
Abstract
Children and adolescents (henceforth “children”) with both attention-deficit/hyperactivity disorder (ADHD) and anxiety experience greater difficulties than children with either alone, though qualitative methodologies are yet to be used to understand the challenges this population experiences. We aimed to explore parent-reported daily impacts of co-occurring anxiety in children with ADHD (ages 8–13 years). Participants were enrolled in an Australian trial evaluating an adapted anxiety intervention and were eligible if their child met diagnostic criteria for ADHD plus separation, social, and/or generalized anxiety disorder. A baseline measure of life impacts associated with child anxiety captured situations parents reported were difficult, due to their child’s anxiety. Reflexive thematic analysis of free-text responses (N = 203) facilitated new insights via inductively generating key themes. Three overarching themes highlighted (1) child difficulties with everyday situations and processes due to their anxiety; (2) the nature of the child’s anxiety being pervasive and unrelenting; and (3) the strain placed on the child’s family system. This study enhances understanding of daily impacts associated with co-occurring anxiety and ADHD and may contribute to an improved understanding of support needs. Results reiterate the need to identify co-occurring difficulties in children with ADHD and support both children and their families.
Attention-deficit/hyperactivity disorder (ADHD) is a common neurodevelopmental condition affecting approximately 5% of children and adolescents (henceforth “children”) worldwide (Polanczyk et al., 2014). Up to 50% of children with ADHD also meet diagnostic criteria for ≥1 anxiety conditions (Jarrett & Ollendick, 2008; Tung et al., 2016; Yoshimasu et al., 2012; Yurtbaşı et al., 2018); most commonly separation, social, and generalized anxiety disorders (SEP, SOC, and GAD respectively; Sciberras et al., 2014). Despite high rates of co-occurrence, little is known about the daily impacts of living with both ADHD and anxiety from the perspectives of parents.
An emerging body of research suggests living with ≥1 anxiety conditions exacerbates difficulties for children with ADHD across a range of domains. The challenges encountered by children with co-occurring ADHD and anxiety exceed those experienced by children with either condition alone (Gould et al., 2018; Halldorsdottir & Ollendick, 2014; Sciberras, Efron, & Patel, 2019). The impact of co-occurring anxiety appears to modify the clinical presentation, prognosis, and treatment response in children with ADHD (D’Agati et al., 2019). For example, in a study examining the clinical characteristics of children with co-occurring ADHD and anxiety (N = 190), having both conditions was associated with experiencing more attentional difficulties, school concerns, and social challenges, compared to children with either single diagnosis (Bowen et al., 2008). In another large study (N = 392), children with ADHD and multiple anxiety conditions had substantially poorer parent-reported daily functioning (i.e., behaviors) and quality of life, compared to children with ADHD alone (Sciberras et al., 2014). Co-occurring anxiety has also been associated with more severe ADHD symptoms in children with ADHD (Tsang et al., 2015). Findings vary regarding associations between co-occurring ADHD and anxiety, and social and executive functioning (Bishop et al., 2019; Bowen et al., 2008; Jarrett & Ollendick, 2012; Menghini et al., 2018). Although it has been suggested that co-occurring childhood anxiety and ADHD may be associated with lower social competence (Bowen et al., 2008) and more executive functioning challenges (e.g., greater distractibility and attentional difficulties; Menghini et al., 2018), further research is needed to understand these relationships, given heterogeneous definitions and measurement of social functioning, and inconsistent conclusions regarding executive functioning (Bishop et al., 2019; Denis et al., 2016; Jarrett & Ollendick, 2012).
Despite growing research in this field, the daily impacts of anxiety in children with ADHD remain poorly understood from parent perspectives. A more nuanced understanding of the impacts of anxiety on the daily lives of children with ADHD may ultimately progress the development and tailoring of effective supports (Tsang et al., 2015). Studies to date examining the impact of anxiety in children with ADHD have used quantitative approaches, largely relying on a range of structured rating scales to assess challenges. A qualitative approach was anticipated to give voice to parents to express their firsthand experiences. Qualitative approaches are increasingly acknowledged as providing complementary insights to quantitative approaches, capturing depth and details that rating scales often fail to capture (Kandasamy et al., 2019). This is particularly important, given growing acknowledgment that understanding the context of children’s lives is important to advance child and adolescent psychiatry (Bassett, 2010). However, to date, studies using qualitative approaches to understand the impacts of co-occurring ADHD and anxiety are lacking.
Some qualitative studies in the general pediatric population have offered insights into the difficulties children experience due to anxiety, compared with their peers. For example, one study used qualitative methods to analyze parental beliefs (N = 48) about the impact of anxiety in their children (ages 9–12 years) who met criteria for an anxiety condition (Beato et al., 2018). This study found parents were concerned about the negative impacts of anxiety in the child’s and family’s daily lives. Specifically, parents identified concerns regarding the impact on the future adjustment of their child, the child’s socialization and social isolation, reduced opportunities to enjoy life and positive experiences, difficulty studying, indecision, and difficulty being alone. Interestingly, some parents felt their child’s anxiety was not negatively affecting their child, even when they identified their child feels uncomfortable or experiences physiological anxiety symptoms (e.g., upset stomach, sweating). Some parents perceived the anxiety had a positive impact, such as leading their child to be a good student who is achieving great school results, or helping their child to mature and make good decisions.
Another study of children living with an anxiety condition (ages 6–16 years) used qualitative methods to enhance understanding of their experiences (N = 30; Kandasamy et al., 2019). This study aimed to understand child perspectives of their concerns, the impacts of their anxiety, and their process of recovery with interventions. Self-reported daily impacts of their anxiety were identified, including impacts on the child’s achievement, interpersonal relationships, and themselves. Participants discussed the impact of their anxiety on performance in academic activities, play, and age-appropriate extracurricular activities. For example, wanting to avoid going to school or out to play due to anxiety, feeling irritable, frustrated, angry, depressed, and experiencing panic attacks related to exams. Children also reported perceived relationship challenges with their peers, family, and school authorities (Kandasamy et al., 2019).
Qualitative studies in children with ADHD and their families have detailed their daily experiences. A review of qualitative studies examining the experiences of parents of children with ADHD (n studies = 21; child age 5–18 years) generated six synthesized findings. These provided insight into parents’ experiences, related to living with a child with ADHD, and their health care experiences (Laugesen et al., 2016). Synthesized results illustrated complex challenges, including parental experiences of guilt, blame, stigmatization, exhaustion, emotions of hope and hopelessness, efforts to collaborate with services, and using strategies to overcome challenges and adapt to their new life.
