
Abstract
Background
Young autistic people often experience social isolation and loneliness. Despite social isolation and loneliness increasing in later life in non-autistic populations, no studies have examined whether middle-aged and older autistic adults are at an increased likelihood of these experiences.
Methods
428 adults (autistic n = 265) aged 40–93 years (mean = 60.5 years) completed questionnaires related to social connectedness/isolation, loneliness, and mental health. Group differences and associations were examined.
Results
The autistic group was less socially connected and lonelier than the non-autistic group. While there were few gender differences in social connectedness, women were lonelier than men in both groups, including when controlling for age and mental health. Social connectedness decreased with age in both groups, loneliness only increased with age in the autistic group. For both social connectedness and loneliness, age associations were significantly stronger in men than women.
Conclusions
Autistic adults may be particularly susceptible to social isolation and loneliness in midlife and older age. While autistic women were lonelier than autistic men, autistic men may be at greater risk of increasing social isolation and loneliness with older age. This study highlights the need for evidence-based interventions to address social isolation and to reduce loneliness for autistic people as they age.
Introduction
Social isolation and loneliness are growing public health concerns. Although the terms social isolation and loneliness are frequently used interchangeably, they are distinct experiences (Fakoya et al., 2020). Social isolation is a multidimensional concept, defined as the objective lack of social connectedness and interactions with family members, friends, or the wider community (Valtorta & Hanratty, 2012). Loneliness is widely referred to as a subjective negative feeling associated with a perceived lack of a wider social network or absence of specific desired companions (Valtorta & Hanratty, 2012).
Social isolation and loneliness are significant determinants of poor mental and physical health in the general population, being consistently associated with adverse effects on mental health and cardiovascular outcomes, including depression, dementia, suicide, and increased all-cause mortality (Leigh-Hunt et al., 2017). While social isolation and loneliness can occur at any age, they become increasingly common experiences in older age (Fakoya et al., 2020; Victor et al., 2000). Older people are more likely to be exposed to risk factors that can lead to or exacerbate experiences of social isolation and loneliness including retirement, bereavement, living alone, and deteriorating health and chronic illness (Donovan & Blazer, 2020). Recent estimates have suggested that one in five older adults in the UK have little or no social contact each week (Age UK, 2019). Despite this, little research has been conducted to examine whether these experiences are found in middle-aged and older autistic populations (Mason et al., 2022; Umagami et al., 2022).
Examining experiences of social isolation and loneliness in autistic midlife and older age is an important topic, as people ageing on the autism spectrum may be particularly vulnerable to these experiences (Umagami et al., 2022). Autistic people often experience barriers to being socially connected; for example, autistic adults tend to have fewer opportunities for social interaction, including being less likely to be in a relationship, being less independent, and having lower rates of employment (Mason et al., 2020). Autistic adults also report experiencing high levels of social stigma, which can act as one of many barriers to making and maintaining friendships (Crane et al., 2018; Sasson et al., 2017). Despite these barriers having an impact across the lifespan, existing research on social isolation and loneliness have predominately focused on autistic children, adolescents, and younger adults. These studies have reported that autistic young people often have smaller social networks, poorer friendship quality, and experience loneliness more intensely and frequently compared to their non-autistic peers (Bauminger & Kasari, 2000; Locke et al., 2010; Umagami et al., 2022). Social relationships are also perceived and experienced differently across genders. In a mixed-methods study, Sedgewick et al. (2016, 2018) examined gender differences in social motivation and friendship experiences of autistic girls and boys and their non-autistic peers. Autistic boys reported having qualitatively different friendships (i.e., less intimate) and were rated as having less motivation for and interest in social contact compared to autistic girls and the non-autistic boys and girls. This points towards possible gender differences in experiences of isolation and loneliness in adulthood, where autistic women are more socially motivated/better socially connected but could be more susceptible to feelings of loneliness than autistic men.
An emerging body of literature suggests that social isolation and loneliness may indeed persist into later adulthood in autistic populations. In a recent systematic review of 34 articles on loneliness in predominately younger and middle-aged autistic adults, Umagami et al. (2022) concluded that autistic adults often long for connection, and commonly experience more feelings of loneliness than non-autistic adults. The authors highlight numerous gaps in the literature, including that loneliness was primarily examined as part of broader research questions, that many studies did not include a non-autistic comparison group, and that most participants were in early to middle adulthood. A study by Charlton et al. (2023) further documented the subjective sense of being socially supported and its link with quality of life in their sample of over 350 autistic adults aged 40–83 years. Charlton et al. (2023) found that social support is an important predictor of physical, psychological, social, and environmental quality of life for middle-aged and older autistic people.
