
Abstract
Background
Paramedics operate in diverse, unpredictable environments where they encounter people requiring not just clinical intervention but compassionate, dignified care. Currently, paramedicine has no conceptual framework specific to their profession. Person-centredness is the global standard for healthcare delivery, offering an appropriate philosophical foundation for emergency practice contexts.
Aim
This hybrid scoping/methodological review examined international literature on person-centredness in paramedicine, specifically its conceptualisation and implementation in emergency settings, and paramedics’ understanding and delivery of person-centred approaches in practice.
Method
Systematic searches across five databases identified relevant studies. Critical realist analysis employed the Person-Centred Practice Framework as analytical infrastructure, maintaining appropriate epistemological boundaries for secondary literature. The JBI checklists assessed methodological quality, and thematic synthesis examined conceptual patterns, research approaches and structural mechanisms shaping practice.
Results
Seventeen studies were included: 13 qualitative studies, 2 quantitative studies, and 2 systematic reviews. Geographic concentration was striking; 76% originated from Sweden, where ambulance personnel are nurse-trained rather than paramedic-trained, representing fundamentally different professional preparation for scopes of practice. Analysis revealed systematic tensions across three domains. Conceptually, paramedics lack shared understanding of what person-centredness means for emergency practice. Relationally, they navigate emotional regulation, power asymmetries and temporal constraints that challenge person-centred ideals. Ethically, they face conflicts between autonomy principles and risk management demands. A fundamental paradox defines current practice: paramedics demonstrate excellence in relational care yet reject person-centred language, citing poor conceptual clarity and lack of profession-specific guidance.
Conclusion
The articulation of person-centredness is largely absent from paramedic-specific evidence. Systematic tensions expose gaps between theoretical ideals and practice realities shaped by structural constraints, organisational cultures and professional hierarchies. Without paramedic-led research and context-specific frameworks, person-centredness risks remaining borrowed rhetoric rather than authentic professional identity. Future research must develop profession-specific conceptualisations that bridge policy frameworks, educational programmes and practice cultures to embed person-centredness within paramedic professional identity.
Keywords
Introduction
Contemporary paramedicine faces a substantial challenge in balancing the pace of professional evolution with quality care delivery. While the discipline has transitioned from emergency response and transport services to autonomous, evidence-based healthcare provision,1–3 this rapid advancement has outpaced the development of supporting educational frameworks and practice standards. 4 Traditional models of paramedic education have been scrutinised regarding their alignment with the complexity of contemporary practice. 5 Despite advancements, both systematic and scoping reviews6,7 identify that practice has outpaced scientific understanding 7 compounded by inconsistencies in teaching methods, content and clinical experiences.8,9 This suggests there is a need for more scientific, holistic and integrative approaches to education and practice. 5
Paramedics operate in diverse, often unpredictable environments where they encounter people requiring not just clinical intervention but compassionate, dignified care. Person-centredness represents a research-based, global standard for individualised, collaborative healthcare delivery 10 which may offer an appropriate philosophical framework for paramedic practice in out-of-hospital environments. This framework is derived from medicine and nursing, 11 requiring in-depth exploration of how person-centred principles might relate directly to paramedicine. Therefore, this hybrid scoping/methodological review aims to explore what insights the international literature offers regarding the conceptualisation and implementation of person-centredness in paramedicine, and to examine paramedics’ understanding and delivery of person-centred practice (PCP) in out-of-hospital environments.
Background and context
Over the past two decades, paramedicine has evolved significantly both nationally and internationally. Ongoing pressures on healthcare systems and concerns about overcrowded emergency departments have driven considerable changes in the profession. 1 Contemporary paramedics no longer solely respond to emergencies and transport patients to hospitals; they have become autonomous healthcare professionals utilising comprehensive, evidence-based practices.2,3 This transformation has necessitated new approaches to out-of-hospital healthcare delivery and professional development, 10 creating opportunities and challenges for paramedics to expand their practice and work more collaboratively with patients. 12
Despite paramedicine being recognised as an essential component of wider healthcare systems, achieving consensus on a universal definition of paramedicine remains elusive. 13 This definitional ambiguity has led to inconsistent terminology across different contexts and uneven development of practice standards. 14 Eaton 15 contends that these discrepancies contribute to professional inconsistency, with paramedic practice evolving unevenly across countries and even among states and provinces. Furthermore, Colling-Hughes et al. 16 argue that variation in regulatory functions and lack of self-governance prevent paramedics from experiencing the same global mobility as other allied healthcare professionals. These challenges raise fundamental questions about professional identity: what a paramedic is and does, and the implications of being a paramedic.3,17 Central to addressing these questions of professional identity and standardisation has been the evolution of paramedic education itself.
