
Abstract
Within ADHD scholarship, clinical discussion and lay discourse, there exists a conceptual and ideological conflict between the two dominant theoretical paradigms aimed at understanding ADHD. The paradigm adhered to by an individual, whether it be a biomedical model or a social/neurodiversity paradigm, presents important practical implications with regard to all aspects of their work and its intended audience. For researchers, their chosen ADHD paradigm informs the chosen methodology, theoretical perspective, applicability of findings and readership. For clinicians, their paradigm has direct implications on patient care, advice and intervention use. This paper details the justifications and benefits of each paradigm, alongside the primary criticisms directed from its opposition. The paper concludes with a nascent conceptual heuristic for developing your own theoretical perspective of ADHD to aid in the strengths and implications of your position. This heuristic assists those writing and discussing ADHD to acknowledge and respond to the likely criticisms of their conceptual position.
Lay Abstract
When talking about and trying to understand ADHD, there are many different perspectives in how we should think about ADHD within research and healthcare. The two main ways of looking at ADHD are: the medical way (which is mostly used in healthcare and uses language such as disorder and deficit), and the neurodiversity way (which often describes ADHD as a difference and sometimes a strength). This research paper presents the current strengths and problems with both of these perspectives to help researchers and clinicians develop their own position and be able to respond to any potential criticisms of their way of thinking before they begin their work. This paper also presents a framework or simple model to help people do this, by bringing up some expected challenges to your way of thinking to consider from the very start of your work.
Position Statement
Dr Tom Nicholson is a neurodivergent (AuDHD) lecturer of mental health nursing at Northumbria University where he developed the role of neurodiversity champion of EDI for Nursing, Midwifery and Health. He is a neurodiversity activist and ADHD researcher with an interest in parental experience of neurodivergence, identity formation and illness narrative post-diagnosis, and gifted-neurodivergent (2E) people.
The Conceptual Tension Between Paradigms of ADHD
Attention Deficit Hyperactivity Disorder (ADHD) is one of the most diagnosed childhood conditions (Barkley, 2015; Faraone et al., 2021), affecting an estimated 7.6% of children aged 3–12 and 5.6% of teenagers aged 12–18 (Salari et al., 2023) and 2.5% of adults (Faraone et al., 2021) globally. However, there exists a conceptual and ideological conflict between two dominant paradigms aiming to understand ADHD and other neurodevelopmental conditions which present important practical implications: the medical model versus the neurodiversity paradigm. Sonuga-Barke and Thapar (2021, p. 560) recently discussed whether the neurodiversity concept is helpful for clinicians and scientists; concluding that there are advantages to ‘incorporating the concept of neurodiversity alongside mainstream research and clinical practice’. This paper continues the work of scholars exploring this theoretical tension (Knopes, 2025; Sonuga-Barke & Thapar, 2021) by detailing the primary strengths and criticisms of each paradigm to support clinicians and researchers to develop their own conceptual conclusions regarding the appropriateness of the paradigm's use in their academic and/or clinical work.
Background
The dominant and most pervasive conceptualisation of ADHD in English-speaking Western society defines ADHD as a heterogeneous neurodevelopmental disorder where an individual exhibits deficit within the areas of impulsivity, inattention and hyperactivity. These three core symptom areas form the basis for the categorisation of ADHD under the umbrella of neurodevelopmental disorder within the American Psychiatric Association's (APA) Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-V; APA, 2013) and the World Health Organisation's (WHO) International Classification of Diseases (ICD-10/11) (WHO, 1993, 2018). These two diagnostic manuals form the ‘rulebook’ from which medical authority presents scientific evidence of what can be identified and considered as medical disorder and disease, granting practitioners a categorised list of clinical understandings, potential diagnoses and evidence-based treatment options. However, prior to an exploration and implicit acceptance of a biological construction of ADHD, it is important to illustrate the significant theoretical tension between two opposing paradigms in ADHD's conceptualisation. This theoretical tension exists between the dominant neurobiological medical conceptualisation of ADHD and nonmedical and/or social paradigms of ADHD utilised by the neurodiversity movement and disability scholars.
Despite its categorisation within psychiatric diagnostic manuals, some have argued that there exists ‘no absolute consensus historically or currently on ADHD's status as a health condition’ (Horton-Salway & Davies, 2018, p. 69). Although Pajo and Cohen's (2013) systematic review found 27 of the 30 studies analysed defined or asserted ADHD as a valid disorder, the language used by researchers to describe ADHD varied significantly across the studies, with definitions ranging from: ‘psychiatric disorder’, ‘developmental disorder’, ‘behavioural disorder’, ‘childhood disorder’, ‘neurobiological and neurodevelopmental condition’, ‘neurodevelopmental disorder’, ‘hyperactivity disorder’, ‘invisible disability’, ‘psychiatric illness’ and most commonly ‘attention deficit hyperactivity disorder’. The variable terminology used to frame ADHD within these studies demonstrates a potential controversy within ADHD research; how does one conceptualise ADHD?
