
Abstract
Neurodivergent people (e.g., dyslexic people) do not always agree with the terms commonly used by others (e.g., professionals) to describe their neurodivergence. Our mixed methods study aimed to investigate terminology preferences for different categories of developmental neurodivergence (e.g., autism, dyspraxia) among people from those communities. Participants (n = 902) completed an online survey, ranking the likeability and offensiveness of a range of person-first and identify-first terms for their diagnoses. We invited them to tell us reasons for their preferences via open text response, which we analysed using thematic analysis. Paired samples on identity vs. person first preferences showed identity first language was significantly more likeable, and significantly less offensive for most categories, but not all (stuttering and Tourette syndrome). For the thematic analysis, we developed two key themes, (1) ‘How they talk about us’, which focussed on the inadequacy of existing terminology, and the stigma associated with particular labels, and (2) ‘How we talk about us’, which focussed on viscerality of certain terms, agency to express personal preferences, debates around identity vs. person first terms, and identification with the concept of ‘disability’. Our findings have implications for how neurodivergent people are described, especially by those in professional services.
Keywords
Introduction
Neurodiversity is an umbrella term used to describe the idea that there are many different ways that humans might think and behave, and that these differences are underpinned by variations in our neurology (Botha et al., 2024; Dallman et al., 2022; Kapp et al., 2013). Neurodiversity includes both neurotypical people (people whose way of thinking and behaving aligns with the assumed norm (Botha et al., 2024), and neurodivergent people (people whose way of thinking and behaving diverges from the assumed norm (Stenning & Rosqvist, 2021). There are debates as to who counts as neurodivergent, despite the fact that the term neurodivergent was intended to be used inclusively (Asasumasu, 2016). Some academic researchers use the term to refer only to people with a developmental diagnosis (e.g., autism, dyslexia) whereas others follow Asasumasu's designation, including psychiatric conditions (Stenner et al., 2025; Wise, 2023) and other acquired neurological differences (Rose, 2024; Walker, 2021). Though we the authors subscribe to the latter view, this paper focuses on developmental neurodivergence only (which for us includes people with learning disabilities, often referred to outside of the UK as ‘Intellectual Disabilities’) as that is where our collective expertise lies.
Historically, the approach to developmental neurodivergence has been one of pathology, framed through a medical model approach (Chapman & Botha, 2023; Pearson & Rose, 2023). Diagnoses such as autism, attention deficit hyperactivity disorder (ADHD), etc., were formulated as developmental disorders, representing deficits and impairments across a range of domains compared to the neurotypical population (American Psychiatric Association, 2013). This approach aligns with the notion of ableism, which is characterised by harmful assumptions, beliefs, or behaviours inferring that disabled people are inferior (Wolbring, 2008).
The broader disability rights movement led critics of the medical model to advocate for a less pathologizing approach to disability, including the use of person-first language (PFL) to describe ‘people with disabilities’ (including those with developmental disorders), putting the person before the diagnosis to de-stigmatise them. However, PFL was not necessarily the preference of disabled people themselves (see Andrews et al., 2022a, 2022b). Disability advocates argued that attempts to separate the person from their disability perpetuates stigma by asserting that the disability is something ideally removed or eradicated (Botha et al., 2020; Oliver & Oliver, 1996). Attempts to distance oneself from the label of disabled is termed ‘internalised ableism’, that is, taking on the assertion that to be disabled is to be lesser (Brown & Leigh, 2020). Disability advocates propose that identity-first language (or IFL) recognises how entangled disability is with other defining aspects of selfhood, and that others should not need to be reminded that someone is a person first to treat them like one.
The tension between medical and social approaches has led to the emergence of a rich dialogue in autism research regarding the pathologisation of autistic people (Botha, 2021a; Bridget et al., 2023), and the harms that this facilitates (Botha & Cage, 2022; McGuire, 2016; Neumeier & Brown, 2020). Community members and researchers have provided recommendations for shifting towards a more humanising approach (Botha, 2021c; CAPTAP, 2023; McGreevy et al., 2024; Pearson, 2021). Anti-ableist language (i.e., language that does not frame autistic people as lesser) is one such recommendation (Bottema-Beutel et al., 2020), based on the role that language, labelling and rhetoric can play in creating and perpetuating stigma (Keates et al., 2025; Natri et al., 2023). Anti-ableist language can also help address the issue of hermeneutical injustice, that is, the exclusion of marginalised groups from collective meaning-making about themselves leading to a lack of suitable terminology to understand their experiences (Harding, 1991). Most global Northern research on autistic language preferences points towards a community-level 1 preference for identity-first terminology (Botha et al., 2020; Bury et al., 2023; Keating et al., 2023a; Kenny et al., 2016; Taboas et al., 2023) in addition to avoidance of terms such as ‘disorder’ and ‘deficit’, though this is certainly not unanimous in nature (Buijsman et al., 2023; Flowers et al., 2023).
However, we currently know very little about whether such terminology preferences exist among other developmentally neurodivergent people and groups, though there is an emerging body of evidence (Louis, 1999; Nah & Lim, 2025; Zisk & Konyn, 2022). The term disabled people became politicised through the disability rights movement (Oliver & Barnes, 2012). From this perspective, impairment 2 is what differentiates individuals; under the social model, disability arises through the lack of fit between person and environment (e.g., lack of wheelchair access), whereas impairment refers to individual characteristics of a particular condition (e.g., being unable to walk). As such, social modelists to use the term disabled people for groups, and PFL to refer to specific impairment types, for example, people with dyslexia, etc. As the neurodiversity movement has evolved, IFL has increasingly been applied for individuals, for example, dyslexic people, despite some groups historically preferring person-first (Louis, 1999). This shift represents an extension of the original politicised terminology that emerged from the UK disability rights movement. Similarly, there is an increase in uptake of neurodiversity-related terminology among other neurodivergent groups beyond autistic people (see ADHD Foundation, n.d.; British Dyslexia Association, n.d.) and an emerging discussion around the impact of pathologisation and stigma on members of these communities (Carr-Fanning, 2020; Cook, 2024). Nah & Lim, (2025) recently explored identity versus person first language preferences among university students with a diagnosis of autism, ADHD or Speech and Language Difficulties, finding an overall preference for person-first terminology. However, the authors acknowledge that the terminology options provided to participants might have underpinned these preferences.
