
Abstract
Autistic people experience elevated rates of mental health conditions compared to non-autistic people; however, significant barriers to services are encountered. This study reports on the problems autistic people experience when accessing, or trying to access, mental health services in Australia. This report also highlights what would support improvements or solutions to these problems. Open-text responses by 539 participants (including 250 autistic people) were collected via an online survey. Every participant's response was read and coded using content analysis. The most frequently reported problems were a lack of skilled therapists and therapists who understood autism. Respondents identified training needs about autism, more neurodivergent professionals, and increased funding as factors necessary to reduce the problems. An exploratory analysis examining responses through an intersectional lens (specifically autistic people who identify as women, LGBTQIA+, low socioeconomic status, older, or living in regional/remote areas) suggests differing perspectives and experiences. While overlapping identities were not analysed cumulatively, the findings offer a foundational view to guide future, more granular inquiry to improve mental health service experiences for autistic people.
Lay Abstract
Many autistic people will experience mental health challenges, such as anxiety or depression. Sometimes these challenges can become significant enough that support is needed from a mental health professional. In this study, we wanted to find out what experiences autistic people have when they seek help from a mental healthcare professional or a mental health service. We also wanted to know what can be done to improve these experiences. We received responses from 539 people. Nearly half were autistic people, others were parents/caregivers/family, and allied health, medical or mental healthcare professionals. The most common problem reported was difficulty finding therapists who are skilled or who understand autism. Many people suggested that mental health professionals need more training about autism, and that better funding is needed to help autistic people access appropriate support. We know that not all autistic people have the same experience. So, we went on to look at the data more closely to see how experiences differed based on factors such as gender or age. This analysis showed that different groups can face different barriers or challenges. These findings suggest that more research is needed to better understand the needs of specific groups and to improve mental health services for all autistic people.
Introduction
There is a wealth of evidence describing the elevated prevalence of mental health conditions in autistic people across the lifespan. Anxiety is diagnosed in 42% of autistic children and 28% of adults, and depression in 14% of autistic children and 33% of adults (Micai et al., 2023). These rates far exceed general population estimates of 6.5% for child anxiety and 2.6% for child depression and remain elevated in population-based studies that control for referral bias (Mutluer et al., 2022; Polanczyk et al., 2015; Steel et al., 2014). Mental health challenges have a significant impact on the lives of autistic people, with increased levels negatively influencing quality of life (Adams et al., 2019, 2020; Lawson et al., 2020), social experiences (Ambrose et al., 2021; Rhodes et al., 2023), and education and employment outcomes (Adams, 2022; Ambrose et al., 2024; Southey et al., 2024). This paper adopts a neurodiversity-informed, social-contextual perspective, recognising that these challenges are not solely intrinsic but are shaped by environmental barriers, stigma, and lack of support.
Despite the recognised elevated prevalence of these challenges, autistic people report unmet healthcare needs for their mental health (Nicolaidis et al., 2013). Multiple systematic reviews have identified potential barriers to autistic people receiving mental healthcare. Adams and Young (2021) reviewed nine studies (k = 3 quantitative, k = 6 qualitative), six of which were based upon autistic adults’ self-reports and three on parental reports. The most frequently reported barriers to access from these were the professionals' poor knowledge of autism and/or ability to tailor their approach to support autistic clients, long waiting lists, lacking access know-how or confidence to access the services, costing issues, and not fitting into services/being bounced between services. Brede et al.'s (2022) review identified 38 studies, 24 of which reported first-person accounts from autistic adults, 10 from family members, and 13 from professionals. Their meta-synthesis identified three superordinate analytical themes describing service and therapist level difficulties/barriers in accessing support, impacts of being autistic on treatment and needs for a flexible and comprehensive approach, and the importance of relationships and autistic lived experience. However, Brede et al. noted that the vast majority (33 out of 38; 87%) of their included studies were from the United Kingdom (UK) or the United States of America (USA). As health systems and policies, as well as funding models for healthcare and support for autistic individuals, differ between countries (Cacace et al., 2013; Rees & Long, 2021), further work is needed. This would help identify common challenges faced by autistic individuals across diverse contexts and issues that may be related to specific healthcare systems or policy environments.
Mental healthcare services exist within a complex, multilayered system that can be conceptualised using Bronfenbrenner's ecological systems theory (Bronfenbrenner, 1979). This highlights how individuals, their health and well-being are influenced by multiple, nested levels of the environment. These levels include the microsystem (directly interacting with the autistic person, such as their family or clinicians) to the macrosystem (e.g., cultural values and policies). Factors impacting access to such services may be proximal or distal to the autistic person and may exist within a single layer or across multiple layers of the system. Therefore, to meaningfully understand factors influencing service experiences, it is essential to gather perspectives of multiple informants from across different levels of the system. Only 21% of the studies in Brede et al.'s (2022) review reported on the perspectives of multiple respondents, and only one included autistic people, family members, and mental health professionals. However, as Brede et al. synthesised the findings of all informants into a single analysis, similarities or differences in perspectives from people from different levels of the system cannot be inferred. Adams and Young (2021) only included studies from autistic people and/or their family members; therefore did not report on the perspectives of mental healthcare professionals. To identify effective pathways to reduce barriers to access, consideration must be paid to both barriers identified across the system and those uniquely experienced by people in different roles. To have maximum impact on service development with sensitivity to structural constraints, such work should also ask about positive experiences, highlighting examples of good practice and opportunities for improvement.
Exploring Mental Healthcare Experiences Through an Intersectional Lens
Research literature around autistic people's mental health and experiences of mental health services shows there is a need to consider additional factors associated with health inequities experienced by autistic people. Such factors impact, influence, intersect, and/or interact with experiences of an autistic person to influence their healthcare. There needs to be a recognition of autistic diversity and personal identity, including race, ethnicity, gender, sexuality, age, ability, and socioeconomic status (SES). Applying an intersectional lens emphasises these dimensions, and how they intersect and impact the experiences of autistic people (and/or their supporters; Lopez et al., 2022). Exploring data from the nexus of autistic people's identities informs responsive policy, research, and supports (Malone et al., 2022).