Educational evolution and challenges
To promote greater standardisation, paramedic education in the United Kingdom (UK) has transitioned from short, in-house apprenticeship-style programmes to university-based undergraduate degrees. 18 The Health and Care Professions Council 19 (HCPC) has elevated minimum qualification requirements to a bachelor's degree, with the paramedic title now legally protected, 17 ensuring paramedic education meets the academic standards expected of registered professions. However, Cavanagh et al. 4 argue that advancements in paramedicine may have outpaced the scientific understanding needed to support these practice changes. This gap is compounded by the distinctive attributes that characterise paramedicine and set it apart from other disciplines, which pose unique challenges necessitating innovative strategies for practice-based learning and education. Addressing these challenges requires theoretical frameworks that can support both the advancement of paramedic practice and the humanistic values central to healthcare delivery.
Person-centred practice
One approach to enhancing collaborative, respectful paramedic professionalisation involves drawing on person-centredness principles. 13 McCance, McCormack20,21 defines person-centredness as ‘A global movement in healthcare, because it reflects the importance of keeping the person at the centre of healthcare systems. It prioritises the human experience and places compassion, dignity and humanistic caring principles at the centre of healthcare delivery that are translated through relationships that are built on effective interpersonal processes’(p. 2).
Over the past two decades, McCormack and McCance 22 have developed this philosophy into a comprehensive mid-range theory, operationalised through the Person-centred Practice Framework 22 (PcPF). This framework is increasingly integrated into strategic documents and practices across various healthcare sectors, 23 providing a structured approach to implementing person-centred principles in clinical practice.20,24
The PcPF's 22 five constructs are ordered from outside to inside (Figure 1), culminating in achieving a healthful culture, the expected outcome of developing effective PCP. A healthful culture is characterised by shared decision-making (SDM), collaborative relationships, transformational leadership and support for innovative practices. 22 While person-centred care (PCC) has long been associated with nursing, it fundamentally involves treating people as individuals, respecting their rights, fostering mutual trust and understanding, and developing therapeutic relationships, representing a standard that keeps patients central to care delivery. 25
Person-centred practice framework. 22 (p27)
Implementation challenges and knowledge gaps
Despite growing recognition of the significance of person-centred cultures in healthcare education and clinical practice, 26 McCormack 10 asserts that while ‘person-centredness is the aspired standard of healthcare globally, its conceptualisation and translation across multiple contexts remain a challenge’ (p. 85). Although person-centredness has influenced healthcare strategy development, there is a notable absence of accompanying government arrangements and work programmes supporting full implementation. 27 Failure to integrate person-centred principles into practice results in patients and their families reporting poor care experiences across healthcare systems. 28 Additionally, healthcare staff, including paramedics, work in challenging environments where overall care quality assessment is often unsustainable. 29 Effective PCP implementation requires evaluating the interplay between practitioners’ competencies and role commitment, as well as the care delivery environment.
Critically, there has been a lack of literature exploring person-centredness specifically within out-of-hospital environments and paramedic roles. This represents a notable knowledge gap given the unique nature of paramedic practice. Unlike other healthcare professionals who work in controlled clinical environments, paramedics function within emergency medical services, where they practice under medical guidance or autonomously in unplanned, unpredictable and rapidly changing situations. These challenging circumstances raise the fundamental question: How does paramedicine conceptualise and implement person-centredness in the reality of practice? This hybrid scoping/methodological review addresses this question by examining conventional paramedic practice, where practitioners are dispatched to address medical and traumatic emergencies.
Aim
This review aims to explore what the international literature reveals about person-centredness in paramedicine and out-of-hospital care, examining both the conceptualisation and implementation of PCP and the methodological approaches.
Method
Design
A hybrid scoping/methodological review was conducted to examine how person-centredness has been conceptualised, operationalised and theorised within paramedicine research. This approach enabled a comprehensive mapping of the research landscape while critically examining the methodological and theoretical approaches employed, identifying both explicit findings and implicit assumptions embedded in research design choices. The philosophical foundations and analytical approach are detailed below, followed by the systematic search and screening process.30,31 The scoping component mapped research breadth, whilst the methodological component critiqued research approaches; both required synthesising how researchers have conceptualised person-centredness across diverse studies.