The aim of the current study was to examine language and terminology preferences related to developmental neurodivergence among neurodivergent people themselves, using a mixed methods survey.
Method
Positionality and community involvement
All members of the research team are neurodivergent, and among us we have experience of many of the categories of neurodivergence that we include in the current study. Where we did not have lived experience (e.g., Tourette's), we asked people from those communities to discuss terminology options and potential terms for inclusion.
Participants
We recruited participants using convenience and snowball sampling between May and September 2022. We distributed the survey across various organisations (including BoingBoing, North East Autism Society, Autistic UK, ADHD UK) and personal/social networks (e.g., X – formerly Twitter, Facebook). Eligible individuals were:
Aged 18 years or older. Living in the UK. Neurodivergent (including diagnosed or self-identifying), defined as having at least one form of developmental neurodivergence from a list provided (see Supplemental Materials).
3
Once we had removed people who did not answer any questions after completing the consent form, we had a total of 902 participants (see Table 1).
Demographic Data for all Participants.
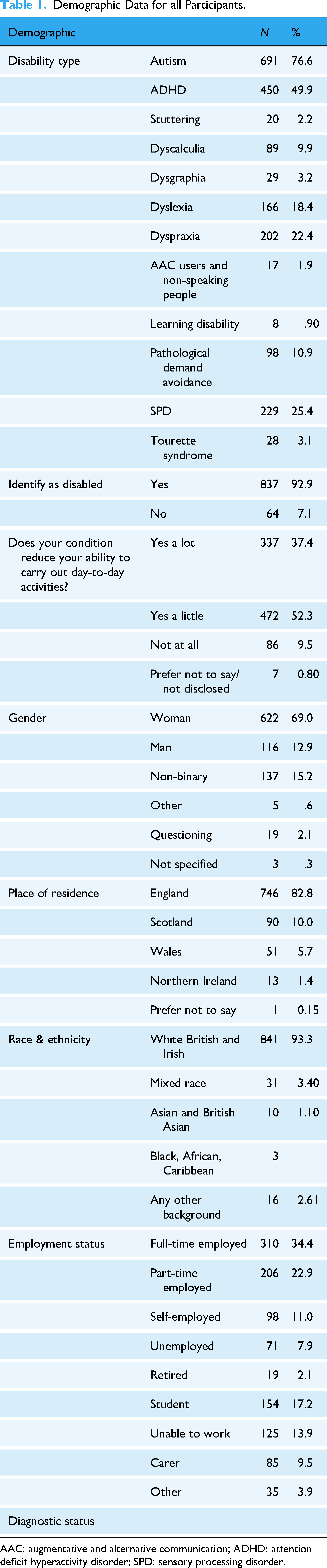
AAC: augmentative and alternative communication; ADHD: attention deficit hyperactivity disorder; SPD: sensory processing disorder.
The age of participants who answered the closed questions ranged from 18 to 80 (M = 37.7; SD = 10.8).
The majority of people who took part had a clinical diagnosis, however this varied by category (see Table 2). The majority of people had more than one diagnosis (M = 2.2).
Diagnostic status per Category.

AAC: augmentative and alternative communication; ADHD: attention deficit hyperactivity disorder; PDA: pathological demand avoidance; SPD: sensory processing disorder.
In total, 511 people answered the qualitative opened-text question about why they use the language that they do per each disability (see Supplemental Materials). The demographic split between those who only did the ranking exercise, versus those who also answered the specific qualitative questions is largely similar. This study received ethical approval from the University of Sunderland.
Design
We took a mixed methods approach, gathering both quantitative (rating) data, and qualitative (open text) data, enabling examination of how strongly people felt about terminology, and why they felt this way. We wanted to know how much people liked their preferred terms, and how offensive they found their non-preferred terms. In the qualitative data, we explored the reasons people gave for their preferences.
Materials
We developed an online survey hosted on Qualtrics software. During survey development, we decided that it was important to keep language as plain as possible to try to increase accessibility. We reviewed the questions multiple times to ensure they were written in plain English. The survey had four main sections (see Appendix 1 for full instrument in Supplemental Materials). First, we collected demographic data (see Table 1). Second, we asked questions about each neurodevelopmental disability participants reported. We used the term ‘neurodevelopmental disability’ as we felt it was a neutral descriptive term and wanted to avoid biasing participants towards or against neurodiversity paradigm language with our own framing. For each reported disability we asked participants to rate how much they liked each term on a 7-point Likert scale (from strongly dislike to strongly like) and then to rank the terms from most to least favourite. We also asked them to rate each term on offensiveness on a 7-point Likert scale (from low offensiveness to extremely offensive). We provided open text boxes for participants to explain why they had made these decisions. Finally, we asked participants two closed questions on neurodiversity, and some open questions about neurodiversity language which we report separately (Grant et al., 2025).
Procedure
Upon opening the survey, participants read an information sheet and completed a consent form. They then completed each section of the survey for each disability they selected, followed by the open-text questions. Finally, we thanked them for their time.