Reviews of intersectionality research with non-autistic people highlight how ‘multiply marginalised’ identities experience increased inequities from mental health services above those who are not ‘multiply marginalised’ (Fagrell et al., 2019; Vargas et al., 2020). They report accessing care difficulties, unmet health needs and unsatisfactory treatment responses. Qualitative studies highlight how a person's social identities are important in therapy and how provider knowledge of experiences by minority communities strengthens therapeutic relationships (Hempeler et al., 2024). Sadly, they also highlight microaggressions and microinvalidations, described as ‘testimonial injustice’; a form of discrimination in which a person's credibility is downgraded by negative stereotypes about identity. As per the Minority Stress Model, macro- and microaggressions (i.e., stressors) associated with membership of marginalised groups create disparities in mental and physical wellness due to chronic stress derived from societal stigmatisation and discrimination (Meyer, 2003). Concerningly, this suggests services intended to support mental health may, for some, exacerbate distress. Applying the minority stress model to understand stigma-related stressors’ contribution to mental health and well-being in autistic people shows autistic people experience an added stress burden through multiple minority stressors, including victimisation and discrimination, everyday discrimination, expectation of rejection, and outness (Botha & Frost, 2020; see also in-depth review by Botha & Gillespie-Lynch, 2022). This, therefore, highlights the importance of exploring experiences of mental services through an intersectional lens.
The limited existing research exploring mental health experiences of autistic people through an intersectional lens highlights the importance of this work. For example, a survey of 627 autistic adults or parents of autistic adults in the USA shows that Black autistic adults have poorer service access relative to white autistic adults (Schott et al., 2021). Using USA Medicare extracted data on 117,848 autistic children, Bilaver et al. (2021) found that Black, Asian, and Latinx children also receive fewer outpatient services for mental health relative to White children. In relation to gender, both women and other gender autistic adults report multiple barriers to receiving needed services in the USA as compared to autistic males (Miller et al., 2022). The intersection of autism and LGBTQIA+ identity is also associated with greater disparities in unmet healthcare needs based on USA data from 62 LGBTQIA+ adults and 58 straight/cisgender adults (Wallisch et al., 2023).
Summary
Autistic people experience significantly elevated prevalence of mental health disorders, but also elevated levels of unmet service need with multiple barriers to accessing care. According to Mandy (2022), we have a ‘mental health crisis’. Although some work has sought to understand the experiences of autistic people accessing mental health services (e.g., Brede et al., 2022), this has predominantly been undertaken in the UK and North America and rarely included informants from across the system. Work to date has focused upon barriers experienced, without consideration of solutions to those barriers, nor the positive factors that are working well; such information is important to consider if positive changes are to be made. For maximum benefit to autistic people, it is important to consider how intersectionality may influence the mental healthcare experiences of autistic people. This study was designed to answer the following research questions:
What are the problems identified by the autistic and autism community:
When accessing mental healthcare services in Australia? What factors are causing these problems? What factors could prevent or reduce these problems? What things are working well in relation to mental healthcare services? Do these vary when they are explored by specific individual intersectional identities (e.g., gender, race, and SES)?
Method
This paper reports on data collected as part of a larger landscape mapping project covering multiple service domains, one of which was mental health services (Adams et al., 2023). The project was reviewed by Griffith University Human Research Ethics Committee (reference 2023/121). Informed consent was obtained from all participants prior to their involvement in the online survey. Participants were informed about the voluntary nature of participation, the ability to withdraw at any time, and how their data would be stored and used. Participants were also provided with contact details for mental health support services, including text, voice, and chat helplines, before beginning the survey. They were encouraged to contact these services should they experience distress during or after survey completion.
This study adopts a constructivist interpretivist epistemological approach, focused on understanding different stakeholders’ experiences of barriers and facilitators within mental health service systems. This approach values lived experience and allows engagement with the complexity and nuance of each person's individual experiences, therefore supporting the exploration of intersectionality and its impact on experiences.
Data were collected from 6 March to 5 May 2023; data collection ended due to time constraints of the funding. All survey data were stored securely. Trained coders only had access to anonymised written answers for the specific questions they were coding; they did not have access to any demographic data. Only participants who responded to one or more questions relating to mental health services were included in this study.
Community Involvement and Research Positionality
This project team includes autistic and otherwise neurodivergent authors and researchers who contributed to the study design, survey design, data collection, data coding, data analysis, and write-up. In addition, through AutismCRC, autistic people helped to shape and improve the survey and reporting of results.
The authors and research team reflect diversity in relation to gender, age, ethnicity, sexuality, SES, and experience with mental health services. All team members have completed education beyond compulsory schooling. Some members of our team identify as mental health clinicians, allied health practitioners, and family members of autistic people.
Participants
A volunteer sample of participants was recruited through social media, author and collaborator networks, and community organisations in Australia. A total of 539 participants from Australia stated they wanted to answer the questions on mental health services and provided answers at least to the first survey question on mental health services. This included 250 autistic people, 327 family members or carers of autistic people, 75 mental health professionals, and 130 medical or allied health professionals. People could identify with multiple roles, hence the total number across roles exceeds 539. Of the 539 participants in this study, 161 selected two roles from the above and 49 people selected three or four roles. Figure 1 shows the proportion of participants identifying with each role (note that some roles, such as educator, could be selected by respondents but are not reported on separately in the analysis). As expected, there is significant overlap across the intersectional identities that autistic people identified with (see Figure 2). Responses, therefore, attributed to a particular group (e.g., professionals, autistic people in regional areas) may also include individuals who are, for example, both professionals and parents, autistic themselves or autistic people who live in regional areas who are older adults. While this overlap introduces some complexity and is recognised as a limitation, this approach was chosen over asking participants to respond from a single identity. This decision was informed by our research team and community advisors, who agreed that asking individuals to separate their experiences in this way would not reflect the reality of how intersecting roles shape people's views and experiences.

Venn Diagram Showing the Percentage of Participants Who Identify With One or Multiple Respondent Roles (Note: 22 Participants Identified as Having Roles Not Represented in This Diagram, Notably Teacher, Researcher and Disability Support Worker).

Venn Diagram Showing the Percentage of Autistic Participants With Single or Overlapping Intersectional Identities.