To date, only a few studies have examined loneliness among middle-aged and older autistic people. In a mixed methods study, Ee et al. (2019) examined self-report questionnaire and open-text response data from the ‘Australian Longitudinal Study of Adults with Autism’ cohort. The sample included 220 autistic adults aged 25–80 years (mean age = 42 years) and 146 non-autistic peers. While this study did not specifically examine the experiences of their middle-aged and older autistic participants, they report that the autistic group had significantly higher loneliness scores than the comparison group. Additionally, they note that having an autism diagnosis was the greatest predictor of feelings of loneliness (accounting for 38% of the variance, over-and-above the influence of social skills, anxiety, and depression) in their combined sample. Furthermore, their qualitative analyses indicated that autistic adults face many barriers to socialisation including social communication difficulties, environmental factors (i.e., noise), and negative past experiences. In a small-scale qualitative study by Elmose (2020), focus group and individual interview data from 25 autistic adults aged 18–71 years (72% men, no mean age provided) was thematically analysed. Findings suggest that autistic adults’ loneliness occurred, as expected, due to discrepancies between their desired and actual social relationships. Although Ee et al. (2019) and Elmose (2020) included middle-aged and older adult participants, they did not specifically address older age or changes/associations with age in their qualitative analyses. To the present authors’ knowledge, only one study has specifically focused on the later life social experiences of autistic people; a qualitative study by Hickey et al. (2017) thematically analysed semi-structured interviews with 13 autistic adults aged 51–71 years (mean age = 60 years). Participants revealed that they longed for social connection, and struggled with isolation and loneliness (as well as poor mental health) throughout adulthood and older age.
In summary, recent empirical evidence suggests that social isolation and loneliness are challenges that autistic adults of all ages face. The goal of this study is to build on this emerging body of literature as there are few quantitative studies that examine either social isolation or loneliness in middle-aged and older autistic adults specifically. The current study examined differences in the experiences of social isolation and loneliness among middle-aged and older autistic adults compared with an age- and gender-matched non-autistic comparison group. The effect of gender, symptoms of depression, and anxiety on social isolation and loneliness are also explored. Symptoms of depression and anxiety were included as covariates due to autistic people often experiencing these problems. Depression and anxiety are associated with negative self-appraisal, which could lead to more negative self-reporting of problems. Previous studies (e.g., Ee et al., 2019; Hickey et al., 2017) also highlight their relationship with social isolation and loneliness.
It is hypothesised that (1) the autistic group will be less socially connected (i.e., being more socially isolated) than the non-autistic comparison group, as measured by frequency of contact, availability of help and support, and having confiding relationships with family members and friends. The autistic group will also (2) report more feelings of loneliness than the non-autistic comparison group. When considering gender, men will report being more socially isolated and women will report more feelings of loneliness in both autistic and non-autistic groups, but this gender difference will be larger in the autistic group. That (3) low social connectedness and loneliness will be associated with each other in similar ways in the autistic and non-autistic groups. Finally, when considering age, (4) social isolation and loneliness will be associated with older age in both autistic and non-autistic groups, but the strength of the age association will be stronger in the autistic group.
Method
Study design and participants
This study uses cross-sectional data from the ‘AgeWellAutism’ study, an online survey exploring ageing on the autism spectrum. Prior to the commencement of the study, patient and public involvement (PPI) interviews were conducted; in total 12 middle-aged and older autistic adults were asked in one-on-one interviews (conducted via telephone, email, and instant messaging) what are the key factors that influence their quality of life as they are getting older. The research team then created the AgeWellAutism study survey to address the topics that arose (e.g., mental health, social support networks, and other topics not included in the current study). The survey was then given to three members of the PPI group to give feedback on the content, language use, and accessibility of the survey, however, further PPI was not conducted in the interpretation or dissemination of the current study. PPI members were provided with £20 Amazon gift vouchers for their participation in the interview and for their feedback on the survey.
The AgeWellAutism study was conducted in Spring 2019. Participants were recruited through study adverts on social media (e.g., Twitter, Facebook, Reddit), existing participation databases held by the authors, through recruitment notices on Autistica's Research Network, and advertisements to older adult residential communities. Inclusion criteria for the study were: being 40 years of age or older, having access to an internet-enabled device, and being able to read English. The study had no specific exclusion criteria. Participants accessed the survey via Qualtrics. Prior to beginning the survey, a full information sheet was presented which detailed the aims and objectives of the study. Participants gave informed consent and were reminded on their right to withdraw at any time. Participants were then presented with a series of standardised questionnaires that explored a variety of topics, for example, their health, social experiences, sleep, and quality of life. All questions prompted a response if missed. Upon completion, participants were presented with a full debrief sheet, including links to a range of support services. Participants were entered into a raffle to win one of twenty £20 Amazon gift vouchers. All responses were checked for possible spam participants. Full ethical approval was received for this study through the PNM Research Ethics Subcommittee at King's College London (HR-18/19–10941). The study was not pre-registered.