Data analysis
Quantitative data
Where we had an adequate sample size for meaningful comparison (n > 20) we used paired-sample t-tests to calculate differences in likeability and offensiveness of identity-first, versus person-first variants of language for each neurodevelopmental disability. We did this by grouping construction types (IFL vs PFL), creating mean scores for likeability and offensiveness, and conducting two-tailed paired sample t-tests (we used two-tailed p-values as for most of the groups we did not hypothesize the direction of difference). A threshold of < 0.05 was used to determine significance in any inferential testing and we calculated effect sizes. We then used descriptive statistics to explore nuanced variation in terminology preferences per disability, median ranks of likeability and offensiveness of each phrasing per disability type, and mean scores of likeability and offensiveness of each phrasing. The sample size varies per disability due to the nature of the survey, and each subsample is stated in the findings per disability type. We do not report inferential data where N < 20 (global developmental delay, N = 2, and learning disabilities, N = 8).
Qualitative data
We analysed the qualitative data using a reflexive thematic analysis with an inductive approach following the steps outlined by Braun and Clarke (2006, 2020). We had a large volume of data, however most of the responses were one sentence or less. We imported the data into NVivo 14. AP started with data familiarisation and then coded the data independently in NVivo, one participant at a time. Once AP had coded the data and refined the codes, she met with AG, MB and JL to discuss. AP then further refined these codes and sorted them into initial themes and confirmed with the wider team. We used a critical realist approach to guide our interpretations throughout the analysis, acknowledging that each neurodivergent person's experience of reality is impacted by their own individual circumstances (Botha, 2021b).
Results
Quantitative data
Overall preference for identity-first versus person first language
We used paired sample t-tests to examine whether there was any significant difference in preferences and offensiveness ratings overall between identity and person-first formations across varying disability groups. Identity first language was significantly more likeable, and significantly less offensive than person-first within the categories of autism, ADHD, dyslexia, dyscalculia, dysgraphia, dyspraxia and pathological demand avoidance (PDA) (see Table 3). People who stutter did not show a significant preference towards either identity or person first language, however this sample size was the most restricted, and it trended towards a preference for person-first. Those with Tourette's found person-first significantly more likeable than identity-first, and significantly less offensive. All of the effect sizes for each of these results were large (Cohen's d = >0.80). Figures in Supplemental Materials display the mean scores, and distributions of likeability and offensiveness across categories for each group.
Preference for IFL Versus PFL Within Each Diagnostic Category Based on Offensiveness and Likeability. 4

ADHD: attention deficit hyperactivity disorder; PDA: pathological demand avoidance.
Preference by group
Here we present the rankings for each group. It is worth noting that for some groups ‘other’ was ranked as most likeable and least offensive, however where this is the case, participants did not necessarily provide an alternative ‘other’ preferred term themselves. Where suggested terms were provided, we give examples in Supplemental Materials.
Autism
The highest-ranked terms with the highest mean rating for likeability were ‘autistic’ (M = 6.25), followed by ‘autistic person’ (M = 5.90). The lowest-ranked and least likeable items based on mean scores were ‘aspergic’ (M = 1.70) and ‘person with asperger syndrome’ (M = 2.06). ‘Autistic’ (M = 1.30) and ‘autistic person’ (M = 1.40) were also ranked and rated as being the least offensive with mean offensiveness scores, respectively, whereas ‘aspergic’ (M = 4.58) and ‘person with asperger syndrome’ (M = 4.28) had the highest offensive scores.
Attention deficit hyperactivity disorder
The highest rated item based on mean likeability scores for ADHD was the ‘other’ category, pointing to high variation of preferred terms and a lack of consensus. This is further supported in that despite the overall preference being for IFL in the t-tests, this was namely driven by low likeability scores for ‘person with attention differences’ (M = 2.96), as based on individual items, the second highest mean score was ‘person with ADHD’ with a mean score of 4.38). In terms of rank, both ‘person with ADHD’ and ‘ADHDer’ share a rank preference of 2.
‘Person with ADHD’ had the lowest mean offense rating (M = 2.16), while the most offensive based on means was ‘person with attention differences’ (M = 2.89). This was supported in the rank data with ‘person with ADHD’ and ‘ADHDer’ sharing a rank of 1 (least offensive). However, despite small differences the overall offense ratings could be considered low, given that the minimum score is 1, and the maximum is 7, and all scores cluster below 3.
Dyscalculia
The highest mean score for an individual item was for the IFL formation ‘dyscalculic’ (M = 4.76), followed by a PFL formation of ‘person with dyscalculia’ (M = 4.53). These two items were also ranked the highest alongside ‘dyscalculic person’ (Rank = 2). Person first options seemed weighted down by non-specific terminology variations, that is, ‘person with specific learning disorder’ was rated as the least likeable based on both mean score (M = 2.35) and rank (Rank = 6) (aside from the ‘other’ option).
‘Dyscalculic’ was similarly rated as the least offensive based on both mean scores (M = 1.66) and rank (Rank = 5), with the items ‘person with dyscalculia’ following it (Rank = 4). The non-specific PFL formations were all rated as the most offensive.
Dysgraphia
Based on mean likeability scores, identity first formations were the highest rated for likeability including ‘dysgraphic’ (M = 5.48) and ‘dysgraphic person’ (M = 4.66). These items were also ranked most highly as being the most likeable (Rank = 1; Rank = 2, respectively).
Similarly to dyscalculia, non-specific PFL formations were rated as the least likeable, with a ‘person with a specific learning disability’ having the lowest mean score (M = 2.83), and rated as least likeable and most offensive.