There is a growing interest and popularity in the use of social models of disability and strength-based paradigms of ADHD, in which the medical perspective is amended, disregarded, or directly challenged. The most popular non-medical framework is that of neurodiversity or neurodivergence (Chapman, 2020), in which the language of disease, deficit, and disorder are exchanged for the terms neurodivergent, neurodiverse and neuroatypical. Regarding these terms, ‘neurodiversity’ is a term used to describe populations and groups, whereas ‘neurodivergent’ refers to individual people. As there is some debate on who qualifies as being described as ‘neurodivergent’, for the purpose of this paper, the term neurodivergent describes those who fulfil the criteria for a neurodevelopmental condition, diagnosed or otherwise. The neurodiversity movement frames ADHD and other neurodevelopmental disorders within a social model of disability, where lived reality of disability is brought to attention devoid of medical ‘obfuscation’ (Swain et al., 2003). For proponents of a social or neurodiversity model, the priority is not to develop a deeper awareness of disease aetiology and treatment, but to highlight and combat the ‘social barriers, discrimination and exclusion, societal stigma, lack of access to resources and poor perception of the disabled person’ (Swain et al., 2003, p. 24). Some discussion has emerged regarding the tension between these dominant paradigms, with Sonuga-Barke and Thapar (2021) arguing that positive interaction and collaboration across the paradigms would allow for better understanding in the lives and experiences of neurodivergent individuals by acknowledging and transforming discriminatory and impairing environments and social structures, whilst also forging a ‘shared’ narrative of what ADHD means. Additionally, Browning and Veit (2025) argue that these models can be at times overlapping, contradictory and complementary dependent on context and for what purpose they are being employed. However, individuals positioned at the furthest wings of each paradigm may find little shared ground between the biological position of ADHD as neurological deficit (Barkley, 2015), and the social position that neurodiversity is a beneficial strength and ‘wonderful variation of humanity’ (Singh, 2016, p. 1111).
These contrary positions present an interesting challenge for ADHD research, as a researcher's position directly impacts on the methodology and theoretical perspective of the research project. Pajo and Cohen (2013, p. 23) argue that researchers who acknowledge the controversies with ADHD as a concept are more likely to ‘explore the difficulties of mothers to comply with the myths of motherhood’ and to question the medicalisation of childhood behaviours. They also argue that the construction of ADHD utilised by patients and stakeholders directly influences the decision-making process of whether to utilise medication, as a biological construction identifying the negative impairment associated with ADHD (Browning & Veit, 2025) more readily accepts a medical response when compared with social construction. This paper discusses two conceptualisations of ADHD: Biomedical construction and Neurodiversity Paradigm. This paper does not aim to give a conclusive or exhaustive critique on each argument within the various approaches, but to present the primary arguments of each position alongside common criticisms.
The Biomedical Construction of ADHD
The biomedical construction of ADHD presents ADHD as a discrete, categorial neurodevelopmental disorder originating in early development (Sonuga-Barke & Thapar, 2021). This heterogeneous diagnosis is one of the most commonly diagnosed childhood psychiatric disorders and individuals with childhood ADHD continue to present with problematic symptoms into adulthood (Faraone et al., 2021). A medical diagnosis of ADHD requires the individual to present with developmentally inappropriate levels of inattention, impulsivity and hyperactivity, and for these symptoms to have been present for at least six months (APA, 2013; WHO, 2018; Young et al., 2021). Symptoms must be pervasive in nature by presenting within multiple settings, and must cause impairment in daily functioning, typically in the areas of educational, social, emotional and professional settings (APA, 2013; WHO, 2018). Finally, these symptoms must be present within early to mid-childhood and should not be better explained through another disorder or disease. Since there is no universally accepted objective biometric test for ADHD, as is available in other medical conditions such as diabetes, diagnosis is made through clinical observations of behaviour, neuropsychological testing and rating scales (Young et al., 2021). Although there are criticisms of the supposed objectivity of this method of diagnosis, proponents of a medical model of ADHD claim that this method meets the reliability and validity criteria for the diagnosis of psychiatric disorders generally (Faraone, 2005). The biomedical model of ADHD promotes a ‘brain-based discourse’ (Singh, 2002, p. 598) in which ADHD is represented as a neurological matter requiring medical intervention and treatment (Lasky et al., 2016). The findings from a large fMRI study including over 3,000 participants (Hoogman et al., 2017, p. 317) concluded with the authors stating that those with ADHD have ‘truly altered brains’ after presenting clear evidence of altered brain structure within ADHD when compared with controls. They go on to state that ADHD should be labelled as a brain disorder given the robustness of their findings. Barkley (2011, p. 42) uses more negative terminology when he stated that ADHD is a ‘very profound disturbance in one's brain's capacity’.
