
Abstract
Over the past two decades, mental health has become a global public health concern. Although existing research suggests that the urban living environment is closely related to mental health changes, it remains unclear how this relationship evolves when the urban living environment undergoes sudden, citywide changes due to public health measures. To address this issue, we conducted a three-wave longitudinal survey in Shanghai during and after periods of citywide restriction and reopening, with data collected in May 2022 (during the lockdown), November–December 2022 (prior to the lifting of citywide restrictions), and May–June 2023 (the onset of the second infection wave). Out of 810 responses, 276, 215, and 195 participants provided valid responses in the first, second, and third waves, respectively, yielding a total of 686 valid questionnaires. We calculated the difference scores between each pair of waves and built linear regression models to analyze the determinants of mental health change across two transition periods. Results show that participants’ mental health improved overall. From the lockdown to reopening, improvements were driven by reduced individual stressors, lower family conflict, and higher housing and institutional satisfaction. From the reopening to the onset of the second infection wave, mental health changes were related to changes in individual stressors, housing satisfaction, and social connection. These findings reveal that the determinants of mental health differ across distinct phases of environmental change. The study contributes to understanding how individual stress and social connection jointly shape psychological resilience during crises. Beyond the pandemic, our results highlight the importance of integrating mental health and urban resilience into urban renewal and neighborhood governance agendas. Such integration is crucial for fostering adaptive, inclusive, and sustainable urban development in the face of future social or environmental disruptions.
Introduction
For a long time, mental health has been recognized as a major cause of disease burden (Patel et al., 2018). A recent report indicates that mental disorders remain the top 10 leading causes of disease burden worldwide, with little to no improvement since 1990 (GBD 2019 Mental Disorders Collaborators, 2022). Worse still, the coronavirus disease 2019 (COVID-19) pandemic has posed unprecedented threats to mental health globally (Xiong et al., 2020).
The WHO defines mental health as a state of mental well-being that enables people to cope with the stresses of life, to realize their abilities, to learn well and work well, and to contribute to their communities (World Mental Health Report, 2022: 8). Mental health is determined by a combination of individual characteristics, family conditions, social circumstances, and broader structural factors (Deng et al., 2024; Holt-Lunstad, 2024; Koss et al., 2017). Meanwhile, existing research shows that mental health is also closely related to the urban living environment (Chen and Chen, 2015; Xu et al., 2023). However, most of these studies are cross-sectional and thus cannot capture the impact of substantial changes in the urban living environment on mental health, particularly when such changes are imposed on the public at a large scale (Sui et al., 2022, 2025). Longitudinal research provides opportunities to examine how environmental changes relate to mental health trajectories (Hedeker and Gibbons, 2006). To address this issue, our study examines how the associations between mental health and the urban living environment vary when residents experience dramatic changes in the urban living environment.
The COVID-19 pandemic has affected people worldwide, including their mental health and social life (Xiong et al., 2020). It not only triggered mental health problems such as anxiety, depression, and stress, but may also have altered the underlying mechanisms influencing mental health (Brooks et al., 2020). Recent research indicates that mental health during the COVID-19 pandemic is closely associated with multiple aspects, including individual, family, and societal factors (Burlew et al., 2025; Hommerich et al., 2025; Liu and Cheng, 2025). In this unique context, it is unclear whether and how the determinants of mental health have changed when their physical, social, and institutional living environments are simultaneously altered by public health measures. We focus on Shanghai, one of the most densely populated global cities in the world, which experienced both extended citywide restrictions and a subsequent reopening period. Specifically, we collected three waves of data and compared how key factors, including individual stressors, family conditions, and social contexts, affected mental health across two distinct transition periods. We aim to (1) examine how key determinants of mental health, including individual stressors, family conditions, and social contexts, change across phases of disruption and recovery, and (2) identify the dominant factors at each stage.
This study provides longitudinal evidence on the temporal relationships between environmental change and mental health in a large metropolitan context and expands the conceptual understanding of the urban living environment by integrating individual, familial, and institutional dimensions during a period of global health crisis.
Literature review and research framework
Mental health and its determinants
Mental health issues have become a crucial challenge worldwide, posing a potential threat to individuals’ physical and social functioning and attracting sustained attention in the academic community (Patel et al., 2018). Existing evidence demonstrates that mental health is determined by a combination of factors, including individual, family, and social dimensions (Deng et al., 2024). During crises such as pandemics or disasters, these determinants can shift rapidly, challenging resilience of individuals and communities (Burlew et al., 2025; Hommerich et al., 2025; Liu and Cheng, 2025; Norris et al., 2008).
Individual factors, such as age, education, and relationship status, are strongly associated with mental health (Annequin et al., 2015; Deng et al., 2024; McAneney et al., 2015). Although mental health is experienced by individuals, it is also important to understand the relationship between stressors in an individual’s life and their mental health (McAneney et al., 2015; Varma et al., 2021). Charles et al. (2013) argued that daily stresses and negative events in life have long-term implications for an individual’s mental health. Coley et al. (2022) pointed out that during the COVID-19 pandemic, individual stressors such as perceived food insecurity, housing insecurity, and job insecurity had negative effects on mental health. Research has also found that stressors related to financial conditions and employment changes during the COVID-19 period negatively impacted mental health (Burlew et al., 2025; Varma et al., 2021). Taken together, these studies highlight that individual characteristics and stressors, particularly those intensified during crises, play a critical role in shaping mental health outcomes. However, it remains unclear how the influence of these individual factors may shift when the urban living environment undergoes substantial and rapid changes.
