
Abstract
Few studies have qualitatively explored the beliefs, attitudes and behaviours underlying stigma related to attention-deficit/hyperactivity disorder (ADHD) from the perspective of various key stakeholders, with limited attention to gender. This study explores key perspectives and experiences of young adults with ADHD on ADHD-related stigma across the lifespan. It includes additional insights from key stakeholders to elucidate these themes and examines gendered differences in descriptions provided by young adult men and women with ADHD. Seven focus group discussions engaged 24 respondents, including 14 young adults with ADHD, three parents of seven children with ADHD, four mental health professionals and three primary school teachers. Thematic content analysis revealed overarching themes encompassing overt and subtle stereotypes and prejudice: (a) rejection of ADHD; (b) ADHD as a deficit, with subthemes of blame and negative characteristics; and (c) misconceptions, with subthemes of stereotyping and trivialising ADHD. Discriminatory behaviours and individual impacts encompassed a lack of understanding and appropriate support, facilitating negative self-concept. Gendered nuances appeared in theme descriptions. Young adult women reported scepticism, delayed diagnosis, altered identity development, masking and loneliness, whereas young adult men reported rejection, internalised negative attributions, nondisclosure and limited help-seeking behaviours. Our study contributes a new perspective to the qualitative ADHD-related stigma literature by suggesting gendered patterns as a reinforcing cycle.
Lay Abstract
Children and adults with attention-deficit/hyperactivity disorder (ADHD) may encounter negative beliefs, attitudes and behaviours associated with ADHD, known as stigma. Stigma can have harmful effects on mental health, wellbeing and opportunities in life. There is limited knowledge about the perspectives of young adults and additional key stakeholder groups on ADHD-related stigma, such as parents, mental health professionals and teachers. Our study, conducted in the Netherlands, aims to address this knowledge gap and also explores gender differences in how stigma impacts daily life. In seven focus group discussions involving 24 participants, we identified recurring themes of stigmatising beliefs and attitudes, namely: (a) rejection of ADHD; (b) viewing ADHD as a deficit through blame and associating negative characteristics; and (c) misconceptions that involve stereotyping or trivialising ADHD. Stigma shaped the everyday experiences of people with ADHD, through a lack of understanding and a lack of appropriate support. These interactions can influence how individuals with ADHD view themselves. We found that young women with ADHD mainly reported to grapple with scepticism, a delayed diagnosis, altered identity development, masking and loneliness, while young men reported rejection, internalised negative beliefs, reluctance to disclose their condition and limited willingness to seek help. By highlighting gendered patterns of ADHD-related stigma, our research suggests a reinforcing cycle of stigma. Study findings can aid in preventing gender stereotypes in ADHD-related mental health care, while also better preparing educators and healthcare professionals to support individuals with ADHD in their diverse needs and strengths.
Attention-deficit/hyperactivity disorder (ADHD) is a highly prevalent developmental disorder with a world-wide prevalence of around 5.9% in children and 2.1% in adults (Faraone et al., 2021). ADHD presentation include persistent levels of inattention, hyperactivity and impulsivity, which interfere with daily functioning (Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5); American Psychiatric Association, 2013). Individuals with ADHD are at risk of experiencing stigma across the lifespan (Lebowitz, 2013; Mueller et al., 2012). ADHD is often misconstrued, such as by highlighting hyperactivity over inattentiveness, or by a predominant focus on boys (e.g., Horton-Salway & Davies, 2018). Moreover, people with ADHD may experience rejection (Paulson et al., 2005) and ADHD may be deemed an excuse or fake diagnosis (Holthe & Langvik, 2017). The absence of diagnostic instruments perceived as more objective (either biological or environmental), the considerable heterogeneity in aetiology and presentation, and negative media coverage are all thought to contribute to the distrust of the concept of ADHD, thus perpetuating stigma (Baeyens et al., 2017; Hinshaw et al., 2022; Quinn & Madhoo, 2014). Stigma is found to negatively impact mental wellbeing, treatment efficacy and adherence and access to mental health care and hinder life opportunities, such as access to employment (Mueller et al., 2012; Østerud, 2023; Schoeman & Voges, 2022).
In social psychology, mental illness stigma has been conceptualised as being composed of stereotypes, prejudice and discrimination. These components represent public or internalised cognitive, emotional and behavioural responses to one's devalued identity (Dovidio et al., 2010; Stangor, 2009). Stereotypes are viewed as knowledge structures or beliefs (i.e., cognitive responses) regarding characteristics of an individual or a social group (Crocker et al., 1998; Hilton & Von Hippel, 1996). Stereotypes can exist without people agreeing with them or without being negatively characterised (Jussim et al., 1995). However, when one endorses a negative stereotype, this results in prejudice. Prejudice is the affective reaction (i.e., emotional response) toward oneself, an individual or a social group (Crocker et al., 1998; Stangor, 2009). Prejudice may subsequently lead to discrimination, which represents a biased behavioural response to prejudice. This can be characterised by behaviours such as avoidance, withdrawal or rejection (e.g., Corrigan & Kleinlein, 2005; Paulson et al., 2005). The body of qualitative literature focusing on children or caregivers and adult and health professional perspectives regarding (the impact of) ADHD and ADHD health care is growing (Schrevel et al., 2016; Watters et al., 2018). However, few studies have qualitatively explored the diverse beliefs, attitudes and behaviours underlying stigmatisation from the perspective of various key stakeholders. Furthermore, there has been limited attention to the possible gendered dynamics of stigma in daily life.