Regarding an aetiological cause for ADHD, there exists a complex and extensive body of research in which there is no fully encompassing and accepted answer (Young et al., 2021). The biomedical position for ADHD's cause is multidimensional, as genetic, biological and environmental risks coalesce into a complex picture of causation (Faraone et al., 2015; Young et al., 2021). There is evidence to suggest a genetic component to ADHD in which single genetic abnormality has been implicated (Faraone & Larsson, 2018), alongside specific risk allele interaction (Morris-Rosendahl & Crocq, 2020). The increased incidence of ADHD in identical twins when compared with non-identical twins (Barkley, 2015; Larsson et al., 2014) presents further justification for genetic based arguments of ADHD, with genetic explanations being prevalent in UK media (Horton-Salway, 2013). Evidence of increased hereditability is also important to biological arguments of ADHD (Faraone & Larsson, 2018) with evidence suggesting around 40% of children of parents with ADHD have ‘full ADHD’ themselves (Uchida et al., 2022) and a genetic heritability of ∼80% when considering meta-analyses of twin studies (Grimm et al., 2020). This has led some to declare ADHD to be the most ‘genetically influenced psychiatric disorder’ (Barkley, 2015, p. 357). Finally, additional environmental risk factors which impact on biology have been implicated, with low birth weight, nutritional deficiency, exposure to toxicants, smoking during pregnancy and infection all presenting some evidence of increased ADHD risk (Young et al., 2021).
Biomedical constructions of ADHD place the diagnosis within the remit of disease and disorder, requiring effective intervention and treatment to remove the presence of abnormality (Rowlands, 2016). This biomedical classification allows for healthcare policy to categorise people (Casanova & Widman, 2021) into specific healthcare related groups to ensure appropriate and adequate funding and support is available relevant to the ‘size’ of the diagnosed population. Consequently, central nervous system stimulant medications are presented as an effective treatment of the problems and deficits associated with ADHD due to argued neurochemical imbalance. The use of these medications is typically justified due to their capacity to ‘increase the availability of norepinephrine and dopamine’ (Connor, 2015, p. 666) within targeted areas of the brain to ameliorate the reduced presence of these chemicals in those with ADHD (Volkow et al., 2002). Proponents of a biological repertoire point towards the plethora of benefits associated with stimulant medications such as methylphenidate and Lisdexamphetamine and non-stimulants such as Atomoxetine and Guanfacine (when stimulants are contraindicated or poorly tolerated) as further evidence of its biological objectivity (Faraone et al., 2021). Recent meta-analyses (Boland et al., 2020) demonstrate many benefits of ADHD medication, with significantly reduced risk of mood disorders, substance abuse and traumatic brain injury, alongside significantly improved academic outcomes.
Criticisms of the Biological Construction of ADHD
When discussing criticisms of a biological model of ADHD one must acknowledge that any challenge to medical classification or biological conceptualisations can be perceived as a challenge to the ‘reality’ of ADHD. The intention of this section is not to challenge the lived experience of those with ADHD, but to explore potential limitations of a solely biological position.
Gray (2008) demonstrates how the inherent scientific and positivist epistemology of biomedical understandings of ADHD focuses exclusively on improving precision in classification, diagnosis, and treatment. She goes on to argue how the biological reductionism in this position limits exploration and study of ADHD to that of the simple biological components within the individual, avoiding potentially significant factors important to the experience of those with ADHD. This static ‘disembodied brain-based discourse is devoid of contextual data’ (Lasky et al., 2016, p. 161) as it completely negates the impact and influence of environments on the individual. These biological models of psychopathology are argued not to consider the potential that deficits may be due to difficulties in adaptation to environmental context, rather than inherent psychopathological abnormality (Jensen & Hoagwood, 1997, p. 232). Davies (2014) echoes this approach, describing an exclusively biomedical model to be overly simplistic in understanding the complex and nuanced discussion regarding ADHD. Lasky et al. (2016, p. 161) describe ADHD as contextually fluid, as the experience of those with ADHD is often dramatically altered dependent on environment. They go on to question whether it is even necessary to conceptualise the disorder as ‘within the person’ or ‘mental’ at all, bracketing ADHD outside of solely neurological spheres.
