individuals are entitled to municipal support in the form of community-based day programs. These programs provide structured and purposeful activities for those unable to work, aiming to promote personal development, social participation, and opportunities for future employment. The act LSS applies specifically to individuals with certain functional impairments, including autism, but not individuals with ADHD, which means that these municipal supports influence the types of services and work-related opportunities available to autistic individuals. Under the Swedish Work Environment Act, employers are required to prevent ill-health and ensure safe working conditions, which shape how workplace adjustments are organized for employees, including those with ADHD and/or autism. The Swedish Disability Discrimination Act prohibits discrimination on the basis of disability and requires reasonable accommodations, influencing both the types of support employees may request and the adjustments employers provide. The Swedish Public Employment Service's offers tailored support for individuals with ADHD and autism, including personal job coaching, wage subsidies, and workplace adaptations. These services aim to help individuals find, maintain, and thrive in employment through individualized and inclusive solutions. However, these systems of interventions are not consistently available and do not always match the subjective needs of adults with ADHD and/or autism with and without employment (Högstedt et al., 2026; Hedlund & Jordal, 2024).
The diverse profiles of adults with ADHD and/or autism make a “one-size-fits-all” approach to work placement ineffective (Bölte et al., 2025). One factor that appears more broadly important, however, is the response of the surrounding environment. Negative attitudes and a lack of understanding of ADHD and/or autism can have lasting effects on individuals’ well-being and participation in working life (O’Reilly et al., 2025; Smethurst et al., 2024), whereas being met with acceptance and understanding for functioning differently has proven crucial among Swedish adults 25–40 with ADHD and/or autism (Högstedt et al., 2022). These findings emphasize that the effectiveness of any given intervention depends not only on its content but also on the attitudes and approach of those delivering it. However, understanding which specific conditions promote stable employment requires looking beyond attitudes to how support is organized and sustained over time.
Research also shows the importance of shifting the focus from short-term interventions to long-term vocational development, where the individual's quality of life and strengths are central (Dreaver et al., 2020; Nicholas & Klag, 2020). Continuous support from a trusted professional with knowledge of the individual's everyday functioning has been identified as particularly valuable (Lyhne et al., 2021), as have high-quality supervisory relationships in which supervisors communicate clearly and actively adapt expectations to the individual's needs (Martin et al., 2023). Supportive networks outside the workplace also contribute to sustainable employment (Lorenc et al., 2018; Nicholas & Klag, 2020). However, a systematic review of 32 studies, most focused on younger, autistic males without intellectual disability, found that support provided was often too generic, short-term, or inaccessible, and rarely based on the individual's strengths and life situation (Lorenc et al., 2018).
Although research frequently describes the support that individuals with ADHD and autism receive at work, far fewer studies examine the types of support they themselves prefer. Existing evidence points to a consistent pattern: individuals emphasize practical, individualized, and context-sensitive assistance. Chen & Yakubova (2024) found that young autistic adults in the United States who were currently or formerly employed desired hands-on training, appropriate job-fit, employer accommodations, and an inclusive workplace that fosters self-advocacy. Hedley et al. (2018) drew on perspectives from autistic trainees in an Australian supported employment program, along with their co-workers, support staff, and family members, and identified organizational support structures, collegial assistance, and access to a dedicated support consultant as key enablers. Lyhne et al. (2021) found that young adults with ADHD in Norway emphasized clear tasks, daily routines, self-confidence, and continuous support from a trusted professional as essential for engaging in work. Together, these studies suggest that preferred support extends beyond formal accommodations to include relational, organizational, and environmental factors. However, each study involved a small number of participants, focused on a single diagnostic group, and examined preferences within a specific support context, limiting the extent to which they capture what individuals with ADHD and/or autism want from support when viewed more broadly.
These limitations make it difficult to capture the broader perspectives and preferences of adults with ADHD and/or autism in terms of the conditions under which support is perceived as effective. In the present study, we conceptualize support broadly, encompassing not only what is provided but also who provides it, how it is delivered, when it is available, and for how long. To address this identified gap, the aim of this study was to explore, in a transdiagnostic sample of adults with clinically verified ADHD and/or autism, what characterizes support that is perceived as essential, including how, when, and by whom it should be delivered.