Despite these few examples in the pediatric literature examining children with either ADHD or anxiety, to the best of our knowledge, qualitative approaches are yet to be used to explore daily experiences of anxiety in children with ADHD. Given previous quantitative studies suggest the presence of anxiety can exacerbate difficulties for children with ADHD, it is plausible that qualitative exploration of experiences reported by parents of children with both ADHD and anxiety may reveal differences compared with those reported in studies of children with either ADHD or anxiety. Exploring experiences of co-occurring childhood ADHD and anxiety was anticipated to contribute to a stronger empirical basis to inform tailored interventions to support the specific needs of this population. Traditionally, research in child psychiatry discarded the value of shared construction of meaning with participants (Bassett, 2010), and tended to overlook the involvement of consumers with lived experience who receive interventions, despite research indicating this improves the relevance of research (Werner-Seidler & Shaw, 2019). Furthermore, understanding lived experiences is necessary to develop acceptable, effective clinical treatments (Currie et al., 2018), and rating scales alone often fail to capture the depth and detail that free-text options offer for individuals to tell the story of their experiences (Braun et al., 2021; Kandasamy et al., 2019; York et al., 2011). Free-text approaches allow participants to freely share their experiences, rather than researchers pre-empting what these might be, ensuring results accurately capture perspectives from the consumers that interventions aim to support. This approach, compared with other qualitative methods (e.g., in-depth interviews), can be less burdensome and can provide an opportunity for participants to express themselves anonymously (Braun & Clarke, 2013), which can be helpful to understand experiences that may be associated with stigma (as is the case with ADHD; Laugesen et al., 2016), and to reduce social desirability and interviewer bias (Braun & Clarke, 2013). Therefore, the aim of the current study was to use a free-text approach to explore situations in which parents of children (ages 8–13 years) with co-occurring ADHD and anxiety reported their child’s anxiety to be challenging.
Materials and Methods
Participants
Participants in the current study had been recruited for a large randomized control trial (RCT) in Victoria, Australia, aiming to evaluate the effectiveness of an anxiety intervention adapted for children with ADHD (Sciberras, Efron, Patel, et al., 2019). Trial inclusion required children had previously been diagnosed with ADHD, met ADHD diagnostic criteria at the time of recruitment using the ADHD Rating Scale IV (DuPaul et al., 1998), and also met criteria for either SEP, SOC and/or GAD on the Anxiety Disorders Interview Schedule for Children 5 (Albano & Silverman, 2022). Trial participants were recruited from a list of families who had previously expressed interest in being notified about ADHD research, and via pediatricians (in outpatient public hospital clinics and private pediatric consulting rooms). Children receiving specialized help for anxiety and non-English speaking families were excluded. Participants in the current study were mothers (93.6%), fathers (4.9%), and grandmothers (1.5%) (henceforth ‘parents’; n = 203) of children ages 8–13 years.
Measures
Child Anxiety Life Interference Scale
The Child Anxiety Life Interference Scale (CALIS) assessed life impacts and difficulties associated with anxiety in children (Lyneham et al., 2013), is reliable (α = .90 and .88 for mother- and father-report, respectively), and has shown evidence of convergent and divergent validity (Lyneham et al., 2013). The parent-reported CALIS includes two 9-item scales assessing parent perceptions of impacts during the previous 6 months on both their child’s and their own life, due to their child’s anxiety. The severity of impact in each domain is rated on 5-point scales from 0 (“not at all”) to 4 (“a great deal”; total range 0–72); higher scores reflect greater impacts. The current qualitative study uses parent-reported free-text data in response to the question, “Please give examples of specific situations in which your child’s anxiety is a problem.” This is the measure of interest in the current study.
Anxiety Disorders Interview Schedule for Children 5
This structured interview (Albano & Silverman, 2022) assessed current and past child mental health conditions according to diagnostic criteria (American Psychiatric Association, 2013) and was completed via telephone with parents, for which it has been validated (Lyneham & Rapee, 2005). Modules were administered to detect SEP, SOC, GAD, and other conditions including specific phobia, obsessive-compulsive disorder, posttraumatic stress disorder, major depressive disorder, dysthymia, disruptive mood dysregulation disorder, conduct disorder, and oppositional defiant disorder.
Spence Child Anxiety Scale
The 44-item Spence Child Anxiety Scale provides six subscale scores (i.e., separation anxiety, social phobia, panic/agoraphobia, obsessive-compulsive, physical injury fears, and generalized anxiety; Spence et al., 2003), with higher scores reflecting greater anxiety severity (total range 0–114). It has high internal consistency (α = .92) and acceptable validity (Spence et al., 2003). Parent ratings are reported.
ADHD Rating Scale IV
The ADHD Rating Scale IV (DuPaul et al., 1998) is a standardized 18-item validated scale measuring core ADHD symptoms (total range 0–54; higher scores reflect greater severity), rating both symptom severity and classifying ADHD presentation, that is, predominantly inattentive, predominantly hyperactive/impulsive, or combined presentation. Reported scores were provided by parents during trial eligibility assessment, rated off medication.
Sample Characteristics
Parents reported characteristics for children (i.e., age, gender); parents (i.e., age, relationship to child, employment status, household income, education, single parent status); and if relevant, non-reporting parent/parent’s partner (i.e., age, education). Study-designed questions assessed current child medications, collapsed into antidepressant and ADHD medication (stimulant/atomoxetine) categories.
Procedure
Ethical approval was obtained from the Royal Children’s Hospital Melbourne Human Research Ethics Committee (HREC; 35164) and Deakin University HREC (2016-387). Eligible, interested families completed a baseline assessment, including a parent survey, a child direct assessment, and a child survey. Baseline, pre-intervention data are reported in this study.
Data Analysis
Descriptive statistics were calculated in Stata 16. An inductive approach to reflexive thematic analysis (TA) was used to analyze qualitative data, a method used to identify, analyze, and report patterns (themes) within data (Braun & Clarke, 2006, 2019). Given the lack of previous qualitative research in children with ADHD and anxiety, TA was appropriate as it allowed researchers to explore and identify patterns evident within the parent-reported data. Free-text responses are a source of valuable data and are suitable for TA (Rich et al., 2013). Qualitative research in the general pediatric population examining experiences of living with either ADHD or anxiety (e.g., Beato et al., 2018; Kandasamy et al., 2019; Laugesen et al., 2016) was not examined in detail prior to analyses in the current study, to reduce the likelihood of such literature influencing the results. An inductive approach ensured results of the current study remained closely connected to raw data and allowed the data parents provided to speak for itself, rather than defined within a pre-determined theoretical framework or prior literature. This analytic approach aligned with the study aim, allowing exploration of common patterns in the experiences parents shared, and to capture novel ideas and insights, as qualitative research has been shown to elucidate critical comments not captured when using purely quantitative surveys (Riiskjær et al., 2012).