Gender has been theorised as a set of everyday learned and socialised behaviours and performances, conditioned and regulated by society (Butler, 1990). Gender performativity suggests that individuals ‘do’ or ‘perform’ gender, by conforming to societal norms and expectations associated with social constructions of masculinity or femininity (i.e., gender roles and norms) (Butler, 1990). Gender should thereby be understood as defined through social relations, rather than as defined within the individual (Bohan, 1993). Gender performativity is shaped by what one deems appropriate behaviours for individuals and influences daily behaviours and experiences from a young age. These norms and expectations may change and evolve over time and are highly context dependent. Thus, gender may influence how ADHD is stigmatised and how stigma impacts one's daily life.
Studies have shown that gender influences health beliefs and attitudes and one's management of health conditions, and may thus influence health outcomes (Saltonstall, 1993; Williams, 2000). In the context of ADHD, gender differences in ADHD presentation have been previously identified, and girls and women tend to be less likely to receive a diagnosis (Hinshaw et al., 2022; Quinn & Madhoo, 2014). Furthermore, gender may influence how individuals with ADHD construct exert or protect their femininity or masculinity in a given situation and may thus influence one's coping with ADHD and/or stigma. For example, a literature review identified that girls and women tend to cope with ADHD by better masking ADHD behaviours, in comparison with boys and men (Quinn & Madhoo, 2014). Men compared to women may show a reduced willingness to disclose a mental illness, which was associated with greater levels of public stigma and higher levels of perceived stress (Brown et al., 2018). Therefore, the current study aimed to gain insight into gendered differences in ADHD-related stigma.
This study is exploratory and adopts a qualitative approach, in order to gain an in-depth understanding of ADHD-related stereotypes, prejudices and discrimination, and their impact on the lives of young adults and children with ADHD. The aim of this study was threefold: to gain insight into young adult and additional key stakeholder perspectives and experiences related to (a) positive and negative stereotypes and prejudice related to ADHD; (b) discriminatory behaviours and impact on the daily life of children and young adults with ADHD; and (c) to gain more insight into the role of gender in ADHD-related stigma. Key stakeholders included young adults with ADHD, parents, primary school teachers and mental health professionals. We chose to focus on young adulthood (aged 18 to 30), as young adults are increasingly expected to be independent during this period, which may pose specific challenges for people with ADHD (Lasky et al., 2016). We used focus group discussions (FGDs) as these are suited to explore diverse perspectives and experiences as well as to allow interaction between respondents to co-define and co-construct inputs (Morgan, 1997). We chose to conduct single-sex FGDs for young adults to ensure homogeneity within groups, which could facilitate open and smooth discussions. This approach also incorporated a comparative dimension between perspectives and experiences related to ADHD-related stigma (Morgan, 1997).
Methods
Sample, sampling and recruitment
A total of four small FGDs were conducted with young adult men and women with ADHD (18–30 years). Additional three small FGDs were conducted with parents of children with ADHD, mental health professionals and primary school teachers (see Table 1). To include the perspective of children with ADHD, we asked young adults about their childhood, and included perspectives of parents of children who were diagnosed with ADHD at primary school (6–12 years). We opted for small FGDs, comprising three to five participants, to facilitate in-depth discussions and valuable contributions from all respondents, while fostering a safe environment for sharing experiences on stigma and related impacts. The smaller groups helped avoid a sense of hierarchy between the researchers and participants, likely aided by the fact that one of the interviewers (MV) was relatively close in age to several of the young adult respondents. Additionally, we observed that these small FGDs tended to promote conversational interactions among participants, rather than a question-and-answer dynamic directed solely towards the researcher(s). These benefits have also been observed by Toner (2009).
Respondent characteristics.

Note. FGD: focus group discussion; SD: standard deviation; ADHD: attention-deficit/hyperactivity disorder; C: combined; I: inattentive; H-I: hyperactive–impulsive.
Participants were all mothers of the total seven children diagnosed with ADHD in childhood (<12 years old), including two girls and five boys.
Three respondents had professional experience with children with ADHD, while two respondents had experience with young adults with ADHD.
Participants were recruited between December 2022 and July 2023 through convenience sampling using professional and social networks of the involved researchers, through an advertisement on the website of the ADHD interest group and a parent association, as well as advertisements on social media pages. Inclusion criteria for the young adult groups were age 18 to 30 and those who self-reported recent or past ADHD diagnosis without further exclusion criteria (e.g., comorbidities such as autism spectrum disorder). Caregivers or parents were included when they self-reported that one or more of their children was diagnosed with ADHD at primary school. Mental health professionals were included when they reported to be directly involved in ADHD health care for children and/or young adults. Primary school teachers were included when they reported to have some experience with children with ADHD in primary education.
Focus group discussions
The FGDs followed a semi-structured FGD guide. The FGD design was developed by the authors and went through multiple rounds of review. The FGDs with young adults and parents comprised three activities, while the FGDs with the other stakeholder groups comprised two activities. Activities included individual writing on (online) sticky notes which were then placed on (online) flipcharts followed by plenary discussion. The FGD started with a discussion about both positive and negative perspectives on or experiences with ADHD in daily life (activity 1). This was followed by a discussion regarding ADHD-related stigma and individual impacts across various contexts (including educational, professional, social or family contexts) and gender differences (activity 2) and on ADHD-related stigma reduction (activity 3). During activities 1 and 2 of the FGDs with young adults, we used three flipcharts representing different life stages (childhood, adolescence and present) to facilitate reflection on experiences across their lifespan. Activity 3 is beyond the scope of this paper and findings are described elsewhere (Visser et al., in preparation). The detailed FGD outlines can be found in Supplementary Material 1.