Further criticisms are directed at the subjective nature of the diagnostic process, as there is often limited acknowledgement by proponents of biomedical models of the highly subjective clinician interpretations required in assessment (Gray, 2008). Critics question how one is to quantify the boundaries and remit of what is to be considered an ‘impact on functioning’ as outlined within the DSM (APA, 2013), alongside assertions that what is considered ‘impactful’ to one clinician may be minimised by another. Furthermore, the DSM (APA, 2013) requires children to ‘often fail to give close attention’, leading Davies (2018) to question ‘how often is often enough?’. ADHD assessment is perceived not as a ‘value-free scientific endeavour’ (Davies, 2018, p. 45), but a subjective clinical judgement founded on cultural understandings of abnormality and deviancy (Conrad, 1975; Conrad & Potter, 2000). This position becomes particularly salient when considering the disparities in ADHD diagnosis within minoritised populations. U.S evidence suggests people who are Black, Indigenous and Persons of Colour (BIPOC) are less likely to receive a diagnosis even when controlling for confounding factors (Fadus et al., 2020; Shi et al., 2021) and Black people are less likely to receive a diagnosis even when more likely to have ADHD symptoms (Abdelnour et al., 2022). It is also well documented how women are often referred and diagnosed at older ages when compared with men, indicating a societal failure to recognise ADHD in young women (Attoe & Climie, 2023). The lack of clear-cut boundaries between diagnosis and non-diagnosis, and the woolly and imprecise language of psychiatry (Wakefield, 2013) provides further fuel to this position, as empirical uncertainty invalidates the certainty with which ADHD is often discussed (Sonuga-Barke & Thapar, 2021; Stevens et al., 2018).
Additionally, some sociologists have argued that the (over-) medicalisation of (typically childhood) behaviours which correspond with the ADHD diagnostic criteria presents a significant ethical problem (Conrad, 2007). The steep rise in diagnoses of neurodivergent conditions is presented as the ‘colonisation’ of everyday life by medicine (Lusardi, 2019) to control the treatment of those who do not fit the societal norms of that time (Conrad, 2005). The supposed overmedicalisation of ADHD is often ascribed to the capitalistic greed of pharmaceutical companies who benefit from increased diagnostic rates and the development of new symptoms to be ‘treated’. Lusardi (2019) argues that the development of adult ADHD as a diagnosis illustrates a ‘universalising’ of ADHD as a medical category and the next step on the medicalisation journey.
Linguistically, critics of a biomedical construction of ADHD challenge the negative laden language inherent within the paradigm, in which emphasis is placed on dysfunction, deficit, disorder, and disability. The diagnosis of ADHD alone utilises two of these negative attributes, displaying a prioritisation of failings with no acknowledgement of potential benefits. This concept of disorder assumes an agreed recognition of normality (Nesse & Stein, 2012), though it is noteworthy that the WHO (2018) declare disorder as an inexact term. When one reads Barkley's (2011, p. 42) claim that ADHD is a ‘very profound disturbance in one's brain's capacity that makes us uniquely human compared to other primates’, it is difficult not to feel discomfort at the implication that those of us with ADHD have a ‘less human quality’ when compared to those without (Stewart, 2017, p. 92). Some have argued that as the rate and pace of cultural and societal change increases, we may see increased numbers of individual fulfilling the criteria for ‘disorder’ (Aragona, 2009).
It is reasonable to question why this chapter has discussed a solely biological paradigm of ADHD, given that biopsychosocial models are often utilised within UK contexts and include biological, psychological, and social factors as contributing factors. Although a biopsychosocial model does acknowledge the impact of other factors, it leaves the construction of ADHD as a biological condition ‘largely unchallenged’ (Gray, 2008, p. 16). This ‘awkward alliance’ (Davies, 2018) between the psychological, social, and biological discourses does not remove responsibility for pathological symptoms from individuals or question the validity of ADHD as a medical construct but accepts a biomedical conceptualisation of ADHD whilst leaving criticisms of biological reductionism (Gray, 2008) unanswered.
The Neurodiversity Paradigm and ADHD
In recent years, the neurodiversity movement has rejected dominant biological constructions of deficit and disability in relation to ADHD and other neurodevelopmental disorders. Commonly attributed to Singer (2016), though this attribution is challenged by contemporaries (Botha et al., 2025), the term ‘neurodiversity’ has multiple meanings in popular discourse. Some use the term to refer to the variability and diversity in our neuro-cognitive experience, acknowledges the basic fact of human neurological variation in a manner akin to biodiversity (Hughes, 2020). Others use the term to describe a social movement which alters the discourse on how we describe neuro-cognitive differences generally, aiming to frame those with neurodevelopmental disorders/conditions as neurologically different as opposed to neurologically disordered or deficient (O’Dell et al., 2016).