Demographics (provided by the respondent) for the total sample and for each respondent group are provided in Tables 1 and 2. Percentages are based on the number of participants who provided a response to the question being reported on, rather than the percentage of the entire sample.
Demographics of Participants (Who Responded to at Least the First Question on the Survey).

Note. LGBTQIA+ = lesbian, gay, bisexual, transgender, queer/questioning, intersex, asexual plus; CALD = culturally or linguistically diverse; AAC = augmented or alternative communication. Percentages may not add up to 100% as some people opted not to provide demographic information.
Demographics for Autistic Respondents (Who Responded to at Least the First Open-Text Question on the Survey), Reported by Intersectional Identity.
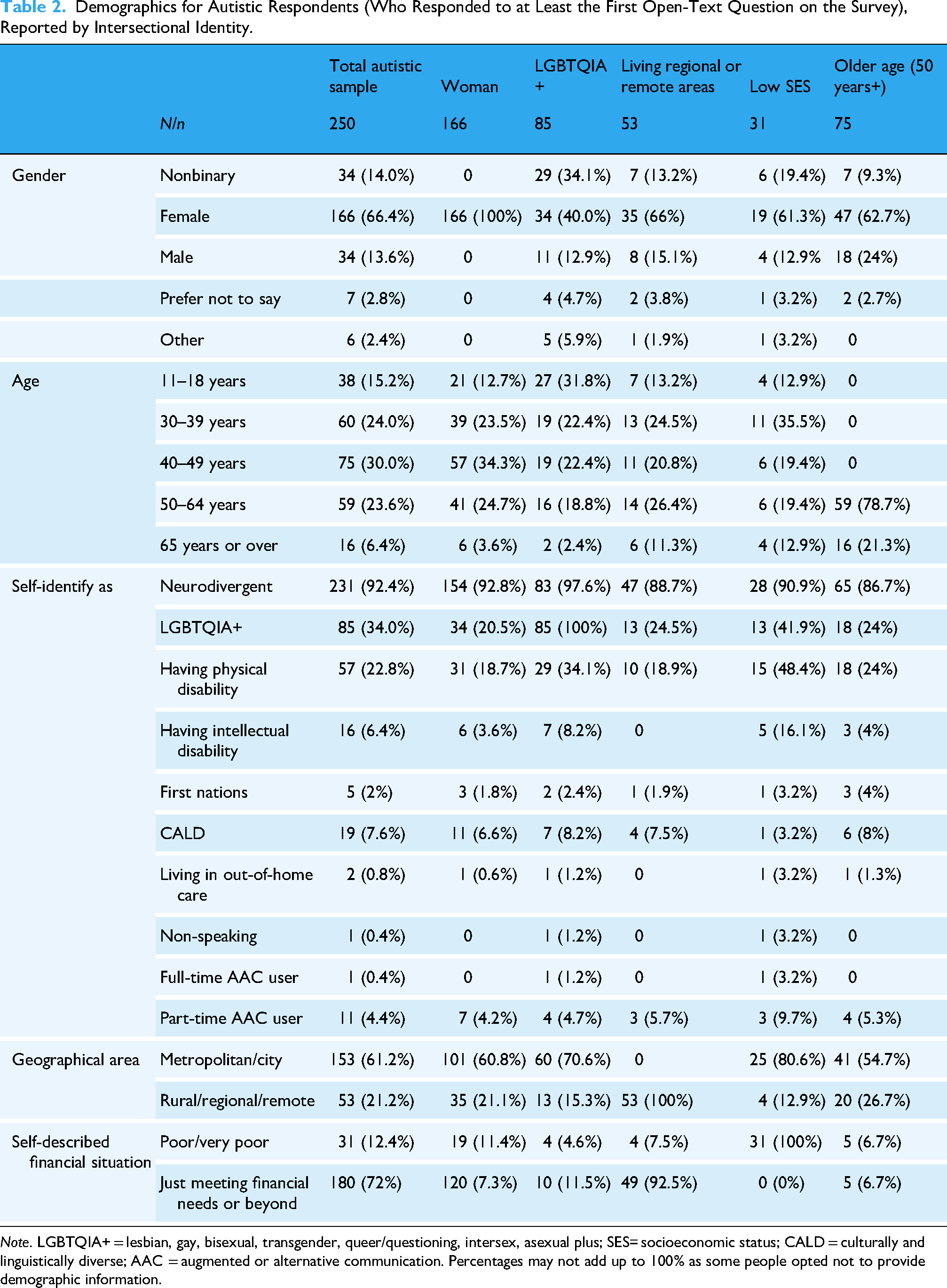
Note. LGBTQIA+ = lesbian, gay, bisexual, transgender, queer/questioning, intersex, asexual plus; SES= socioeconomic status; CALD = culturally and linguistically diverse; AAC = augmented or alternative communication. Percentages may not add up to 100% as some people opted not to provide demographic information.
Survey
The survey was co-designed for a broader project and is available in the Appendix of Adams et al. (2023). Participants followed a weblink to an online survey site (REDCap), which presented the information sheet and consent form. Participants were not reimbursed for their time completing the survey. Once participants had provided consent and basic demographics, they selected which of the eight topics (one of which was mental health services) they would like to answer questions on. For each topic selected, participants were asked four questions (wording in brackets was tailored to each topic/service domain):
What are three problems that autistic people experience when accessing (mental health) services? What do you think is causing these problems? What do you think could prevent or reduce these problems? What is working well, or has worked well, for autistic people within (mental health) services?
After each question, participants were informed they could list up to three things in response to the question or leave the text box blank. To ensure answers reflected participant views (rather than being predefined by the research team and/or their advisors), they answered each question using free text.
Every survey question had an optional information box, designed to support participant understanding. For example, the optional information available to the question ‘Do you want to answer the questions on mental health services’ stated ‘Mental health services include the professionals that provide mental health care – like psychologists, psychiatrists, mental health nurses and counsellors. It also includes things like inpatient services and support lines—like Lifeline and Beyond Blue’. Participants were not asked about whether they had tried or thought about accessing mental healthcare services for themselves or an autistic person they work with or support.