Methods
Language Statement
In this article, we use identity-first language (e.g., “autistic adults”) when referring specifically to participants with autism, in line with research indicating that many autistic individuals prefer identity-first terminology. However, we mostly refer jointly to autistic adults and adults with ADHD; in these cases, we use person-first language (e.g., “individuals with autism and/or ADHD”), as there is no widely established identity-first equivalent for ADHD, and person-first terminology therefore provides clarity and consistency when describing the combined group.
Participants and Recruitment
Our target group consisted of individuals aged 25–40 who, in 2019, had a diagnosis of ASD, ADHD, or a combination of both (ASD + ADHD) according to ICD-10 criteria (World Health Organization (WHO), 1993), and were registered in outpatient psychiatry clinics. Participants were recruited from seven psychiatric outpatient clinics located in southeastern Sweden. Participants were recruited through outpatient psychiatry clinics because these services conduct formal diagnostic assessments and maintain verified diagnostic information, ensuring that all participants had a confirmed diagnosis of ADHD and/or autism. While the minimum age could have been set at 18, we opted for 25 to ensure that respondents had had several years of exposure to the labor market and had had sufficient time to pursue post-secondary studies, engage in employment, participate in internships, or attempt to enter the labor market in other ways. The upper age limit of 40 was chosen to minimize the impact of evolving diagnostic practices and changes in society over time. Psychosis, active eating disorders, substance use disorders, or presence of intellectual disabilities were considered confounders and were controlled for by exclusion. No restrictions were placed on employment status to allow for a diverse and inclusive sample.
Regional Healthcare statisticians identified eligible individuals using medical records. Clinic managers at each clinic received lists of potential participants (n = 2341) and, with support from administrative staff, distributed the survey by mail to their home addresses. Six clinics sent out reminders approximately three weeks later; one clinic was unable to do so due to COVID-19-related disruptions. The information letter explained that participation was voluntary, that participants could withdraw at any time, and included brief information about how the data would be handled. The invitation included a link to the online survey, hosted on Survey & Report (Artisan Global Media, Växjö, Sweden). Data collection occurred between May and September 2020. Of the 2341 surveys sent, five were returned by family members, indicating the patient could not participate, and 33 were undeliverable. This left 2304 surveys presumed to have reached the intended recipients. We received 541 completed surveys (response rate: 23.5%). Ten responses were excluded because the individuals reported not having ASD or ADHD. The final sample consisted of 531 participants (see Table 1).
Demographic Characteristics of Participants (N = 531).

Note. “Graduated secondary school” corresponds to the 9 years of mandatory education in Sweden.
Survey Design
The questionnaire was developed with accessibility in mind, aiming to accommodate a wide range of individuals with ASD and/or ADHD. To support those with attention-related challenges, the survey was kept concise and primarily featured multiple-choice questions. Recognizing that some participants might interpret questions very literally, we included optional free-text fields alongside most items, allowing respondents to clarify or expand their answers. No questions were mandatory. A pilot test with 20 individuals led to minor revisions in the wording of questions related to current employment, but no major comprehension issues were identified.
The survey contained 21 items in three main sections: Background information, Satisfaction with home and leisure situation, and Received and desired support. This study specifically focused on qualitative analysis of open-ended questions in section 3, with a primary focus on how participants describe desired support. Section 2 questions were not included in the current study. Section 1 background information collected included age, gender, education level, ADHD and/or autism diagnoses, marital status, number of children, employment status, and employment rate.
Section 3 had a branching design where participants got open-ended follow-up questions depending on their answer to the following question about received support: “Did you receive any support to be able to obtain or maintain a job? (help / adaptations / treatment / conditions / possibilities / support or similar that you are receiving or have previously received with the aim to obtain or maintain a job)?”, with the options “Yes, support to obtain work,” “Yes, support to maintain work,” “Yes, support with other things I needed in order to be able to work.” “No, it has not been needed,” “No, I have declined,” “No, I have not been offered support but would have needed it,” and “Other (please describe).” Participants could select more than one answer. Participants choosing one of the “yes” options received the follow-up questions (1) “From whom did you receive support?,” (2) “What kind of support have you received?,” and (3) “Would you have wanted additional support? If so, what kind of support?.” Participants selecting “No, it has not been needed.” received the question “Why do you think you have not needed any support to obtain or maintain employment?.” Participants selecting “No, I have declined” received the question “Why did you decline the support that was offered to help you obtain or maintain employment?.” Finally, participants selecting “No, I have not been offered support but would have needed it” received the question “What support would you have wished for in order to maintain or obtain employment?.” Participant flow through this branching node is shown in Figure 1.