Dyslexia
Dyslexic (M = 5.70; Rank = 1) and dyslexic person (M = 4.75; Rank = 2) were rated on the most likeable based on mean scores and rank. These were also rated as the least offensive, respectively (M = 1.93; M = 1.46) and ranked as the least offensive.
Non-specific PFL formations were rated as the least likeable, with ‘A person with a specific learning disorder’ having the lowest mean score (M = 2.50), as they were with other similar diagnoses (dysgraphia, and dyscalculia). These items were also rated as the most offensive by mean scores, and rank.
Dyspraxia
Identity first language formations of ‘Dyspraxic’ (M = 5.85; Rank = 1) and ‘dyspraxic person’ (M = 5.05; Rank = 2) were rated on the most likeable based on mean scores and rank. These were also rated as the least offensive, respectively) (M = 1.48; M = 1.63) and ranked as the least offensive.
Person first formations of ‘Person with a developmental coordination disorder’ (M = 2.78, Rank = 5) and ‘Person with a developmental movement condition’ (M = 2.94, Rank = 4) were rated as the least likeable, having the lowest mean scores and ranks. These items were also rated as the most offensive by mean scores, and rank.
Non-speaking and or AAC users
We had 17 participants in the non-speaking group, however we have chosen to include the rank data as non-speakers are often systematically excluded from research. Augmentative and alternative communication (AAC) user (M = 5.59; Rank = 1) and semi-speaking (M = 5.47; Rank = 2)/non-speaking (M = 5.41, Rank = 3) were rated on the most likeable based on mean scores and rank. Non-speaking was also rated least offensive, with AAC user a close second.
Non-specific PFL formations were rated as the least likeable, with a ‘Person who cannot rely on speech to be understood’ having the lowest mean score (M = 2.47). ‘Mute’ was a close second (M = 2.65) and was also ranked as most offensive (M = 4.24).
Pathological demand avoidance
For PDA, ‘other’ was rated as most likeable (M = 5.56, Rank = 1), and ‘person with demand avoidance’ rated as least likeable (M = 2.52) but person with demand avoidance phenomena was rated as the most offensive (M = 3.76). The least offensive term was ‘PDA’er’ (M = 1.78).
Sensory processing disorder
For SPD ‘other’ was most likeable (M = 4.64) and least offensive (M = 2.20). ‘Person with Irlen Syndrome’ conversely was rated least likeable (M = 3.75) and most offensive (M = 2.52).
Stuttering
‘Stutterer’ also had the highest mean offensiveness score (M = 3.19) but these scores largely overlapped making it hard to differentiate.
Tourette's
For Tourette Syndrome, ‘other’ was rated most likeable (M = 5.17). ‘Touretter’ was both least likeable (M = 3.52) and most offensive (M = 3.15). ‘Person with Tourette's’ was rated least offensive (M = 1.85).
Qualitative data
We developed two overarching themes (see Figure 1) to address what people think about different kinds of terminology. Theme 1 ‘How they talk about us’, explored how the labels used to describe developmental neurodivergence are ill-fitting, and associated with stigmatising perceptions. Theme 2 ‘How we talk about us’, describes the complex and interrelated reasons given for language preferences.

Themes and sub-themes from thematic analysis.
Theme 1: How they talk about us
Theme 1 centred on the development of labels for neurodevelopmental disabilities, and the impact of such labels being used to speak about neurodivergent people.
Existing labels are inadequate
One of the key issues identified by participants was the overall lack of suitable terminology to describe neurodivergence. Existing labels were seen as insufficient and imprecise, with participants describing how they often feel ‘vague’ and ‘awkward’, and do not ‘truly describe lived experience’. Whilst many people described not necessarily finding terms that they disliked offensive, they described finding terminology unsuitable because it did not really align well with their experiences. This was particularly highlighted by participants who argued that terms like ADHD or DCD (aka. Dyspraxia) do not seem to capture ‘all of the struggles’. They argued that such terms can ‘minimise’ their experiences and lead to further misconceptions. Likewise, participants with a diagnosis of PDA felt that the language used currently infers a level of intentionality that suggests they are ‘*choosing* to inconvenience others by not paying attention to priorities set for them by other people’ (p. 44). They highlighted that their experiences of demand avoidance were ‘anxiety. Not just a choice’ and that current conceptualisations suggested that they ‘cannot be trusted with free will and to make good choices’. However, many participants also acknowledged that community attempts to create identity first or more precise terms for labels like ADHD have been ‘clunky’ or grammatically incorrect. As such, participants felt that accurate language was important, but that it was hard to get right: I don't feel any are particularly offensive however the terms ranked at the top are very generic and do not accurately reflect what dyscalculia is. I prefer the term difficulties or disability over disorder. However difficulties can sound trivial. (p24)
For many participants, a crucial issue was how the terminology was used and understood. They felt that many ‘official’ diagnostic terms had been developed in a way that did not integrate the experiences of those being diagnosed (and thus did not accurately reflect their experiences), and that this leads to out-group (or neurotypical) members having a limited understanding as a result: ‘Saying a person with a learning disability or a specific learning disorder or any of the others, is long winded, and non-specific which means it doesn’t relay what help they person may need’ (p. 176). This limited understanding then creates a vicious cycle in interaction with the label itself, whereby ‘labels become filters everything is viewed through and can be used to dismiss us when we say or do something other people do not want to have to think about’ (p. 462).
Similarly, participants highlighted the tendency of labels to lead to expectations of homogeneity. Despite frequent lip service to the ‘heterogenous’ nature of neurodivergent people (both within and across groups), participants felt that imprecise language led to expectations of similarity and stereotyping. For example, despite a large majority of autistic people expressing dislike of the term ‘Aspergers syndrome’, one participant highlighted that such terms had historically been used by some autistic people to ‘achieve the understanding they need in the moment’ (p. 369) when assumptions had been made about the relationship between autism and co-occurring learning disabilities.