Data Analysis
Every participant's answer was read in full. If the participant provided more than three answers in response to the question, only the first three answers were coded (as per Clark & Adams, 2020). Although some overlap in responses was anticipated, the four open-ended questions were designed to capture distinct aspects of participants’ experiences (specific problems, perceived causes, potential solutions, and existing good practice) and were therefore analysed and reported separately to preserve the focus and content of each question.
All research team members undertaking coding were members of the autistic or autism community. Coding team members were predominantly autistic people or family members of autistic people. Others were researchers with backgrounds in psychology, clinical psychology, education, and allied health. The coding team remained consistent for the duration of the project. To enhance the trustworthiness of the analysis, weekly team meetings were held. This enabled peer discussion, addressed coding challenges, and ensured inter-coder agreement. They also provided space for reflexive dialogue about potential biases, and, where possible, triangulation of data sources was employed to corroborate findings.
Due to the overlapping identities of many participants (e.g., autistic individuals who were also parents or professionals), coding was conducted across the entire sample. As the results disaggregate responses by stakeholder group, it is possible to see the proportion of each respondent group reporting a response within each category. Each response was analysed using content analysis, following the four steps of Dey (1993). Content analysis was deemed most suitable for understanding the frequency of specific responses within and across participants (Arnold et al., 2023). Unlike thematic analysis, which often emphasises richly developed themes over patterns of frequency, inductive content analysis allows for the systematic quantification of responses. This was important given our intention to identify points of convergence and divergence across groups, including the frequency with which issues were raised. Frequency was not treated as a proxy for importance, but rather as one indicator of shared experience or systemic patterns. Less frequently mentioned barriers may still reflect significant barriers to access, especially for the most marginalised groups.
Coding was undertaken in two stages. Initial codes were developed inductively from the first 250 responses, allowing responses and codes to be generated based on responses given by the community. The inductively derived codes were reviewed and refined through discussion among the authors, with adjustments made for clarity. The resulting inductively derived coding framework was then applied to deductively code the remaining responses. However, any data that did not align with the existing codes were analysed inductively, with new codes developed as needed to ensure the full range of community responses was reflected in the codes. Final codes were agreed upon through team discussion and applied across the dataset.
Responses were transferred to SPSS for analysis, with each participant marked as either having mentioned (1) or not (0) each category, regardless of how many comments were made within it. Frequencies were calculated for (a) the full sample and (b) each respondent group (noting overlapping identities, e.g., autistic and parent). Categories mentioned by ≥10% of the total sample were retained. The data are explored descriptively; comparisons are not made between the groups as (a) the aim of the paper is to explore, not compare, perspectives; and (b) the groups are not independent of each other (i.e., an autistic person may also be a parent). For ease of visual inspection, in the tables, the three most frequently reported categories per group are shaded in grey, and group-specific percentages differing by >5% from the total sample are bolded.
While a comprehensive intersectional analysis is beyond the scope of this paper, the second stage of the analysis involved an initial exploration of the data through an intersectional lens, focusing on a single intersecting identity. We acknowledge that many autistic individuals have multiple overlapping identities (see Figure 2 for a visual depiction of the intersecting identities). However, due to the sample size of autistic participants with each combination of each identity (see Figure 2), this paper explores responses in relation to one intersectional identity at a time. The limitations of this approach are acknowledged. This work aims to provide a foundational exploration, intended to inform and pave the way for future research, allowing more depth. Where possible, the self-reported demographic information was used to identify intersectionality. Postcode data were used to identify those in rural, regional, and remote areas (using delivery classifications from Post and The Department of Agriculture, Fisheries and Forestry). Autistic people with low SES consisted of those who self-rated themselves as being ‘poor’ or ‘very poor’ in response to the question, ‘Given your current needs and financial responsibilities, would you say that you and your family are…?’. Finally, older adults consisted of those who stated in the demographics section that they were aged 50 years and over. Where numbers suffice (n > 30), descriptive analyses using frequencies of each category were calculated for the total autistic sample and for groups of a specific intersectional identity (i.e., autistic and LGBTQIA+; autistic and older adult). Categories noted by 10% or more of the entire autistic sample, or by any group of autistic people with specific intersectional identities, were presented in the table.
Results
This section highlights the frequency with which respondents identified factors or responses in relation to the four research questions, with findings for each question presented in its own subsection. In each subsection, the first table represents the categories that were identified by 10% or of the overall sample (i.e., autistic, family members, and professionals combined). The second table presents intersectional identity data for autistic respondents only, allowing for differences between intersectional groups to be identified. For all tables, the top three responses for each group are shaded in grey, and any difference of >5% between groups is bolded and underlined.
Problems Experienced by Autistic People When Using or Accessing Mental Health Services
A total of 539 respondents opted to answer this question on the problems autistic people experience when using, or trying to access, mental health services, revealing six categories endorsed by respondents (see Table 3). Nearly a quarter of all participants identified an insufficient availability of, or access to, skilled mental healthcare professionals. A similar proportion of people report that mental healthcare professionals demonstrate a lack of understanding of autism/neurodiversity, its presentation, and its impact across the lifespan. However, patterns differ when responses are examined by a respondent group. For example, while the most frequently reported problem by professionals (mental health and medical/allied health) was the same as autistic people, their second and third most reported issues differed.
Problems Experienced by Autistic People When Using, or Trying to Access, Mental Health Services (Sorted Most to Least Frequently Reported, Based on the Entire Sample).