Search strategy
Multiple digital and online searches were conducted using databases including CINAHL Ultimate, Medline (Ovid), PubMed, Scopus and Web of Science. The initial phase comprised two steps. The first step involved the research team identifying and defining the research topic to ensure its originality and suitability, as well as determining the questions that required exploration within the literature. 32 As the research question centres on how paramedics provide person-centredness, a combination of two sets of terminology was chosen to ensure a high level of relevance in the resulting search. The commissioning of Emergency Medical Services (EMS) varies internationally, being classified either as public health or public safety organisations. The researchers aimed to ensure comprehensive representation by including ambulance clinicians, paramedics, Emergency Medical Technicians (EMTs) and ambulance nurses to achieve a thorough global perspective. The inquiry was designed to search across all fields in the databases, adhering to inclusion and exclusion criteria (Table 1).
Inclusion and exclusion criteria.
This ensured that information was screened in all categories (including title, abstract, topic, affiliations, etc.). Moreover, no restrictions were placed on the publication year of the papers, as paramedicine, as a profession, is continually evolving. To supplement the findings, searches of grey literature were conducted, which involved the examination of repositories (e.g. TRIP), catalogues and additional reference lists for relevant literature. Only papers published in English were selected. Both MeSH terms and truncation techniques were employed in the individual databases (Figure 2). 33
PRISMA flow diagram.
The initial search generated 77 papers, which were managed using Covidence software. 34 Two researchers independently assessed the titles and abstracts in accordance with the established inclusion and exclusion criteria (Table 1), leading to the selection of 23 studies for full-text extraction. The full-text papers were subsequently screened against the criteria in consensus with a third researcher. Any scheduling conflicts were resolved through discussion with a third researcher, although this was not necessary. One researcher conducted forward and backward citation chaining to identify additional eligible studies.
Ontological and epistemological positioning
This review adopts a critical realist ontology,35,36 acknowledging that person-centredness is a phenomenon whose enactment is shaped by underlying structures, contexts and power relations within healthcare systems. Critical realism conceptualises reality as stratified across empirical (observable phenomena), actual (occurring events) and real (underlying mechanisms) domains. 37 This stratification is particularly relevant for examining person-centredness, where disparities between ideals, documented practices and structural enablers/constraints reveal analytically productive tensions.38,39
The epistemological approach integrates interpretivist and critical realist principles 40 while maintaining appropriate boundaries for secondary literature. Recognising that published research represents interpreted accounts already filtered through researchers’ methodological choices and theoretical frameworks, we therefore analyse how person-centredness has been conceptualised and researched rather than claiming direct access to participant experiences.
Positionality and reflexivity
The review team brings multiple perspectives: LMcA (lead reviewer) is a paramedic with 20 years’ experience and a Clinical Support Officer and doctoral researcher, providing insider knowledge while requiring careful attention to ensure that professional familiarity does not replace rigorous engagement with evidence. TMcC (supervisor) co-developed the PcPF 22 and brings deep theoretical expertise from nursing contexts, requiring collaborative negotiation about applicability to paramedicine's distinct professional identity. DG (supervisor) provides external perspectives and methodological rigour less embedded in either paramedicine or PCP traditions. Throughout the analysis, a reflexive awareness was maintained by distinguishing textual evidence from professional inference; interrogating patterns that aligned professional expectations; using review team discussions to surface divergent interpretations; and attending to what existing research does not address.
Methodological approach
This review employs a critical framework-informed methodology to examine how person-centredness has been conceptualised, operationalised and theorised within paramedicine research, a hybrid of the scoping review methodology 41 and the critical methodological review. 42 The PcPF 22 provides an analytical infrastructure rather than a rigid coding framework. The PcPF conceptualises person-centredness as multi-dimensional (prerequisites, practice environment, person-centred processes, outcomes) and enables systematic examination of which dimensions existing research addresses, and which remain underdeveloped. This framework, validated across healthcare contexts,10,43 provides theoretical sensitivity while allowing for paramedic-specific adaptation. The following analytical approach operationalises these critical realist and framework-informed commitments.