Participant flow through the branching design of the received and desired support section. Respondents were asked whether they had received support to obtain or maintain a job and could select more than one response option. Responses were classified into four mutually exclusive groups based on whether any Yes option, any No option, or both were selected. Selection counts within groups exceed group totals due to the multiselect format. Depending on which option(s) were selected, participants received different open-ended follow-up questions. Those selecting a Yes option were first asked from whom they received support and what kind; responses to these questions were used for contextualization but were not part of the primary analysis. Participants who selected both Yes and No options were routed to the follow-up question(s) corresponding to each selected option. Response counts at the follow-up level reflect the number of participants who provided a response, not the number who received the question.
Together, these questions were designed to capture participants’ perspectives on support from multiple angles to address the study's aim of understanding what characterizes support perceived as essential, including how, when, and by whom it should be delivered. The open-ended format for the questions was selected to invite participants to describe, in their own words, the types of support they would have needed to obtain or keep employment. This design allowed respondents to define “support” broadly and let them bring up issues that were meaningful to them, rather than being constrained by researcher-generated categories.
Our main analysis regarded responses to open-ended questions about desired support, whereas responses to questions about already received support were analyzed qualitatively for contextualization of the main results.
Response Coding and Data Preparation
Recoding of background data. We conducted a semiqualitative recoding process of multiple-choice responses in the Background section, as respondents liberally used the permission to select “Other” and write their own text. This involved reviewing the open-ended answers and adjusting the multiple-choice selections when necessary. Educational and employment variables were consolidated into broader categories for presentation in Table 1.
Work Status Classification. Participants’ work status was classified to provide a clear description of the sample's occupational situation, which is relevant for interpreting the study findings. This classification was based on participants’ self-reported current employment situation, supplemented by other questionnaire items when relevant. Individuals were classified as “working” if they reported engaging in paid work, studies, self-employment, or were on parental/sabbatical leave from employment, at a level of 25% or more. This threshold reflects the Swedish context, where part-time work can be a sustainable option for adults with ADHD and/or autism receiving partial disability benefits to mitigate burnout risks (Swedish National Association Attention, 2021). Those reporting less than 25% activity were initially grouped into either “No work” (e.g., on disability leave or actively seeking employment) or “Other work” (e.g., participating in work training programs, internships, or structured daily activities according to the Swedish Disability Support Act LSS). The 25% cutoff was chosen based on the assumption that such minimal engagement likely indicates limited work capacity and financial instability. This assumption was made based on the authors’ professional experience as clinicians working in Sweden.
Categorization of received support. To provide context for the results of the main analysis about desired support, we qualitatively analyzed free-text responses to the two questions about received support (by whom it was provided and what kind of support it was). We used content analysis by Patton (see Qualitative Analysis section for methodological details) to identify the authorities or organizations involved. The responses to the question “What kind of support have you received?” were analyzed using the same procedure. We first examined the data to identify responses that needed clarification before coding, for example, in cases where the provider was unclear. We verified the information by searching for local authority names online. For both questions, deductive coding schemes were constructed, based on expected support sources (e.g., healthcare professionals, employers) and types of support (e.g., support outside of work, support at work). We used an “other or unclear” category for less common actors/support types. The schemes were refined by reassigning responses from the “other or unclear” groups to existing or newly created categories. For example, occupational health services were recorded under “Employer” and support from a neighbor was recorded under “support outside work.” A separate “Other” category was retained for actors mentioned by only one participant, for example, support from the church. We identified six final categories of actors and four categories of types of support (Table 2).
Actors Providing Work-Related Support and Types of Support .