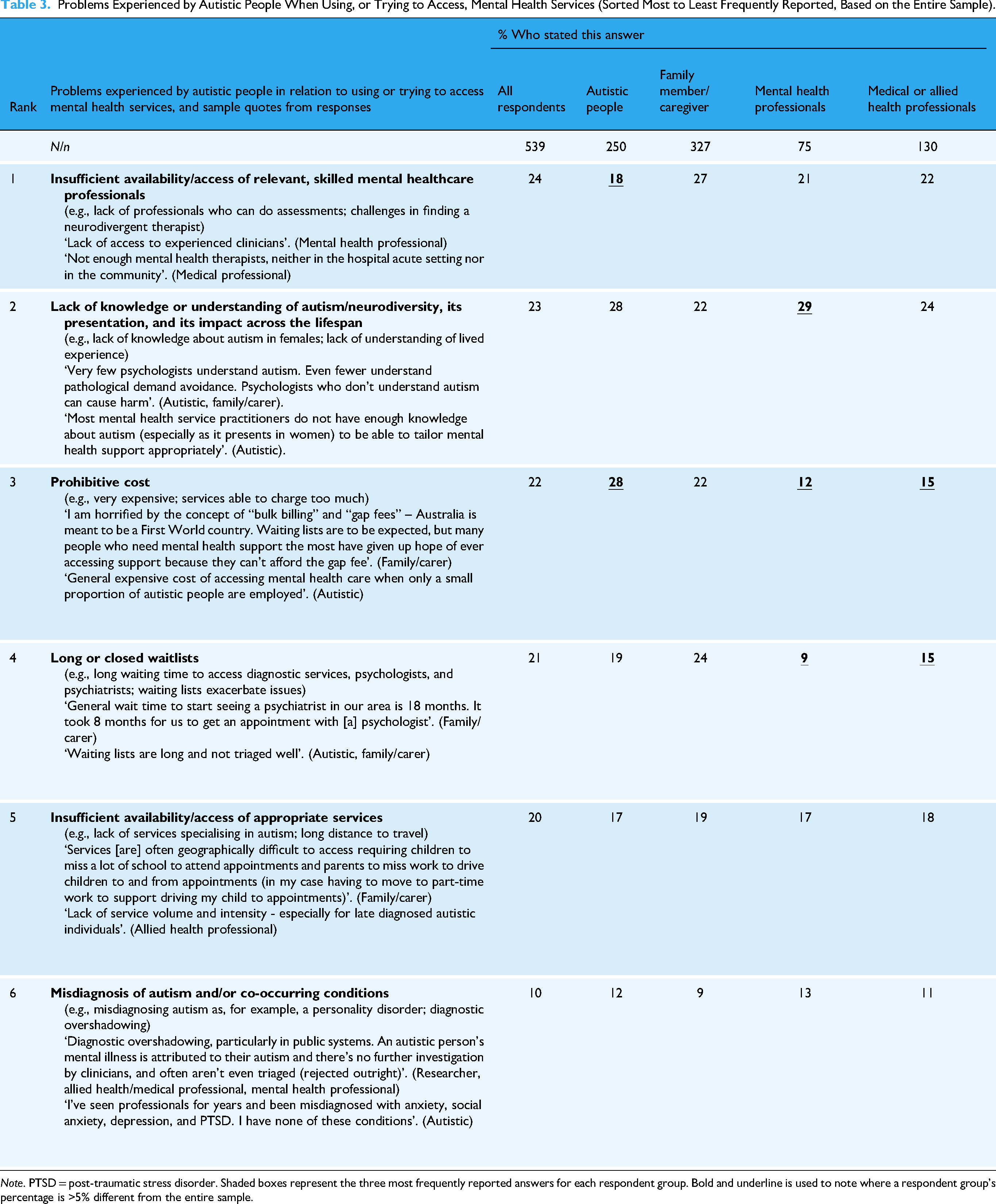
Note. PTSD = post-traumatic stress disorder. Shaded boxes represent the three most frequently reported answers for each respondent group. Bold and underline is used to note where a respondent group's percentage is >5% different from the entire sample.
An Intersectional Lens on the Problems Experienced by Autistic People When Using or Accessing Mental Health Services
Visual inspection of Table 4 indicates problems reported by autistic people with intersecting identities may differ across identities. For example, prohibitive cost is the most frequently reported problem across four of the intersectional identity groups, but not for the older age range. Another example is the problem of misdiagnosis of autism or co-occurring conditions, which was reported by 29% of autistic people with low SES, but only 5% to 14% of the other intersectional groups.
An Intersectional Exploration of the Problems Experienced by Autistic People When Using, or Accessing, Mental Health Services (Sorted Most to Least Frequently Reported, Based on the Total Autistic Sample).

Note. LGBTQIA+ = lesbian, gay, bisexual, transgender, queer/questioning, intersex, asexual plus; SES = socioeconomic status. Shaded boxes represent the top 3 for each intersectional identity. Bold and underline is used to note where the % is >5% different from the entire autistic sample. For explanation of category name, see Table 3.
Factors Causing the Problems Experienced by Autistic People When Using or Accessing Mental Health Services
A total of 452 respondents opted to answer the question regarding factors that cause the problems experienced by autistic people when using, or trying to access, mental health services, with seven categories identified (see Table 5). Some consistency was observed across respondent types, with a lack of training on autism and a lack of knowledge about autism identified as contributing factors to problems experienced by autistic people when using, or trying to access, mental health services. However, there was variability in the proportion of respondents who reported each factor. For example, the proportion reporting ‘a lack of training on autism’ ranged from 17% of the family members/caregivers to 39% of mental healthcare professionals.
Factors Leading to the Problems Experienced by Autistic People When Using, or Trying to Access, Mental Health Services (Sorted Most to Least Frequently Reported, Based on the Entire Sample).

Note. NDIS = National Disability Insurance Scheme. Shaded boxes represent the three most frequently reported answers for each respondent group. Bold and underline is used to note where a respondent group's percentage is >5% different from the entire sample.
An Intersectional Lens of the Factors Causing the Problems Experienced by Autistic People When Using or Accessing Mental Health Services
Visual inspection of Table 6 indicates that autistic people with intersecting identities may identify different factors as causing the problems with accessing or trying to access the mental healthcare system. An example of this includes 15% of autistic people living in regional or remote areas, noting professionals making assumptions about autism as a casual factor, whereas this was only noted by 4% to 11% of autistic people with other intersectional identities. The proportion of autistic people who have low SES who identified non-inclusive therapeutic skills and/or attitudes as a casual factor (32%) was notably higher than that of the other intersectional groups (13% to 24%).
An Intersectional Exploration of Factors Leading to the Problems Experienced by Autistic People When Using, or Trying to Access, Mental Health Services (Sorted Most to Least Frequently Reported, Based on the Total Autistic Sample).