Data analysis
All FGDs were audio recorded and transcribed verbatim. The transcripts were coded and analysed using Atlas.ti 22 and Excel. Data were analysed following thematic content analysis (Braun & Clarke, 2006). First, the first author (MV) familiarised herself with the data and re-read all transcripts. During this process, recurring themes and subthemes were inductively identified through open coding. Then, these codes were categorised into themes that aligned with our research questions. This codebook (see Supplementary Material 2) was discussed with the co-authors before initiating the coding process. Second, MV started deductive axial coding following the codebook on the individual level and additional subcodes were added during coding when relevant. All coding was completed by MV.
The thematic content analysis included a review of all codes included under each category. Quotes pertaining to each subcode were extracted and organised in individual Excel spreadsheets for each stakeholder group. The analysis was thus performed at the stakeholder group level with the aim to identify relevant perspectives per individual stakeholder group. However, the young adult perspectives were prioritised in the analysis for identifying the key thematic categories. These were supported by perspectives from parents, primary school teachers and mental health professionals. Individual quote extracts were grouped under key subcodes under two overarching categories: ‘stereotypes and prejudice’ and ‘discriminatory behaviours and individual impacts’, in line with the research questions. For the first category, the code groups containing individual quotes were given additional labels highlighting the underlying belief or attitude of the individual quotes in each code group (i.e., selective coding). This last step led to the identification of the different types of ADHD-related public and self-stigmatising beliefs and attitudes. For the second category, individual quote extracts referencing perspectives and experiences related to public or internalised behavioural responses (i.e., discrimination) towards ADHD were given additional labels that highlighted the type of discriminatory behaviour or individual impact within educational, professional, social or family contexts. Data were analysed for male and female young adult respondents separately. For the purpose of this article, the quotes were translated from Dutch to English.
Procedure and ethics
Data were collected between December 2022 and July 2023. Prior to participation in the FGD, respondents completed a short online survey concerning demographic information and an informed consent form. All FGDs were conducted in Dutch. The FGDs with young adults with ADHD were organised face-to-face at the Vrije Universiteit, Amsterdam, and took around three hours including breaks. Prior to the FGD, the researchers communicated the planned topics of discussion as well as the process of the FGD with the participants. The FGDs with parents, mental health professionals and primary school teachers were organised online via Zoom and took between 90 and 120 minutes. Only young adults received financial compensation for their participation in the study and travel costs as their FGDs were organised face-to-face. The amount of compensation (100 EUR) was communicated to young adults after participation. The study was approved (reference number VCWE-2022–131) by the Scientific and Ethical Review Board of the Faculty of Behavioural and Movement Sciences at the Vrije Universiteit, Amsterdam. All data were stored on a password protected university drive and the transcripts were stored separately from personal information.
Results
Sample characteristics
A total of 24 respondents participated in seven FGDs, including 14 young adults with six male and eight female respondents with mean ages of 26.2 years (standard deviation (SD): 3.5) and 25.8 years (SD: 4.0), respectively (see Table 1). In addition, three parents participated, all of whom were mothers of one or more children diagnosed with ADHD. The group of seven children consisted of two girls and five boys. Finally, we included three primary school teachers (all women) with experience in teaching students with ADHD, and four mental health professionals (one man/three women) with experience in the assessment and treatment of children and/or adults with ADHD.
Key findings for each main theme discussed in the FGDs from the perspective of the various stakeholder groups are presented. First, results for ADHD stereotypes and prejudice expressed by young adults and endorsed by other stakeholder groups, are presented. Second, discriminatory behaviours and individual impacts are presented separately for young adult men and young adult women. A table including all key supporting quotes can be found in Supplementary Material 3. Quotes included in this paper are numbered (Q1 refers to quote 1) and correspond to the numbering in Supplementary Material 3. Each respondent was also assigned a number, and supporting quotes include a reference to the respondent’s number (e.g., R1).
Perspectives on ADHD-related stereotypes and prejudice
All stakeholder groups were able to identify stereotypes and prejudices underlying ADHD-related stigma. Further, young adults identified that public beliefs and attitudes related to ADHD may be expressed, among others, through unintended and/or well-meaning, yet harmful comments or interactions. Both the occurrence (Q1) and negative impact (Q2) of these stigmatising interactions were highlighted.
Three major themes of ADHD-related stigmatising beliefs and attitudes were derived from the FGDs: (a) rejecting ADHD; (b) ADHD as deficit via blame or attributions of negative characteristics; and (c) misconceptions stereotyping or trivialising ADHD. In addition, stakeholder groups identified balanced and inclusive beliefs and attitudes. An overview of the three categories of stigmatising beliefs and attitudes is presented in Table 2. The thematic categories of beliefs and attitudes presented in the subsequent section of the results were consistently highlighted by young adults. Further, we indicated per category whether and how perspectives received endorsement from other stakeholder groups.
Everyday stereotypes and prejudices towards individuals with ADHD and/or family members.

ADHD: attention-deficit/hyperactivity disorder.
Defined by the authors based on the work of Sue and colleagues on microaggressions (Sue et al., 2007).