Analyses were conducted from a critical realist perspective, which suggests that language gives an understanding about our social realities, with consideration of the possibilities and constraints of our material world (Sims-Schouten et al., 2007). A critical realist approach provided a methodological framework appropriate for the research question, aiming to explore parent-reported experiences, but is not associated with a particular method (Fletcher, 2017). A descriptive theoretical framework was applied, where real-life events are summarized, rather than interpreted beyond what participants provide (Sandelowski, 2000). Semantic, rather than latent coding was applied, with translation to the anticipated audience of clinicians, researchers, and families held in mind. Exploring responses from such a large sample was anticipated to enable comprehensive understanding of experiences, with larger samples typical for free-text analyses (Braun & Clarke, 2013; Braun et al., 2021; Rich et al., 2013).
Qualitative data were exported into Microsoft Excel, in which coding was conducted. Excel was selected as written responses were relatively short in length. A reflexive TA approach was followed (Braun & Clarke, 2019). First, the researcher leading analyses familiarized themselves with the data by carefully reading all items several times, noting initial coding ideas, and getting a sense of the data. This allowed engagement with the complexities of the data and opportunities for reflection by reading actively and considering parent perspectives. The development of initial codes, representing specific, meaningful units in the data, was driven by the data items themselves. This ensured the nuances and richness within the data were retained, though the precise names of some codes evolved as coding progressed. Data coding was conducted in a systematic and inclusive manner, which meant some data were coded in multiple ways to capture the complexities of real participant experiences. Finalized codes were organized into meaningful groupings based on connectedness, with visual mapping of codes then occurring on a whiteboard, to consider conceptual connections. Organizing codes into visual maps to generate various conceptual connections was conducted prior to generating fully realized themes. Mapping codes into various possible conceptual organizations allowed them to be linked in a manner that spoke best to the research question, to present data in a coherent and useful manner (Braun & Clarke, 2006). Following this, themes were generated, with researchers reflecting on the common, underlying patterns evident in the data. Consistent with reflexive TA (e.g., Braun & Clarke, 2019), theme generation is not simply summarizing grouped responses or counting how many times something is reported, but rather articulating the central underlying patterns of shared meaning, to create an in-depth understanding of experiences (Evans et al., 2016; Kidder & Fine, 1987; Silverman, 2000). Research team discussions allowed identification of underlying patterns of meaning contained within the dataset, and review of themes, to ensure key ideas relevant to answering the research question were presented and that themes and patterns remained closely linked to raw data. This also allowed for consideration of relationships between and within themes. Generating and mapping codes, and generating themes, are active and iterative processes, informed by considering the research question and drawing upon researcher subjectivity and reflexivity (Braun & Clarke, 2006, 2019). The final themes contain multiple, conceptually related ideas and closely reflect the dataset, making meaning of participant experiences. Producing theme abstracts (The University of Auckland, n.d.) supported the clarification and definition of themes, including the limits of each. This also supported the process of shaping the overall narrative to answer the research question and produce the report.
The research team met regularly to discuss codes, themes, and possible explanations of the data. The structure of themes and subthemes was refined to ensure a coherent interpretation of the data was provided and did not reflect a single researcher’s perspective. Although some analytic approaches include both qualitative and quantitative elements, reflexive TA does not include coding reliability (Braun & Clarke, 2019). The experience and subjectivity of researchers in this context are seen as a resource and strength of this approach (Clarke & Braun, 2018). Regular discussions allowed consideration of analytic decisions and various perspectives, and supported reflexivity and trustworthiness (Buckingham et al., 2016).
The research team was predominantly female and consisted of quantitative and qualitative researchers, clinical psychologists, a pediatrician, and a provisional psychologist. Inclusion of parents and non-parents promoted consideration of data from both insider and outsider perspectives (Braun & Clarke, 2013). A reflexive journal was utilized as per TA best practice guidelines, enhancing trustworthiness (Braun & Clarke, 2006). This provided the primary author further systematic opportunities for reflection, including documenting decision-making processes, identifying and acknowledging potential researcher biases, enhancing self-awareness when reading and interpreting data, ensuring analyses were conducted rigorously, and reflecting on how the professional and personal backgrounds of research team members may influence analytic processes (Birt et al., 2016). Triangulation was used to enhance the credibility (trustworthiness) of findings (Buckingham et al., 2016; Carter et al., 2014; Noble & Heale, 2019), including integrating findings with anxiety-related experiences in general pediatric samples to consider commonalities and differences (Beato et al., 2018; Kandasamy et al., 2019), investigator triangulation (i.e., inclusion of several researchers), and theory triangulation (i.e., data interpretation from multiple professional perspectives by including different disciplines; Guion, 2002).
Results
Table 1 presents the characteristics for all RCT participants (N = 232), grouped by those who provided qualitative data analyzed in this study (n = 203) and those who did not (n = 29). Compared with parents who did not provide qualitative responses, parents who responded reported more severe child ADHD symptoms, higher life impact from child anxiety, and were more likely to have completed high school and university. No other systematic differences between groups were evident.
Characteristics of Families Included and Excluded in Qualitative Analysis.