Analytical process
Critical realist principles shaped analysis in four keyways: multi-level data extraction attended to empirical (reported findings), actual (contextual descriptions) and real (proposed mechanisms) domains, examining both what researchers found and how underlying mechanisms were theorised. Whereas retroductive reasoning37,44 worked backwards from observed patterns to identify generative mechanisms. When geographic, professional or methodological patterns emerged, we examined what structural factors might produce them and their implications for transferability across paramedicine contexts. Contradictions were treated as indicators of structural tensions 39 rather than noise, reframing implementation challenges from individual deficits to systemic constraints. Framework-informed gap analysis used the PcPF 22 to identify which constructs received research attention, revealing what dimensions of person-centredness paramedicine research privileges or marginalises. Analysis proceeded iteratively through familiarisation, collaborative pattern identification, critical framework application and reflexive integration.
Power dynamics and limitations
In order to pay attention to power dynamics, during analysis the research team remained cognisant of the PcPF's 22 nursing origins. This necessitated critical awareness of whether we imposed external frameworks rather than developing indigenous paramedicine theory. As practitioner-researchers, we navigated tensions between professional loyalty and critical analysis and remained mindful that published research provides uneven access to interest holders’ perspectives. This approach enabled critical examination of conceptualisations, identification of methodological patterns, analysis of theorised mechanisms and recognition of knowledge gaps. Working with a framework-informed assessment of comprehensiveness did not enable access to latent meanings in the original participant data, generate new empirical claims from synthesis alone or represent beyond what published research documents. 45 This epistemological honesty justifies the necessity of subsequent primary research while maximising legitimate insights from existing scholarship.
Quality appraisal
During the data evaluation stage, the screened papers were assessed for methodological quality. Qualitative studies were evaluated using the Joanna Briggs Institute (JBI) Checklist for Qualitative Research. 45 Quantitative studies were assessed with the JBI Analytical Cross-Sectional Studies checklist, 46 while systematic literature reviews were evaluated using the JBI Checklist for Systematic Reviews and Research Syntheses. 47 Consistency with the JBI critical appraisal tools was scored as either Yes (1), No (0), Unclear (0) or Not applicable (0), and a total score was calculated for each paper to indicate its relative quality. Although a range of quality was identified, no papers were excluded based on this appraisal due to the limited existing research in the field. Inclusion prioritised theoretical contribution, each study's potential to illuminate conceptualisations, contexts, mechanisms or structural factors shaping person-centredness, over methodological rigour alone, consistent with critical realist principles that value explanatory depth. 36 However, the quality ratings and limitations were reported for each study (Table 2).
Summary of the included papers (n = 17).
* Qualitative studies were evaluated using the Joanna Briggs Institute (JBI) Checklist for Qualitative Research (Lockwood et al. 45 ).
** Quantitative studies were assessed with the JBI Analytical Cross-Sectional Studies checklist (Moola et al. 46 ).
*** Systematic literature reviews were evaluated using the JBI Checklist for Systematic Reviews and Research Syntheses (Aromataris et al. 47 ).
Data extraction and analysis