Those with a neurodevelopmental diagnosis or atypical neurological development are often referred to as neurodivergent, neurodiverse, or neuro-atypical; terms felt by many to be more positive and inclusive than the medical use of disability and disorder (Smith & Kirby, 2021). Although there exists ongoing debate within the movement on this terminology due to its assumption of ‘divergence’ or ‘typicality’. This reframing allows the neurodevelopmental disorders to be conceptualised as human variance in which the language of sickness and disease is inappropriate (Tan, 2018). Often pioneered and championed by neurodivergent individuals, the neurodiversity movement promotes a strength-based approach to neurological differences whilst acknowledging the daily challenges faced by neurodivergent people (Houting, 2018). The neurodiversity paradigm is heavily influenced by the social model of disability (Oliver, 2013; Swain et al., 2003) and typically acknowledges the lived experience of impairment whilst denying the framing of the individual as disabled or disordered. Medical models of disability and disorder are argued to ignore the role played by society in excluding those labelled as ‘disabled’ and the contribution of the non-disabled majority in creating social environments where the disabling aspect of impairment is magnified (Anastasiou & Kauffman, 2013; Barnes, 1991). The neurodiversity paradigm defines the experience of impairment as the ‘functional limitation within the individual caused by physical, mental, or sensory impairment’ (Barnes, 1991, p. 2) and places the onus on environments to minimise the impact of impairment and not the individual to treat or ‘cure’ impairment. Consequently, the majority of disadvantages faced by neurodivergent individuals are argued to be due to prejudice, stigma and other systemic, social and environmental barriers rather than inherent biological disability (Shields & Beversdorf, 2020). This perspective positions the neurodivergent as a societally oppressed minority group instead of a medically sick one and has paved the way for the introduction of the term ‘neurominorities’ to communicate this (Doyle, 2020; Smith & Kirby, 2021). Proponents use historic examples of inappropriate medicalisation to further this claim, such as the American Psychiatric Association's (1994) classification of homosexuality as medical disorder until 1973 and subsequent reclassification to social difference (Runswick-Cole, 2014). The linking of neurodivergence with other forms of societal marginalisation and discrimination leads some neurodiversity advocates to argue that any desire to ‘cure’ neurodivergent conditions such as autism and ADHD is on par with wanting to cure someone who is ‘gay, Black, or left-handed’ (Ortega, 2009, p. 9). Consequently, the neurodiversity approach is counter to any intervention aiming to cure or normalise neurodivergent adults (Dwyer, 2022).
A primary tenet within the neurodiversity paradigm is that all neurological diversity is valuable within the right context and environments (Houting, 2018). Although there have been few empirical studies focussing specifically on the strengths of ADHD, a variety of ADHD related benefits have emerged across the literature. These positives include increased creativity (Brod et al., 2012), improved creativity in problem solving (Schreuera & Dorot, 2017; Zentall et al., 2001), higher levels of passion, enthusiasm and performance in areas of specific interest (Lasky et al., 2016), increased energy and speed (Rosenfield et al., 2008) and increased entrepreneurship (Wiklund et al., 2017). The neurodiversity paradigm claims that biomedical conceptualisations of ADHD not only minimise or ignore these ADHD-related strengths, but risk the eradication of these strengths through medicalisation, ‘treatment’ of difference, and deficit driven narratives. Unlike biomedical and biopsychosocial approaches, the neurodiversity paradigm may be used to directly oppose the core assumptions of a biological model of disability for ADHD, as the reduction of the ‘unwanted symptoms’ of inattention and hyperactivity through the altering of brain chemistry via medication is seen as a masking of the ‘real’ issue. Proponents of neurodiversity may argue that if a child with ADHD is struggling to engage with schoolwork, then responsibility is on the school environment to adapt and alter to fit the needs of the child, and not for the child to be chemically altered to fit in with an ineffective environment.