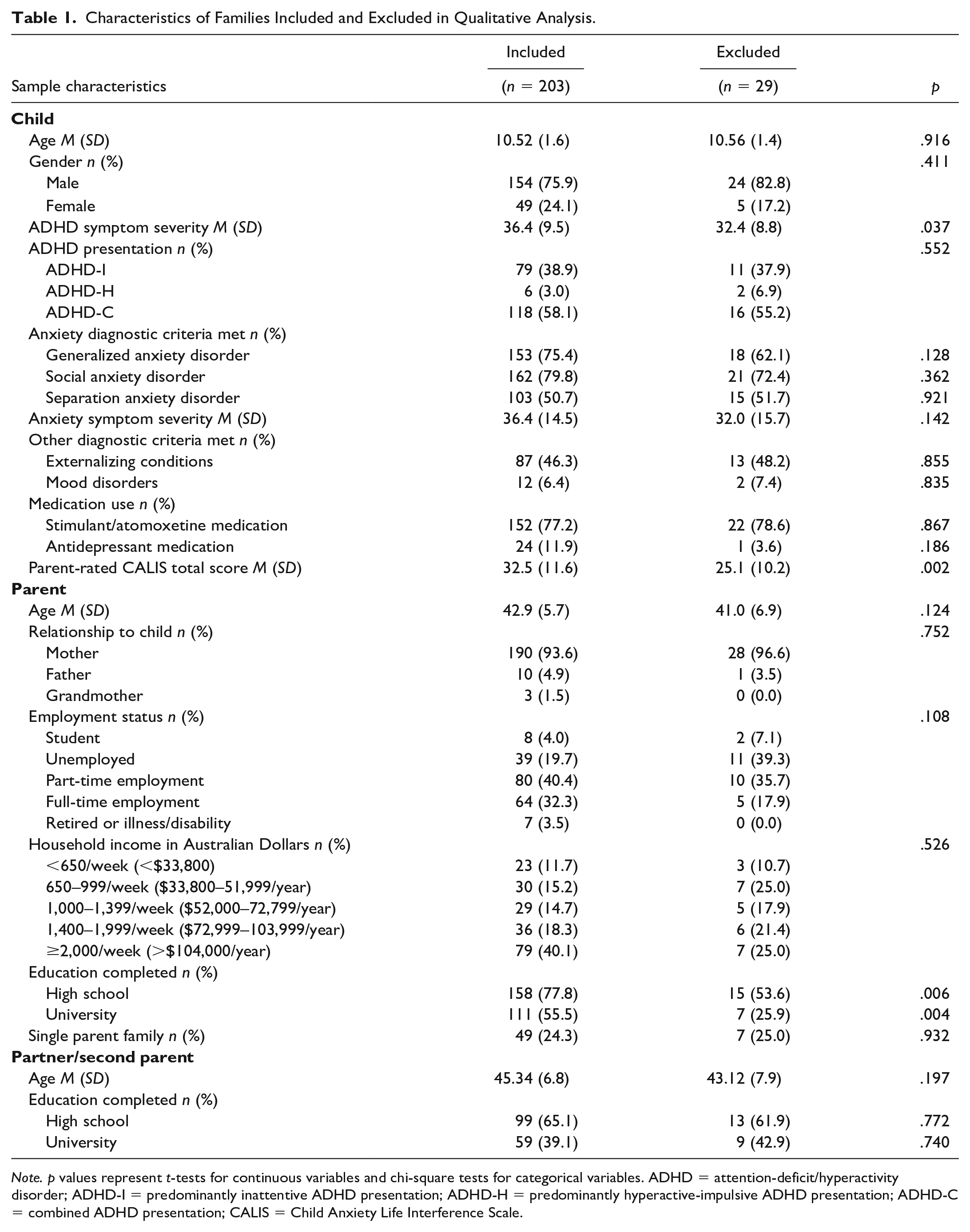
Note. p values represent t-tests for continuous variables and chi-square tests for categorical variables. ADHD = attention-deficit/hyperactivity disorder; ADHD-I = predominantly inattentive ADHD presentation; ADHD-H = predominantly hyperactive-impulsive ADHD presentation; ADHD-C = combined ADHD presentation; CALIS = Child Anxiety Life Interference Scale.
Three overarching themes and within-theme distinctions (i.e., subthemes) were generated. These are summarized in Table 2 and discussed in-text to demonstrate patterns in the data. Additional quotes and summaries are presented in Table 3.
Themes and Subthemes of Impacts Related to Anxiety in Children With ADHD.
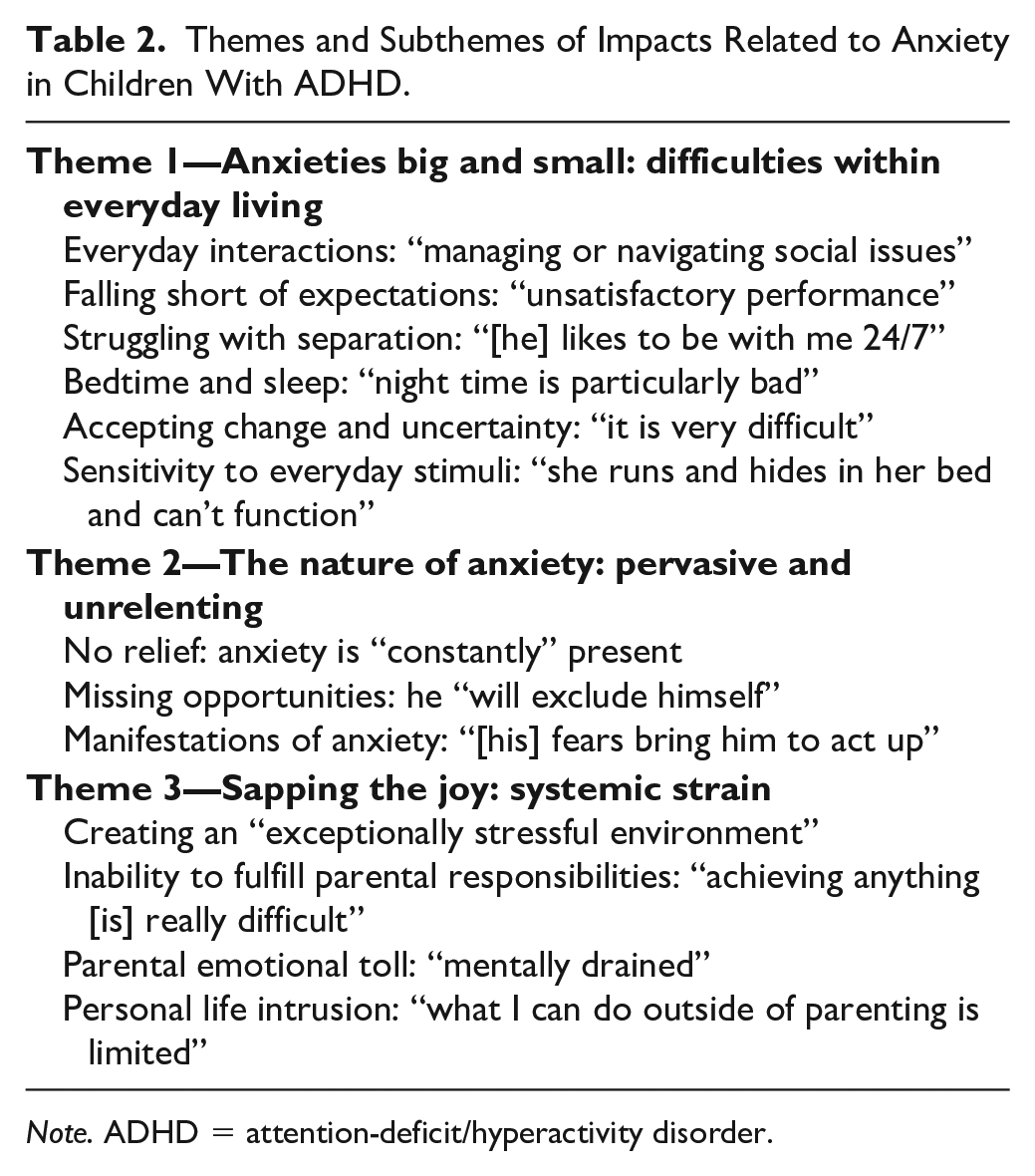
Note. ADHD = attention-deficit/hyperactivity disorder.