The family plays a nurturing and protective role, serving as an essential context for fostering mental health (Ryan et al., 2010). Van Herreweghe and Van Lancker (2024) found that changes in depressive feelings were associated with variations in received intergenerational support, underscoring the importance of family relationships in times of crisis. However, family discord can trigger various negative emotions, adversely affecting mental health (Koss et al., 2017). A study showed that family conflict may cause mental health problems that jeopardize the transition from adolescence to young adulthood (Choe et al., 2014). In addition, housing conditions are closely associated with mental health (Suglia et al., 2011). Housing is more than a shelter—it provides comfort, privacy, and security, and can affect mental health (Suglia et al., 2011). A longitudinal study indicated that after moving to higher-quality housing, residents exhibited higher mental health outcomes (Evans et al., 2000). Akbari et al. (2021) indicated a positive association between housing satisfaction and mental health, particularly satisfaction with kitchen, living room, and terrace. A study conducted during the COVID-19 pandemic in Shanghai also found similar results (Liu and Cheng, 2025). Overall, the family acts simultaneously as a social unit that can nurture or strain mental health and as a physical living environment that directly affects well-being. Major changes in the urban living environment may therefore alter both the quality of family interactions and the physical conditions under which they occur.
Social environment is crucial for preventing mental health issues, sustaining positive mental health, and supporting recovery from both moderate and severe mental health conditions, while isolation and loneliness are associated with poorer mental health (Holt-Lunstad, 2024). A study found that social support may protect mental health in the COVID-19 pandemic (Jarego et al., 2024). Thoits (2011) emphasized that positive social connections, especially emotional support, can buffer the harmful effects of stress exposure on mental health. Hommerich et al. (2025) also revealed that social capital resources played a crucial role in mitigating mental health impacts. Recently, the role of social institutions in promoting mental health has been increasingly recognized, particularly during times of disaster (Lee, 2022; Thoresen et al., 2018). Clay and Abramson (2021) reported that for each additional prosocial institution established in the community during recovery from a hurricane, children were less likely to be diagnosed with a mental health disorder. Research conducted during the COVID-19 pandemic indicated that institutional trust was significantly positively associated with the mental health of older adults (Lee, 2022). Deng et al. (2024) also revealed certain institutional characteristics may play a significant role in mental health. These studies show that social environments affect mental health both through interpersonal support networks and through institutional trust and capacity. Crises such as COVID-19 can disrupt or reshape both dimensions, yet existing research seldom tracks how their relative roles evolve over time.
Changes in urban living environment during the pandemic
The global outbreak of COVID-19 in late 2019 led to a series of unprecedented public health measures across countries, including temporary business closures, mobility restrictions, and physical distancing guidelines designed to curb transmission (Benke et al., 2020; Ren, 2020). While necessary for infection control, these interventions profoundly altered the urban living environment, reshaping patterns of work, mobility, and social interaction (Zhang et al., 2020).
Social life was particularly affected during the COVID-19 pandemic (Stuart et al., 2021). Social connection is a fundamental human need and is associated with higher happiness, belonging, safety, lifespan, and social sustainability (Holt-Lunstad, 2024). However, distancing measures limited face-to-face contact (Holt-Lunstad, 2024). Benke et al. (2020) revealed that stricter restrictions, reduced social contacts, and greater perceived life changes were associated with higher mental health impairments. As a result, COVID-19 forced a shift from in-person interactions to greater reliance on online communication (Stuart et al., 2021). In the United States, internet use grew by nearly 50% in 2020, especially for video call platforms. Online interactions with family members and close friends were associated with higher well-being (Tibbetts et al., 2021), and Stuart et al. (2021) further found that such online connections buffered the negative effects of health anxiety under isolation, thereby protecting mental health.
Existing research indicates a strong connection between the urban living environment and mental health change (Sui et al., 2025). However, the pandemic context introduced a degree of environmental disruption rarely seen in modern urban history, raising new questions about whether and how the determinants of mental health change during phases of restriction and reopening. While cross-sectional research has identified the short-term psychological effects (Zhang et al., 2020), few studies have employed longitudinal designs to trace how these effects evolve over time.
Research framework
Drawing on the literature review, we used longitudinal data to examine the effects of urban living environment changes on the determinants of mental health across three dimensions: individual, family, and social. In this study, we define the urban living environment as the set of living conditions that includes access to housing, adequate drinking water, sanitation systems, and food safety, which may be disrupted by environmental threats (Quah and Cockerham, 2017). Specifically, we employed one variable to capture individual factors (individual stressors), two variables to measure family factors (housing satisfaction and family conflict), and two variables to represent social factors (social connection and institutional satisfaction). By analyzing how these factors vary across different phases of the pandemic, our framework allows us to assess whether their relative importance changes in response to major environmental disruption. The research framework is illustrated in Figure 1.