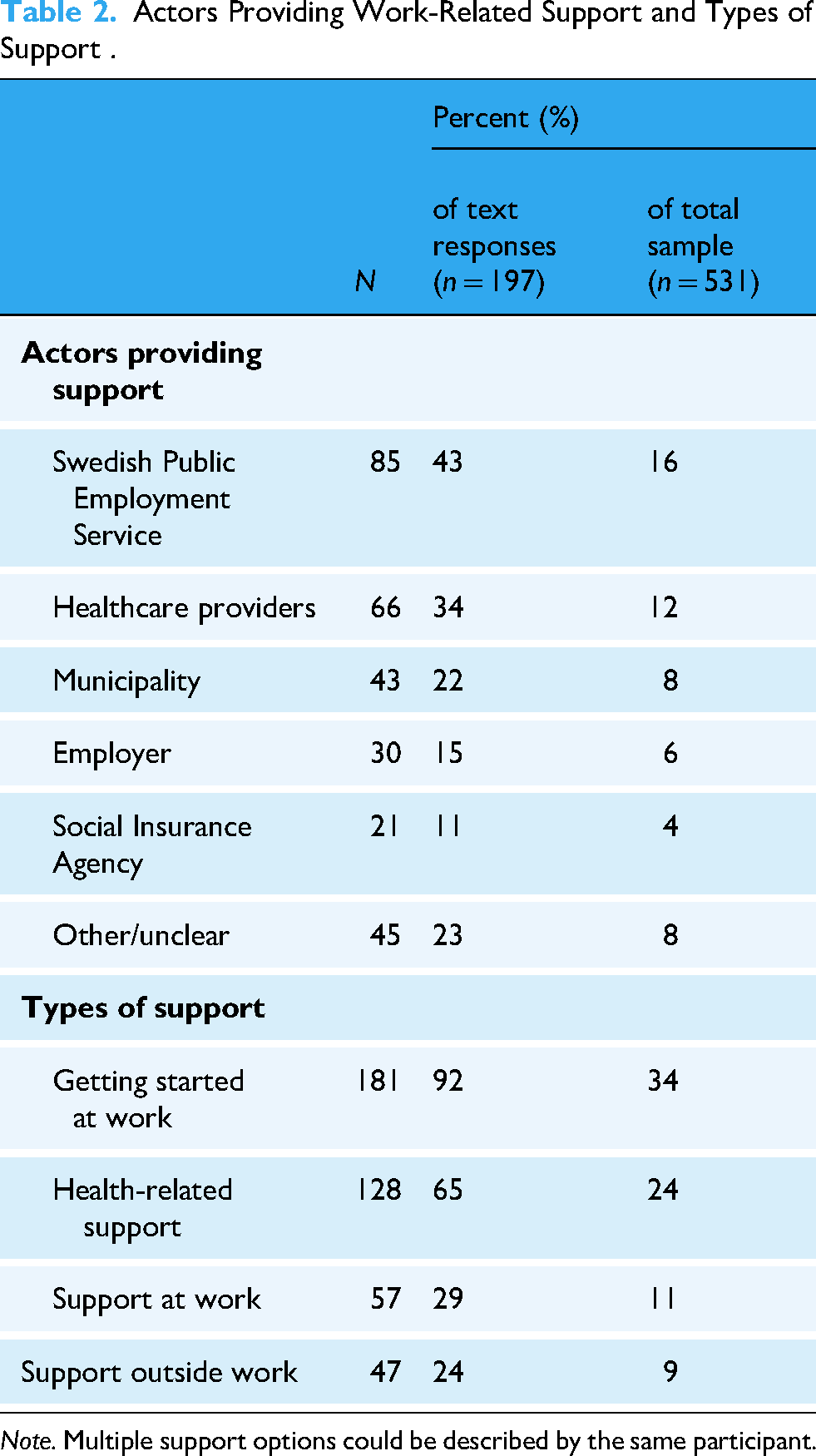
Note. Multiple support options could be described by the same participant.
Qualitative Analysis
We conducted a qualitative content analysis (Patton, 2015). The analytic process was conducted systematically with documentation of coding decisions to strengthen rigor. Two independent coders (EH and TE), one being an autistic individual with lived experience of employment, carefully read through all responses to the questions to identify patterns and categories in the material. Reflexive notes were kept to acknowledge and critically examine pre-understanding.