In total, 502 completed surveys were recorded, of which 70 were removed due to suspected spam (i.e., very short completion times and/or irregular responses to open-text questions, such as repeating the question text or nonsensical text). This resulted in a final total of 432 participants aged 40–93 years completing the online survey. Participants who disclosed that they either had an autism diagnosis (n = 254) or self-identified as autistic (n = 11) formed an autistic group (total autistic n = 265). The autistic group were asked when they received their autism diagnosis/began to identify as autistic; responses ranged from the current year to 43 years ago as a child (mean years since diagnosis = 10.3 years, 17 (6.4%) of sample diagnosed under 18 years of age). The remaining participants formed a non-autistic comparison group (total non-autistic n = 167). Groups were matched on age (autistic mean age = 60.6 years; non-autistic mean age = 60.5 years) and gender ratio (autistic group men % = 46.8%; non-autistic group men % = 50.3%). The groups were also comparable in education level. Some group differences were found in demographic characteristics, specifically, autistic participants reported lower rates of employment, and were more likely to live with non-marital family members. Specific data on race/ethnicity and socio-economic status were not recorded. See Table 1 for demographic characteristics of the autistic and non-autistic groups.
Demographic characteristics of the autistic and non-autistic groups.

Note. Effect size calculated using Cohen's d or Cramer's v. nb/t = non-binary, transmen and transwomen.
* p < .05, ** p < .01, *** p < .001.
Materials
Demographic characteristics – Participants provided detailed demographic information including age, gender, education level, employment status, and living situation.
Social Connectedness and Isolation – Participants reported their experiences of social connectedness using the six-item self-report Lubben Social Network Scale (LSNS-6; Lubben et al., 2006). The LSNS-6 has two subscales that explore social integration and support access availability from (a) family members and (b) friends. Using a six-point scale (ranging from ‘none’ to ‘nine or more’) to indicate the number of family members/friends the question would apply to, the measure asks (1) ‘How many [family members/friends] do you see or hear from at least once a month?’, (2) ‘How many [family members/friends] do you feel at ease with that you can talk to about private matters?’, and (3) ‘How many [family members/friends] do you feel close to such that you could call on them for help?’ Scores are totalled for each subscale for a family member total and a friend total, as well as an overall combined total score. High scores indicate the individual has good social integration and support access, while low scores suggest the individual may be socially isolated with poor support access. The LSNS-6 has been widely used in older non-autistic adult populations and has high internal consistency and stable factor structure (Lubben et al., 2006). To the authors’ knowledge, the psychometric properties of the LSNS-6 have yet to be examined in autistic populations of any age. In the current sample, the internal consistency of the LSNS was very good in the autistic group (Cronbach's α = .83) and excellent in the non-autistic group (Cronbach's α = .93).
Loneliness – Symptoms of current loneliness were measured using the 20-item self-report UCLA Loneliness Scale (UCLA-LS3; Russell, 1996). The UCLA-LS3 uses a 4-point scale (1 = never to 4 = always), and asks a range of questions related to the individual's dissatisfaction with their current social relationships (e.g., ‘How often do you feel alone?’; ‘How often do you feel that your relationships with others are not meaningful?’; ‘How often do you feel that there are people you can talk to?’). Scores are totalled (range 20–80), with higher scores indicating greater loneliness. The UCLA-LS3 has been widely used in older non-autistic adult populations and has high internal consistency and stable factor structure (Russell, 1996). The UCLA-LS3 has good internal consistency in the autistic adult population (Cronbach's α = .90) and autistic adults tend to prefer the UCLA-LS3 over other widely used measures of loneliness such as the Social and Emotional Loneliness Scale for Adults (SELSA) (Grace et al., 2023). In the current sample, the internal consistency of the UCLA-LS3 was very good in both autistic (Cronbach's α = .87) and non-autistic groups (Cronbach's α = .86).
Depression – Symptoms of depression were measured using the Patient Health Questionnaire (PHQ-9; Kroenke et al., 2001). The PHQ-9 is a nine-item questionnaire with a 4-point scale which ask the participant to report whether they have been bothered by a range of problems over the past two weeks such as anhedonia, low mood, sleep problems, fatigue, poor appetite or weight change, concentration difficulty, psychomotor disturbance, and suicidal ideation. Using the conventional cut-off score of ≥10, the PHQ-9 has a sensitivity of 88% and a specificity of 88% for major depressive disorder. The PHQ-9 has been validated with autistic adults (Arnold et al., 2020).
Anxiety – Symptoms of anxiety were measured using the General Anxiety Disorder questionnaire (GAD-7; Spitzer et al., 2006). The GAD-7 is a seven-item questionnaire with a 4-point scale which asks the participant to report whether they have been bothered by a range of problems over the past two weeks such as nervousness, uncontrollability of worrying, issues relaxing, restlessness, and irritability. Using the conventional cut-off score of ≥10, the GAD-7 has a sensitivity of 89% and a specificity of 82% for generalised anxiety disorder. To the authors’ knowledge the psychometric properties of the GAD-7 have yet to be examined in autistic populations of any age. In the current sample, the internal consistency of the GAD-7 was acceptable in both autistic (Cronbach's α = .78) and non-autistic groups (Cronbach's α = .74).
Data analysis
All statistical analyses were performed using SPSS (version 25.0; IBM Corp., 2017). To examine group differences (autistic group vs. non-autistic group) in demographic characteristics, t-tests and chi-square (χ2) analyses were used for continuous and categorical variables, respectively.