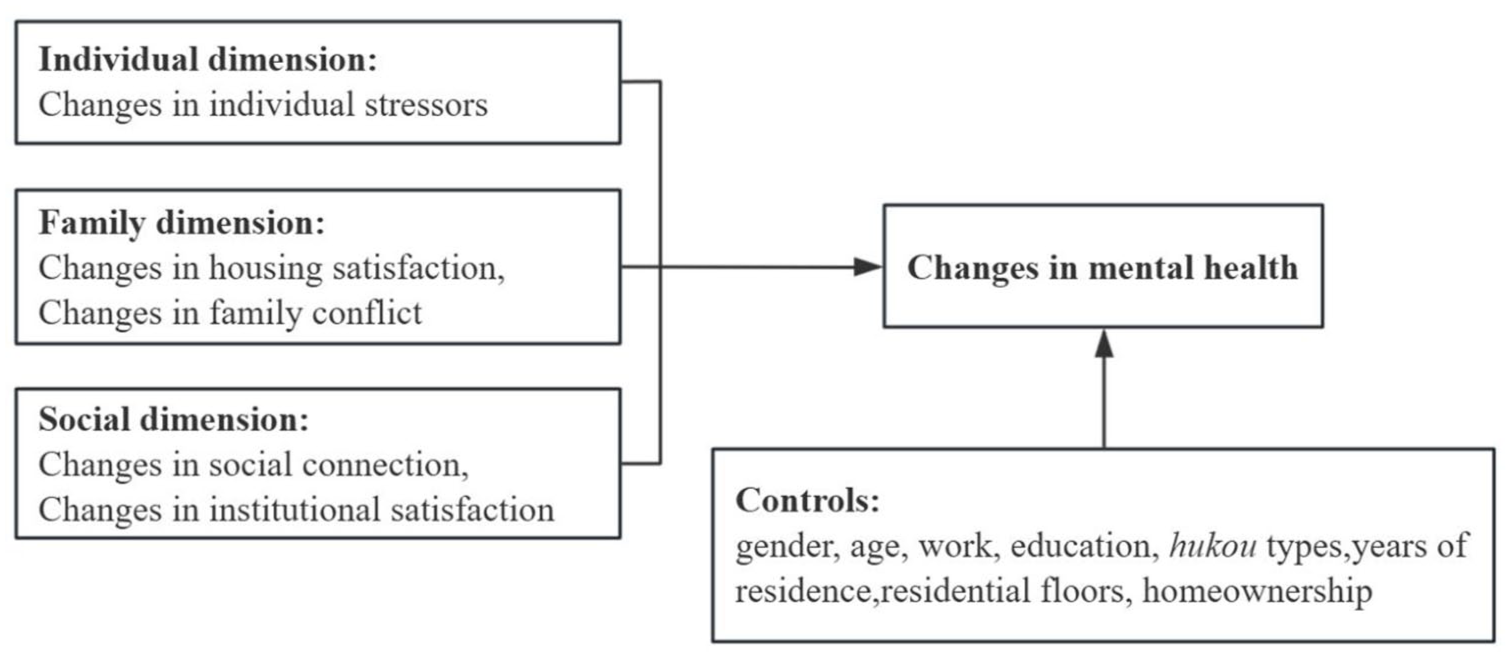
Research framework.
Data and methods
Data collection
As a highly dynamic international metropolis, Shanghai has long undergone rapid changes in its urban living environment (Xiao et al., 2025), providing an ideal context to explore how such changes relate to residents’ mental health. In March 2022, following a COVID-19 outbreak in Shanghai, a citywide stay-at-home order was implemented to contain the virus (Xiao et al., 2023). In December 2022, citywide restrictions were lifted (Ioannidis et al., 2023). To capture changes in mental health across distinct policy contexts, we conducted surveys at three stages of COVID-19 control in Shanghai. The first wave was conducted in May 2022, during the strict citywide lockdown, yielding 276 valid responses. The second wave took place in November–December 2022, following the lifting of citywide restrictions, with 215 valid responses and a follow-up response rate of 78%. The third wave was conducted in May–June 2023, at the onset of the second wave of infections, yielding 195 valid responses and a follow-up response rate of 91%. Across three waves, we obtained 686 valid responses (matched within waves for analysis) from 810 collected questionnaires. The surveys were conducted in one residential neighborhood that closely followed citywide public health measures, reflecting a typical case of Shanghai’s pandemic experience. Within the neighborhood, questionnaires were distributed to each building unit. Since face-to-face surveys were not possible during the lockdown, we employed an online survey platform (Wenjuanxing) to collect questionnaires. This platform has been widely used in previous studies for administering surveys during COVID-19 lockdowns (Gan et al., 2022; Shen et al., 2025; Wang et al., 2020). Although the data were collected from a single neighborhood, the sample reflected broader urban conditions as similar restrictions were uniformly implemented across Shanghai during the lockdown.
Measurement
Dependent variable
The dependent variable for this study is changes in mental health. We employed the Depression, Anxiety and Stress Scale (DASS-21) to measure the mental health status of respondents (Parkitny and McAuley, 2010). The DASS-21 has been widely used as a measure of mental health, especially during the COVID-19 epidemic (Xiong et al., 2020; Wang et al., 2020). Participants rated their responses using a 4-point Likert scale according to their level of agreement (from 1 = “totally agree” to 4 = “totally disagree”), with higher scores indicating better levels of mental health. The Cronbach’s alpha coefficients for the three waves were 0.97, 0.96, and 0.93. Changes in mental health were calculated as the difference between scores from consecutive waves (Wave 2 – Wave 1, and Wave 3 – Wave 2).
Independent variables
We employed changes in individual stressors as the independent variables for the individual dimension. From a psychological perspective, stressors can be events or environments that individuals might consider demanding, challenging, or threatening individual safety (Deckers, 2018). Respondents were asked to rate the following questions: “Fear of infection,” “Reduced income or debt pressure,” “Unable to meet friends,” “Small and boring interior spaces,” “Unconfirmed information or rumors,” “Difficulty in accessing medical services.” Each item was rated on a 5-point scale (from 1 = “not worried at all” to 5 = “extremely worried”). The Cronbach’s alpha coefficients of this scale in each wave were 0.75, 0.84, and 0.81.
Changes in family conflict and housing satisfaction were used as independent variables for the family dimension. We asked participants about changes in the frequency of family conflicts in the second and third waves. This was assessed with the question “Compared to the time of the last questionnaire, how has the frequency of verbal or physical conflicts with your family members or co-residents changed?” Responses were recorded on a 5-point Likert scale according to the extent of changes (from 1 “increased greatly” to 5 “decreased greatly”). Housing satisfaction was measured by seven items covering “housing size,” “housing layout,” “decoration of housing,” “soundproofing of housing,” “ventilation of housing,” “lighting and sunlight conditions,” and “refrigerator capacity.” Participants rated these items based on their actual experiences using a 5-point scale. The Cronbach’s alpha coefficients of this scale in each wave were 0.84, 0.83, and 0.78, respectively.