Note. LGBTQIA+ = lesbian, gay, bisexual, transgender, queer/questioning, intersex, asexual plus; SES = socioeconomic status. Shaded boxes represent the three most frequently reported answers for each intersectional identity. Bold and underline is used to note where the % is >5% different from the entire autistic sample. For explanation of category name, see Table 5.
Factors Which Could Prevent or Reduce Problems Experienced by Autistic People When Using or Accessing Mental Health Services
Seven categories were constructed to summarise factors that could prevent or reduce problems experienced by autistic people (see Table 7). The most frequent factor was increased access to training on autism for mental health professionals (including learning from autistic people with lived experience), which was reported by 42% of the entire sample. This factor was typically at least twice as frequently reported than the second-rated factor, ‘more mental health professionals who are autistic’ (reported by 20% of all respondents). There were differing proportions identifying more funding and improved access to, and quality of, services across the respondent groups; for example, only 9% of autistic people but 19% of mental health professionals feel that improving access to, and quality of, services would reduce the problems autistic people experience in relation to mental health services.
Factors That Could Prevent or Reduce the Problems Experienced by Autistic People When Using, or Accessing, Mental Health Services (Sorted Most to Least Frequently Reported, Based on the Entire Sample).

Note. NDIS = National Disability Insurance Scheme. Shaded boxes represent the three most frequently reported answers for each respondent group. Bold and underline is used to note where a respondent group's percentage is >5% different from the entire sample.
An Intersectional Lens on the Factors Which Could Prevent or Reduce the Problems Experienced by Autistic People When Using, or Accessing, Mental Health Services
Visual inspection of Table 8 suggests that all intersectional groups identified increased availability of, and access to, training on autism as a factor that could prevent or reduce the problems autistic people are experiencing when accessing services. This was most frequently endorsed by respondents from low-SES situations (61%). More mental health professionals and more funding for mental health services were also commonly identified factors. There was some variability in the third-highest factor identified, with older autistic adults and autistic LGBTQIA+ people identifying different factors from the other groups.
An Intersectional Exploration of the Factors That Could Prevent or Reduce the Problems Experienced by Autistic People When Using, or Accessing, Mental Health Services (Sorted Most to Least Frequently Reported, Based on the Total Autistic Sample).

Note. LGBTQIA+ = lesbian, gay, bisexual, transgender, queer/questioning, intersex, asexual plus; SES = socioeconomic status. Shaded boxes represent the three most frequently reported answers for each intersectional identity. Bold and underline is used to note where the % is >5% different from the entire autistic sample. For explanation of category name, see Table 7.
Factors That Are Working Well, or Have Worked Well, in Relation to Autistic People Using, or Accessing, Mental Health Services
Four categories were identified as factors that are working well or have worked well (see Table 7). However, ‘nothing/not a lot’ was the most frequently endorsed response (21% of the entire sample, 25% of autistic people, and 23% of family members or caregivers). Mental health professionals and medical or allied health professionals most frequently identified finding a professional who understands autism as something that is working well or has worked well (26% and 24%, respectively). They also identified National Disability Insurance Scheme (NDIS) funding as something that is working well (21% and 22%, respectively). However, only 18% of autistic adults and 16% of parents/caregivers identified finding professionals who understand autism as something that is working well, and only 13% of each group identified NDIS funding as something that is working or has worked well (Table 9).
Things That Are Working Well, or Have Worked Well, for Autistic People When Using, or Accessing, Mental Health Services (Sorted Most to Least Frequently Reported, Based on the Entire Sample).

Note. NDIS = National Disability Insurance Scheme. Shaded boxes represent the three most frequently reported answers for each respondent group. Bold and underline is used to note where a respondent group's percentage is >5% different from the entire sample.
An Intersectional Exploration on the Factors That Are Working Well, or Have Worked Well, in Relation to Autistic People Using, or Trying to Access, Mental Health Services
Visual inspection of Table 10 suggests that, regardless of the intersectional lens, a notable proportion of autistic people stated that nothing or not a lot is working well in relation to autistic people accessing mental health services. Notably, half of those from low-SES situations said that nothing is working well. Autistic people from low-SES situations had differing response patterns from the other groups: they had lower proportions of respondents identifying that mental health services work well when you find the right professional, and when NDIS funding supports needs. These groups had higher proportions of people identifying flexible or alternative access as working well to support their access, and those from low-SES situations had over twice as many respondents as the other groups, highlighting the importance of support from family, friends, and the neurodivergent/autistic community.
An Intersectional Exploration of the Things That Are Working Well, or Have Worked Well, for Autistic People When Using, or Accessing, Mental Health Services (Sorted Most to Least Frequently Reported, Based on the Total Autistic Sample).

Note. LGBTQIA+ = lesbian, gay, bisexual, transgender, queer/questioning, intersex, asexual plus; SES = socioeconomic status; NDIS = National Disability Insurance Scheme. Shaded boxes represent the three most frequently reported answers for each intersectional identity. Bold and underline is used to note where the % is >5% different from the total autistic sample. For explanation of category name, see Table 9.
Discussion
This study reported on the problems that autistic people experience in relation to mental health services, as reported by 539 members of the autistic and autism community. It also reported on the community views with regard to factors leading to these problems, the factors that could help prevent or reduce the problems, and what is working well for autistic people in relation to mental health services. An initial exploration of viewpoints through an intersectional lens was also undertaken for those who identify as women, LGBTQIA+, living in regional or remote areas of Australia, having low-SES, or are older in age (50 years+). The key findings are discussed in turn below, but this is done with acknowledgement that the data within the tables provide further rich and informative explorations which have important implications for policy, service reform, and future research. Whilst the findings are also discussed with recognition of the importance of considering intersectionality, we also acknowledge the limitation of considering data in relation to individual rather than multiple intersecting identities.
Problems Experienced by Autistic People in Relation to Mental Health Services
Of the 539 respondents, almost one in four identified a lack of availability of/access to skilled mental healthcare professionals as a key problem experienced by autistic people in relation to mental health services. Almost one in four also identified a lack of knowledge or understanding of autism or neurodiversity as a problem. These issues align with those reported in prior reviews (Adams & Young, 2021; Brede et al., 2022), underscoring their global relevance as well as potential for wide-reaching solutions.