Analysis of desired support. This analysis comprised responses to the questions “Would you have wanted additional support?” (given to respondents saying they had received some support) and “What support would you have wished for?” (given to those saying they had not received support, even though they needed it). We used content analysis as described above and also identified themes. EH assigned labels and definitions to the categories, patterns, and themes, after which TE reviewed them. Then, we each categorized the material individually and then compared our results. To enhance trustworthiness according to Patton's (2015) quality and credibility standards, we used analyst triangulation through regular discussions within the research team. We then analyzed the results by counting the frequency of codes, identifying patterns, and themes and exploring relationships between codes. Our conclusions resulted in three overarching themes described in the Results section. We aimed to provide each theme with rich descriptions and illustrative quotations to support interpretive credibility.
Analysis of reasons for not needing support. To further understand the different mechanisms of support in working life, we performed content analysis on free-text responses from the participants who indicated that they did not need support (“Why do you think you have not needed any support?”). This led us to identify a meaningful subset of “No”-participants who clearly stated that they actually did need support; these results were reported as an unexpected finding.
Author Positionality Statement
The first author does not identify as autistic or ADHD and does not belong to any minority group based on race, gender, or diagnostic status. The first author's perspective is shaped by extensive professional experience as an occupational therapist working person-centered with autistic and/or ADHD adults across assessment, everyday life, and work-related contexts. This background provides a well-developed pre-understanding of support needs and participation barriers, which serves as a resource when interpreting the data. The first author has actively reflected on how this pre-understanding may influence the analytic process and has worked to critically examine underlying assumptions. The author team also includes co-authors with lived experience of neurodivergence, ensuring that multiple perspectives informed the study.
Results
Participants
Basic demographic data of the final sample (N = 531) are shown in Table 1. The participants were aged 25–40 years, and there were more women than men, with 59% (n = 315) women and 38% (n = 200) men. A majority of 56% (n = 299) had an ADHD diagnosis only, 27% (n = 142) had an autism diagnosis only, and 17% (n = 90) had both ADHD and autism.
Received Support
Text responses about who had provided support and types of support were categorized and presented in Table 2.
Of the 255 participants who reported having received support, 197 provided free-text responses. Another 258 participants selected one of the negative options (N = 117 had no need for support; N = 137 had not been offered support; and N = 8 declined offered support). Thirteen individuals indicated both having and not having received support, which reflected a discrepancy between the support available and the support they actually needed, in either timing or type.
Among the 197 participants who had received work-related support (and provided free-text response), 53% had received support with obtaining work, 25% in maintaining work, and 52% other types of work-related support. The most common support actors were the public employment service and healthcare providers, followed by municipalities.
Based on the coding of free-text responses, we categorized support into four groups: (1) getting started at work, (2) health-related support, (3) support at work, and (4) support outside work. Percentages refer to the proportion of the 197 individuals who had received support. Group 1: Most participants (92%) who were receiving or had received support reported that it focused on obtaining employment and “getting started” at work. Examples included help with CV writing, finding and applying for jobs, matching suitable positions, wage subsidies, coaching, and interview preparation. Group 2: 65% reported health-related support, such as medication, psychological interventions and occupational therapy, diagnostic assessments, and educational courses related to the diagnosis. Other mentioned cognitive aids and help with co-occurring conditions such as anxiety, depression, sleep disturbances, chronic pain, substance use, and autism/ADHD-specific interventions. Group 3: 29% reported support focused on the work situation itself, including adjusted working hours, tasks prioritization, clear expectations and routines, understanding from managers, access to a private office, noise-reducing headphones, a workplace mentor, the ability to work at one's own pace, access to rest areas or the option to take short breaks, reassignment of tasks, and a work environment without demands for social interaction). Group 4: 24% receiving support related to life outside work, such as social support from family, friends or colleagues, housing support, a legal guardianship, or a personal contact person.
Desired Support
Some respondents describe that the support they sought equaled what they received, but this group was a small minority. The qualitative analysis of text responses (n = 334) included answers from respondents who received support and desired something more (n = 197) and respondents who did not receive support but needed it and specified desired support (n = 137). The results revealed that participants not only described specific forms of desired support but also emphasized how they wanted to be treated and helped. Three themes were identified: To be seen, understood and treated with respect; person-centered support; and sustainability.
To be seen, understood, and treated with respect
A key topic was the need to be seen and understood by others, such as employers, colleagues, healthcare providers, and other professionals. Understanding and respectful interactions were described as essential for any form of support to be effective and were seen as prerequisites for other interventions. Would be great, I think, to be offered a job or internship at a workplace where there is tolerance and room for executive functioning difficulties. I am thinking that, despite the support I get, there's a lack of understanding, despite the conversations between my manager and me, things suddenly come up that I’m expected to know, but that no one has told me about. So I just stand there, being showered with crap for something I had no idea about, so I think clarity and understanding would have been good.