The independent variables for the social dimension are changes in social connection and institutional satisfaction. Social connection was measured by five items on a 5-point Likert scale, including “I know many people in this neighborhood,” “Residents often chat with each other (online),” “Residents in this neighborhood get along well,” “I would seek help from my neighbors when I am in trouble,” and “I’m willing to do what I can to make my neighborhood better.” The Cronbach’s alpha coefficients of this scale in each wave were 0.78, 0.73, and 0.77. Institutional satisfaction was measured by five items: “Neighborhood council,” “Property management company,” “Homeowners’ committee,” “Neighborhood volunteers,” and “Neighborhood administration office.” Each item was rated on a 5-point scale. The Cronbach’s alpha coefficients of this scale in each wave were 0.84, 0.89, and 0.88.
Except for changes in family conflict, changes in all independent variables were calculated as the difference between scores from consecutive waves (Wave 2 – Wave 1, and Wave 3 – Wave 2), consistent with the calculation of changes in mental health.
Control variables
We collected demographic characteristics including gender, age, employment status, education, and hukou status (i.e., household registration status) as control variables. Since most people were confined to their residences during the lockdown period, residential variables may also be related to mental health. For this reason, we controlled for variables including years of residence, floor level, and homeownership.
Analytical approach
The aim of this study is to investigate the impact of changes in the urban living environment on mental health. To achieve this aim, we calculated the changes in mental health and key variables using difference scores. In longitudinal studies, the difference score approach is a commonly used method to assess changes in variables between two time points (Nesselroade and Cable, 1974; Wang and Wang, 2020). Subsequently, we employed multiple linear regression models to examine the relationships between the main variables and identify the determinants of changes in mental health in different periods. To address potential multicollinearity, we calculated variance inflation factors (VIFs) for each variable. The VIFs of all variables in the two models ranged from 1.03 to 2.46, indicating a low likelihood of multicollinearity.
Results
Table 1 shows the demographic information. Of the participants, 59.50% were male. The mean age of participants was 46.54. Economically, 66.20% of the participants were employed, 73.40% were homeowners, and 44.20% had a monthly household income exceeding 10,001 RMB. In terms of education, 38.50% held a bachelor’s degree and 16.90% held a master’s degree or higher. Overall, our sample had a higher proportion of local residents and was slightly skewed toward the upper-middle socioeconomic class.
Sample profile.
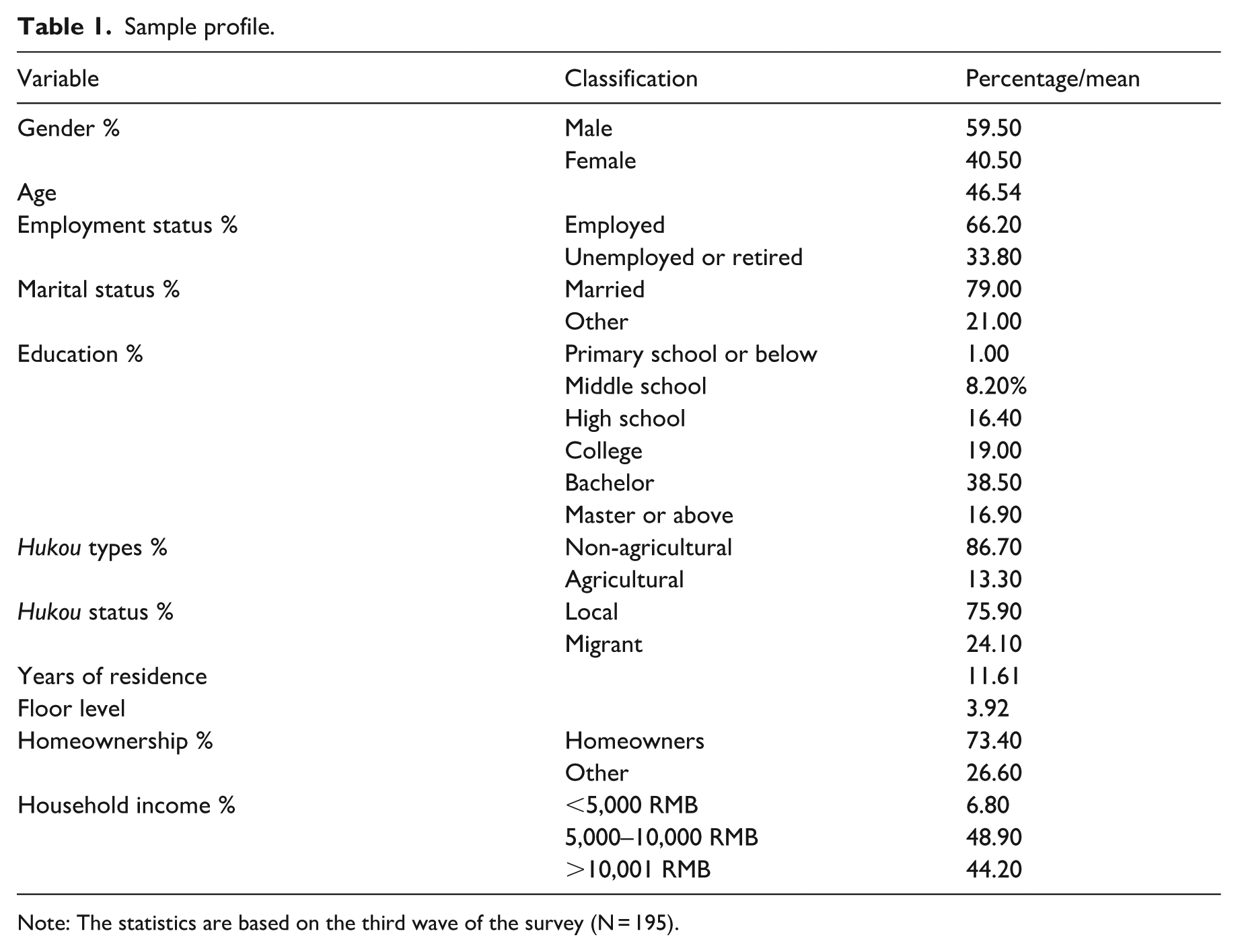
Note: The statistics are based on the third wave of the survey (N = 195).
