
Abstract
Background:
Mental health professionals play an important role in providing care and treatment for adults with intellectual disabilities. A number of studies use qualitative methods to explore the experiences of these professionals and their perspectives regarding the mental health services for this population. A systematic review using meta-ethnographic approach was undertaken to summarise this research.
Method:
A systematic search found 14 relevant studies which were critically appraised. Key themes from these studies were extracted and synthesised.
Results:
Three main themes were identified: 1) Understanding the person, 2) Relational interaction and 3) Organisational factors.
Conclusions:
The findings of this review identified the issues mental health professionals raised in relation to their work. They described the complex presenting problems as intense yet fulfilling therapeutic relationships with their clients and their wish to improve their knowledge and skills. They identified organisational issues that need to be addressed to improve staff morale and efficiency.
Keywords
Introduction
Many governments have guidelines and legislation to promote access for people with intellectual disabilities to mainstream services. For example, the UK government published a document entitled Valuing People (Department of Health, 2001) to encourage accessibility of mainstream services for people with intellectual disabilities. Trollor (2014) recommends accessible mainstream as well as specialist mental health services for this population in the UK. A recent review indicates that barriers to mental health services are related to deficits in knowledge and stigmatising attitudes among mental health professionals (MHPs; (Whittle et al., 2018)), highlighting the need to provide staff training (Woodward and Halls, 2009) to improve attitudes, as well as skills and knowledge of intellectual disabilities amongst MHPs (Rose et al., 2013).
There has been an increased interest in using qualitative methods in the field of intellectual disability to explore subjective experiences among different groups. For example, parents of people with intellectual disabilities have shared their views and experiences of interacting with professional staff (Doody et al., 2018), people with intellectual disabilities have related their experiences of services received (Ferguson et al., 2010) and of treatment (Evans and Randle-Phillips, 2020; Lewis et al., 2016), and support staff have described their experiences of taking care of people with intellectual disabilities in a residential setting (Ćwirynkało et al., 2017).
Qualitative research involving healthcare professionals has identified their perspectives about general (physical) healthcare services and their experiences working with people with intellectual disabilities. Themes found amongst healthcare professionals are related to the service delivery, organisational work culture, level of knowledge and competency which have an impact on the care quality (Chapman et al., 2017; Morin et al., 2018; Ouellette-Kuntz et al., 2003; Wilkinson et al., 2012). There has been little research on the experiences of MHPs providing mental health services for people with intellectual disabilities, highlighting the necessity to further explore their experiences and the challenges they experience in providing mental health services to people with intellectual disabilities which can lead to improvements in the quality of services for this population.
So far there has been no qualitative review of the experiences and perspectives of MHPs to understand the positive or negative aspects of their work with this specific client population. Research involving MHPs has primarily used quantitative methods to examine knowledge, skills or perceptions of people with intellectual disabilities without exploring personal experiences of working with this client group. The quantitative research findings have not provided much insight into how MHPs’ experiences affect their working practice or how they identify their roles and the services they provide for people with intellectual disabilities (Pelleboer-Gunnink et al., 2017; Werner and Stawski, 2012). Qualitative research can complement the quantitative findings by exploring experiences and attitudes of MHPs (Mays and Pope, 2000). Collating and synthesising qualitative findings is becoming increasing common and offers a rich source of easily accessible and clinically relevant information that may be used to inform policy makers and ultimately improve service delivery (Mays et al., 2005).
Aim of the review
The purpose of this review is to combine and analyse data from qualitative studies that report on the experiences of MHPs providing services to people with intellectual disabilities and mental health problems. This paper systematically reviews recent qualitative research on the experiences of MHPs working with people with intellectual disabilities by searching and collating the evidence to answer the following questions: How do MHPs experience their work of providing services to adults with intellectual disabilities and mental health problems? What are the challenges and facilitating factors that MHPs encounter which affect the care and treatment of adults with intellectual disabilities?
Method
Search strategy
A systematic search was carried out in 30 June 2020 to identify peer-reviewed articles published between 2006 and 2020 using the electronic databases PubMed, OVID PsychINFO, ProQuest, CINAHL, MEDLINE, PsyARTICLES and ScienceDirect. Past reviews included studies before 2006 and hence, the current review focuses on more recent studies which were published after the adoption of United Nations Convention on the Rights of Persons with Disabilities in 2006.