Person-centered support
Being treated as a unique individual and receiving support based on one's own needs, in an appropriate manner, was described as important. Many respondents emphasized that support needs to be effective as well as tailored to the person's individual circumstances. It was also considered essential to receive information about what types of support were available. Respondents expressed a need for help in filtering and understanding that information. They also expressed a preference for forms of support that did not require them to independently manage the process of accessing assistance. Such an approach was perceived as enhancing autonomy and reducing stress, while simultaneously making support more accessible and manageable.
Respondents expressed a need for increased knowledge of the diversity of the diagnoses. They wished for greater understanding and competence among those providing support to ensure that interventions were relevant and aligned with individual needs. They also wished for more flexible and adaptable accommodation tailored to the person and the situation. I've mostly had to try on my own to find employers and workplaces that are able and willing to provide adaptations. I would need that kind of support instead of having to carry the whole burden by myself. I've had to fight alone in my desire to work. But the Public Employment Service has worked against me for a long time in my efforts to do the kind of work I'm capable of. I would have liked to be understood and accepted for who I am to a greater extent.
Sustainability
A unifying theme in the respondents’ statements was sustainability, a desire for long-term solutions, balance, and support that lasted over time. This theme was about achieving a functioning everyday life, being able to work part time in a financially sustainable way, and receiving support that was tailored, predictable, and preventive. The most frequently requested specific intervention was continuous long-term supportive counseling. Occupational therapists, psychologists, and housing support staff were mentioned most often, generally with the wish to develop effective strategies and routines to manage everyday life. Many expressed a need for support that extended over time, not just during certain phases. They needed help to keep a job, receive support that evolved with the individual's needs, and they needed to be relieved of carrying the full responsibility alone. Predictability was described as crucial—both in working life and in contact with authorities and healthcare. Constantly meeting new staff or therapists created stress and insecurity. Participants asked for clear tasks, understandable professional roles, and continuous support contacts. Getting advice and help on how to make everyday life work without falling apart.
Financial sustainability and support to be able to work part time were recurring themes. This was described as allowing balance between work and recovery, having good routines both at and outside of work, and avoiding the energy drain that led to exhaustion Money is a constant stress that doesn't improve the well-being.
Participants Without Support
A number of respondents (N = 117) stated that they did not need any support to obtain or maintain employment. However, the analysis revealed that some of these individuals (N = 35) did, in fact, wish for or require support, but that employment was not currently relevant to them. Others described refraining from seeking support because they did not want to appear vulnerable, or because they had prioritized work at the expense of other areas of life. One respondent expressed this by saying: Because I really give it my all. I might feel completely exhausted after work, but it's worth it.
A few respondents also explained why they had declined support aimed at helping them gain or retain employment. In these cases, the support offered was perceived as poorly adapted to their needs, or they lacked the energy to wait for support.
Discussion
This study explored what characterizes support that adults with ADHD and/or autism consider essential for their working lives, with a particular focus on how support is delivered, when it is available, and by whom it is provided. Extending earlier work indicating that autistic individuals reported on the support they had received, our findings reveal a pronounced discrepancy between the support provided and the support desired. Participants consistently emphasized that the effectiveness of support depended not only on what was offered but also on the attitudes and approach of those delivering it, the degree of individualization, and whether support was sustained over time. These dimensions corresponded to three overarching themes: being seen, understood, and treated with respect; person-centered support; and sustainability.
Across all three themes, participants described current systems as fragmented and narrowly intervention-focused, such as offering help with writing a CV rather than delivering comprehensive, individualized solutions. Many of the preferred forms of assistance require neurodiversity awareness and employer understanding, barriers extensively documented in previous research (Black et al., 2020; Khalifa et al., 2020; O’Reilly et al., 2025; Oscarsson et al., 2022; Waisman-Nitzan et al., 2021; Whelpley et al., 2021). Importantly, many of these measures are simple and cost-neutral when willingness and knowledge are present, echoing findings by Chen & Yakubova (2024), who reported that autistic young people value practical, low-cost strategies such as clear written instructions. This underscores that the challenge is not primarily financial but organizational, rooted in knowledge gaps, attitudes, and a lack of systemic coordination.