Figure 2 and Table 2 present changes in mental health across the three waves. In our study, participants’ mental health showed an increased trend. Mean mental health scores increased from 3.41 during the lockdown to 3.61 during the reopening period. The t-test results reveal that this change was statistically significant, suggesting that the majority of the participants experienced a notable improvement in mental health following the end of the COVID-19 lockdown. Although the increase in scores (from 3.61 to 3.68) between the end of the lockdown and the onset of the second wave of COVID-19 was not statistically significant, the overall trend remained upward.
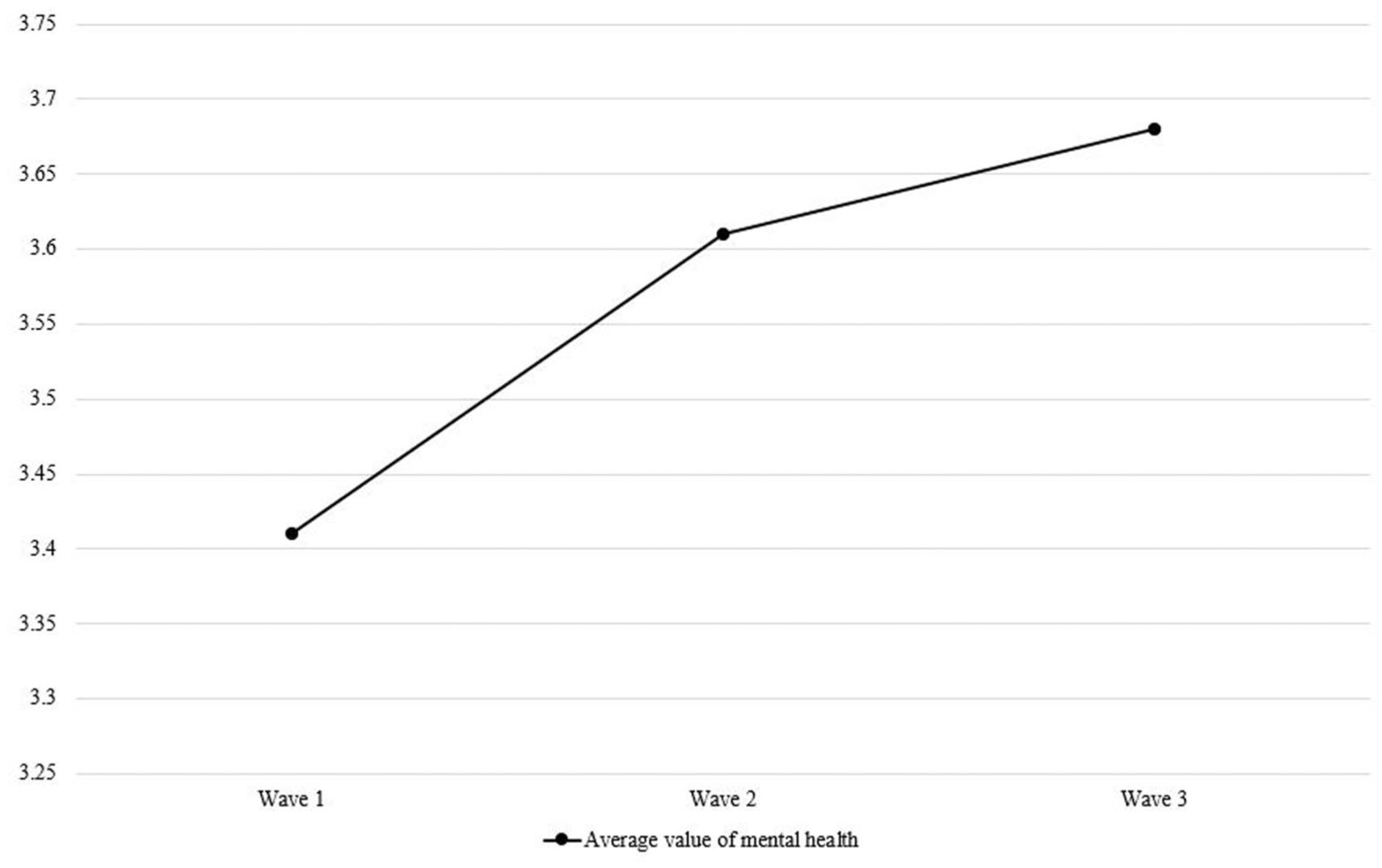
Mean mental health score for each wave.
Mean value and t-test of mental health for each wave.
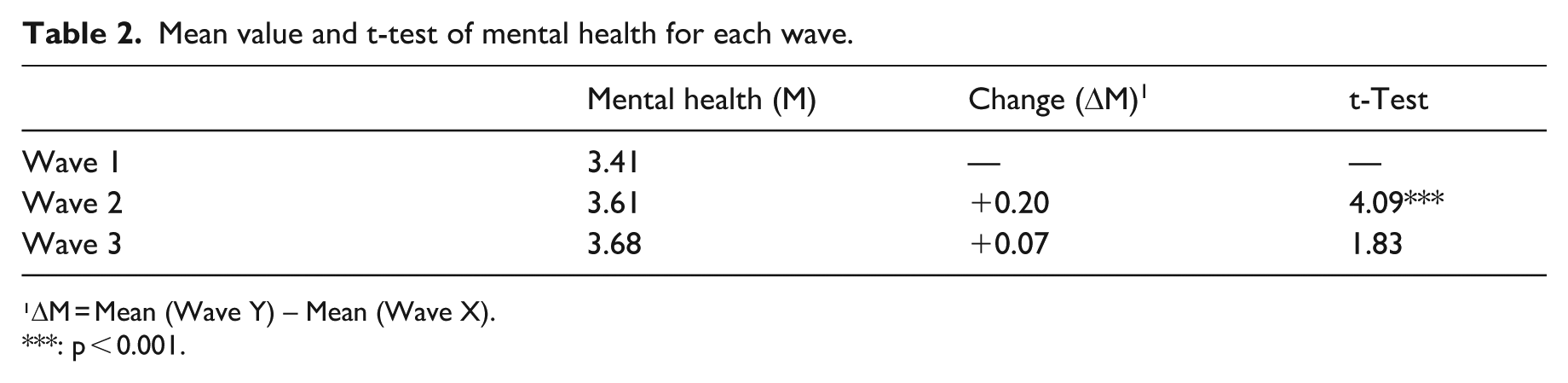
¹ΔM = Mean (Wave Y) – Mean (Wave X).