Themes and Subthemes of Challenging Situations, Descriptions, and Example Excerpts.
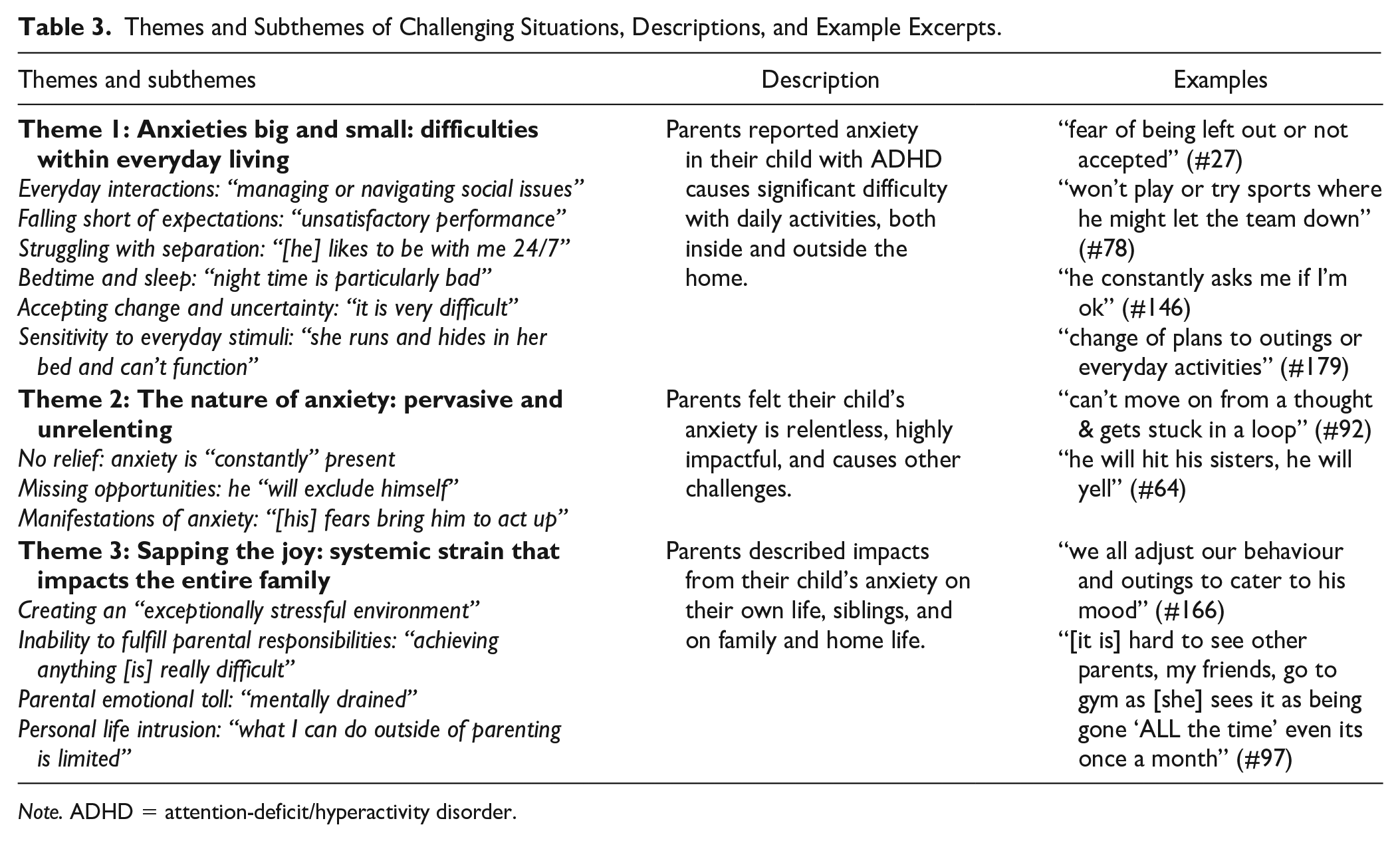
Note. ADHD = attention-deficit/hyperactivity disorder.
Theme 1. Anxieties Big and Small: Difficulties Within Everyday Living
Parents reported the processes involved in everyday activities, both inside and outside the home, to be difficult for their children due to anxiety. School-related challenges were commonly reported, including general concerns regarding “going to school” (#25) (see Note 1) or that “school has always been a problem” (#5), whereas other parents identified specific aspects of school-related processes that were challenging.
Subtheme: Everyday Interactions: “Managing or Navigating Social Issues.”
Interactions at school with peers, including being teased and worrying about being left out, were commonly reported challenges. One parent elaborated that a minor fall-out at school or their child’s fear of being left out “would keep him awake at night” (#27). Social interactions outside the school environment also proved challenging, such as “he gets very worried about parties, and will ask to not go or leave early” (#178) and “not wanting friends over for play dates” (#45).
Subtheme: Falling Short of Expectations: “Unsatisfactory Performance.”
Parents reported their child’s anxiety interferes with their performance at school, including reluctance to ask questions in class and “conducting oral presentations” (#214) in front of others, as well as completing exams. Performance outside classroom settings were challenging too, such as “going to restaurants and ordering” (#152) and “practising new skills like bike riding” (#68). Children worried about letting others down during extracurricular activities, such as “any/all sporting activities including swimming where people might be watching his performance or relying on his teamwork abilities (team sports)” (#93). Parents reported significant challenges with homework, calling it “an epic battle” (#99) that their children avoid “due to worries that it won’t be good enough” (#94).
Subtheme: Struggling With Separation: “[He] Likes to be With Me 24/7.”
Situations involving separation from parents were reported as challenging by many parents, including difficulty leaving the house to buy groceries or going to the toilet without their child, due to their child’s anxiety. These children were reported to be worried “something might happen” (#131) to their parent, with one child reported to refer to their parent as “her security blanket” (#196). Separating from parents to sleep was reported as difficult, with many children refusing to sleep in their own bed, unable to fall asleep without their parent present, and unwilling to stay elsewhere overnight, “because he can’t stand the thought of being away from me if I died or he died during the night” (#49).