Our findings also highlighted that participants prioritized how support was delivered over specific interventions. They consistently expressed a desire to be met with understanding and acceptance for who they were as individuals. This is consistent with previous research showing that interpersonal attitudes and social support significantly influence psychological well-being and employment outcomes (Dreaver et al., 2020; Hedley et al., 2018; Holwerda et al., 2013; Lai, 2023; Liebel et al., 2024). When the support person has an approach that lacks empathy and recognition, the content of the intervention becomes secondary. These results reinforce the importance of embedding relational competence and neurodiversity awareness into all workplace practices.
Timing and sustainability also emerged as additional critical factors. Support must be available when needed, in relation to other interventions and life circumstances, and it must be sustained over time. Even well-designed interventions fail if offered too late or terminated prematurely. This aligns with previous studies showing that long-term support and enduring networks increase participation in working life (Holwerda et al., 2013). Our findings indicate that short-term, fragmented interventions, often focused on job acquisition rather than long-term employment, are insufficient, echoing concerns raised by Sharpe et al. (2022). A systemic shift is needed toward holistic approaches that synchronize efforts across stakeholders and prioritize sustainable employment rather than short-term placement.
The tendency of individuals to refrain from seeking support demonstrates, in line with many previous studies, the importance of avoiding stigma. This reluctance may stem either from managing on their own at a very high personal cost or from not wanting to be perceived as vulnerable. Whether and how individuals receive support is shaped by the critical issue of disclosure, which can determine if support becomes accessible at all. Previous research indicates that fear of stigma and negative consequences often deters individuals from disclosing a diagnosis (O’Reilly et al., 2025), limiting access to accommodations. Conversely, disclosure can facilitate adjustments and foster inclusion (Khalifa et al., 2020; Lindsay et al., 2021), but it also carries risks of discrimination (Lindsay et al., 2021). This underscores the importance of creating supportive environments where employees feel safe to disclose if they choose, while ensuring that accommodations are available regardless of disclosure status. Inclusive workplaces, where understanding is built through individualized, participatory approaches rather than generic training, are key to reducing stigma and promoting well-being (Romualdez et al., 2021; Tomas et al., 2023). Generic autism training risks reinforcing stereotypes and may do more harm than good; instead, employers should adopt individualized training strategies that involve the employee and reflect their unique experiences, needs, and strengths.
Another key contribution of this study concerns the tension between individualized support and the standardized frameworks that organizations often rely on. Although standardization facilitates implementation and legal compliance, excessive rigidity may impede person-centered support. Our findings suggest that this tension can be addressed by adopting flexible models that combine structured procedures with substantial room for individual tailoring, a challenge also highlighted in previous research on welfare delivery, where human service organizations struggle to balance standardization and individualization (Nordesjö et al., 2022). Future research should explore how structural safeguards, such as clear procedures and independent review mechanisms, can complement individualized support and reduce reliance on managerial attitudes. Such systems may be crucial for protecting employees from discrimination while preserving the flexibility needed for person-centered accommodations.
Another barrier identified in this study is the lack of information about available support. Without clear communication about available support, individuals cannot make informed decisions or advocate for their needs. This underlines that structural elements, such as information accessibility, are as critical as interpersonal factors. To be effective, support must be person-centered, tailored to the individual's current needs, and delivered through dialogue rather than imposed as a generic solution. This aligns with person-centeredness (Santana et al., 2018), which emphasizes individualized, goal-oriented interventions grounded in the person's perspective. Without such an approach, support risks becoming fragmented and ineffective, which is the opposite of what participants consistently called for. Importantly, the relevance and accessibility of support shape not only how helpful it is but also whether people choose to use it at all. This means that an apparent lack of support uptake should not be interpreted as an absence of support needs. The free-text descriptions of unmet needs provided by participants who had declined support indicate that existing support options may fail to align with what individuals perceive as meaningful or helpful, highlighting the importance of designing and communicating support in ways that resonate with individuals’ lived realities if support is to be utilized and experienced as valuable.
At the same time, our findings suggest that an apparent lack of support uptake should not be interpreted as an absence of support needs. The descriptions of unmet needs, given in free text by participants who had declined support, indicate that there may be a failure of the available support options to align with what individuals perceive as meaningful or helpful.