Table 1 lists the search terms chosen based on reading relevant literature and were combined to obtain the results of the literature search. Research has found that challenging behaviour is the most pronounced feature of mood disorders in people with intellectual disabilities (Hurley, 2008), and there are associations between people with intellectual disabilities having behavioural problems displaying symptoms of psychiatric disorders (Myrbakk and von Tetzchner, 2008). Hence, the term challenging behaviour is regarded in the paper as a symptom of mental health problems and is included in the search.
List of search terms.
Table 2 shows the inclusion and exclusion criteria that were used to evaluate and select the studies. The first author carried out the screening of the articles and the screening stage was verified by the second and third authors who ensured that relevant studies met the criteria.
Inclusion and exclusion criteria for qualitative review.
Extraction of data for meta-synthesis
A type of meta-synthesis named meta-ethnography (Noblit and Hare, 1988) was used as it was deemed to be the most appropriate way of extracting and analysing reported themes across the qualitative studies whilst maintaining the integrity of the primary data. The synthesis was conducted at the level of themes rather than quotes, with themes reported in the included studies being used to develop the overarching themes presented in this review. The first author (JE) first read the included articles and extracted the key themes reported in each paper. He then identified patterns and connections across the themes, grouping them into relevant categories. The first author’s views and interpretations were shaped by his profession as a clinical psychologist with background experience of working with people with intellectual disabilities. He was aware of his own experiences and kept a reflective journal during the analytical process and aimed to keep an open mind to minimise potential biases. He engaged in regular discussions and supervision with the second and third authors (JR and BSK) to carry out third order interpretations and develop superordinate themes for each relevant category. Lastly, the superordinate themes were arranged and labelled to form an overall narrative that answered the research questions, illustrated with relevant quotes from the studies.
Results
A total of 1196 papers was yielded after the systematic search. These publications were screened according to the relevance of title and abstract as well as removing the duplicates, which left 135 papers. From these, the abstracts of these 135 papers were read and 82 articles were removed after failing to meet the inclusion criteria. The main text of the remaining 53 papers were read and 39 papers failed to meet the inclusion criteria, leaving 14 studies for quality assessment and review.
The references of publications were examined to identify additional studies that met the inclusion criteria. None were identified resulting in a final total of 14 studies. Figure 1 shows the flow diagram of the selection process for the review.
Flow diagram of the qualitative review.
Study characteristics
A summary of the papers reviewed detailing the characteristics, findings, strengths and limitations is presented in Table 3. The studies included in this review will be referred to by the numbers allocated in Table 3.
Five of the studies used semi-structured interviews (4, 7, 8, 12 and 14), three studies used a mix of focus groups and semi-structured interviews (2, 9 and 10) and four studies used solely focus groups (1, 3, 5, 13). The remaining two studies (6 and 11) used free association narrative interviews. Most of the studies provided additional information on the questions used to guide the interviews (1, 2, 3, 8, 9, 10, 11, 13 and 14).
The most common qualitative approach utilised by seven studies was thematic analysis (4, 5, 7, 9, 11, 13 and 14), followed by Interpretative Phenomenological Analysis (10 and 12), content analysis (4), thematic analysis with a psychodynamic theoretical framework (6), systematic text condensation (8), grounded theory (1) and two did not specify any approach (Studies 2 and 3).
The sample sizes of the studies ranged from 5–44 (median = 13) and included 196 MHPs in total. Studies 6, 7, 11, 12 and 14 recruited nurses (n = 50). Studies 8 and 13 recruited psychologists (n = 9) and general practitioners (n = 10) respectively. The rest of the studies employed a mixture of MHPs including psychiatrists (n = 5), nurses (n = 42), psychologists (n = 12), medical social workers (n = 20), speech therapists (n = 3) and occupational therapists (n = 4).
Quality assessment tool
The quality of studies was evaluated and critically appraised by adapting the checklist from Cesario et al. (2002) and Mays and Pope (2000). Combining the two assessments provides more rigour for the assessment of the quality of the papers and allows the studies to be scored.
The checklist consists of 10 criteria and each criterion can be given a maximum score of 3 points. The scores across the 10 criteria are added to give an overall total score (see Table 3). The first author carried out the the quality assessment which was verified by the second and third authors.
Four of the studies (9, 10, 11 and 12) stood out for having attained a high quality ratings (24+). These studies have a detailed background literature, clearly defined hypotheses, appropriate explanation of the use of the methodology to collect the interviews and a detailed explanation of the analysis process to develop the themes.