To examine group differences (autistic group vs. non-autistic group) in social connectedness ratings, χ2 analyses were used. Additional χ2 analyses were used to examine gender and group differences in the social connectedness ratings (gender: men, women; vs. autism group: autistic, non-autistic). Adjusted residual values were examined to identify statistical differences in the proportions/ratings.
To examine group differences (autistic group vs. non-autistic group) in loneliness, depression, and anxiety scores, t-tests were used. χ2 analyses (autistic group vs. non-autistic group) were also used to examine frequencies of participants passing cut-off scores in depression and anxiety symptoms. Analysis of variance (ANOVA) was used to examine main effects of gender and group, as well as any interaction between gender and group, in loneliness, depression, and anxiety scores. Analysis of covariance (ANCOVA) was used to examine group differences (autistic group vs. non-autistic group) in loneliness scores, when accounting for depression and anxiety scores, and for the influence of living alone.
To examine associations between (A) connectedness and loneliness and (B) age and other variables (i.e., connectedness, loneliness, depression, anxiety), bi-variate correlation analyses were used within each group (i.e., autistic group only, non-autistic group only), with Fisher's r-to-z transformations used to test for differences in correlation coefficients between the autistic and non-autistic groups. Within-group correlations and between-group comparisons were selected due to the hypothesised autistic versus non-autistic group differences in the study variables.
Multiple comparisons were controlled for using the false discovery rate (FDR) method (Benjamini & Hochberg, 1995), with an initial α-value of 0.05 being used. FDR was applied to all p-values, with adjusted α-values being assigned based on the p-value rank. The final α-value after FDR was applied was 0.039.
Results
Social connectedness – frequency of contact
The autistic group reported being in contact with significantly fewer family members and friends each month compared to the non-autistic group. The effect size of these differences were large (family v = .55, friends v = .58). When considering the number of participants who may be socially isolated, 18% of the autistic group had no contact with their family members over the past month compared to 4% in the non-autistic group. Additionally, 28% of the autistic group had no contact with friends over the past month compared to 8% in the non-autistic group. When family member and friend contact is combined, 11% of the autistic group and 4% of the non-autistic group had no contact within the past month. See Table 2 for social connectedness responses.
Number of family members and friends reported by autistic and non-autistic groups.

A significant difference in adjusted residual values between cells.
***p < .001.
A gender and group difference (explored using χ2 analyses) was found in the distribution of ratings made by autistic men and women regarding their contact with friends (χ2 = 11.93, p = .036). Comparison of adjusted residual values indicated that more autistic men were in contact with ‘three or four’ friends than autistic women (18% vs. 6%). The effect size of differences in these ratings were small (v = .21). No other gender and group differences were found in family or friend contact. Due to the small number of non-binary/trans/genderfluid participants (n = 4), comparisons with this group were not made. See Supplemental Tables S1 and S2 for social connectedness responses by gender.
Social connectedness – confiding relationships
The autistic group reported significantly fewer family members and friends that they could talk to about private matters compared to the non-autistic group. The effect sizes of these differences were large (family v = .58, friends v = .52). When considering the number of participants who have no confiding relationships, 27% of the autistic group had no family members they could talk to about private matters compared to 4% in the non-autistic group. Additionally, 13% of the autistic group had no friends that they could talk to about private matters compared to 1% in the non-autistic group. When family member and friend contact is combined, 7% of the autistic group and nobody in the non-autistic group had no one they could talk to about private matters. See Table 2 for social connectedness responses.
A gender and group difference was found in the distribution of ratings made by the autistic men and women regarding having confiding relationships with friends (χ2 = 11.26, p = .046). Comparison of adjusted residual values indicated that more autistic women had confiding relationships with ‘two’ friends compared to autistic men (31% vs. 21%), and more autistic men had confiding relationships with ‘three or four’ friends than autistic women (23% vs. 10%). However, the effect size of these differences were small (v = .21). No other gender and group differences were found in confiding relationships with family or friends. See Supplemental Tables S1 and S2 for social connectedness responses by gender.
Social connectedness – availability of help/support
The autistic group reported significantly fewer family members and friends that they could rely on for help/support compared to the non-autistic group. The effect sizes of these differences were large (family v = .54, friends v = .45). When considering the number of participants who have nobody to rely on for help/support, 11% of the autistic group had no family members they could ask for help/support from compared to 1% of the non-autistic group. Additionally, 14% of the autistic group had no friends they could ask for help/support compared to 1% of the comparison group. When family member and friend contact is combined, 6% of the autistic group and less than 1% of the non-autistic group had no one they could turn to for help and support. See Table 2 for social connectedness responses.
A gender and group difference was found in the distribution of ratings made by autistic men and women regarding their availability of help/support from family (χ2 = 13.22, p = .010). Comparison of adjusted residual values indicated that more autistic women had help/support from ‘one’ family member than autistic men (39% vs. 19%), while autistic men had more help/support from ‘two’ family members than autistic women (43% vs. 31%). However, the effect size of this difference was small (v = .16). No other gender and group differences were found in family or friend help/support availability. See Supplemental Tables S1 and S2 for social connectedness responses by gender and group.