Subtheme: Bedtime and Sleep: “Night Time is Particularly Bad.”
Separating from parents was not the only night-time challenge; managing evening routines around bedtime and sleep were widely cited as challenging, with some children so stressed it “often ends up in tears” (#21). Some parents described child bedtime resistance and delaying sleep due to anxiety, “some nights it can take hours to get him finally asleep” (#212). Many parents reported regular overnight waking and difficulty resettling children due to their anxiety, “he cannot calm down” (#31), which can result in the child appearing “shattered in the morning” (#151).
Subtheme: Accepting Change and Uncertainty: “It is Very Difficult.”
Parents reported processes involving transitions and uncertainty left children feeling out of control and anxious, such as engaging in new or unplanned activities, going to unfamiliar places, or “when plans are not kept, or situations change unexpectedly” (#219). Parents reported that children often seek reassurance to quell their anxiety, but that this is rarely effective, “he will continue to ask the questions despite me giving him answers” (#176).
Subtheme: Sensitivity to Everyday Stimuli: “She Runs and Hides in Her Bed and Can’t Function.”
Encountering specific feared or sensory stimuli was challenging for some children, due to anxiety. This included stimuli encountered infrequently, such as “flying” (#126) and “storms” (#212); however, for most, commonly encountered stimuli such as “crowded or noisy places” (#118), car travel, “clothing” (#11), swallowing food and medication, or “toileting” (#79) induced significant child anxiety. Some parents described their child experiencing “extreme anxiety” (#189) or “melt downs” (#226) when encountering anxiety-inducing stimuli, often unable to continue with activities until it is removed.
Theme 2. The Nature of Anxiety: A Pervasive and Unrelenting Threat
The nature and impact of anxiety on children with ADHD was seen to hinder the child’s daily life substantially. Many parents offered insights into their child’s ever-present anxiety, describing how anxiety has led their child to miss opportunities, and manifests as a range of difficult outcomes.
Subtheme: No Relief: Anxiety is “Constantly” Present
Many parents characterized the nature of their child’s “constantly” (#114) present anxiety, saying their child’s anxiety “can be in any situation” (#20), even during “doing general tasks around home [and] just general life” (#39). Parents reported daily tasks, such as eating, toileting, and showering, produced significant levels of anxiety. Some parents listed regular daily situations that triggered their child’s anxiety, with others noting, “it’s not always easy to recognise what the issue is” (#5). Parents commonly reported their child has no break from their pervasive anxiety, stopping their child from engaging in activities “for a couple of days” (#32). For some parents, the anxiety was seen to be so relentless that their child “seems miserable despite having a great life” (#99).
Subtheme: Missing Opportunities: He “Will Exclude Himself.”
Many parents revealed their child forgoes opportunities due to their anxiety, such as “going to fun but unknown activities” (#17), and missing opportunities “because he [is] scared he won’t do well” (#186), with “fear of making a fool of himself stops him joining in” (#156). Avoidance of anticipated anxiety was reportedly responsible for many children missing school camps, play dates with friends, team sports, and other team and family recreational activities.
Subtheme: Manifestations of Anxiety: “[His] Fears Bring Him to Act Up.”
Many parents chose to use this opportunity to describe manifestations of their child’s anxiety, which were clearly challenging for parents to navigate. Often the expression or outcomes of their child’s anxiety was what parents felt made situations challenging and “need[ed] to be managed” (#73), though there was a sense from parents that at times, the behaviors resulting from their child’s anxiety felt out of control. Many parents spoke about their child using violence with siblings and peers when anxious, such as “his fear often turns to anger and he can get aggressive with siblings and friends” (#184). Parents also spoke about physical manifestations, such as “his anxiety builds up over the day and manifests as a migraine” (#7), and “he feels sick constantly” (#128), and noted the detrimental impacts of physical symptoms on their child’s daily life.
Theme 3. Sapping the Joy: Systemic Strain That Affects the Entire Family
The child’s anxiety was described by parents to burden “everyone in the home” (#124) and to cast a shadow over their family’s quality of life.
Subtheme: The Child’s Anxiety Creates an “Exceptionally Stressful Environment” for Everyone Present in the Home
Many parents noted their child’s anxiety affects quality of life in those around the child, including parents, siblings, and the family unit. Many parents expressed how daily life is “draining and stressful for all of us” (#174), describing “there’s a lot of stress in the home and not much calm” (#97) and that their child’s anxiety “causes significant parental and family conflict and distress” (#224). Some parents highlighted conflict with and between parents, with the child’s anxiety seen to be “intruding upon every calm moment” (#174), and the emotional impact on family quality of life prominent, “when he can’t move on from a thought . . . [it] starts to impact family wellbeing” (#92). Families were seen to carry the burden of impacts from the child’s anxiety, “we all adjust our behaviour and outings to cater to his mood” (#166). Many families attempted to compensate for or prevent challenges, such as organizing “separate holidays” (#112) to prevent siblings and parents from missing out altogether. Diverse impacts on siblings were articulated, including conflict and aggression, poor quality relationships, and receiving less attention from parents while they “deal with” (#140) anxiety and related challenges experienced by their child with ADHD.
Subtheme: Inability to Fulfill Parental Responsibilities: “Achieving Anything [is] Really Difficult.”
On a practical level, many parents expressed they struggled to attend to their work, volunteering, and parental responsibilities, including completing routine errands in a timely manner, or at all, as their child’s anxiety “makes achieving anything really difficult” (#13). Parents commonly stated their capacity for paid work is reduced or eliminated due to their child’s anxiety, with others detailing barriers to fulfilling extracurricular responsibilities, such as “going out at night (e.g., parent dinner for school or info evening, being on local kinder committee) . . . Next year I wont do any volunteering because of this, but it will still be hard to [complete essential tasks]” (#97). Parents also reported experiencing impacts from disturbed sleep, “waking up several times a night makes it difficult for me to function” (#31), and acknowledged that their child’s “emotional difficulties like becoming angry or upset that can impact others and take time to resolve” (#205).
Subtheme: Parental Emotional Toll: “Mentally Drained.”
Many parents articulated their child’s anxiety elicits strong emotional responses from themselves, such as an “escalation from calm persuasion through to screaming frustration” (#174), in response to their child’s anxiety. Parents reported the anxiety “gets me really frustrated” (#8), as “he is often too scared to try [new things], which causes massive frustration and some anger” (#107). Many described feeling guilty when their child is distressed when separating from them, or in general; this led some parents to “get very upset” (#3) and doubt their parenting, “are we doing enough to support him at home” (#103). Many parents spoke about carer fatigue or burnout, “feel like I don’t stop” (#105), “I often feel too mentally drained to enjoy outings so we stay home” (#125), and “I can become overwhelmed with his constant demands for answers of the same questions” (#176).