Theme 1. Rejecting ADHD
This predominantly public belief and attitude rejects ADHD as legitimate diagnosis and questions the credibility and validity of one's experience. Young adults and parents provided examples of instances where others deemed ADHD to be a ‘fashion phenomenon’, ‘fake diagnosis’ or ‘fabrication’. While all stakeholder groups acknowledged the presence of such beliefs and attitudes, they were most often mentioned by young adults and parents (Q3–5). I have often heard “oh yes, you want to belong, don't you”. Then you really feel misunderstood. (Q4, R3, Women, FGD 1)
Theme 2. ADHD as a personal deficit: Blame and attributions of negative characteristics
Public and internalised deficit beliefs and attitudes impose blame and responsibility in terms of ADHD-related challenges on individuals with ADHD and their family members, and attribute negative characteristics. First, young adults reported beliefs and attitudes associating ADHD with mainly negative characteristics, such as incompetence and disruptive behaviour, while ADHD-related strengths are not, or to a lesser extent, recognised (Q6 – 8). I don’t like to start telling [that I have ADHD] now, because if I tell, everyone will see you as hyperactive and annoying. (Q7, R6, Women FGD 2)
Second, these deficit beliefs and attitudes may lead to blame by attributing ADHD-related behaviours, such as inattention, impulsivity or hyperactivity, to deliberate opposition or to a lack of intelligence and discipline. For example, the parents reported to encounter situations wherein others would attribute their child's behaviour to an inadequate parenting style (Q9). Teachers identified deficit beliefs and attitudes among parents towards ADHD in a school context, in which these parents refuse their child to get tested for ADHD and push teachers to ‘be tough’(Q10). That student …, [his] parents don't want to see it at all, don't want to test him either. But it's becoming a really big problem in the classroom. …The parents have a different idea…, they say “just be tough on him and then he will stop”. Yeah, you don't want that either. (Q10, R22, Teachers)
Theme 3. Misconceptions of ADHD: stereotypical attributions and trivialisation
Young adults and parents encountered situations where they perceived or were affected by misconceptions regarding ADHD. The most common misconceptions included stereotypical attributions of ADHD, such as assuming that ADHD exclusively affects young boys or presents solely through hyperactivity or a lack of focus (Q11–13). Young adults admitted to internalising such misconceptions while growing up, particularly the belief that ADHD only affects young boys (Q14–17). That's really the biggest thing. People just think you're very hyperactive, and that's all ADHD is. … while it is so much more than that. (Q14, R12, Men, FGD 2) Oh, but they are hyperactive boys in class, which is not me. (Q15, R8, Women, FGD 2)
Further, young adults, parents and mental health professionals in particular reported trivialising notions of ADHD, underestimating or generalising ADHD. For example, these include responses such as ‘everyone is a little ADHD’, ‘we all have trouble planning sometimes’ or ‘ADHD is of less importance alongside other classifications’. The unique ADHD-related challenges, as well as strengths, may thereby be downplayed, dismissed or left unrecognised (Q18–20).
Balanced and inclusive beliefs and attitudes
Across all stakeholder groups, perspectives and experiences related to balanced and inclusive public and internalised beliefs and attitudes were shared, recognising both the strengths and challenges associated with ADHD. These included that individuals with ADHD are seen as enthusiastic, curious and creative, for example. One young adult man shared that he and his family always suspected he had ADHD from a young age, and it was accepted and supported (Q21). During the FGDs, we explicitly asked respondents to think about both positive and negative beliefs and attitudes regarding ADHD. The positive associations remained the minority of ADHD-related beliefs and attitudes raised. This imbalance was explicitly acknowledged by young adults and parents (Q22). That I'm seen as enthusiastic and creative, but otherwise I personally can’t really think of many positive things that society has to say about me. This actually was a painful realisation. (Q22, R4, Women, FGD 2)
Discriminatory behaviours and individual impacts
Core to ADHD-related public stigmatising behaviours (i.e., discrimination) identified by young adults was the pervasive lack of understanding of ADHD and lack of appropriate support and discriminatory treatment. These themes were endorsed by both young adult men and women. Reflections from the other stakeholder groups supported these perspectives and experiences, drawing from observations and experiences with their children (for parents) or within their professional contexts (for primary school teachers and mental health professionals). While these themes were reported by both young adult men and women, we identified nuanced differences in how these behaviours and their impact on individual lives were described. An overview of thematic categories and their distinct descriptions, which appeared typical among women and men, can be found in Table 3.
Descriptions of discriminatory behaviours and individual impacts typical among young adult women and men.

Young adult women
Two core themes of public discriminatory behaviours were identified by women: (1) a lack of understanding, characterised by ignorance and scepticism and (2) a lack of appropriate support and discriminatory treatment. At the individual level, these public behaviours were associated with (3) a lower self-concept, related to an impact on identity development, masking and loneliness.
I mustered up the courage to tell my supervisor at work, and his reaction was actually such that he could not recognise [ADHD] in me. That gives me the impression like “oh, he doesn't believe it, or he doesn't get it, or he doesn't get me”, and that made quite an impact on me. … He said, “but how does that manifest itself, because I don't notice anything, you've finished everything neatly”. Then I think yes, but if only you knew …. [Responses] like, “it's not that bad”, that is very hurtful if you are very worried about something. With that [I] unknowingly continued to mask, …. I also think “I should not have said something because he doesn't realise it all”. Eventually you notice there is no space anymore to raise it again. (Q23, R2, Women, FGD 1)
Further, young adult women experienced scepticism, referring to responses of disbelief or distrust regarding the validity of one's ADHD. For example, sceptical responses included ‘are you sure’ or ‘it does not look like you have ADHD’. Young adult men endorsed that experiences among women and men may differ and noted that women may experience relatively more scepticism (Q24). Two young adult women also compared their experience to how people respond to men with ADHD. In their view, men with ADHD may be associated with more favourable stereotypes such as being funny and energetic (Q25).