Strength-based approaches may also include even more positive conceptualisations of ADHD, in which it is narrated as a superpower. This growing trend is proving increasingly popular outside of academia, and is often utilised in children's books (Larson, 2020; Lazarus, 2021) and UK news articles (Brown, 2019). On the more radical end of the neurodiversity movement, some argue that any impairment faced by a neurodivergent individual occurs due to the mismatch of individual and society, and that further research and exploration into improving diagnosis and treatment of ADHD is theoretically inappropriate (Sonuga-Barke & Thapar, 2021). This wholly positive conceptualisation of ADHD, within which ADHD children may be labelled ‘indigo’ or the ‘next stage of human evolution’ has been argued to stretch beyond the boundaries of the neurodiversity movement and has become a movement in its own right (Carroll & Tober, 1999; Lench et al., 2011; Singler, 2015, 2017). As one parent in Nicholson (2023) states: ‘I think they are like the superheroes of society. People in the world label it as a “disability”, but I completely disagree with that. It's wrong. It's completely wrong’.
Criticisms of Neurodiversity
As with the biological paradigm of ADHD, noteworthy criticisms have been directed towards a solely social or neurodiversity conceptualisation. Naturally, the arguments brought forward within this paper on the strengths of a biomedical model are utilised by proponents of a biological perspective to challenge the neurodiversity perspective; however, these arguments do not typically challenge the theoretical perspective of neurodiversity. The framing of ADHD and other neurodevelopmental conditions as ‘cultural identity’ or individual difference is argued to disregard the experience of those who feel disabled and impaired by their ADHD experience (Houting, 2018). One must acknowledge how the paradigm can lead some to a ‘Pollyanna’ version of the movement, in which excessively optimistic portrayals of neurodevelopmental difference ignore the real-life experience of challenge and impairment. Although a social model of disability would prioritise disability arising from ableist prejudice and gaps in accessibility within social structures (Shields & Beversdorf, 2020), critics of a solely neurodiversity perspective and many with neurodevelopmental conditions point towards the individual experience of impairment outside of these structures. Additionally, the ‘identity’ perspective of neurodiversity has been likened to ‘identity politics’ which result in ‘oppressor versus oppressed’ mentalities between competing groups (Casanova & Widman, 2021).
A second criticism relates to how the neurodiversity movement is felt to be primarily appropriate for those with minimal support needs, often described as ‘higher functioning’ individuals (Houting, 2018). Those outside of this ‘higher functioning’ group are argued to be less able to utilise the movement's rhetoric due to a more pronounced experience of disability. However, Houting (2018) disagrees, declaring that the dichotomisation of people into high- and low-functioning categories erases the variation in ability across multiple skills and ability inherent to the movement's perspective. The denial of autonomy and agency for those classed as ‘low functioning’, alongside restriction of access to support for ‘high functioning’ individuals, exemplifies the ableist prejudice the paradigm aims to abolish. However, the homogenisation of ‘disabled’ people and their experiences has also been criticised (Runswick-Cole, 2014), and the binary grouping of individuals into neurodivergent/neurotypical may further marginalise and exclude those with differing needs within the group. The restriction of access to support is of particular interest, as the positive framing of neurodiverse conditions may imply a reduced need for social support due to it being a ‘natural variation’. This does present a challenge for neurodiversity campaigners and advocates who aim to extol the strengths and benefits of neurological variation and cultivate respect and acceptance, whilst also fighting for the support and interventions necessary to meet these differing needs. Runswick-Cole (2014, p. 1124) points towards the ‘inherent contradiction’ of arguing for neurodivergent rights and recognition for their ‘differences’ whilst also wishing to claim natural variation. The simultaneous claim that neurodivergent and ‘non-neurodivergent’ people are both the same and different presents a theoretical challenge which is exacerbated further by positioning of individual into us versus them groups of the ‘neurodivergent’ versus ‘the neurotypical’ (Casanova & Widman, 2021). Incidentally, the complete de-pathologisation of neurodivergence may inadvertently prevent individuals from being able to access evidence-based treatments and supportive services (Knopes, 2025) if neurodivergence no longer represents a ‘medical problem’.
Hughes (2020) presents a further challenge to the neurodiversity movement with regard to the heterogeneity of autism. As with the diagnosis of ADHD, there exists huge variation across the experience of ‘being autistic’ or even ‘being neurodivergent’. Chapman (2019) argues that those with very significant challenges may have their difficulties presented as ‘obviously pathological’ and not wholly social. For those whose sensory sensitivities leave them unable to tolerate common environments or experience significant emotional distress at minor changes in routine, a fully social paradigm may be deemed inappropriate as active intervention is required to render these experiences less disabling (Hughes, 2020). With regard to ADHD, this area of the severity spectrum includes individuals with such significant impulsivity they are physically harmed due to their own actions (such as motor accidents or death by misadventure) independent of societal discrimination. As Hughes (2020, p. 55) states, ‘severe manifestations with impulse control may remain significantly disabling even when all possible (and plausible) forms of support have been provided’.