: p < 0.001.
We employed multiple linear regression models to investigate the determinants of the changes in mental health in different periods (Table 3). In Model 1, the beta coefficients for changes in individual stressors, family conflict, housing satisfaction, and institutional satisfaction are statistically significant, while the beta coefficient for changes in social connection was not. These findings suggest that during the lockdown, the reduction in personal stress and family conflicts, as well as the improvement in housing satisfaction and institutional satisfaction, contributed to better mental health. Model 2 reveals that the beta coefficient for changes in individual stressors, housing satisfaction, and social connection were statistically significant, while the beta coefficient for changes in family conflict and institutional satisfaction were not. This outcome suggests a strong association between changes in individual stressors, housing satisfaction, social connection, and changes in mental health during the reopening and the onset of the second wave of COVID-19. Overall, the determinants of mental health differed between the lockdown and reopening periods.
Modeling results.
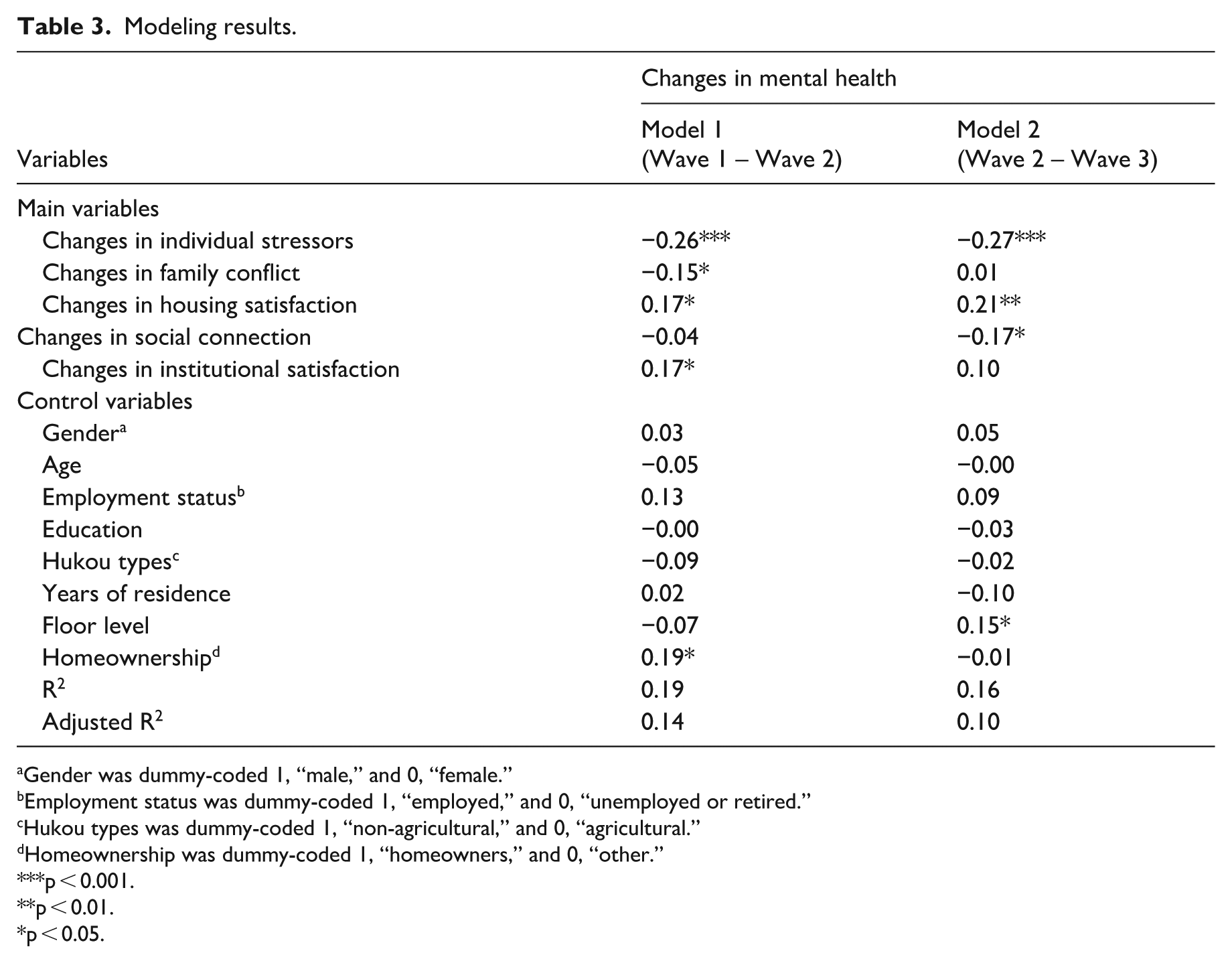
Gender was dummy-coded 1, “male,” and 0, “female.”
Employment status was dummy-coded 1, “employed,” and 0, “unemployed or retired.”
Hukou types was dummy-coded 1, “non-agricultural,” and 0, “agricultural.”
Homeownership was dummy-coded 1, “homeowners,” and 0, “other.”
p < 0.001.
p < 0.01.
p < 0.05.