When I didn't have [a diagnosis] yet, my mother often got very frustrated with me like “why don't you notice that, why don't you keep your appointments…”. She sometimes got angry and was completely unaware that I had ADHD. (Q32, R1, Women, FGD 1)
Further, one woman reflected on not feeling understood by mental health professionals and that she was offered group therapy that was of little practical use to her. This was also recognised by another respondent (Q34). Another woman shared her experience with a general lack of flexibility and support in a professional setting due to negative beliefs associated to ADHD. She detailed she was terminated from a job due to being too disorganised (Q35). I also … recently got fired … because I was too chaotic. … I had addressed it during the conversation, that I have [ADHD] and that this makes it difficult for me to deal with a lot going on at the same time…. I hoped they could support me …. They were not willing to do that and that was painful. It felt like I was being discriminated against …. That really hurt me a lot. … She said, “we really like you, but…”. (Q35, R4, Women, FGD 2)
I also find it very unfortunate that it is still that image of that hyperactive little boy, because I did show the signals in the past …, but it was never recognised. While now that I know, I do have more compassion for myself and I'm now also getting help, so therapy and medication, which just makes my life easier. I also think “if only I had known sooner”, because of that. (Q37, Women, FGD 2)
Young adult men
Two key themes of public discriminatory behaviours were mentioned by young adult men: (1) a lack of understanding, characterised by ignorance and rejection and (2) a lack of appropriate support and discriminatory treatment. These public behaviours were associated with (3) a lower self-concept, related to negative attributions, nondisclosure and limited help-seeking behaviours.
I think that image [that you are overreacting] is very Dutch. Maybe we are educated that way like, “just do it, go, get started!”. It's just when you're struggling with something, then it's just; “you started it, [so] go finish it”, “you're almost there, what kind of nonsense is this”, “turn off the television and finish it”. (Q38, R9, Men, FGD 1) My [childhood] has been quite difficult. You just had a lot of experiences of rejection when you were younger, from friends, teachers, society, on so many levels. I think that, for me, contributed to developing a kind of hypersensitivity to that kind of rejection. To again become that odd boy in the corner of the classroom that nobody really understands. (Q39, R14, Men, FGD 2)
R13: Girls are a bit more mature and a bit more serious [during high school]. That comes later with boys. But I really wish someone had said to me; “hey, you never pay attention, you're always doing other things and you catch up at night. That's fine but try it once and …if you do not manage, come back”. … I really noticed that people actually said yes well, … he will develop this naturally. But that's not the case at all. I only just started that. … I would have liked to have had it [help] or got tested. R14: Yes, … I really would have wanted that many times, that someone was just like, let's take this person seriously, instead of writing this person off immediately. But yes, that's part of it, boys will be boys. (Q42, R13 and R14, Men, FGD 2)
Young adult men acknowledged that stereotypes and prejudice impact their willingness to disclose their ADHD. Some of the young adult men expressed to recognise themselves in various negative beliefs and attitudes towards ADHD from a young age, influencing their willingness to disclose (Q48). Sometimes I can recognise there is some truth to lot of things. And of course, that also comes from childhood, and you would rather not show that to anyone. (Q48, R10, Men, FGD 1)
Further, they noted various challenges to their help-seeking behaviours, including their pride and not wanting to reveal they are struggling (Q49–50). Another man perceived that help-seeking for behaviours deviating from stereotypical presentations of ADHD is met with reduced social acceptance (Q51). This phenomenon among boys and men with ADHD was validated by mental health professionals. Some noted the challenge of getting boys and men, as well as fathers of children with ADHD, to see a mental health professional (Q52–53). Not wanting to get it wrong. That's really something. If I ask for help now, I'm showing that I cannot do it. (Q49, R12, Men, FGD 2) I also think girls are more open to it. The adolescent girls - if we make a proposal like “look, we think it is also important that a therapeutic process is started…”- agree to participate more often compared to the boys we see. (Q53, R18, mental health professionals)
Discussion
This FGD study identified pervasive stigmatising messaging towards individuals with ADHD in different contexts. ADHD-related stigmatising beliefs and attitudes can be characterised by rejection of ADHD, deficit thinking through blame and attribution of negative characteristics and misconceptions stereotyping or trivialising ADHD (see Table 2). Some of these responses are expressed subtly (e.g., ‘just try a little harder’) and in some cases are well-intended or implicit (i.e., based on unconscious beliefs, attitudes and behaviours). For example, responses such as ‘I never noticed anything’, are negating responses which may be well-intended. However, such responses exert a negative impact on individuals with ADHD and their family members. We also identified balanced and inclusive beliefs and attitudes regarding ADHD, including ADHD-related strength such as creativity. These findings are in line with a study on self-reported strengths of individuals with ADHD in the Netherlands (Schippers et al., 2022). In the current study, however, beliefs and attitudes based on ADHD-related strengths remained the minority of public beliefs and attitudes identified, highlighting the dominance of negative public beliefs and attitudes towards ADHD.