Overall, existing terminology was seen to be limiting, inadequate and a potential reinforcer of harmful stereotypes. Participants longed for appropriate and fitting terminology, but struggled to find alternative terms that did not lead to the same issues being replicated.
Pathology, Ableism and stigma
One of the most frequently cited reasons for terminology preferences was a dislike of language that pathologises, reinforcing the idea that being ‘neurotypical’ is most desirable and perpetuating stigma against people who diverge from this allegedly ideal norm. The term ‘disorder’ was overwhelmingly highlighted as implying ‘deviation from an imagined normal’ (p. 874) or an ‘unobtainable version of perfect’ (p. 108) and made people feel like there was ‘something incredibly wrong’ (p. 593) with them. Participants also explicitly noted that such terms have negative connotations due to the stigma that accompany them, making it ‘harder to be accepted’ (p. 515) by others. They wanted to make it clear that they were not ‘defective’. This was true even where participants saw their neurodivergence as causing significant difficulties, as highlighted by one of our participants with a diagnosis of dyspraxia: My dyspraxia causes physical injury a lot and has to be factored in with my physical health (e.g., on my hospital risk of falling notes) so I'm less offended by clinical terms like ‘person with dyspraxia’. It's also not crucial to my identity like autism is because it only really impacts my movement and coordination. But I really don't like disorder language still, it implies I'm broken. (p. 201)
Participants wrote about the impact that such labels had on them, noting that words like disorder ‘set us up for shame’ (p. 576). They also suggested that it was possible to ‘understand these issues [that people experience] in a neutral way … which can occasionally be problematic but not always’ (p. 161), hinting at the role that society and environment play in shaping outcomes for neurodivergent people. Indeed, participants suggested that accessibility and accommodations challenge the view that there is only one way ‘to learn or access the world’ and that it is ‘very old fashioned to think that there is a right way of the brain working and all the other ways are wrong or something out of the norm’ (p. 36). They felt that being ‘forced to live in a neurotypical way’ (p. 137) underpinned many of the difficulties that they experienced and that a more inclusive approach would be to recognise and support divergence from an assumed norm, instead of labelling them as disordered for failing to meet normative expectations.
Autistic participants specifically outlined how pathologisation and stigma underpinned a strong dislike of the term ‘Aspergers Syndrome’. It is worth noting that across autistic participants there were 124 references to Hans Aspergers links to Nazism (see Czech, 2018) in relation to finding the term ‘Aspergers syndrome’ offensive. Many autistic participants chose not to use this term due to the associations with Nazism, and referenced the label being used to ‘divide’ autistic people and create a ‘hierarchy’, reinforcing ableist norms about who was seen as a worthwhile member of society, and who was not.
Overall, a desire to not be pathologised and othered was a crucial factor in personal terminology preferences, regardless of language choice (i.e., whether people preferred person-first or IFL).
Theme 2: How we Talk About us
Theme 2 highlighted the varied reasons that participants personally held for their own preferences, and how they felt about group-level preferences among other neurodivergent members of their shared communities.
Visceral Responses
Participants highlighted how preferences for terminology are often driven by how the terms themselves made them feel. A large number of people wrote about disliking terms because they sound ‘odd’ or ‘euphemistic’. Euphemistic language in particular was thought to be ‘completely ridiculous’ (p. 131), with one participant comparing the term ‘person with attention differences’ to ‘calling short people “vertically challenged”.’ (p. 131).
Others said that they judged a term based on how much it caused a ‘visceral response’ (p. 49) and made them ‘bristle’ or their ‘skin crawl’. Several people noted not liking ‘the sound’ of a particular word, though this was often due to the association the participant felt it had to other terms. For example, participants said that the term ‘Aspergic’ sounded like ‘a lung disease’ and ‘allergic’, and that ‘Dyscalculic’ ‘sounds like alcoholic’. Additionally, participants highlighted how particular terms felt like, or sounded similar to offensive language, for example, ‘touretter feels very much like a slur’ (p. 453) and ‘really don’t like “dyspraxic” think it's similar to spastic’ (p. 645), which made them feel uncomfortable hearing it, or using it themselves.
Many people also expressed a particular dislike for what they felt were ‘twee’ terms, for example finding the term ‘ADHDer’ ‘childish’, or ‘gimmicky’. Likewise, the term ‘Aspie’ was viewed as ‘trivialising, cutesy’ and ‘dismissive’, and the term ‘phenomena’ (with relation to demand avoidance phenomena) was suggestive of ‘some mystical fairy thing’ (p. 2) with one participant stating: ‘I’m not the Northern Lights’ (p. 20). These comments suggest that some of the visceral dislike of terminology is linked to its use in othering, and how it can be used by out-group members to minimise the difficulties they face. Indeed, many expressed a preference for direct, factual terms to be used because ‘adding a load of unnecessary words doesn’t change the facts’ (p. 840).