Among the control variables, homeownership is closely associated with changes in mental health during the lockdown. Specifically, participants who owned their homes reported higher levels of mental health compared to others. In Model 2, there is a positive correlation between floor level and changes in mental health. This result indicates that during the reopening period, participants living on higher floors reported better mental health.
These results indicate that the correlates of mental health shifted across two distinct transition periods. From the strict citywide lockdown to the reopening stage, improvements in housing and institutional satisfaction, along with reductions in individual stressors and family conflict, were the primarily associated with better mental health. In contrast, from the reopening stage to the onset of the second wave of COVID-19, housing satisfaction and reduced individual stressors remained important, but social connection emerged as a significant factor, while family conflict and institutional satisfaction lost statistical significance. These changes highlight how the factors of mental health vary in response to urban living environment changes.
Discussion
Changes in mental health across the three waves
Our results show that mental health improved across both transition periods, with the most pronounced increase occurring between the strict citywide lockdown and the reopening stage. This finding is consistent with Rehman et al. (2023), who reported that in India, symptoms of depression, anxiety, and stress declined over time, reaching their lowest levels after lockdowns ended. Similarly, Mata et al. (2021) observed that although participants’ mental health was at its worst shortly after the onset of lockdown, it improved gradually over time. By contrast, Vloo et al. (2021) found that in the Netherlands, symptoms of depression and anxiety increased at the onset of the lockdown and did not return to pre-lockdown levels even after restrictions were lifted. These divergent results suggest that contextual factors, such as the degree and duration of lockdowns and timing of reopening, may play a critical role in shaping mental health trajectories. In the case of Shanghai, our three-wave panel data capture a unique sequence of strict lockdown, abrupt policy reversal, and subsequent epidemic resurgence, revealing that mental health responses are highly sensitive to substantial changes in urban living environment.
Determinants of changes in mental health across different periods
Individual dimension
We found that from the strict citywide lockdown through the reopening stage, and subsequently to the onset of the second COVID-19 wave, changes in individual stressors showed consistent negative associations with changes in mental health. Our findings align with Foster et al. (2023), who found that perceived COVID-19-related stressors during lockdown were related to depression and anxiety symptoms, with a lasting adverse impact. Brooks et al. (2020) noted that quarantine may trigger stressors, including fear of infection, frustration and boredom, inadequate supplies, and insufficient information. A U.S. study indicated that during the COVID-19 pandemic, food insecurity, disrupted medical care, unemployment, housing insecurity, and experiencing disruptions in education were associated with anxiety and depression (Coley et al., 2022). These results reveal that the stressors caused by the COVID-19 lockdown jeopardize people’s mental health. In addition, Chandola et al. (2022) showed that despite the lifting of some lockdown conditions in the U.K., stressors related to loneliness, unemployment, financial problems, and domestic work continued to influence common mental disorders. Haucke et al. (2021) similarly concluded that the mental health of vulnerable populations remained challenged by COVID-19-related stressors after the lifting of a strict lockdown in Germany. It is evident that the stressors brought about by COVID-19 lockdowns are long-lasting, since many of these stressors (e.g., ongoing financial strain, fear of infection) do not resolve immediately upon reopening, but instead persist and adapt to the post lockdown context. Thus, even after the lifting of lockdown measures, the stress and subsequent potential impacts of COVID-19 continue to harm people’s mental health.
Family dimension
From the strict citywide lockdown to the reopening stage, changes in family conflict were negatively associated with changes in mental health. However, this relationship was not evident from the reopening stage to the onset of the second COVID-19 wave. Family conflicts during lockdown could arise across multiple relationships. For example, heightened marital tensions may result from increased time at home and financial strain (Prime et al., 2020). Nasar et al. (2024) noted that when adolescents returned to live with their parents during the pandemic, differing demands and expectations caused interpersonal conflicts. Magson et al. (2021) reported that increased conflict with parents predicted a rise in mental health problems among adolescents during the lockdown. A similar pattern is also observed by Xu et al., (2023), who found that in multigenerational households, lockdown altered household chore and caregiving arrangements, with some tasks shifting from senior parents to younger parents working from home, while others had to take on additional elder care, creating dual pressures on working-age adults. Nevertheless, family conflicts may diminish or return to pre-pandemic levels once restrictions ease. For instance, Arbeau et al. (2025) revealed that in families with children or youth, conflict decreased after reopening. This trend is likely because prolonged cohabitation during lockdown had unintentionally heightened tensions, adversely affecting mental health. Once daily routines resumed and family life returned to normal, such conflicts no longer had a measurable impact on mental health.
Our findings indicate that changes in housing satisfaction are closely associated with changes in mental health in both transition phases. During lockdown, as activities that would usually take place elsewhere (e.g., working, studying, or relaxing) are transferred to domestic spaces, people spent substantially more time at home, thereby increasing demands for housing (Hansmann et al., 2021). Alamel et al. (2023) also noted that as a shelter, housing matters during the lockdown period, and reported a significant effect of housing conditions on students’ psychological distress. After the lockdown was lifted, the impact of housing conditions on mental health remained significant, which is unsurprising given that housing is a basic need for people, and its physical characteristics are closely related to people’s mental health (Akbari et al., 2021). Suglia et al. (2011) pointed out that a house not only provides a physical space but also offers comfort, privacy, and a sense of security, with specific features closely associated with mental health. Thus, regardless of whether lockdown measures are in place, housing remains important for mental health.