Data extraction and synthesis were conducted using thematic synthesis approaches appropriate for scoping and methodological reviews.48,49 One researcher independently extracted data from each included study relating to how person-centredness was conceptualised, operationalised and investigated in out-of-hospital contexts. The extracted data were confirmed by the supervisors and compiled into a data matrix. Themes were developed through an iterative process of identifying patterns, convergences and divergences across the included studies regarding definitions, methodological approaches and reported findings related to person-centredness. This systematic synthesis enabled the identification of key conceptual and methodological patterns within the existing research literature. 49
Results
Search outcomes
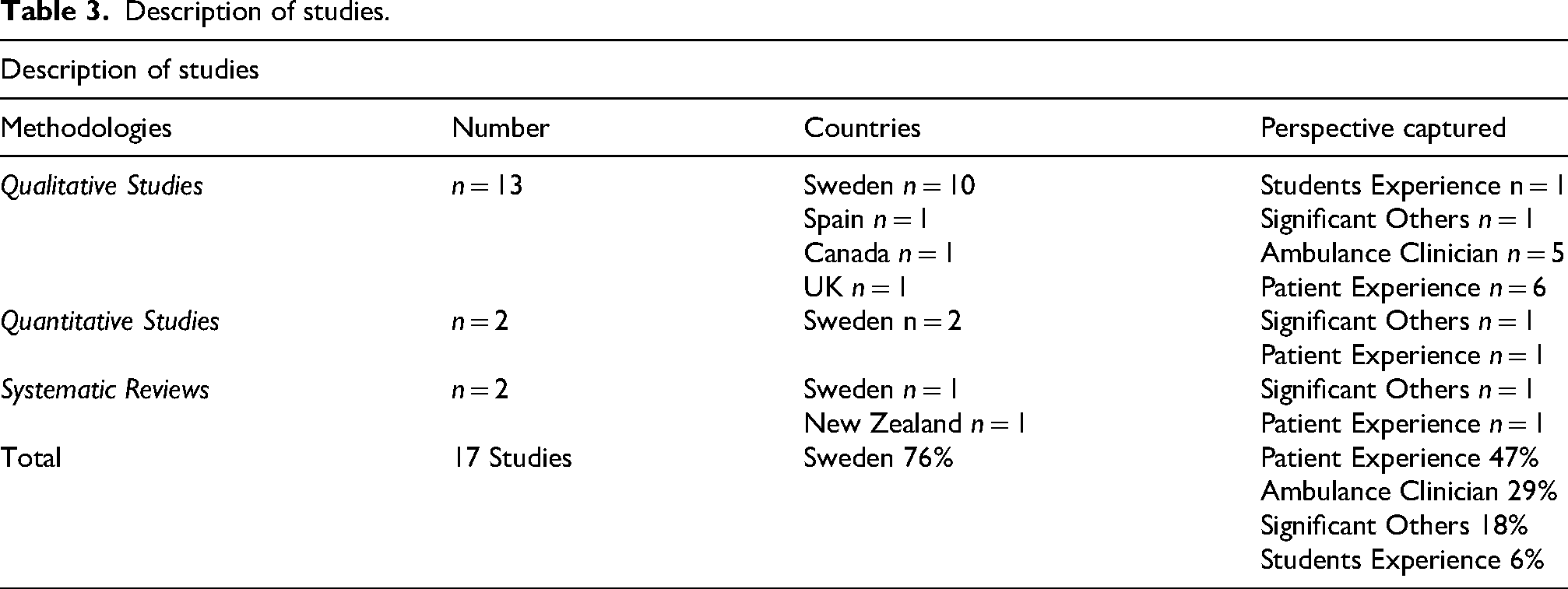
This hybrid scoping/methodological review analysed 17 papers, comprising 13 qualitative studies, 2 quantitative studies, and 2 systematic reviews. The research concentrated on experiences of person-centredness within out-of-hospital emergency and urgent care settings. The largest portion (47%) explored patients’ experiences, while 29% examined ambulance staff's perspectives, 18% considered significant others’ (SOs) perspectives and 6% reflected student paramedics’ perspectives (Table 3). The papers predominantly originated from Sweden (76%) and included ambulance clinicians, paramedics, EMTs, and nurses working on ambulances. Analysis revealed six interconnected themes clustering around three domains: conceptual foundations (lack of shared understanding), relational dynamics (emotional regulation, power, temporal constraints) and ethical-practical tensions (autonomy, risk management). Each theme reveals contradictions between person-centred ideals and practice realities, shaped by the notable geographic concentration of existing research originating in Sweden. Each theme is explored in depth below.
Description of studies.
Conceptual landscape
Lack of shared understanding
The evidence reveals a core misalignment between theoretical conceptualisations of person-centredness and its operationalisation in paramedic practice. Whilst consistent patterns emerge that emphasise core values, respect, dignity, compassion and patient involvement as equals,50,55,63 this consensus masks persistent conceptual ambiguity. Most studies failed to provide explicit definitions of PCP, using ‘patient’ and ‘person’ interchangeably, defaulting to unidirectional biomedical perspectives and failing to acknowledge alternative philosophical frameworks. This definitional vagueness has consequences for practice implementation. Rantala et al. 60 found that some paramedics described person-centredness as a mere ‘catchphrase’(p. 9) that offered no substantive improvements to care delivery. The authors argued that in the absence of a shared philosophical foundation, PCC risks being reduced to superficial rhetoric or procedures, rather than being enacted as a comprehensive, rational approach to care.
Only one study 13 explicitly employed an established theoretical framework to examine person-centredness in paramedicine. McAteer and Brown 13 found paramedic students demonstrated a fundamental understanding of person-centred values and their connection to safe, compassionate care. However, students combined person-centredness with patient-centredness, recognising the centrality of the patient but failing to comprehend that person-centredness also encompasses collaboration within the professional team. The authors noted that implementing comprehensive person-centred frameworks presents important challenges in paramedic education and practice settings, suggesting that translating theoretical frameworks into emergency care contexts requires some adaptation.