Asserting and respecting agency
Chosen and preferred terminology was seen as a way to assert agency and to push back against the injustice and ableism outlined in theme 1. Many participants actively acknowledged inconsistent and dissenting views within their own communities, particularly around the use of person first vs. identity first language (see theme 2.3). There was a strong sense that this variation among community members was to be expected and respected: I prefer identity-first language over person-first language, (the idea that you need to be reminded of my personhood feels insulting) but I don't mind what others choose for themselves, though I prefer non-autistic people and/or people referring to autistic people as a group to use identity-first language. (p. 336)
Participants highlighted that they might not personally ‘be offended by the way that a person chooses to describe themselves’ (p. 620) but likewise that they would ‘never want that word applied to me’ (p. 335). There was an acknowledgement that ‘some people get really passionate about this’ (p. 175), but some participants found this frustrating, citing that there were bigger issues for communities to worry about: ‘Yes, I prefer Identity-first, but with all the shit going on in the world, to create melodrama around wording is unforgivable’ (p. 22). Similarly, participants highlighted how the shifting discussions around language could lead to demonisation of community members, for example, autistic people avoiding the term ‘Asperger syndrome’ to ‘avoid conflict’ with other community members who might accuse them of being a Nazi sympathiser. However other participants acknowledged that this was the language some people had previously been given to understand themselves and that it might be hard for some to move away from it: ‘I have some compassion for people who identify that way [Aspergers]: I'd hate to be told that the word Autistic – which changed my life – is actually a bad word’ (p. 575).
In addition to respecting the agency of other community members, preferred terminology was seen as a way to assert agency in the face of hermeneutical injustice. The acceptability of a particular term was not just influenced purely by the intention of the user (theme 2.3) but who the user was. Participants highlighted that whilst many terms were ok to be used by in-group members, this was not the case for out-group members, for example, ‘ADHDer is an in-group term. I would use it and describe my friends with it, but I wouldn't want neurotypicals to use it?’ (p. 326). Participants felt like ‘the offensiveness varies significantly based on who is using the term, in what venue, and why’ (p. 330), and acknowledged that there were terms they liked that could be used in a ‘mocking or pejorative’ way (e.g., the use of ‘autist’ by ‘alt-right communities’). Their comments suggested that whilst it was ok for in-group members to favour different terms, consensus-based community preferences should be respected by out-group members. This was felt particularly strongly by those who had experienced being ‘corrected’ (e.g., told to use person-first language) by parents or educators who were not themselves neurodivergent. Participants felt that ‘softening the language’ was used to make ‘neurotypical people feel more comfortable’ or ‘spare their feelings’ and that this should not be the aim of shifting terminology. Overall when it came to how others spoke about them, our participants highlighted that the offensiveness of particular terms or phrases was heavily interwoven with ‘context or intention’. Participants also highlighted how ‘proper’ (consensus-based preferences) could be used to perform inclusivity without holding good intentions: Not fussy at people who have good attitude but use language they didn't know was currently seen as ‘outdated’ etc. Good people don't mind altering language once they know it causes offence and twats can hide behind ‘proper’ use of language whilst spewing forth prejudice with a smile. (p. 146)
Whilst there have been heated recent discussions within the academic literature as to the use of particular terminology (see Natri et al. 2023), the comments here highlight how important it is to understand why people tend to hold strong preferences. Language can be used in a hollow and performative manner, whereas shifts in understanding are more meaningful and impactful.
Person versus identity first debate
In the open text comments, there was disagreement between many participants as to whether they preferred person first, or identity first language, however the reasons given by both groups tended to hinge on their perception of their own identity and the respectfulness of the language used. Many people who preferred identity first language viewed their neurodivergence as an ‘integral’ part of themselves and their ‘identity’ and saw it as something that could not ‘be removed’. These participants described feeling like their neurodivergence impacts on how they ‘see the world’ and that it is not an ‘accessory’. This was true across multiple groups, including those for whom the link between terminology and identity has not been previously explored: ADHD is part of my identity and experience of the world, not something separate to me’. (p. 199) ‘It focuses on my identity and gives me power, while saying a person with dcd says behind this condition, I am a normal person’. (p. 605) ‘Everything I do is influenced by dyspraxia and it is a part of me with undefined edges’. (633)
There was a sense that PFL could be ‘clinical’ and ‘dismissive’, and ironically that it could reduce a person to their diagnosis, suggesting that it was the ‘only notable thing about them’ (p. 70).
However, those who preferred PFL expressed disliking being defined ‘as a label’ and stated that they are ‘a person first … before considering any attributes like skin colour, sex or disability, even if those attributes affect every aspect of my life’ (p. 849). Participants advocated for their opinions being respected, even if it differed from the general consensus. Autistic participants (for whom previous research has shown a strong community level preference for IFL) wrote about how harmful it could be for their individual preferences to be dismissed because of community-level preferences: I hate identity first language and being told I must be a self-hater or brainwashed by my parents because I prefer person first. Autism isn't all of me. I'm so much more (a partner, a friend, a dad) and identity first has become such an ideology in the community it tries to make autism the defining feature of me. It's not. I define me (p. 658)
Importantly, the underlying reasons regardless of person first or identity first preference tended to be a dislike of being ‘pathologized’ by others. Some participants found the notion of PFL as dehumanising ‘unconvincing’, but others strongly felt that others shouldn’t have to be reminded of their humanity through the use of person-first terms. Overall our participants wanted to be respected for who they were and not made to feel lesser than other people, even where they felt significantly ‘disadvantaged’ by, or ‘bitter’ about, their neurodivergence.