Subtheme: Personal Life Intrusion: “What I Can Do Outside of Parenting is Limited.”
Many parents spoke about their own lost opportunities for recreation due to their child’s anxiety, “we have no evening to relax” (#151). Many noted the impossibility of “a weekend away with my husband” (#14) or going away “with close friends as [my child] would not cope” (#95). A lack of “family support or extended family” (#187) limited non-parenting activities for many, whereas for others, the challenge was not a lack of support, but that their child would not cope with other carers, “it’s very difficult to find anyone to babysit her what I can do outside of parenting is limited” (#145). Parents described lost friendships, hobbies, and opportunities in their own lives, noting how attending to their child’s needs had compromised their personal identity, friendships, hobbies, and romantic relationships.
Discussion
This qualitative study aimed to advance understanding of parent-reported situations that are challenging due to anxiety in children with ADHD. The results describe situations that are commonly challenging for children with ADHD and their families. Patterns in the parent-reported data were generated into themes, producing three central ideas that detail the anxiety-related difficulties experienced by these children in everyday processes and activities that they regularly encounter; the pervasive and relentless nature of the anxiety; and the consequences of the child’s anxiety on their whole family. Subthemes characterize important within-theme distinctions and demonstrate nuances in the dataset. These findings provide a comprehensive picture of daily experiences, beyond what previous studies have established using structured rating scales.
Findings in the current study suggest the impacts of co-occurring anxiety in children with ADHD are evident in everyday life and significantly interrupt their ability to engage with a range of activities. This extends upon previous research that has shown that co-occurring anxiety exacerbates challenges for children with ADHD (Gould et al., 2018; Halldorsdottir & Ollendick, 2014; Sciberras, Efron, & Patel, 2019) and may help in understanding the nature and impact of the additional difficulties established in prior studies. Extending upon previous research that reported co-occurring anxiety can exacerbate ADHD symptoms (Tsang et al., 2015), anecdotes in the current study provide firsthand examples of challenges due to anxiety. Children of parents in the current study were reported to contend with difficulties in many or all daily activities due to their anxiety, including separation from parents, everyday social interactions, and asking questions in classroom settings. It is remarkable to consider that the difficulties reported in this study, while impairing in their own right, occur in addition to those already posed by ADHD and associated challenges (e.g., lower academic performance and more peer difficulties for children with ADHD, compared with peers without ADHD; Efron et al., 2014). To our knowledge, the current study represents the first opportunity this population have had to share their experiences of co-occurring anxiety in an open-ended way. Parents reported consequences of their child’s anxiety extends far beyond the child themselves, impacting the whole family and intruding upon everyday family interactions, activities, and quality of life. Although some of these challenging situations may be age-appropriate and common among a wider population of same-age peers, activities occurring every day or otherwise regularly can present significant challenges for these children and families.
Many parents articulated impacts on the siblings of children with co-occurring anxiety and ADHD, including receiving less parental attention and/or quality family time, being involved in or victim to sibling violence, and being subject to stressful home environments. Little research explores impacts on siblings, with previous studies of children with ADHD and anxiety appearing to have had limited scope to investigate sibling impacts. Considering impacts on siblings and parents is important to optimize the support system around the child, prevent carer burnout, and minimize other difficulties within the family, particularly given families are commonly involved in supporting child difficulties (Wei & Kendall, 2014). Past literature has reported children with ADHD and their siblings experience reduced quality of life (Peasgood et al., 2016), however, supports for siblings of children with ADHD remain largely unexplored. The current findings demonstrate the importance of considering sibling needs when working with children with ADHD and their families.
The impacts reported by parents in this study on family quality time their capacity to complete parental responsibilities align with previous literature that suggested parents of children with ADHD can feel less competent, experience more parenting stress, and experience increased mental health difficulties, compared to parents of children without ADHD (e.g., Humphreys et al., 2012; Pfiffner & McBurnett, 2006; Van der Oord & Daley, 2015). By using a qualitative approach, we extend these previous findings in a novel manner, to consider the impact of both ADHD and anxiety from family perspectives, to generate rich descriptions of specific impacts within the family environment in a large sample of parents, that would not have been possible by examining quantitative scores only. Although literature from the wider pediatric population has noted a small number of individuals who mentioned negative family impacts related to child anxiety (Beato et al., 2018; Kandasamy et al., 2019), this has not been a key theme, which contrasts with the current study, in which parents commonly voiced substantial negative impacts on themselves, their child’s siblings, and the family unit. Moreover, some parents in the earlier general population studies reported their child’s anxiety does not have negative impacts, or that it leads to benefits (e.g., enhancing school performance/results; Beato et al., 2018). In contrast, parents in our sample did not report positive or neutral experiences, though this may be attributable to the wording of the survey question.
Previous literature has recommended clinicians screen children with ADHD for anxiety (e.g., Maric et al., 2018; Tsang et al., 2015). The current study reiterates the importance of this and extends this recommendation by highlighting the need for clinicians, families, and teachers to understand that the challenges these children regularly face are substantial; and importantly, that the whole system around children with ADHD and anxiety are affected, every day, in many or all activities. These factors should be considered when planning supports, to optimize outcomes for both children with ADHD and those around them. Family supports should be explored by clinicians in contact with children with ADHD and anxiety, including asking parents about their own coping if feasible (e.g., impacts on parent mental health, support for themselves, strategies to support siblings). Furthermore, given the high heritability of anxiety and ADHD, it is important to consider how supports can engage with parents who may also experience ADHD and/or anxiety, and how integration with adult support services can occur (Thapar et al., 2013).