Emotional regulation
The evidence revealed that out-of-hospital care occurs within contexts of acute emotional volatility for patients, families and practitioners. The waiting period for ambulance arrival generates considerable emotional distress.50,52 Patients and SOs can experience fluctuating emotional states: heightened anxiety and fear about their condition, uncertainty about the situation, perceived loss of control and sometimes anger or frustration stemming from prior healthcare experiences or trauma.51,58,61 Feelings of helplessness compound this complexity, as patients face pressure to navigate complex decisions without adequate support. 62 Satchell et al. 62 positions emotional regulation, the psychological process of modifying emotional intensity to respond to environmental challenges, 62 as essential to person-centred out-of-hospital care. However, as paramedics working environments differ markedly from the stable healthcare settings, other practitioners work within, there is a need for them to balance their own emotional regulation with sensitivity to patients’ emotional states.55,62,64
Managing emotional volatility requires recognising and responding to patients’ psychological states, 56 with practitioners’ ability to cultivate safe environments and demonstrate compassion significantly enhancing patients’ emotional well-being. The literature demonstrates convergence on holistic approaches to managing emotional dysregulation, but it stops short of explaining how paramedics can systematically achieve this emotional alignment under severe time pressure and environmental constraints. Tikkanen and Sundberg 65 emphasise the subjective nature of health, particularly for older adults, advocating for care discussions that address psychological, social and emotional dimensions alongside clinical concerns. Lindström et al. 56 demonstrate that tailoring interactions to patients’ psychological states is essential in psychiatric emergency care contexts. However, the literature provides limited empirical guidance on operationalising these emotional competencies within the acute time constraints and challenging environmental conditions that define out-of-hospital care. A gap remains between recognition of emotional regulation's importance and evidence-based guidance on its operationalisation within emergency response.
The power of powerlessness
The available literature reveals a paradoxical power dynamic inherent to emergency paramedic practice. Whilst patients and families experience acute vulnerability and powerlessness during medical crises, the structural positioning of paramedics inadvertently amplifies these asymmetries. 54 Paramedics enter patients’ homes during periods of intense suffering and distress, 54 encountering individuals at their most vulnerable. This vulnerability manifests across multiple dimensions, emotional, physical and psychological pain, leading to feelings of powerlessness or surrender to practitioners’ authority.55,56,62 SOs, immersed in the crisis yet ill-equipped to confront it, experience parallel powerlessness.54,58,61 This vulnerability intersects with structural hierarchies embedded within healthcare delivery. The ambulance uniform itself signifies power and authority derived from professional knowledge, skills and social legitimacy, 64 creating fundamentally unequal relationships.58,64 Svensson et al. 64 consider the consequences are behavioural with patients tends to conform to paramedics’ views even when they disagree, often remaining silent in the face of ambiguity 64 (p73). Tikkanen and Sundberg 65 shapes the response by perceived illness, knowledge gaps, 65 and the hierarchical structure of the healthcare encounter. Holmberg et al. 54 argue that these dynamics place responsibility on paramedics within these temporary relationships, as patients operate from positions of disadvantage.
High-quality out-of-hospital care is essential because it often represents patients’ initial contact with the healthcare system,54,64 occurring in challenging environments that serve as ‘last resorts 64 (p75)’. Addressing power imbalances requires intentional skill deployment, empathy, adaptability and rapid trust-building. A key theme across the evidence is that trust, effective communication and respect for dignity constitute the most crucial elements of therapeutic relationships.51,64 Rantala et al. 61 specifically advocate for patient involvement as a mechanism to equalise power dynamics. However, the evidence reveals a tension.50,60,61 Whilst person-centred ideals demand power-sharing and collaborative partnerships, emergency contexts embed structural hierarchies that systematically disadvantage patients. The literature acknowledges this complexity but does not resolve how paramedics can effectively counterbalance these power differentials.