Feeling disabled
Interestingly, we found variations with regards to how comfortable participants felt identifying with the ‘disability’ label that tended to cluster across groups. There was a general consensus among autistic and ADHD participants that they identified as ‘disabled’ and found the label useful to describe their experiences. Participants in these groups explicitly described finding terminology such as ‘differences’ unhelpful compared to the term ‘disability’: [Condition] is yet another way to water down the idea that it's [autism] a disability and basically give our rights away. (p. 133) ‘person with attention differences’ completely underplays the very real disability that my ADHD causes me. (p. 348)
However, there was more variation across participants with a diagnosis of dyspraxia, dyslexia and dyscalculia. Some expressed finding disability-focussed language helpful, stating that the term difficulty ‘makes it seem like disability is a bad word’ (p. 463), or ‘makes it sound like I’m just not trying hard enough’ (p. 480). Participants highlighted how they had experienced significant barriers or felt they had been ‘prevented from achieving certain things’ (p. 22) and as such identified with a disability label. However, a larger number of participants from these stated that they did not view dyslexia, dyspraxia and dyscalculia ‘as a disability’. For some people this was because they did not ‘feel disabled’ by their diagnosis, however others questioned whether the label of disability properly represented ‘what it's truly like to think different to other people and process the world differently’ (p. 515).
These variations suggest that the acceptance of disability-related terminology among neurodivergent people may be controversial, but that the reasons for this are not straightforward, that is, driven by internalised ableism with regards to distancing oneself from a disability label. However, internalised ableism was also explicitly noted as a factor in a dislike of disability terminology: Having been 6 when I was diagnosed with one disability, I hate that particular word as it was used against me and something that seemed to mean I wouldn't amount to anything. If I am going to use anything I prefer learning differences, because I can still learn to the best of my abilities, just maybe in a different way to others. (p. 247)
Some participants felt that they would not be justified in using disability terminology as they didn’t feel that they had experienced being disadvantaged by their neurodivergence. These comments have implications for how we consider the relationship between disability studies/activism and the neurodiversity paradigm.
Discussion
The aim of this study was to examine terminology preferences among people in the UK who are developmentally neurodivergent, using a mixed methods approach to establish terminology valence and the underpinning justification for likeability and offense ratings. To our knowledge, this is the first study to explore terminology preferences alongside underpinning motivations (for a previous study on preferences among autistic, ADHD and SLD participants see Nah and Lim, 2025) among neurodivergent people more broadly (i.e., beyond autistic people alone) and thus can act as guidance to researchers and practitioners working with a range of neurodivergent populations.
PFL Versus Identify-First Language
We replicated a common preference for IFL among autistic people (see Bury et al., 2023; Keating et al., 2023a, 2023b; Kenny et al., 2016) in the current study. Moreover an IFL preference was found across the majority of the other diagnoses (seven of nine, with Tourette's and stuttering the exception) included in the paired samples t-test, despite some of the individual IFL terms being ranked as less likeable and more offensive when drilling down into the individual group rankings (i.e., ‘Aspergic’, where the lower rating was driven by distancing from the ‘Asperger’ label among participants, and not a general IFL vs. PFL preference). Qualitative data suggested that many participants found PFL cumbersome, which is consistent with arguments seen in the broader disability terminology literature (Erin E. Andrews et al., 2022a, 2022b). Terminology like ‘autistic’ or ‘dyslexic’ were viewed as factually accurate and concise. However, when examining the rank likeability and offensiveness data for each diagnosis, the narrative was slightly more complicated. Consistent with some existing research, identity first terms were rated as most liked, and least offensive for autism (e.g., see Keating et al., 2023b), and dyslexia, dysgraphia and dyspraxia (Anthony et al., 2025), however for the other diagnoses ‘other’ was ranked highest. For ADHD, participants ranked ‘person with ADHD’ and ‘ADHDer’ similarly in terms of likeability and offensiveness, and person with attention differences as least likeable/most offensive. These rankings were explained in the qualitative data as representing a lack of community informed, accurate terminology to describe being diagnosed with ADHD. IFL was seen as awkward and grammatically incorrect, and the term ADHD in general was seen as not representative of the core challenges (and strengths) that participants experienced. Similar results were found for PDA, SPD, and Tourette syndrome, where overall findings were driven by inadequate existing terminology, rather than strong preferences for any of the terms. Participants suggested that existing terminology is inadequate and does not accurately capture their experiences, which reflects the presence of hermeneutical injustice (Fricker, 2007) in the conceptualisation of developmental neurodivergence. Though the importance of community participation and lived experience is gaining more traction within research and practice (Pellicano, 2020; Sonuga-Barke et al., 2024), it is crucial that future discussions over terminology and the updating of diagnoses include neurodivergent people themselves. Overall, these findings suggest that broad IFL vs. PFL preferences may not always necessarily represent the nuanced views people have of individual terms within these categories, and that a more stratified approach may be useful. However, we would caution against throwing the baby out with the bathwater, especially when it comes to more established IFL preferences (i.e., autistic, as replicated here).
An additional interesting discussion of IFL and PFL preferences were present in the qualitative data. Many of the participants across groups saw their diagnosis as central to their identity, extending previous findings from autistic people (Botha et al., 2022; Bury et al., 2023; Cooper et al., 2021). Whilst the historical use of PFL was argued to promote a humanising approach (Andrews et al., 2022a, 2022b), many participants felt that it is misaligned with how neurodivergence is currently framed (e.g., something that leads to tangible differences in ways of processing information and thinking). This framing may reflect the use of strategic essentialism, that is, the positive use of essentialised biomedical features (e.g., neurological differences) to create in-group identity and community connectedness (Ellis, 2023). Interestingly, those who expressed a preference for PFL cited the multifaceted nature of identity as a key factor in their choice. They highlighted how the use of IFL can foreground their neurodivergence as their defining feature (Botha et al., 2022), which they found to be reductionist. These strong preferences were clear within the discussion of community tensions around IFL vs PFL usage across groups. Some of the PFL proponents wrote about being accused of internalised ableism (Brown & Leigh, 2020) because of their preference, and some of the IFL proponents specifically mentioned the importance of respecting individual preferences from other community members. These tensions highlight how academic practices (i.e., debates around language use, see Natri et al., 2023; Singer et al., 2023) can have unintentional consequences for community members. Academic debates about humanising approaches filter out into communities, and individual community members become stigmatised for using the ‘wrong’ terminology. Here, individuals are effectively held to account for systemic issues over which they have very little individual control (like the continued dehumanisation of neurodivergent people in the academic and public sphere), and become marginalised from their own communities as well as broader society.