Further, the current study highlighted key public discriminatory behaviours, including a lack of understanding of ADHD and a lack of appropriate support and discriminatory treatment. While it is difficult to fully differentiate between the impact of ADHD behaviours (e.g., the negative impacts of inattention) and ADHD-related stigma, this study strengthens the body of literature showing that public stigmatising messaging has a detrimental impact on individuals with ADHD through lower self-concept and hindering access to appropriate support and mental health care (Corrigan, 2004; Corrigan & Kleinlein, 2005; Oexle et al., 2018; Singh et al., 2010). Moreover, this study identified key gendered nuances to discriminatory behaviours and individual impacts. Women typically reported scepticism, altered identity development, masking and loneliness, whereas men typically reported rejection, internalised negative attributions, nondisclosure and limited help-seeking behaviours. Important to note here is that the gendered nuances to discriminatory behaviours and individual impacts presented in the results do not suggest that these thematic categories for young adult men and women are gender-specific, nor that they should be understood as exclusively ‘male’ or ‘female’ impacts, determined within individuals or groups. Rather, these nuances suggests that discriminatory behaviours and individual impacts are shaped by gender performance, norms and roles.
Our finding that subtle stigmatising messages can have a negative impact on adults with ADHD is in line with previous literature recognising that mental health stigma may be implicit and persist via subtle expressions, as explicit and overt stigma have become less accepted (Stier & Hinshaw, 2007; Young et al., 2019). However, stakeholders in the current study also identified overt expressions of ADHD-related stigma, such as blame and rejection as well as experiences of conflict within the family or social exclusion in educational settings. Continuous and cumulative experiences of both overt and subtle stigmatising messaging identified in this study may, at some point, lead to a detrimental impact on identity development, health and wellbeing of individuals with ADHD. The concept of microaggressions was first coined in the race literature to describe subtle and everyday forms of prejudice and discrimination directed towards marginalised groups, particularly towards black people (Pierce, 1974). Later, this thinking extended to other marginalised identities relating to gender, sexuality, disability (Capodilupo et al., 2010; Keller & Galgay, 2010; Nadal et al., 2010; Weber et al., 2018) and mental illness (Gonzales et al., 2015). Sue and colleagues (2007) described microaggressions as daily exchanges, either intentional or unintentional, coded with denigrating messaging towards individuals with a marginalised identity. Using this work, exemplary stereotypes and prejudices, as shared by respondents in this study, and the underlying stigmatising messages are articulated in Table 2. Moreover, our findings corroborate with earlier work identifying stigma as a hidden and underestimated risk factor to health and wellbeing of individuals with ADHD (Mueller et al., 2012). Future research may engage with a microaggressions framework to study the underlying mechanisms of these subtle and hidden forms of ADHD stigmatisation.
Our findings indicate that ADHD stereotypes, prejudice and discrimination negatively impact one's self-concept, which, in turn, may hamper one's help-seeking behaviour and/or access to appropriate support and health care. We argue that this pattern may be seen as a reinforcing cycle, as shown in Figure 1. In this figure, the lack of appropriate support can be observed to disempower individuals with ADHD, based on respondents’ reflections on their own and their environments’ limited knowledge and understanding of ADHD and coping strategies. This was linked to reinforcing public and internalised ADHD-related stigma. Further, we identified nuanced differences between descriptions of discriminatory behaviours and individual impact typical among men and women. Our results thus suggest that the patterns of this reinforcing cycle of stigma may be influenced by gender performance, roles and social norms. This suggested cycle is in line with previous work on mental illness stigma, which has identified a vicious cycle of mental illness stigma due to discrimination, low self-esteem and low treatment efficacy (Sartorius & Schulze, 2005). Further, literature on discrimination in the workplace has previously conceptualised workplace discrimination as a subtle cyclical process (Jones et al., 2017).