Autonomy and engaging in shared decision-making
The literature conceptualises autonomy as both a fundamental ethical principle and a relationally constituted practice, revealing tensions between theoretical ideals and pragmatic constraints in emergency care. 61 Autonomy operates as self-determination centred on patients’ capacity to make rational decisions and moral choices.54,63 This requires that individuals receive comprehensive information about their condition, treatment options, risks, benefits and alternatives, including the right to refuse care even when refusal may lead to harm. 64 However, this individualistic framing is challenged by evidence suggesting autonomy operates relationally, shaped through social interactions rather than being an isolated attribute. 52 Decision-making capacity emerges as the central constraint on autonomy with researchers agreeing that patients must possess cognitive ability to comprehend information and recognise the consequences of decisions.50,61 However, emergency contexts frequently involve individuals with impaired capacity, particularly older adults with cognitive impairments. 61 This creates a fundamental ethical dilemma: how to respect self-determination when capacity is compromised. The evidence suggests that paramedics must continuously assess capacity whilst adapting to individual situations and ethical considerations,55,63 yet there is limited guidance on how this occurs under time pressure.
SDM emerges as a mechanism to operationalise autonomy in practice, enabling care congruent with patient preferences, enhanced patient knowledge, reduced anxiety and improved clinical outcomes. 62 However, realising these outcomes in time-pressured emergency contexts requires paramedics to assess capacity whilst preserving dignity and facilitating rapid, meaningful participation, a notable departure from traditional emergency response models focused primarily on clinical stabilisation 13 This includes recognising decision needs, understanding available evidence and incorporating patient values and preferences into choices. Tikkanen and Sundberg 65 position acknowledging patients’ reality and unique personhood as essential to preserving dignity within this process.
Being in a temporary presence
The intense time pressures inherent in paramedic practice create profound challenges for delivering PCC that distinguish emergency response from other healthcare contexts. The literature consistently characterises paramedic-patient encounters as brief, intense and focused on immediate medical interventions or technical procedures.13,53,64 Studies describe this as an obstacle to a comprehensive understanding of individual needs, values and preferences, elements identified as crucial for PCP. 13 Students and practitioners alike observe that forming therapeutic relationships appears unrealistic given time constraints. 13
Despite temporal limitations, the evidence suggests these brief encounters carry disproportionate relational significance. Initial impressions prove pivotal, with paramedics’ expertise, experience and interpersonal skills substantially influencing patients, particularly older adults with cognitive impairments and frailty effects. 59 Rantala et al. 61 characterise the relationship that develops as ‘a surrender from one's own struggles to dependence on others and trust in ambulance clinicians. 61 (p251)’ They describe it as dynamic, ongoing, yet inherently fragile. This fragility is compounded by the dual focus required: encounters primarily involve addressing medical issues whilst simultaneously managing patients’ and families’ frustration and fear,53,58 which limits opportunities for deeper relational development.
The literature converges on a resolution to this temporal constraint: paramedics must cultivate trust by equally emphasising technical medical interventions and relational skills, 64 establishing trust and security in patients and SOs. 51 However, this prescription reveals an unresolved tension in the evidence. Studies acknowledge that therapeutic relationships are foundational to effective PCC, yet paramedic practice operates within temporal parameters, encounters measured in minutes, that fundamentally constrain relationship development. The literature acknowledges this constraint,56,61,63 but offers limited insight into how practitioners can achieve the relational depth person-centredness demands within encounters characterised by brevity rather than sustained contact. This represents a gap between person-centred ideals and the operational realities of emergency care delivery.
Ethical risk management
Fear of reprimand for incorrect decisions generates internal conflict that compromises ethical conduct and accountability,52,55 manifesting in defensive medicine and reliance on risk-averse guidelines and protocols. 63 This reflects an embedded culture of blame influenced by the prevailing medical paradigm, 60 producing a consequential dynamic: paramedics may adopt paternalistic approaches, making decisions on behalf of patients, potentially against their will. This practice conflicts directly with autonomy. 63 The literature frames this as a core ethical dilemma involving the weighing of risks against patients’ best interests.52,55 Bennesved et al. 50 conceptualise paternalism as an ethical perspective that overrides patient values in favour of another's judgement, 50 (p6) raising questions about whether decisions meet the ‘best interests’ standard. Whilst Jacobsen et al. 55 acknowledge that clinical guidelines and standards ensure appropriate care, they argue that these should be applied judiciously, considering individual patient circumstances. Through such an application, defensive practice may be precluded.