The majority (N = 9) of the studies were judged as being of a lower quality as they did not provide a detailed description of the audit trail or explained the rationale for choosing the particular epistemological stance for analysis.
Study 3, with the lowest quality score of 13, lacked a detailed description of the sample size, objectives and aims of the study. There was no information regarding the type of analysis used and lacked details about how the data were collected.
Summary of qualitative studies (in chronological order).
Meta-synthesis findings
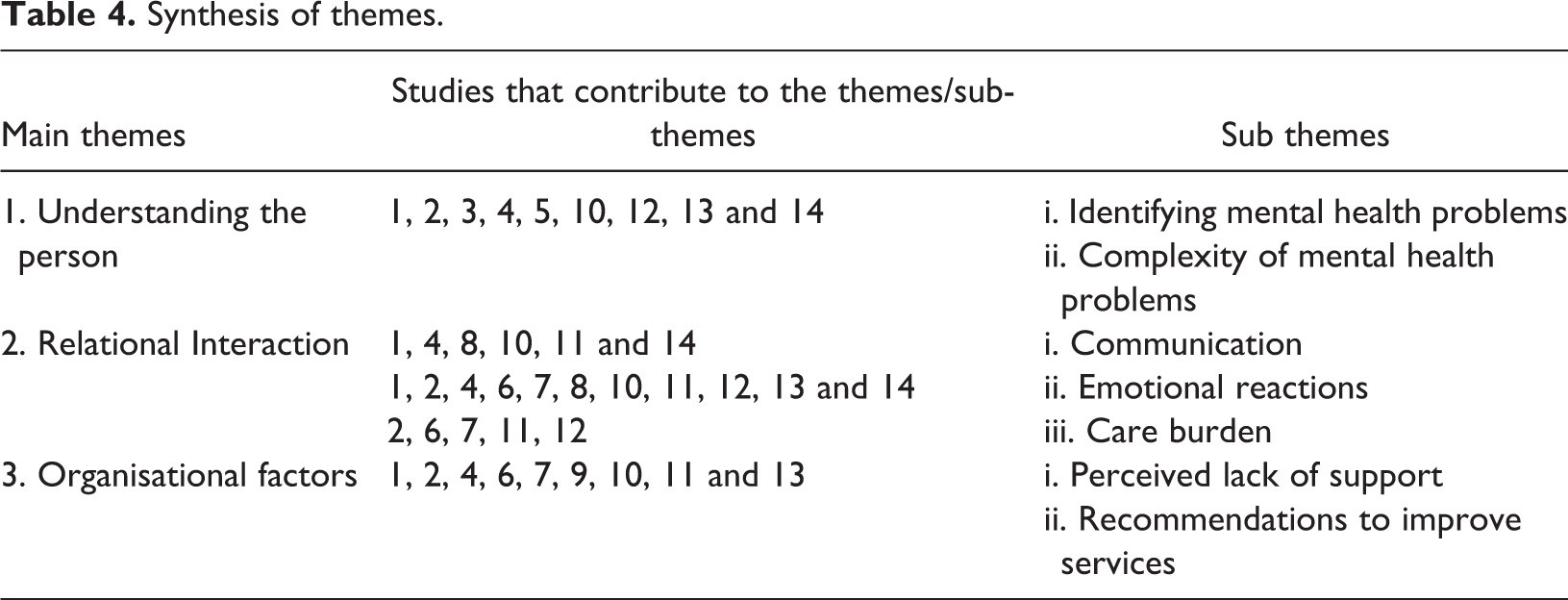
Table 4 shows the three main themes that were identified which were 1) Understanding the person; 2) Relational Interaction between healthcare professional and the service user and 3) Organisational factors. The second theme consists of three subthemes while the others consist of two subthemes.
The quotations from the MHPs in the studies are presented in italics whereas the quotations from study authors are not.
Synthesis of themes.
Theme 1: Understanding the person
This theme describes how MHPs develop an understanding of the adult with intellectual disabilities in a holistic manner while at the same time identifying the individual’s mental health problems during the assessment phase.