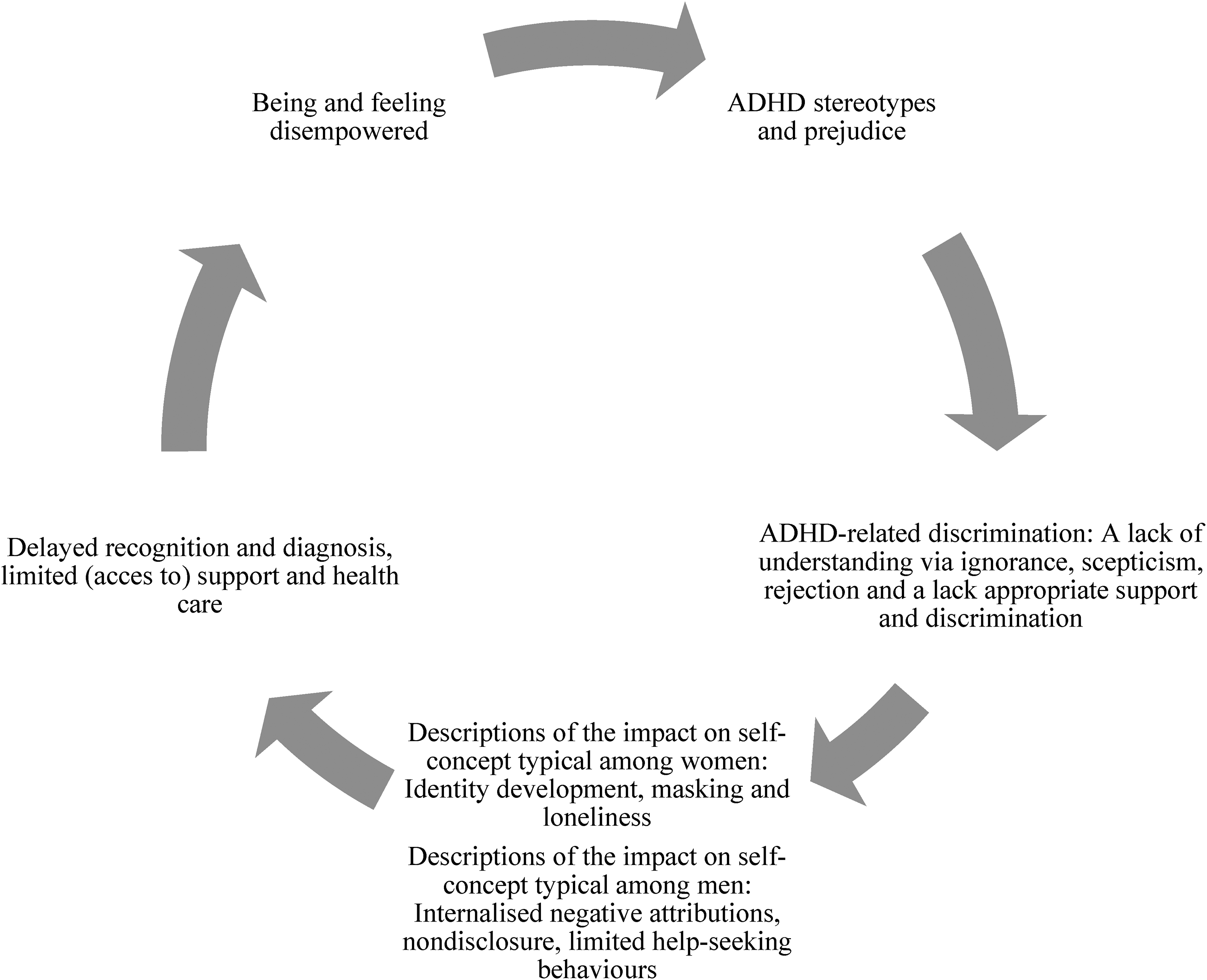
Theoretical model on the gendered reinforcing cycle of attention-deficit/hyperactivity disorder (ADHD)-related stigma.
Applying a gender lens to ADHD-related stigma may help us understand the suggested reinforcing cycle. Various respondents in our study confirmed an ongoing impact of unequal gender representation in public understandings of ADHD, shaping stigma. Experiences with a lack of recognition, scepticism and delayed diagnosis were particularly identified by those not fitting stereotypical images of ADHD (i.e., the hyperactive boy). This refers to girls and women with ADHD or boys and men with the inattentive presentation of ADHD. In the current study, young adult women in particular reported both public and internalised notions doubting validity of their diagnosis and experiences (e.g., ‘are you sure’, ‘it does not look like you have ADHD’ or ‘those are hyperactive boys I class, which is not me’).
Nuanced variations in discriminatory behaviours and individual impacts reported by male and female study respondents suggest that feminine and masculine ideals may contribute to shaping stigma and its impacts. Feminine norms are typically characterised as being kind, sensitive and patient, among others (Prentice & Carranza, 2002) as well as being engaged with one's own and others’ health, relating to health-seeking behaviours (Lyons, 2009). These may influence ADHD-related stigma, especially when individuals diverge from these norms. Stigma towards girls and women may be informed by negative judgments related to (the classification of) ADHD (e.g., rejecting ADHD or disbelief), gendered understandings of ADHD (e.g., ADHD only exists in young boys) and negative judgments based on diverging from feminine ideals (e.g., impulsivity or disorganisation). In turn, these dynamics may contribute to constructing girls’ and women's coping behaviours such as internalisation and masking (Quinn & Madhoo, 2014). Young adult women in our study reported individual impacts such as lower self-concept, related to altered identity development, masking and loneliness. A recent systematic review of studies focused on adult women who received an ADHD diagnosis in adulthood supports these findings, reporting women struggle with self-esteem and self-efficacy, and feel different and alienated (Attoe & Climie, 2023). The review also reports relief and increased self-acceptance after women receive a diagnosis.
Masculine norms typically include being assertive, competitive, ambitious and self-reliant, among others (Prentice & Carranza, 2002). As with women, conforming to or deviating from traditional gender roles can influence ADHD-related stigma and its impacts. The current study characterises ADHD-related stigma towards men through negative attributions, misconceptions (such as ADHD presenting solely via hyperactivity) and negative judgments regarding the need for support. Specifically, the young adult men in our study reported experiencing ignorance and rejection, as their needs were typically characterised as overreactions or exaggerations, and they were negatively attributed. Both teachers and young adult men shared experiences with public notions to ‘push through’ or to ‘just be tough on him’. This stigmatising response includes explicit notions to conform to masculine norms such as competitiveness and invulnerability. Further, boys’ and men's hesitancy to disclose their ADHD diagnosis or to seek help may be the result of their wish to figure it out by themselves first (coded by self-reliance and independence) and a fear of shame or judgment due to not achieving masculine ideals. These findings contribute to the growing body of literature identifying lower help-seeking behaviours of men regarding their mental health (Addis & Mahalik, 2003; Pattyn et al., 2015).