The sample size and use of content analysis allowed for exploration of factors, such as respondent type, that may influence the problems reported. Notably, autistic people and family members reported cost and long waiting lists as significant issues more frequently than mental healthcare professionals, which mirrors prior research (Camm-Crosbie et al., 2019). Long waiting times are associated with multiple negative outcomes, including an increase in mental health symptom severity and risk of dropout from treatment, as well as decreased engagement and likelihood of improvement in treatment (see Peipert et al., 2023). The suggestion of differences in perspective between autistic adults/family members, and mental health professionals may reflect the fact that these informants are situated within different elements of the system. Barriers or problems may be prominent within specific elements of the system, for example, mental health professionals are unlikely to see the impact of cost as much as the person paying for the support. Alternatively, it could reflect differences in perception of these elements as a ‘problem’. Delineating some of the reasons for the differences between informant group perspectives will be useful to address and reduce the impact of these problems on service use and access.
Factors That Lead to, or Reduce, the Problems Experienced by Autistic People in Relation to Mental Health Services
There was a clear and consistent message across most respondent groups: the lack of knowledge or training in autism and/or neurodiversity, its presentation, and impact is leading to the problems autistic people experience in relation to mental healthcare services. Increasing access to this training is the most frequently identified factor that could prevent or reduce the problems listed. In a study by Mazurek et al. (2023), when asked, ‘How important is it to you that your therapist knows a lot about autism?’, the average score on a 5-point scale (1 = not at all important to 5 = very important) from 303 autistic adults was 4.48. Mazurek et al. suggest this reflects how much autism knowledge of therapists underpins autistic people being able to feel heard, accepted, and validated, noting this was ‘central to therapeutic success’. Mental healthcare professionals report limited knowledge of autism and autism-specific mental healthcare, leading to one in three indicating they are not open to working with autistic clients (Lipinski et al., 2022). Increasing the level of autism knowledge is important in enabling therapists to better understand their autistic clients and how their neurotype may be impacting their well-being, as well as enabling therapists to deliver effective supports tailored to their needs (Lipinski et al., 2019, 2022; Montazeri et al., 2020). Training in autism has been identified as an important factor in the successful delivery and adaptation of mental health interventions for autistic people (Moore et al., 2023).
However, whilst there was a clear message about the need for more knowledge and training, this response should be considered in the context of all the systemic, structural, and interpersonal barriers reported, each of which may intersect and compound one another. Systemic barriers such as funding limitations, policy constraints, and inconsistent service provision create conditions under which interpersonal barriers, such as the lack of specialised knowledge among mental health professionals, become more pronounced or impactful. For example, funding issues may impact the ability to access training, or long waiting times and high caseloads may limit the use of inclusive therapeutic skills. By exploring the issues in this way, it becomes clear that solutions must not only target individual-level factors (such as therapist training or attitudes) but must also address systemic and structural changes, including improved funding, better policies, and access to resources.
Approximately 20% of respondents identified more mental healthcare providers who specialise in autism, including those who are autistic and/or neurodivergent themselves, as a possible factor that could prevent or reduce the problems experienced by autistic people when accessing services. This aligns with the double empathy problem (Milton, 2012) or perhaps the triple empathy problem that has been suggested for healthcare settings (Shaw et al., 2023), and with Muggleton et al.'s (2022) suggestion that autistic psychologists may be well placed to intuitively align their approach with autistic clients. However, as highlighted by Jellett and Flower (2024), there are multiple systemic level barriers for autistic psychologists feeling safe to disclose their autism and to have the value of lived experience recognised. Similar reflections around stigma and safety to disclose are also present in the literature exploring other healthcare professions (e.g., doctors; Shaw et al., 2023) and those in other service domains (e.g., teachers; StEvens, 2022).
Things That Are Working Well or Have Worked Well for Autistic People in Relation to Mental Healthcare Services
Twenty percent to 25% of members of each respondent group, other than the mental healthcare professionals, said that nothing, or not a lot, is working well for autistic people in relation to mental healthcare services. This finding, for a group of people who are at elevated risk of mental health problems from early childhood and an increased risk of suicidal attempts, is concerning. The findings echo Mandy's (2022) perception of the current ‘mental health crisis’ for autistic people. Things need to change as autistic people's negative experiences with mental health services can erode trust and prevent help-seeking in the future (Brede et al., 2022). Loizou et al.'s (2024) systematic review of approaches to improving mental healthcare for autistic children and young people concluded that the quality of the evidence is low, as most studies were underpowered and lacked a comparison group.
Interestingly, there was variation across the proportion of people in each respondent group who stated that alternative/flexible access options are working well. The average across the entire sample was 10%, although the response was listed by 13% of autistic people, 6% of mental healthcare providers and only 3% of medical or allied health professionals. This disparity in proportions may suggest that the importance of having alternative and flexible access options is underestimated by providers. They may not be aware of previous work showing 62% of autistic people cite calling to make an appointment as a barrier to accessing primary healthcare, and experiencing that barrier was associated with a range of adverse health outcomes (Doherty et al., 2022). The provision of mental healthcare delivered over telehealth (‘telemental health’) was limited before the COVID-19 pandemic due to concerns amongst therapists and mental healthcare professionals (e.g., Cowan et al., 2019), but has since become commonplace, with both autistic people and therapists accepting the benefits and challenges (L. Adams et al., 2023). Although not infallible, results for mental health supports suggest equivalence, or potentially a little benefit, of telemental health over face-to-face, especially in terms of indirect costs and equity of access across geographical location (L. Adams et al., 2023).
Exploring Responses Through an Intersectional Lens
A full intersectional analysis exploring multiple identities was beyond the scope of this paper; however, given the recently recognised importance of research exploring the nexus of people's identities (Malone et al., 2022), an initial exploration of responses was undertaken through an intersectional lens. Figure 2 highlights the multiple intersectional identities within the autistic participants, thereby highlighting the complex nature of this area.