Social connectedness – associations with age
When combining the family and friend scales of the social connectedness measure into a total combined score, social connectedness significantly decreased with age for both the autistic and non-autistic group. These associations were small-to-moderate in the autistic group (rs = −.22 to −.42 for family items, rs = −.26 to −.41 for friend items) and moderate in the non-autistic group (rs = −.45 to −.48 for family items, rs = −.41 to −.54 for friend items). The strength of these associations were found to differ between the autistic and non-autistic groups, with the strength of the association in the non-autistic group being significantly more strongly negative with age for confiding family relations, family help/support, and friend confiding (zs = 2.06 to 3.20). This suggests that the non-autistic group may have a greater reduction in their social connectedness with increasing age, compared to the autistic group who are less socially connected throughout middle and older age. See Table 3 for correlations. See Figure 1 for visualisations of these age associations.

Scatter plots of age associations by group.
Correlations by group between age and social connectedness items, and loneliness, depression, and anxiety total scores; and fisher's r-to-z transformation for comparison of coefficients by group.
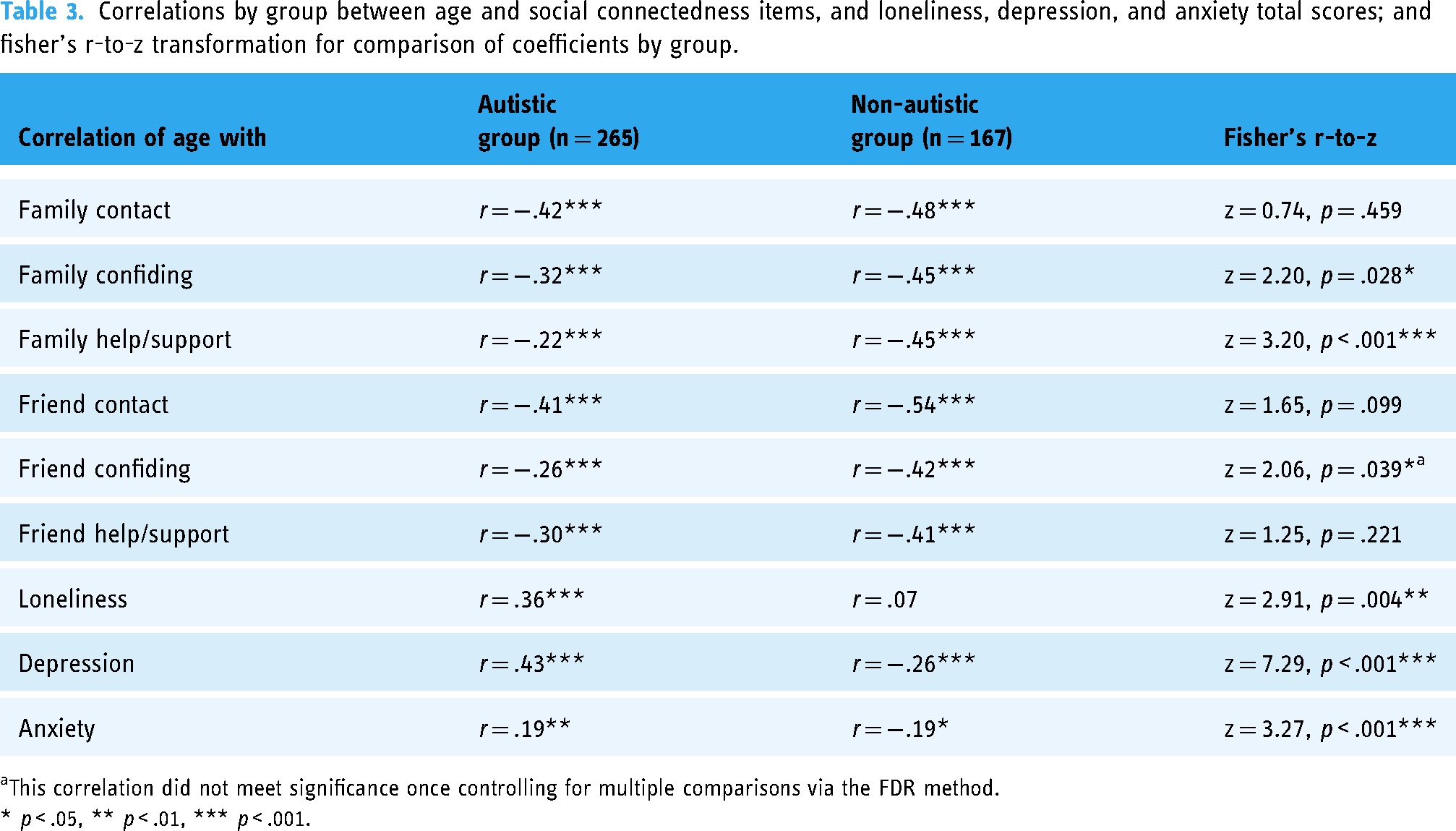
This correlation did not meet significance once controlling for multiple comparisons via the FDR method.
* p < .05, ** p < .01, *** p < .001.