Sub-theme 1: Identifying mental health problems
MHPs recognised that adults with intellectual disabilities had a higher prevalence of mental health problems and that their family members often did not seek help until they were unable to manage. MHPs noted that the behaviours of the person with intellectual disabilities became the main focus of treatment where family members looked for a cure to eliminate the behaviours or transfer the burden of care to them, They [the carers] bring the patient to the ER looking for a miracle pill or wanting the hospital because they can’t cope. (Lunsky et al., 2008: 449) I think people just look at it all together really, they think it’s just challenging behaviour, they don’t think about the mental health issues. (Rose et al., 2007: 55) Again a lot of physical problems, maybe presenting to casualty, overdosing, self-harming, just self-neglect again, one or two of them are very vulnerable and I feel that a lot of them have maybe been exploited, financially and query sexually. (McLaughlin et al., 2009: 136) It’s a matter of trial and error…it’s important to take the time to listen, taking the time to observe, trying things, failing…learning from those mistakes. (Taua et al., 2017: 636)
This was particularly difficult for MHPs working in mainstream settings because of the high service demands, ‘We’re obviously swamped and the more people we can keep out the better’ and the lack of resources available in mainstream services, ‘…you really do need much more resources…where would you even get that…?’ (McNally and McMurray, 2015: 355).
The benefits of having extra time during the assessment helped MHPs to conduct a comprehensive assessment of the person with intellectual disabilities to have a holistic understanding of the person as a whole, They’ve all got their own special qualities, when you actually see the person, not the personality disorder and not the learning disability. (Lee and Kiemle, 2015: 243)
Sub-theme 2: Complexity of mental health problems
This sub-theme describes the complexity of mental health problems that MHPs encountered, the underlying risk factors and the challenges their clients face that contribute to their negative cognitions and feelings, and poor coping strategies, I have a few women who definitely use alcohol as a coping mechanism. They struggle with the expectations placed on them and they don’t see themselves as meeting these expectations, therefore they are depressed and lonely, using the alcohol to give them a reprieve and a release from feeling that way. (Taggart et al., 2010: 95)
MHPs observed that their clients’ mental health problems were often not addressed due to their intellectual disabilities, Most people that we see have a learning disability have a mental health problem, but actually, when I think, a lot of them don’t have a diagnosis. (McNally and McMurray, 2015: 357)
Theme 2: Relational interaction
This second theme relates to how MHPs view their therapeutic relationships with their clients as a ‘deeply emotional, intimate’ (Kittay et al., 2005: 444) and finding a sense of fulfilment when engaging with them during the intervention process but also reporting on negative emotions.
Sub-theme 1: Communication
MHPs described challenges in communicating with people with intellectual disabilities and mental health problems and in establishing therapeutic relationships with them, The hardest part is communication, getting yourself across in the right manner. (Rose et al., 2007: 55) A lot of experience I had was…using pictures and diagrams and just learning to actually think quite laterally about how can you explain things in quite a basic way…explain something in a way that is empowering and not patronizing. (Taua et al., 2017: 634) We have to prepare them for the community, but when they go…I am very sad…I have to walk away. (Capri and Buckle, 2015: 176)
Sub-theme 2: Emotional reactions
All of the studies, with the exception of 3, 5 and 9 highlighted the emotional reactions that MHPs experienced when working with adults with intellectual disabilities and mental health problems. MHPs in Capri and Buckle (2015) shared that they ‘feel proud’ and ‘enjoy doing the work’ despite acknowledging that ‘it is not easy working’ with this population, reflecting a ‘noble self-perception’ (p. 173) of providing services and care to someone with high care needs and mental health problems.