A broad pattern was noted across the four questions. There was general consistency across intersectional group responses in the most frequently reported response to each question, and some consistency across the second most frequently reported response. However, there was more variability in the responses, which were third or lower in terms of frequency reported. The importance of this tentative exploration is highlighted by multiple examples where the proportion who reported a specific problem or factor in third to lower positions is at least 1.5 times more or less that reported by the entire autistic sample; for example, 29% of people from low-SES situations report misdiagnosis of autism and/or co-occurring conditions as a problem faced by autistic people, which is more than double the proportion (12%) reported by the total autistic sample. The proportion of older autistic adults (19%) who identified enhancing the therapeutic skills of mental health professionals as a way to reduce the problems experienced is 1.7 times the proportion reported for the entire autistic sample (11%). This is an important reminder to researchers that overall group frequency may focus on the most visible barriers, and/or large group numbers may obscure the most significant barriers to access for some of the multiply marginalised groups. However, given we did not explicitly ask these participants to identify the problems in relation to intersectional identities (e.g., an autistic person who is LGBTQIA+), and the data from Figure 2 showing the complex interaction of intersectional identities in autistic people, further work is needed to explore these initial findings and to understand the role of the intersectionality in autistic people's experiences.
The minority stress model (Meyer, 2003) may offer a useful lens for understanding how barriers reported by participants may be experienced at multiple levels, impacted by and interacting with intersectionality. At the systemic level, structural factors such as long waitlists, high costs, and a lack of autism-informed services represent chronic stressors that may disproportionately affect those at the intersections of marginalised identities (e.g., autistic individuals who are also low SES or living regionally). Interpersonal stressors, such as stigma, clinician bias, or assumptions based on gender identity or sexuality, may, over time, contribute to internalised stress, where autistic individuals feel invalidated, blame themselves for poor service experiences, or avoid seeking help altogether. Botha and Gillespie-Lynch (2022) discuss this further, exploring how intersecting identities may compound exposure to minority stress across these levels, shaping both the accessibility and emotional safety of autistic people's mental health. Future work could build on this by explicitly examining how these levels interact to affect mental health outcomes and service engagement, ideally using studies that centre lived experience and use participatory approaches.
Limitations
Limitations of this study include the sample size, although a good size, was all from a single country, so it may only represent the Australian service delivery context. The sample was all recruited online, so the study only reached those who engage with social media. Word document versions of the survey were provided to participants who requested them, but this still required online access. As a result, the experiences of individuals who do not participate in online communities are underrepresented.
The sample did not include enough autistic people with high or complex disability/support needs to explore their experiences in depth. Furthermore, it is unclear which specific informants (e.g., parents or professionals) were reporting on behalf of this underrepresented group. The study also did not include enough participants from culturally and linguistically diverse (CALD) backgrounds to analyse their experiences separately. Purposeful engagement and recruitment of this community are likely important for understanding their intersectional experiences and ensuring a more inclusive perspective in future research.
The intersectional analysis here considers intersectional identities separately and, as such, means the study does not fully describe the complexity of multiple intersecting identities. As described by Botha and Gillespie-Lynch (2022), autistic people ‘embody, juggle and experience’ multiple layers of identity (e.g., gender, race, and SES; see Figure 2). The sample size in relation to the complexity of overlapping identities limits the extent to which this study was able to examine cumulative marginalisation (e.g., autistic, LGBTQIA+, and low SES) as well as cumulative epistemic positioning (e.g., autistic parents who are also professionals). Nonetheless, this work underscores the importance of considering intersectional identities in future research to better understand the diverse experiences within the autistic community.
Finally, there are potential biases in the study related to how respondents were asked to identify their ‘top three’ problems. No specific guidance was provided regarding whether participants should report those most commonly experienced or those with the greatest impact, which may have led to variability in the types of responses. Additionally, the interpretative nature of the content analysis introduces the possibility of bias in coding. While steps were taken to ensure consistency and reliability in the coding process, the subjective nature of interpreting qualitative data means that researcher bias may influence the identification and categorisation of themes. These limitations are inherent in qualitative research and should be considered when evaluating the findings.
Implications for Future Directions and Practice
This work has many implications for future research and clinical practice. Best practice requires us all to note and to act upon these research findings and address the ‘mental health crisis’ among autistic individuals. One clear pathway to addressing this is for autistic people to be heard and listened to, so mental health service provision can be improved. This can begin in training for all mental health professionals, ensuring that those in training (and those developing the training) have the opportunity and time to learn from the first-hand experience of autistic people accessing or trying to access the mental health system. This also extends to those who have qualified, who may not have received sufficient training, or have had training that is not up to date with current understandings of autism. Future research could evaluate the impact of such input, not only evaluating the impact on the therapy provided but also on the accessibility of paths to mental health supports and services.
This study has multiple implications for research, training, and clinical service provision. Addressing the ‘mental health crisis’ (Mandy, 2022) among autistic individuals requires meaningful, systemic change informed by lived experiences. One pathway towards this is through free and easy-to-access training for all mental health professionals. This should include opportunities to engage directly with the perspectives of autistic people, especially regarding barriers to access and unmet needs. However, we acknowledge that training gaps are not solely due to a lack of willingness; clinicians often face systemic constraints, including limited access to professional development, funding restrictions, and burnout. Therefore, improving knowledge and practice through training also requires a system-wide shift. Future research could examine how integrating autistic voices into training influences not only therapeutic outcomes but also service accessibility and trust.
The findings of this research highlight the importance of considering intersectionality as something that is relevant and impactful for autistic people. Whilst considered individually here, a person's intersectional identities all exist simultaneously and potentially interact, so if services are to be truly person-centred, consideration of all elements of a person's identity and their intersection is critical. Future work with larger samples can begin to explore how multiple intersecting identities impact experiences for autistic people; such work is needed if we are to understand how to provide genuinely person-centred services and supports for autistic people.
Footnotes
Author Contributions
DA and SM: conceptualisation. DA, SM, and AC: Data curation. DA, SM, JB, and AC: Formal analysis. DA and SG: funding acquisition. DA, SM, and AC: Investigation. DA, SM, SG, and WL: Methodology. DA, SM, and SG: Project administration. DA and SM: Resources and software. DA, SM, and SG: Supervision. DA: Writing – original draft. DA, SM, AC, JB, and SG: Writing – review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge the financial support of Autism CRC. This study utilised research data, owned by Autism CRC, which was collected and analysed in a project funded by the Australian Government Department of Social Services.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.