Regarding gender differences, men in both autistic and non-autistic groups had stronger negative associations between aspects of social connectedness and age (i.e., social connectedness decreased with age) when compared to autistic women and non-autistic women, respectively. See Supplemental Table S3 for correlations by gender.
Experiences of loneliness and other mental health problems
The autistic group had significantly higher loneliness scores than the non-autistic group. The effect size of this difference was large (d = 2.71). The autistic group also had significantly higher current depression and anxiety scores than the non-autistic group. The effect sizes of these differences were also large (d = 1.37 and 1.52, respectively). See Table 4 for loneliness and mental health scores.
Descriptive statistics and group differences of loneliness, depression, and anxiety scores of the autistic and non-autistic groups.

Note. Effect size calculated using Cohen's d or Cramer's v. Due to the scoring method of the UCLA loneliness scale, possible scores range 20–80. Social Connectedness measured using a combined scale of family and friend responses.
When controlling for the possible influence of depression and anxiety symptoms on loneliness scores, group differences between the autistic and non-autistic groups on loneliness scores remained significant (F(1,428) = 330.12, p < .001) with a large effect size (d = 1.79). The same pattern of results was also found when controlling for the influence of living alone on loneliness scores (F(1,428 = 764.65, p < .001).
Associations were found between loneliness, social connectedness, depression, and anxiety. A significant moderate negative association was found between loneliness and social connectedness for both the autistic and non-autistic groups (r = −.50 and −.47, respectively), and the strength of these associations was not found to differ (Fisher's r-to-z = −.39, p = .69). Additionally, significant moderative-to-strong positive associations were found between loneliness and depression and anxiety scores for both autistic and non-autistic groups (rs = .38−.73), except for loneliness and anxiety in the non-autistic group (r = .05).
Regarding gender differences, autistic women reported significantly higher loneliness scores than autistic men. When accounting for the possible influence of depression and anxiety symptoms on loneliness scores, gender differences between the autistic men and women on loneliness scores remained significant (F(1,257) = 7.32, p = .007) with a small effect size (d = 0.33). No gender differences in loneliness scores were found in the non-autistic group. No other gender differences were found in depression or anxiety scores in either autistic or non-autistic group. No interactions were found between group and gender for loneliness, depression, or anxiety. See Supplemental Table S4 for loneliness and mental health scores by gender.
Experiences of loneliness and other mental health problems – associations with age
For the autistic group, loneliness significantly increased with age. This association was moderate (r = .346). However, this age x loneliness association was not found in the non-autistic group (r = .071). The strength of the association in the autistic group was significantly greater than in the comparison group (z = 2.91, p = .036). Additionally, significant associations were found between age and depression for both the autistic and non-autistic groups. However, the direction of these associations was found to differ. Depression and anxiety were both found to be positively associated with age in the autistic group (i.e., increasing with age) and negatively associated with age in the non-autistic group (i.e., decreasing with age), and the strength of these associations were found to significantly differ (depression z = 7.29, p < .001; anxiety z = 3.27, p < .001). See Table 3 and Figure 1 for visualisations of these age associations.
Regarding gender differences, associations between age and loneliness were significantly stronger for men compared to women in the autistic group (z = 2.34, p = .019). In the non-autistic group, age and loneliness were associated in men but not women, and these associations significantly differed in strength (z = 2.97, p = .003). A similar pattern of associations with age was found for men and women in both groups for depression and anxiety. See Supplemental Table S3 for correlations by gender.
Discussion
The current study documents the rates and experiences of social isolation and loneliness of over 260 autistic adults aged 40 to 90+ years old, compared to an age and gender-matched non-autistic comparison group. As hypothesised, middle-aged and older autistic adults were found to be less socially connected (i.e., be more socially isolated) and be lonelier than the non-autistic comparison group. While there were no gender differences in rates of social isolation, women reported being lonelier than men in both the autistic and non-autistic groups. Additionally, a similar pattern of results was found when controlling for age and symptoms of current poor mental health (i.e., depression and anxiety). While social isolation increased with age for both the autistic and non-autistic groups, loneliness only increased with age in the autistic group. For both social isolation and loneliness, the associations with age were significantly stronger in men than women in both groups. These findings suggest that autistic adults may be particularly susceptible to social isolation and loneliness in older age. While autistic women reported being lonelier, autistic men may be at greater risk of increasing social isolation and loneliness with older age.
The first key finding in the current study is that the middle-aged and older adults in the autistic group reported significantly fewer social connections and sources of social support than the non-autistic comparison group (hypothesis 1). When considering gender differences, autistic women were found to be in contact with fewer people and have fewer confiding relationships than autistic men.