An additional criticism of note is Neumeier's (2018) concept of ‘neurodiversity lite’. Neumeier argues that the paradigm may be adopted by ‘non-neurodivergent newcomers’ to neurodiversity who wish to utilise the feel-good positive language of the movement and give lip service to neurodivergent individuals’ inherent worth with minimal changes in effective accommodation or inclusivity. Those who employ the rhetoric of neurodiversity without fully understanding the foundational assumptions of the movement are likely to cause harm to its aims and credibility and may end up infantilising or placing neurodivergent individuals on a pedestal due to misunderstandings. Neumeier (2018) defines this process as ‘neurodiversity lite’, arguing that at best it unintentionally undermines the movement by using language which overlooks or contradicts the core concepts of neurodiversity, but at worst ‘disguises ableist stereotypes and harmful practices’ by allowing service providers to sound like they are supporting neurodivergent individuals whilst doing nothing to change practice.
The final criticism to consider challenges the conceptual legitimacy of the neurodiversity paradigm itself. Emerging discussion queries whether the theoretical concept of neurodiversity has become a white, Eurocentric or Global North paradigm which ‘destabilises the social justice and emancipation goals of the movement’ (Nair et al., 2024). Scholars question whether the lack of inclusion of Global South perspectives and the erasure of non-northern, non-white knowledge has led to a theory of neurodiversity which fails to truly acknowledge the impact of racism, ableism, white supremacy colonialism, imperialism, patriarchy, capitalism and other marginalising forces (Nair et al., 2024, p. 2). By ‘unmasking’ neurodiversity as being principally ‘white neurodiversity’ stemming from the USA, UK and Australia, we are then able to incorporate knowledge production not solely from a Global North or Eurocentric perspective, situating the current neurodiversity paradigm as ‘part of a vast global knowledge continuum, rather than a singular dominant Western notion’ (Nair et al., 2024).
A Conceptual Heuristic for Developing Your Own Perspective of ADHD
The following section includes a nascent heuristic that could be used by academics, clinicians, and other professionals working in the field of neurodiversity to aid in some conceptual considerations of their chosen paradigm. Attempts to develop conceptual models amalgamating the medical and neurodiversity perspectives have already been presented by others, such as Casanova and Widman's (2021) Biological Gradient Model (BGM). The BGM attempts to be a ‘neutral’ functional middle ground between the two models which remains rooted in ‘biological science (Casanova & Widman, 2021, p. 370). However, the heuristic presented within this paper is not intended to be a ‘catch-all’ improvement on the models presented thus far, but a tool for academics and researchers to consider when thinking about their own perspectives. The heuristic presents a series of paradigm specific considerations and queries to assist those writing about neurodiversity/neurodivergence to respond to, or at least acknowledge, the primary criticisms