Taken together, these findings point to the need for a paradigm shift in how workplace support for individuals with ADHD and/or autism is conceptualized and implemented. Support cannot be viewed as isolated interventions but must be integrated across individual, organizational, and systemic levels. Collaboration between employers, healthcare providers, social services, and policymakers is essential to create sustainable solutions. Long-term funding and structural coordination are prerequisites for success. Ultimately, effective support is not about offering more interventions but about offering the right interventions (what) that are delivered (by whom) in the right way (how), at the right time (when), and for the right duration (for how long). These findings underscore the need for systemic, person-centered approaches that prioritize flexibility, sustainability, and collaboration across stakeholders.
Methodological Discussion
One limitation of this study is the relatively high attrition rate of 76.5%. Since participants were recruited exclusively through psychiatric clinics, there is a risk of sampling bias, which may have resulted in an overrepresentation of individuals with conditions such as anxiety or depression. At the same time, having a formal diagnosis is at least one way to communicate support needs, and individuals without a diagnosis may still have substantial needs. Expanding recruitment beyond clinical settings could have mitigated this bias and potentially improved participation rates. Nevertheless, we chose to maintain a clinically defined sample, as recommended by Bennett and Goodall (2021), given the necessity of formal diagnoses for determining eligibility for support services. We still consider the large number of respondents a key strength of the study.
The group that completed the survey closely reflects the larger population to whom the survey was distributed in terms of age and diagnosis, although women were slightly overrepresented among respondents. Beyond this, little is known about those who chose not to respond, which can be seen as a limitation—for example, we do not know to what extent respondents were employed compared to the entire sample. Unexpectedly, the survey yielded a substantial amount of qualitative data, suggesting that many participants used the opportunity to share their experiences. A challenge was conducting qualitative analysis on written responses without the possibility of asking follow-up questions.
It could also be viewed as a limitation that individuals with ADHD, autism, and co-occurring conditions were included in the same study. However, many people with ADHD and/or autism experience similar challenges, such as difficulties with executive functioning. This study does not focus on diagnostic categories but rather aims to contribute to a more holistic understanding of ADHD and/or autism in working life and to provide guidance for more flexible and individualized support design. Employers, support professionals, and authorities often encounter individuals with overarching needs rather than diagnosis-specific ones.
Implications
Support must address not only what is provided but also how it is delivered in practice, by ensuring that all interactions consistently demonstrate respect, understanding, and patience—factors identified by participants as decisive for whether support is perceived as helpful or not.
Person-centered support requires clear and ongoing assessment to ensure that support can be continuously adjusted as needs change. To ensure that support accurately reflects individuals’ needs, systems should include regular, structured, and collaborative check-ins.
Assessing individuals’ support needs based on their acceptance of or attitude toward specific interventions may not fully capture their actual needs.
Sustainable support depends on clearly defined and coordinated structures that maintain continuity across changes in employment, health, and service providers. Participants who received no support described concrete unmet needs, indicating that easily accessible information, clearly assigned responsibilities, and low-threshold entry points (e.g., single points of contact) are essential to prevent gaps and delays in support provision.
Future research should focus on how the relational, temporal, and organizational dimensions identified affect outcomes over time. Longitudinal and codesigned studies are needed to identify which configurations of support actually produce sustainable outcomes in everyday working life.
Footnotes
Acknowledgments
The authors want to thank those who participated in the study and the administrators at the psychiatric clinics for their support in administering the surveys. The authors used Microsoft Copilot, powered by OpenAI's GPT-4, to assist with partial translation from Swedish to English during article preparation. All translated content was reviewed and edited by the authors to ensure accuracy and clarity.
Ethical Considerations
The research adhered to the principles outlined in the Declaration of Helsinki and was approved by Sweden's national ethics review authority (2019-00668).
Consent to Participate
Prior to participating, all respondents in this study provided written, informed consent.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Vetenskapsrådet, Forskningsrådet i Sydöstra Sverige, (grant number 2018-02131, FORSS-910651, FORSS-931117).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data that support the findings of this study are not publicly available due to restrictions. Participants provided consent for data to be shared only at an aggregated group level, ensuring that individual respondents cannot be identified.