To the authors’ knowledge, no study has explored the number of social contacts and sources of social support in middle-aged and older autistic populations, thus making comparisons to the existing literature difficult. However, a study by Charlton et al. (2023) documented the subjective sense of being socially supported and its link with quality of life in their sample of over 350 autistic adults aged 40 to 83 years. The findings of the current study are not directly comparable to Charlton et al. (2023) due to differing study design and measures. Charlton et al., for example, only included autistic people in their study, while the current study has a non-autistic comparison group. Charlton et al. also used a subjective measure that explores how supported the person feels, while the current study more objectively quantifies the number of social connections and support sources (albeit through self-report). Despite these differences, the two studies viewed together do have significant implications regarding the necessity of social support later in life for autistic people. Charlton et al. (2023) documented that social support is a key predictor of physical, psychological, social, and environmental quality of life for middle-aged and older autistic people. This key finding, taken alongside the current study that documents that many older autistic people lack social contact and support, highlights the need for support and possible interventions to ensure that autistic people have good quality of life as they get older.
The second key finding in the current study is that the middle-aged and older adults in the autistic group reported being significantly lonelier than the non-autistic comparison group (hypothesis 2). This result remained, with large effect, even when controlling for symptoms of depression. When considering gender differences, autistic women reported significantly higher feelings of loneliness than autistic men, however this difference was of small effect size. This gender difference was not found in the non-autistic comparison group, but no interactions were found between gender and autism group for loneliness.
While experiences of loneliness have yet to be specifically explored in middle-aged and older autistic adult populations, our findings are comparable to two studies that have included older adult participants. Ee et al. documented that their autistic participants experienced high rates of loneliness compared to their non-autistic comparison group. Additionally, Elmose (2020) also documented that loneliness was commonly felt. The findings of the current study are also comparable with the wider literature on loneliness in younger autistic populations. In a recent systematic review by Umagami et al. (2022), autistic adults often feel lonely and disconnected from those around them, including feeling disconnected more broadly from their community and society. However, this review identified a limitation that studies that explore loneliness in autistic populations often represent the experiences of autistic men, in young to middle adulthood, who live predominately with their parents or a caregiver, and who are highly educated. In the current study, our autistic sample is comprised of those aged 40–91 years old, 52% are women, only 8% live with a parent, and only 28% have a university level qualification. While our findings are broadly comparable to those in Ugamami et al.'s review, our study provides valuable information about often neglect populations in autism research (i.e., the experience of older people and women, more broadly) and highlights that elevated feelings of loneliness are also found in middle-aged and older autistic populations.
The final key findings of the current study are that social connectedness and loneliness are associated in similar ways in autistic and non-autistic people (hypothesis 3), and that a decrease in social connectedness and an increase in loneliness was found with increased age (hypothesis 4). This study documented that being socially connected and having sources of social support were negatively associated with age (i.e., people become less connected and have fewer sources of support as they get older) for both the autistic and non-autistic groups. Furthermore, feelings of loneliness were positively associated with age in the autistic group (i.e., autistic people felt lonelier as they got older); however, this association was not found in the non-autistic group. When considering gender differences, the association between age and social connectedness and loneliness was found to a greater extent in men (in both autistic and non-autistic groups) than in women, suggesting that men may become more isolated and lonelier as they get older compared to women. This study also found that age was positively associated with depression and anxiety in the autistic group, while the opposite was found in the non-autistic group; although while these correlations were significant, the strength of the associations was weak. Inconsistencies have been found in the existing literature in age associations in mental health; some studies (e.g., Lever and Geurts, 2016) have found negative associations, with others (e.g., Charlton et al., 2023 and Yarar et al. (2022)) have found positive associations. Further work, including longitudinal studies, is needed to further examine age-related change in autistic peoples’ mental health in midlife and older age.
When these age associations with social connectedness and loneliness are taken together, a complex pattern of gender differences is within our results. These associations suggest that while autistic women and non-autistic women may report being less connected and have more feelings of loneliness than their male counterparts, autistic men and non-autistic men appear to become less connected and lonelier as they get older. This pattern of age associations could place autistic and non-autistic men at an increased risk of becoming socially isolated later in life, which may disproportionately impact autistic men due to their higher rates of loneliness. This may be a particularly important finding, due to the negative consequences associated with being socially isolated and lonely late in life. In a systematic review exploring the consequences of social isolation and loneliness in the general population, Leigh-Hunt et al. (2017) report a consistent finding that social isolation and loneliness were predictors of poor physical and mental health outcomes, including increased rates of dementia, suicide, and all-cause mortality. Given the relationship between social isolation and loneliness and these negative life outcomes, interventions are needed to mitigate the risk of poor outcomes for autistic populations across the lifespan, but particularly in older age.
When contextualising the findings of this study, it is important to consider limitations, as well as strengths. A strength of the AgeWellAutism study is that we involved a group of middle-aged and older autistic people in PPI interviews to decide the important topics to be considered within the study and review the survey wording and accessibility. Another strength of this study is that we used a wide range of recruitment methods, which included social media advertisements (e.g., Twitter, Facebook, Reddit), as well as advertisements being circulated to existing research participation databases (e.g., the Autistica Network). Additionally, we advertised to older adult residential communities and community centres, to try to reach those who do not engage with social media platforms. This varied approach to recruitment resulted in a sample that is somewhat representative of the general population in terms of demographic characteristics, such as in gender ratio and in education level.