Social dimension
We found that from the strict citywide lockdown to the reopening stage, changes in social connection are not statistically significant in relation to changes in mental health, which is inconsistent with the common assumption that social connections generally promote mental well-being (Chang et al., 2023; Jarego et al., 2024). One possible explanation is that during the strict lockdown, social connection was limited and often dominated by pandemic-related topics, which may have included misinformation or alarming news. This aligns with evidence that during the COVID-19 period, increased online engagement could also facilitate the spread of negative information and emotional contagion, potentially undermining mental health benefits (Kaya et al., 2021). Such effects could offset potential benefits, resulting in a non-significant association with mental health. From the reopening stage to the onset of the second COVID-19 wave, however, we found that increased social connection is associated with poorer mental health. This may be because the increase in social connection occurred against a background of ongoing pandemic uncertainty. In this context, more frequent interactions may have amplified exposure to anxiety-inducing information and pandemic-related concerns, thereby contributing to a decline in mental health (Kaya et al., 2021), rather than providing the protective effects typically associated with social support.
We further found that changes in institutional satisfaction are closely related to changes in mental health from the strict citywide lockdown to the reopening stage, but this connection is absent during the second transition phase. These findings are consistent with Lee (2022), who found that during the COVID-19 pandemic, participants who scored higher on trust toward institutions were more likely to report better mental health. In times of crisis, community institutions mobilize their resources to deal with urgent needs (Thoresen et al., 2018). Nie et al. (2024) also noted that resident committees’ staff addressed residents’ urgent needs to visit hospitals and purchase medication during the lockdown, while also taking on the responsibility of daily food supply. The assistance provided by these institutions addressed residents’ pressing needs during the lockdown, thereby alleviating their psychological stress and anxiety. In the second transition phase, as daily life normalized and institutional involvement in residents’ daily lives declined, its direct influence on mental health may have diminished.
Conclusion
Our study uses longitudinal data from Shanghai during the COVID-19 pandemic to examine how mental health responds to major changes in the urban living environment. Across three waves of surveys, mental health generally showed an upward trend, with the most notable improvement occurring during the transition from strict lockdown to reopening. From the strict citywide lockdown to the reopening stage, reductions in individual stressors and family conflict, along with increases in housing satisfaction and institutional satisfaction, were associated with better mental health. From the reopening stage to the onset of the second COVID-19 wave, changes in individual stressors, housing satisfaction, and social connection were closely related to changes in mental health. These findings suggest that the factors associated with mental health vary across different phases of major social and physical changes in the living environment, reflecting the evolving patterns of this relationship.
Our contributions are threefold. First, this study extends the literature by demonstrating that individual stressors are a stable correlate of mental health regardless of changes in urban living environment. This finding adds to the understanding of how personal stress is linked to psychological outcomes during major environment changes, and underscores the need for targeted social support for vulnerable groups. Second, this study reveals, in certain crisis contexts, increased social connection may be associated with poorer mental health. While this finding differs from the prevailing narrative of social connection as inherently protective, it aligns with emerging research highlighting the potential for information overload and anxiety transmission through social networks during a crisis. The finding challenges existing theoretical frameworks and calls for a more nuanced investigation of the dual role of social connection in supporting and undermining mental health. Third, this study provides evidence that factors shaping mental health vary in response to significant changes in the urban living environment. This finding emphasizes the importance of adaptive mental health strategies to meet the psychological needs during changes of physical, social, and institutional living environments. Ultimately, safeguarding mental health in times of crisis requires timely and context-specific responses to address uncertainties and challenges arising from the changing urban living environment.
Although the COVID-19 pandemic represents an exceptional case, the analytical framework developed in this study can be extended to other large-scale disruptions that alter the urban living environment. Such disruptions may include population displacement and resettlement driven by environmental risks or large-scale urban redevelopment. These events, like the pandemic, generate public shocks that test the adaptive capacity of individuals and neighborhoods. Our framework offers a new lens for understanding mental health across different stages of change. During the initial shock phase, institutional safeguards and family cohesion function as critical psychological buffers. Once the new environment becomes normalized, the quality of housing and the reconstruction of social capital become central to sustaining mental well-being. Beyond the pandemic, these insights can inform adaptive, stage-specific interventions that strengthen urban resilience and mental health in diverse sociocultural contexts.
From a policy perspective, the findings suggest that mental health and urban resilience should be addressed in an integrated manner. During a pandemic, institutional safeguards, neighborhood-based support, and effective communication mechanisms are essential for buffering psychological stress. As cities transition toward recovery, housing quality, neighborhood design, and opportunities for social reconnection become central to sustaining well-being. Beyond the specific context of the pandemic, these insights are generalizable to other large-scale transformations in the urban living environment. Our findings call for the need to integrate mental health and urban resilience into urban renewal and neighborhood governance agendas. Future urban research and planning practices should further explore how built environment improvements and localized social networks can support residents’ adaptive well-being in rapidly changing cities.
Several limitations should be acknowledged. First, this study collected data from a single residential neighborhood. Although the sample reflected broader urban conditions, the findings should be interpreted with caution because local variations in urban living environments may not have been fully captured. Second, due to data collection constraints, only three survey waves were conducted, limiting our ability to trace residents’ long-term mental health trajectories. Future studies could collect longer-term panel data across multiple neighborhoods and employ fixed-effects models to examine the sustained impacts of urban living environment changes on mental health.
Footnotes
Acknowledgements
We are deeply grateful to the editors, the special issue editors, and the three anonymous reviewers for their thoughtful guidance and constructive suggestions. Responsibility for any errors and omissions remains with the authors.
Ethical statement
This study was approved by the Ethical Review Board of the School of Sociology at Huazhong University of Science and Technology (Project No. 500200219).
Consent to participate statement
Informed consent was obtained from all individual participants included in the study.
Consent for publication
Not applicable. All data presented in this manuscript are anonymized, and no identifiable personal information or images are included that would require specific consent for publication beyond the general consent for participation in research.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge the funding support from National Natural Science Foundation of China (NSFC) [grant numbers 42571265; 42301274; 42371245]; The Fundamental Research Funds for the Central Universities [2024QKT006].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author, but restrictions apply to the availability of these data due to privacy/ethical restrictions, and so are not publicly available.