By providing detailed insights from parents about the difficulties experienced by children with ADHD and anxiety, this study extends upon existing literature by demonstrating the significant impacts in daily activities that these children face every day, articulated by families themselves. These difficulties need to be recognized by those around the child, including parents, teachers, and clinicians. The descriptions provided by parents may help others to understand the function of some behaviors. For example, “tantrums” may at times reflect a manifestation of underlying anxiety, rather than oppositionality. Children should be referred for supportive intervention as early as possible to minimize the risk of ongoing and future anxiety and other conditions that commonly develop in instances of untreated anxiety, such as depression (Kendall et al., 2010). There is preliminary evidence that using adapted cognitive-behavioral strategies to treat anxiety in children with ADHD reduces the proportion of children meeting criteria for an anxiety condition (Costin et al., 2002; Gould et al., 2018; Houghton et al., 2017; Sciberras et al., 2018). The sample in the current study participated in a larger RCT targeting anxiety in children with ADHD (Sciberras, Efron, Patel, et al., 2019), the results from which will be available shortly
This study had a number of strengths. To our knowledge, this is the first qualitative exploration of the impacts of anxiety in children with ADHD. Although structured rating scales have previously rated anxiety-related difficulties, this study offered families the opportunity to express their unfiltered views without being restricted to the existing items in rating scales, allowing parents to use evocative or descriptive language and to write as much as they would like, to communicate their difficulties. In reading the data, researchers gained a sense of their experiences and imagine their daily challenges, with some participants having chosen to write extensive descriptions of the challenges their family encounter, often with little support. These findings represent a comprehensive summary of experiences in the everyday terms of those events, and are of use to understand the difficulties this population face more clearly. In addition, this study included comprehensive assessment of ADHD, anxiety, and other co-occurring conditions, using psychometrically sound measures, in a relatively large sample. Furthermore, the research team composition of clinicians, researchers, a pediatrician, and a provisional psychologist, provided opportunity to approach the data through both a qualitative lens and include team members with clinical experience. This facilitated rich discussions around consistency between parent reports and team members’ clinical experience, and an openness to further insights, such as the reported impacts of anxiety in children with ADHD on others around them. As efforts to develop tailored interventions to support this population continue, this study reinforces the need to carefully consider the system around children with ADHD, to ensure the intended consumers of interventions are heard, and interventions are effective (Evans et al., 2016). Inductive analysis allowed this study to give a voice to parents with firsthand experience, rather than what researchers may have pre-empted. These observations lend themselves to the growing recognition that rigorous and systematic qualitative approaches can contribute substantially to child and adolescent research (Bassett, 2010), including enhancing understanding of daily challenges this population encounter.
This study should also consider some limitations. No self-reported information was available from children on the qualitative measure of interest, and most participants were mothers. Although some studies have reported discrepancies between child- and parent-reported anxiety ratings (Niditch & Varela, 2011), and that using multiple informants is ideal where possible (Spence, 2018), psychometric evaluation of the CALIS has shown significant inter-rater reliability between mother-, father-, and child-reported quantitative ratings of impact and interference due to child anxiety (Lyneham et al., 2013). Furthermore, using the parent-reported data allowed insights not only regarding child impacts but also enhanced understanding of impacts on parents, siblings, and broader family life (Lyneham et al., 2013). Future research could build upon the current findings with qualitative perspectives from children and fathers (which could differ from mothers’ perspectives; e.g., Beato et al., 2018), and inclusion of families with diverse sociocultural backgrounds, as experiences may vary (Slobodin & Masalha, 2020). Although the survey format used in this study did not allow researchers to clarify responses with follow-up questions, probing and prompting are not warranted to generate meaning from the data (Braun & Clarke, 2019). Furthermore, examination of free-text data afforded a large sample from this population an opportunity to provide novel and meaningful contributions, without requiring more burdensome data collection methods. The value of free-text survey approaches should not be discounted, as they can capture a diversity of perspectives, experiences, and sense-making, while ensuring participant anonymity, and reducing social desirability and interviewer bias (Braun et al., 2021; Rich et al., 2013; York et al., 2011). It cannot be assumed the difficult situations identified are exhaustive, as participants were asked to provide examples. Furthermore, data are limited to descriptions of challenging situations, rather than interpretive reflections on the lives of the child and others. For example, no parents mentioned stigma, responses from outside the family related to the child’s anxiety, or the interplay between the child’s ADHD and anxiety, though this may be attributable to how the question was worded. The descriptive-type research question guiding the analysis was proposed intentionally, with the needs of the intended audience in mind, for example, psychologists, pediatricians, and families (Sandelowski, 2000). Although this study did not ask parents explicitly about the interplay of ADHD and anxiety, future research could utilize alternative methods (e.g., interviews, focus groups) to explore this in-depth. Although more onerous, such approaches may complement the current study’s insights by providing opportunities for probing, prompting, and member checks (Birt et al., 2016). Clarifying further the interaction between ADHD and anxiety may assist in identifying specific intervention opportunities, potential treatment barriers related to the influence of both ADHD and anxiety, and modifications to overcome these.
The children of participants in this study were identified from clinical samples and had relatively severe ADHD symptoms, thus their experiences may not represent those of all children with ADHD and anxiety. However, the descriptive TA approach used in this study does not seek to provide a complete summary of all experiences, but rather, to provide valuable insights that clinicians and researchers can consider regarding potentially helpful supports for this population. Data were read with the knowledge that the children of participants met diagnostic criteria for ADHD plus one or more anxiety conditions, though these may not have been diagnosed. Furthermore, most members of the research team had training and experience in childhood clinical settings and practice. These factors may mean data were read through a diagnostic lens. To reduce bias, research team members with specialist ADHD and/or childhood anxiety knowledge did not lead the analysis, and team discussions were conducted regularly to question analytic interpretations and explore possible alternative explanations, to ensure results do not reflect a single researcher’s perspective.
This study contributes to a richer understanding of the challenges faced by children with ADHD and anxiety. Children with anxiety and ADHD may experience pervasive and relentless impacts due to their anxiety, and thus require timely and appropriate assessment and support, as well as consideration of the needs of those around them. The findings reiterate the need for clinicians to provide anxiety-targeted supports for children with ADHD and anxiety, and their families.
First qualitative examination of daily impacts of anxiety in children with ADHD
Everyday processes and activities can be difficult for children with ADHD and anxiety
Anxiety in children with ADHD is pervasive, unrelenting, and affects their opportunities
Parents and siblings of children with ADHD and anxiety are affected substantially
Identifying anxiety in children with ADHD and providing targeted support should be prioritized
Footnotes
Acknowledgements
The authors would like to thank all families involved in this study for their contributions.
Declaration of Conflicting Interests
A/Prof. Sciberras receives royalties from her book published through Elsevier: Sleep and ADHD: An Evidence-Based Guide to Assessment and Treatment. All other authors have no conflicts of interest to declare.
Funding
This project was funded by the National Health and Medical Research Council (NHMRC) of Australia (1106427) and the Sidney Myer Fund and Myer Foundation. A/Prof. Sciberras is funded by an NHMRC Career Development Fellowship (1110688: 2016–21) and Veski Inspiring Women’s Fellowship. The Murdoch Children’s Research Institute is supported by the Victorian Government’s Operational Infrastructure Support Program.
Ethical Approval
This study was approved by the Royal Children’s Hospital Melbourne Human Research Ethics Committee (HREC; 35164) and Deakin University HREC (2016-387).