MHPs in other studies reported on the fluctuating emotions, It’s one of the hardest jobs in the world. And it was like a roller coaster ride. Erm, and sometimes you’d find it really overwhelming. (Lee and Kiemle, 2015: 242) Stressed and quite scared sometimes, sometimes angry that we should be exposed to this – it is a mixture really. (Campbell, 2013: 44) I don’t know whether it’s actually training but some kind of awareness sessions or some to staff in feeling less intimidated maybe because I think a lot of it is that they [the staff] feel intimidated. (Rose et al., 2007: 56) It makes me feel, not all the time but it does make me feel vulnerable and sometimes I must admit I have actually thought ‘what am I doing here’, ‘why am I doing this’ and then I think about it. (Campbell, 2013: 44) I feel really alone on this topic with these patients. I don’t really know what to do. (Fredheim et al., 2013: 5)
Sub-theme 3: Care burden
MHPs described having negative experiences of being verbally or physically targeted, affecting their sense of motivation to continue working in this field. Some expressed caution when they talked of developing therapeutic relationships and preferred to remain emotionally distant from some of their clients, The symptoms, if you like, of personality disorder make you a lot more wary of developing a relationship, yep, erm, yea again, you’re kinda a lot more suspicious! (Lee and Kiemle, 2015: 242) Every day when you walk on a shift or when you walk onto the unit until you know what is actually happening you need to be aware that it [violence] can happen at any time…(Lunsky et al., 2008: 43) It can be quite tiring cos obviously, a lot of the behaviours are repeated, over and over, and that’s quite frustrating. It can feel quite hard cos you don’t seem to move on from things and move forwards. (Lee and Kiemle, 2015: 241) She’d also know things that pushed my buttons.…that was really tiring, cos she would just be on you and you knew, you’d trip up before she would if you weren’t careful ‘cos she was that good at it…she’d have a subject that she knew I couldn’t, I wouldn’t, I was weak on and she’d always manage to trip me up…. (Storey et al., 2012: 233) It would have been nice to know that there would be someone…if I’m having these feelings that I’m bottling up…I can go talk to. We don’t have that. (Capri and Buckle, 2015: 177)
Theme 3: Organisational factors
The final theme described the organisational barriers and support that MHPs encountered and their views and recommendations to improve services.
Sub-theme 1: Perceived lack of support
This sub-theme describes the lack of support in the workplace. They identified an increased workload as a result of unnecessary administrative procedures, staff shortages which affected their morale, and stress when they were unable to do their job satisfactorily (Storey et al., 2012: 232; Stenfert Kroese et al., 2013b: 9). They agreed that heavy workload and long working hours led to emotional fatigue, ‘Sometimes it feels so overwhelming’ (Capri and Buckle, 2015: 174), often resulting in stress-related symptoms and leaving them feeling exploited and unappreciated, You get tired, working long hours, when you get home, you don’t really have time for your family, you just want to get in the bath and into bed. (Capri and Buckle, 2015: 174) There is sort of a feeling that we are not supported enough because…I think management have got this idea that there is a certain threshold/tolerance level for violence in the workplace that has almost become acceptable. So I often feel…we don’t get the support that we should be getting. (Campbell, 2013: 44) Sometimes [the doctors are] very nasty…they criticise. The nurse’s voice is not always so important unless it’s the doctor…if it’s a nurse who sees there’s a need then they won’t jump to help you. (Capri and Buckle, 2015: 175)
Sub-theme 2: Recommendations to improve services
MHPs talked about the importance of early detection of mental health problems of people with intellectual disabilities. They spoke about the lack of coordination between different services and a lack of knowledge regarding where adults with intellectual disabilities and mental health problems can seek help, The system is fragmented. We don’t know what’s out there and it’s hard to navigate. (McLaughlin et al., 2009: 450) I don’t think our service is geared up to be sympathetic to a client group that might be struggling with the confidence to actually say, oh yes I could get myself to wherever to see this psychologist on my own…(Rose et al., 2007: 57) …people with intellectual disabilities being placed with [psychiatric] hospital staff that haven’t got the knowledge to work with them or might even find it quite frustrating to work with somebody with a learning disability if they haven’t done before…(Stenfert Kroese et al., 2013b: 11) From an equality point of view, it would be difficult to argue anything but that they have a right to access the mainstream adult mental health setting. (McNally and McMurray, 2015: 357) If I wanted to refer a patient with these problems, NN was the person. NN, a psychiatrist with long experience, is easy to turn to, because he provides good answers to my questions. (Fredheim et al., 2013: 5) I think it’s about helping them access the generic services especially the housing…and substance misuse and employment. (Hemmings et al., 2009: 26)
They also recognised the importance of using screening tools to detect early signs of mental health problems so that people with intellectual disabilities can be referred to appropriate services for a more comprehensive assessment and treatment (McNally and McMurray, 2015: 96).
Discussion
This paper focused on the experiences of MHPs providing services for adults with intellectual disabilities and mental health problems. Findings of the meta-synthesis identified three main themes: (1) understanding the person beyond their diagnoses (2) therapeutic relationship and interactions with people with intellectual disabilities when working with them and lastly (3); organisational barriers and recommendations to improve the mental health services to this population.
MHPs reported that mental health symptoms were sometimes misattributed to their clients’ intellectual disabilities and not promptly treated. Reiss et al. (1982) termed this misattribution bias ‘diagnostic overshadowing’ which may influence the treatment of adults with intellectual disabilities and may lead to negative perceptions or stigmatising attitudes towards them (Jopp and Keys, 2001).