However, there are limitations to the AgeWellAutism study and opportunities for future research. Despite rigorous steps being taken to minimise the risk of spam participants, this study was conducted through an online survey, as such, we are unable to ensure that participants’ responses were accurate and genuine (see Pellicano et al., 2024 for a discussion on online data integrity). Furthermore, as this was an online survey, we will not have reached all groups within the autism spectrum (for example those with intellectual disability). In addition, like much ageing research, there is the problem of the ‘survivor effect’; older adults who take part in research are often healthier and in better life circumstances than others of their age. While this study has a near even 50:50 gender balance in both the autistic and non-autistic groups, we had only a small number of transmen, transwomen, and non-binary autistic participants take part. Due to the small number of trans/non-binary participants, we were unable to explore whether the results of the current study differ in these populations. Due to the societal stigma that trans and non-binary people face (King et al., 2020), they may be at an increased risk of being socially isolated. Further, regarding the design of the study, all measures reported in the current study are self-reported, and the use of self-report alone is a limitation. Additionally, when reporting on the number of people they are in contact with in the Lubben Social Networking Scale, while we provided definitions of what to consider family and friends, some people may have acquaintances (e.g., a neighbour, an online contact) or an employed supporter (e.g., a carer or support worker), who may provide social contact and support, but may have been omitted as they did not fit into the provided definitions. Moreover, the Lubben Social Networking Scale does not ascertain the participant's satisfaction with their social contacts, which could be an important factor to consider in future research. Additionally, we did not probe the nature of the connections (i.e., in-person connections, virtual connections) and the modes of contact (i.e., in-person contact, virtual contact), which may have differing influences on becoming/feeling lonely. We were also limited in exploring the influence on demographic factors in this study, and future research could consider ways to design their studies to be able to account for the influence of these factors, e.g., employment/retirement status, types of employment, retirement activities, etc. And finally, this study uses cross-sectional data, so we are unable to infer age-related change from these findings. Future studies should use longitudinal data to examine how social connectedness and loneliness change with age, which will give insight into how social networks change in autistic populations as they get older. Despite these limitations, the current study provides vital information about an often-neglected population in autism research and provides important evidence that reinforces the need for the development of evidence-based interventions that will mitigate the risk of autistic people being isolated and lonely later in life.
In conclusion, this study quantitively examines experiences of social connectedness and loneliness an autistic population in midlife and older age. As hypothesised, and in line with the previous literature examining younger autistic populations, we found that middle-aged and older autistic adults have fewer social connections and social support sources when compared to non-autistic adults. Furthermore, approximately 10% had no social contact with family or friends over the course of a month. We also found that middle-aged and older autistic adults reported more feelings of loneliness than the non-autistic adults in the current study. And finally, social connections diminished while loneliness increased with age in both the autistic and non-autistic groups, but to a greater extent in the autistic group. This meant, particularly for autistic men, that they could become socially isolated and very lonely later in life. These results support and extend the previous studies that have suggested that autistic people have fewer social connections and report higher levels of loneliness from childhood through to young adulthood. As isolation and loneliness can lead to negative consequences both mentally and physically, a better understanding of their causes in old age is essential to provide evidence-based interventions to this population. Importantly, studies must also identify evidence-based strategies to strengthen middle-age and older autistic adults’ social networks and alleviate their feelings of loneliness.
Supplemental Material
sj-docx-1-ndy-10.1177_27546330241245529 - Supplemental material for Experiences of social isolation and loneliness in middle-aged and older autistic adults
Supplemental material, sj-docx-1-ndy-10.1177_27546330241245529 for Experiences of social isolation and loneliness in middle-aged and older autistic adults by Gavin R. Stewart, Emily Luedecke, William Mandy, Rebecca A. Charlton and Francesca Happé in Neurodiversity
Footnotes
Acknowledgements
The authors are grateful to the 12 autistic people who offered suggestions on content and provided feedback on the language use and accessibility of the AgeWellAutism study. We would like to thank Autistica for advertising this study to their Network members. We would also like to thank Susanne Grobe, who assisted with data collection during her time as an MSc student at King's College London. At the time of data collection, GRS was funded by the Economic and Social Research Council (ESRC) via the London Interdisciplinary Social Science Doctoral Training Partnership. When preparing this manuscript, GRS was funded by the ESRC via the UCL, Bloomsbury and East London Doctoral Training Partnership. GRS is currently funded by a British Academy Postdoctoral Research Fellowship. FH is part-funded by the NIHR Maudsley Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King's College London. The funders have had no role in the data collection, analysis, interpretation, or any other aspect pertinent to the study. The authors have not been paid to write this article by any agency. This article represents independent research conducted by the authors, and the views expressed are those of the authors and not necessarily those of the ESRC, BA, NIHR, NHS, or KCL.
Author contributions
Authors GRS, RAC, and FH conceived the current study. GRS designed the online survey and selected materials. GRS and EL conducted analyses. GRS and EL wrote the manuscript, with WM, RAC, and FH reviewing and editing drafts. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Economic and Social Research Council, NIHR Maudsley Biomedical Research Centre.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.