of their conceptual position within their work. The heuristic does not present an exhaustive list of considerations, nor is it claimed to be the perfect tool to ensure theoretical congruence across the literature. It is hoped to assist those writing from their position on the medical-to-neurodiversity paradigm in responding to the most likely criticisms from those elsewhere on said paradigm to enable more robust and considered theoretical positioning within academic and clinical work.
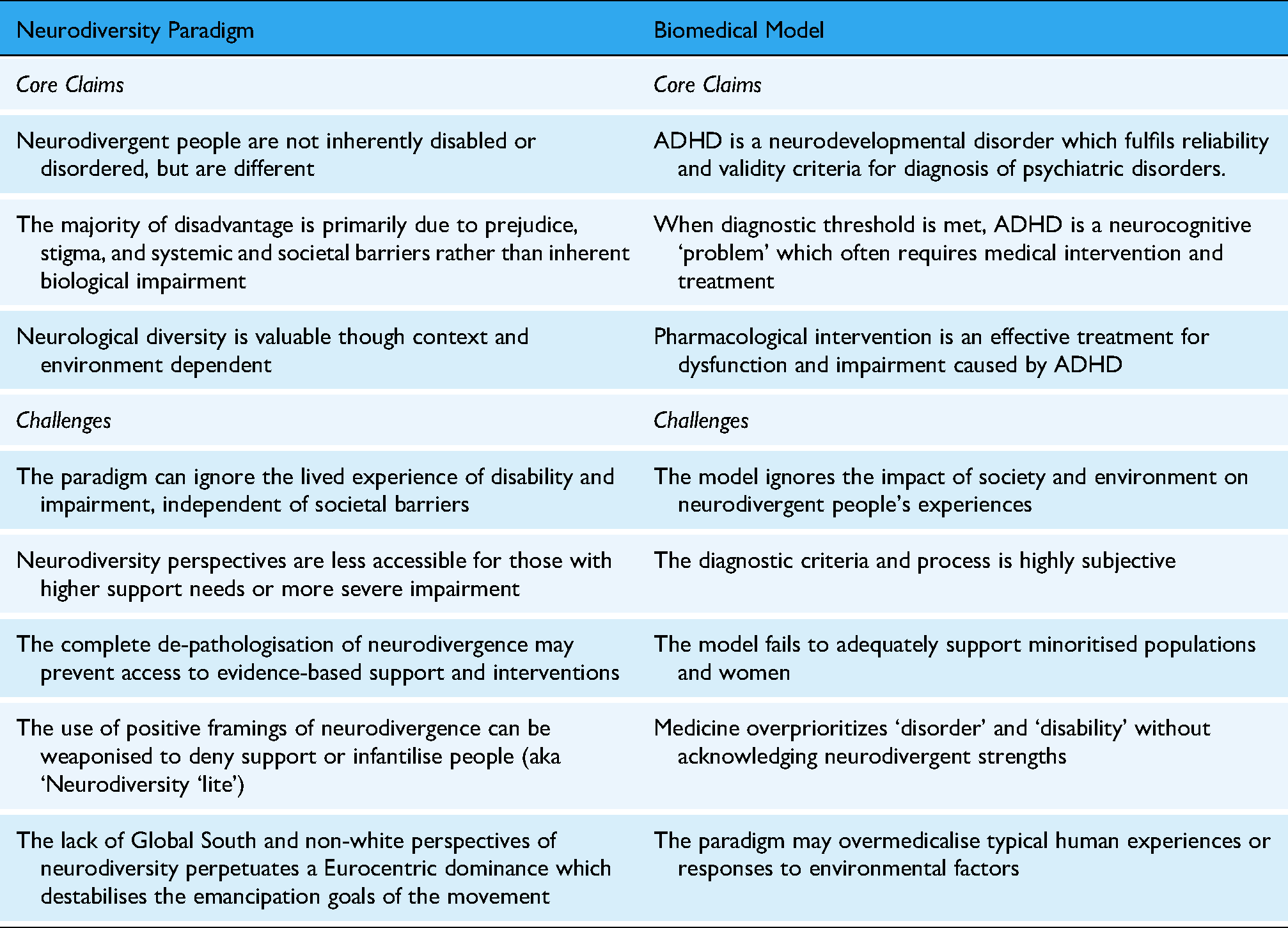
Summary Table of Paradigm Claims and Challenges
Paradigm Heuristic
Questions to consider when developing your own theoretical perspective of neurodivergence:
Am I assuming there is a ‘normal’ brain from which others deviate, and does this constitute a medical problem?
What are my beliefs around the limits of medicine and medicalisation?
What do you consider to be the benefits of diagnosis and medical treatment?
What should be done to help those with the most severe impairments?
How can ‘neurodiversity lite’ be avoided?
What impact do you think colonialism and Eurocentrism has had upon the neurodiversity paradigm?
If neurodiversity was fully accepted as simply a ‘difference’ and not ‘medical problem’, how can we justify medical support or interventions for those who want/need it?
What are the main strengths of the biomedical paradigm?
What impact do you think social environments have upon the success of diagnosis and medical treatment?
What can be done to help those without a diagnosis?
In what way are diagnostic criteria subjective?
How can we quantify the threshold between ‘diagnosis’ and ‘non-diagnosis’?
Why is it important to consider the views and experiences of non-white and marginalised populations in relation to neurodiversity?
What are the main strengths of the neurodiversity paradigm?
Conclusions
In conclusion, the biological and neurodiversity paradigms of ADHD pose an interesting and contentious area for debate. This paper does not attempt to convince readers of which paradigm is the ‘right’ model of ADHD as this is the ‘wrong question’ to ask (Browning & Veit, 2025) but instead aims to develop understanding of the interplay between these dominant paradigms so that researchers and clinicians alike can make conscious and informed decisions on their use. The ability for clinicians tasked with assessing and diagnosing neurodivergent conditions to have nuanced conceptual discussions regarding medical and/or neurodiversity models of ADHD is becoming increasingly important. Emerging evidence has demonstrated that the narratives of parents of children undergoing the ADHD diagnostic journey typically present a preference for one of the two dominant paradigms (Nicholson, 2023; Nicholson & Lee, 2024), where other research has shown how people with neurodivergent conditions employ multiple models of mental health to find meaning in their experiences (Knopes, 2025). However, these preferences are often amorphous and changeable over time, with parents and patients attempting to develop a personal conceptual position of ADHD which encompasses the benefits of a neurodiversity paradigm alongside those of a medical one.
Footnotes
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.