Due to the complexity of presenting problems, MHPs reported taking longer and needing more resources when working with people with intellectual disabilities, which they did not often have, especially when working in mainstream services. As a result, they were at times overwhelmed and MHPs acknowledged that psychotropic medication is often used as the first treatment of choice. Some MHPs may view the mental health problems solely from a medical treatment model perspective and consider the problem to lie with the person with intellectual disabilities for being unable to adjust to their environment (Williams and Heslop, 2005). This may explain the feelings of frustration when MHPs struggle to make progress and lead them to view their clients as untreatable.
Previous studies have explored the effectiveness of training for MHPs to increase their understanding of mental health issues of people with intellectual disabilities and found an increase in their level of confidence and knowledge after attending a teaching programme (Costello et al., 2007; Mohr et al., 2002). However, these improvements may not be maintained over time due to factors such as repeated exposure to violence and aggression, which may increase their care burden and evoke negative emotional reactions as highlighted in this review. The current findings are consistent with quantitative research conducted with direct care staff which found a positive correlation between negative emotions experienced by staff and severity of clients’ aggressive behaviours as well as predicting use of coercive measures to manage these behaviours (Hensel et al., 2014; Knotter et al., 2013).
It is interesting that although MHPs recounted positive experiences, many indicated that they experienced negative emotions and stress that affected their therapeutic relationships with their clients. They also perceived a lack of coping resources in their workplace and insufficient support from managers which exacerbated their stress, leaving them to feel burnt out and unappreciated. A growing body of literature suggests that this is common among MHPs where high levels of stress and burnout negatively affects staff motivation and increases staff turnover (Langdon et al., 2007; Søndenaa et al., 2015). Frequent exposure to aggressive behaviours has also been found to contribute towards emotional difficulties in MHPs (Hensel et al., 2014).
In the main theme Relational Interaction, MHPs understood the importance of building rapport with people with intellectual disabilities. Having a trusting therapeutic relationship (Ramsden et al., 2015) is essential and can only be acquired by working competently over a period of time. The therapeutic relationship is important for people with intellectual disabilities and they identified the ability to build such relationships as a desirable quality that MHPs should possess and only feeling comfortable sharing their emotional difficulties after a genuine working relationship has been established (Lewis et al., 2016; Weiss et al., 2009).
Our findings confirm that more support is required to address the mental and emotional well-being of MHPs working with people with intellectual disabilities and mental health problems (Edwards and Burnard, 2003). Help-seeking behaviours among MHPs are likely to be influenced by their work culture and environment (Chan and Huak, 2004) where there may be a lack of motivation to use appropriate resources for fear of being penalised. Regular supervision sessions and/or stress management interventions for staff are regarded as essential for creating a positive organisational culture. Having an experienced supervisor can help junior staff to cope with work stress and demands (Acker, 2011). Stress management interventions for support staff have been shown to reduce levels of distress, may improve well-being and mitigate negative emotions (Innstrand et al., 2004; McConachie et al., 2014).
There is no clear consensus among MHPs regarding the need for specialist mental health services for people with intellectual disabilities. Some were keen on a specialist mental health service whilst others expressed concerns that this could be viewed as a way of depriving them of the right to access mainstream services. They advocated instead for more resources to adapt mainstream services to become accessible and responsive to the needs of people with intellectual disabilities. One suggestion is for the specialist services to be embedded within community settings or co-located in primary healthcare services to increase the rates of early detection of mental health problems in people with intellectual disabilities and improved access to services and treatments (Ervin et al., 2014; Hemmings et al., 2014). Further research should explore the views of other stakeholders regarding specialist services to inform future commissioning.
There are some limitations of this review which must be noted. The selected studies lacked details to demonstrate evidence of reflectivity and description of audit trails as was highlighted in the quality appraisal. Also, the majority of the studies were carried out in western countries (and 10 of the 14 studies in the UK) where culture, clinical practice and experiences may differ from other parts of the world, hence the findings may not be generalisable to non-western countries. Moreover, the findings from the meta-synthesis are based on qualitative data that was derived from different participant groups, with different levels of work experience and working in different environments. The themes thus represent the common experiences, emotional reactions and challenges faced and any nuanced differences between the participant groups has not be considered.
Footnotes
Authors’ note
Derived data supporting the findings of this study are available from the corresponding author [JR] on request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.