Despite its strengths, this study has some limitations to note. First, we used a (relatively small) convenience sample and our sample lacks diversity in terms of ethnicity and gender identity, and includes relatively high educational levels and a dominant urban representation. This may have limited our ability to capture a comprehensive range of perspectives and experiences pertaining to ADHD-related stigma. In addition, the average age of receiving an ADHD diagnosis is relatively high in our sample, 19.8 and 23.8 years for men and women, respectively, which may have led to underrepresentation of early childhood experiences and overrepresentation of experiences with ignorance and late recognition of ADHD. Given the limited sample size, our study did not aim to assess stigma within distinct contexts or age groups. Nevertheless, the themes of discriminatory behaviours and individual impacts reported in the current study were comparable across various contexts and the lifespan. Experiences with stigma reported by young adults were frequently traced back to childhood and persisted into adulthood. A key difference observed is that when discussing ADHD-related stigma towards children, some of the stigma attached to ADHD was attributed to caregivers, whereas among young adults, stigma was particularly attributed to themselves. However, the FGDs with primary school teachers and parents predominantly focused on stigma towards children. Future studies should engage these stakeholder groups to further explore stigma in young adulthood. Further, we differentiated our FGDs and our analysis between men and women to uncover gendered dynamics. Despite our efforts to recruit a diverse sample of respondents, our study did not include perspectives of fathers or male teachers. Our analysis employed a binary approach to gender, thereby overlooking experiences of individuals who identify outside of the male-female binary. Future studies could engage with gender as a continuum, and should include individuals with diverse gender identities to further explore the role of gender. Moreover, additional research is needed to unpack the role of other intersecting markers of identity (Bergey et al., 2022), in order to develop a comprehensive understanding of ADHD-related stigma.
There are various implications of these findings. Our findings suggest a need for recognition of the profound impact of ADHD-related stigma on the lives of individuals with ADHD, particularly in light of the gendered impacts. More attention should be paid to efforts reducing prevailing misconceptions of ADHD among the general public, mental health professionals, teachers, and individuals with ADHD and their family members. Education and contact-based interventions have previously been found most impactful in changing knowledge, attitudes and behaviours related to mental health (Corrigan, 2012; Dalky, 2012; Morgan et al., 2018). Moreover, our findings point to a need for improving interventions to target the implicit beliefs, attitudes and behaviours underlying ADHD-related stigma. While studies on the reduction of implicit stigma related to mental illness (Young et al., 2019) or among health professionals (Sukhera et al., 2020) are being conducted, few studies have investigated and aimed to reduce implicit stigma related to ADHD. Lastly, this study suggests a need for sensitising mental health support and services to gendered patterns of ADHD-related stigma, by tailoring services to individual needs and facilitating support groups, for example.
The responses identified by key stakeholder groups encapsulated both overt and more subtle stigmatising messaging towards individuals with ADHD from an early age. Our study suggests a possible reinforcing cycle of ADHD stigmatisation, influenced by context and social norms, wherein gendered patterns play a role, impacting the health and wellbeing of individuals with ADHD throughout their lives. Future research could investigate the underlying mechanisms of stigma, including how to interrupt the reinforcing cycle of stigma. For example, research could focus on the role of gender performance, roles and norms in shaping ADHD-related stigma, and how these factors may influence the ways individuals cope with ADHD and stigma. Understanding the underlying mechanisms of stigmatisation may help us to avoid gendered stereotypes in diagnosis and mental health care services, as well as better equip individuals working in education and health care in supporting individuals with ADHD in their diverse needs and strengths.
Supplemental Material
sj-docx-1-ndy-10.1177_27546330241274664 - Supplemental material for Understanding ADHD-related stigma: A gender analysis of young adults and key stakeholder perspectives
Supplemental material, sj-docx-1-ndy-10.1177_27546330241274664 for Understanding ADHD-related stigma: A gender analysis of young adults and key stakeholder perspectives by Marlies J Visser, Ruth MH Peters and Marjolein Luman in Neurodiversity
Supplemental Material
sj-docx-2-ndy-10.1177_27546330241274664 - Supplemental material for Understanding ADHD-related stigma: A gender analysis of young adults and key stakeholder perspectives
Supplemental material, sj-docx-2-ndy-10.1177_27546330241274664 for Understanding ADHD-related stigma: A gender analysis of young adults and key stakeholder perspectives by Marlies J Visser, Ruth MH Peters and Marjolein Luman in Neurodiversity
Supplemental Material
sj-docx-3-ndy-10.1177_27546330241274664 - Supplemental material for Understanding ADHD-related stigma: A gender analysis of young adults and key stakeholder perspectives
Supplemental material, sj-docx-3-ndy-10.1177_27546330241274664 for Understanding ADHD-related stigma: A gender analysis of young adults and key stakeholder perspectives by Marlies J Visser, Ruth MH Peters and Marjolein Luman in Neurodiversity
Footnotes
Acknowledgements
We wish to thank the Dutch interest group Impuls & Woortblind and parent association Balans in supporting us with the recruitment of respondents for this study. Furthermore, we wish to express our gratitude to our respondents for their time and contributions to the focus group discussions.
Data availability statement
Research data are not shared. The data are not publicly available due to privacy or ethical restrictions.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This study has been approved by the Scientific and Ethical Review Board (VCWE) of the Faculty of Behavioural and Movement Sciences, Vrije Universiteit, Amsterdam, reference number VCWE-2022-131.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.