The participant comments around IFL vs PFL raise a little considered issue in the discussions of terminology preference: Motivation. Our participants highlighted how the identity, and the motivations of the user were crucial as to how offensive terminology could be. The preferences of other in-group members (i.e., other neurodivergent people) were viewed as something to be respected, but participants felt that out-group members (e.g., non-neurodivergent researchers) should stick to group-level community preferences when making general statements. Their comments emphasised that at the heart of it, terminology discussions, particularly in an academic setting, are not about language at all, but the lingering dehumanisation of people considered ‘disordered’ or ‘abnormal’ (Peruzzo, 2020). Terminology would not matter if actions were not shaped by the way we speak about stigmatised groups (Botha et al., 2020; Bottema-Beutel et al., 2020). Yet terminology does shape action: The language we use in academic settings filters out into clinical practice, and government policy, and shapes how society treats neurodivergent people (Hall, 1997; Proctor, 1995; Rose & Vivian, 2020). Language reflects dominant norms of the time; words like disorder reflect ways of thinking, and it is the wider conceptual categorisation and systematic exclusion of people from shaping knowledge about themselves that is the key issue, not simply the words people use.
Disability identity
Interestingly, participants also had quite diverging views on whether they considered themselves disabled. While many of the ADHD and autistic participants specifically noted the utility of a disability identity (e.g., access to reasonable adjustments), there was more variation among the dyslexic, dyspraxic and dyscalculic participants. These differences may reflect the way that certain forms of developmental neurodivergence are categorised, that is, the label of a specific learning difficulty vs. a global difference. Recent research has demonstrated that distancing from a disability label may be more common among dyslexic people (Anthony et al., 2025; Wissell et al., 2025), who may view themselves as less disabled once adjustments are implemented. However, the variation in viewpoints here also likely represent the heterogenous nature of neurodivergence; many dyslexic people experience co-occurring difficulties, and this may feed into whether someone considers themselves disabled (i.e., some of our participants talked about feeling more disabled by some aspects of their neurodivergence than others). This is an area that future research may want to explore.
It is also possible that distancing oneself from a label of disability reflects internalised ableism, whether that be stigma about what it means to be disabled (Brown & Leigh, 2020), or a skewed view of what counts as ‘disabled’ (see Bantjes et al., 2015 for a discussion on perceptions of a hierarchy of disability). This was certainly reflected in some of the comments from participants who said that a label of disability for them was associated with being viewed as lesser. The impact of internalised ableism can mean not just distancing oneself from a label, but also from potential community support and shared meaning making (Han et al., 2023).
Viscerality
The visceral dislike participants took to particular terms is a novel and interesting finding. It has long been noted that neurodivergent people can both use and experience language differently: Autistic people for example are often more predisposed to engage with the sensorial aspects of words (Williams & Benge, 2024). It is possible that participants are especially alert to the sound associations of these terms, causing a radical dislike. It is also possible that these aversions – framed by associations to existing medicalised and stigmatising terms – reflect a deeper dissatisfaction with the pathologisation of the medical model.
Strengths and limitations
The mixed methods nature of our study is a significant strength, as the qualitative data contextualises the quantitative, providing additional detail to participants’ terminology preferences. Ours is also the first study to our knowledge to examine language preferences in a heterogenous neurodivergent sample, going beyond autism alone. However, there are some limitations to this work. Though we had a large proportion of autistic participants, other groups were much smaller. Our sample was also majority female and white, and we only recruited participants from the UK. Despite the diversity of views within this study, it may not represent the true diversity seen within the wider population; it is possible that our recruitment avenues (i.e., primarily online, and skewed towards those engaged in neurodivergent communities) may have impacted our findings. Future work may want to focus on recruiting from a more diverse pool of people to examine whether preferences shift depending on factors such community connectedness, or level of knowledge regarding one's own particular diagnoses.
Conclusions
Our study is the first to examine neurodivergent language and terminology preferences alongside their underpinning motivations among the wider neurodivergent community. Our heterogenous findings highlight that language is a symptom, not a cure. Focusing on words rather than actions can obscure the real issue, which is a need for more affirming practice and epistemic humility when working with neurodivergent people. Overall, the mixed findings emphasise that there is no single right answer for taking a humanising and respectful approach with neurodivergent people: Actions speak louder than words. We recommend listening to neurodivergent people about their preferences and integrating these into your practice alongside a more affirming approach.
Supplemental Material
sj-docx-1-ndy-10.1177_27546330261428235 - Supplemental material for ‘It's like calling short people vertically challenged’: Language and terminology preferences among neurodivergent adults in the United Kingdom
Supplemental material, sj-docx-1-ndy-10.1177_27546330261428235 for ‘It's like calling short people vertically challenged’: Language and terminology preferences among neurodivergent adults in the United Kingdom by Amy Pearson, Aimee Grant, Jennifer Leigh, Stephen J Macdonald, Kathryn Williams, Gemma Williams, Elliott Spaeth, Kieran Rose, Ann Memmott and Monique Botha in Neurodiversity
Footnotes
Acknowledgments
The authors would like to thank all of the people who gave their time to taking part in this study
ORCID iDs
Ethical Approval
This study received ethical approval from the University of Sunderland (Reference 010358).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data for this project is not freely available.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.