The scope of ethical risk management extends beyond individual patient encounters to encompass patient safety, legal compliance, advance care planning and harm disclosure.62,64 Nonetheless, these multiple accountabilities demands create pressures that push practitioners towards protocol-driven rather than person-centred responses. The literature reveals an organisational context that systematically constrains this agency through blame cultures and risk aversion.54,57 Studies document the phenomenon but provide limited evidence on how paramedics might navigate ethical complexity to preserve both patient safety and person-centred principles.50,52,62 Achieving person-centredness in paramedic practice may thus require not only individual skill development but fundamental shifts in organisational cultures that currently prioritise defensive practice over relational ethics.
Methodological landscape
How person-centredness has been researched in paramedicine: geographic and professional context of the evidence base
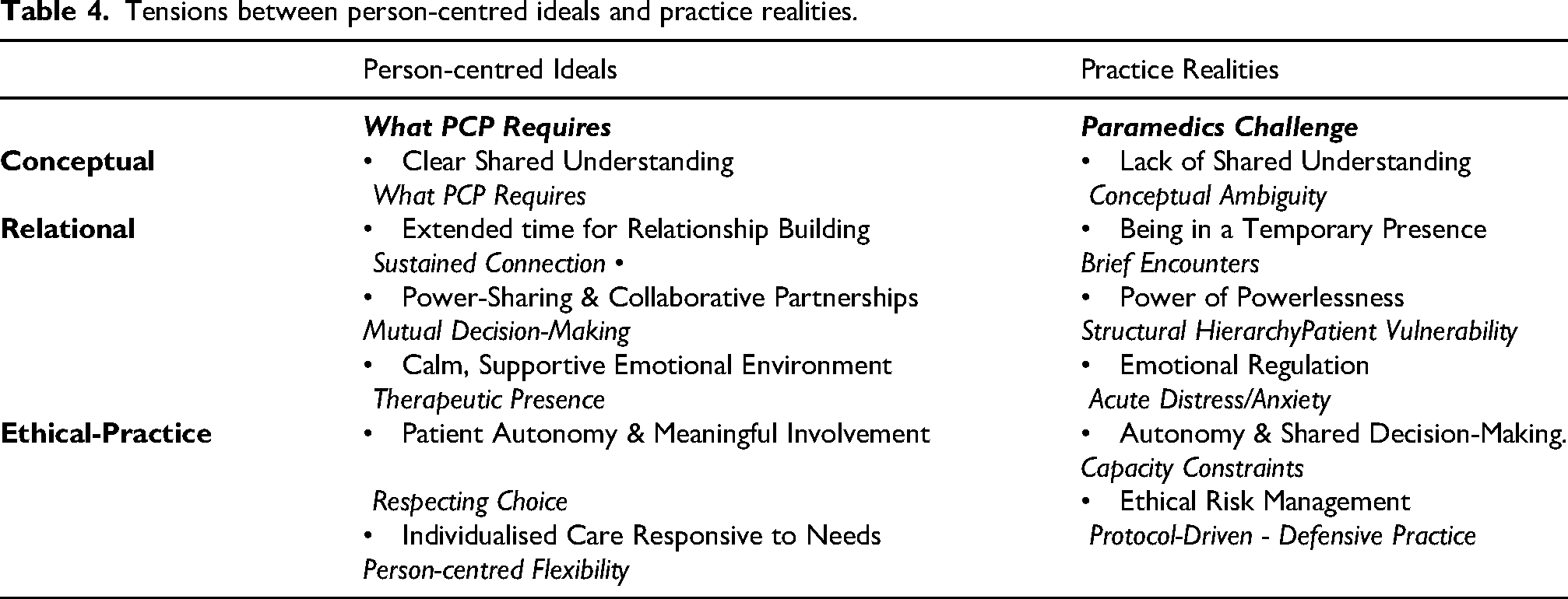
The evidence base for person-centredness in out-of-hospital care reveals a striking geographic concentration that fundamentally shapes knowledge claims in this field. Thirteen of the seventeen included studies (76%) originated from Sweden, with the remaining research conducted in other countries. This concentration reflects a particular professional context: in these countries, ambulance personnel are predominantly trained as nurses before specialising in out-of-hospital care.53,63,64 This geographic clustering has profound implications for knowledge transferability. Person-centredness has been fundamental to nursing philosophy and education for decades, embedded within nursing curricula and professional identity formation. In Sweden, when ambulance personnel enter out-of-hospital care with established nursing foundations, person-centred values and frameworks are already integrated into their professional worldview. The literature reviewed here thus represents person-centredness as understood and practised within a nursing-derived professional context, not paramedicine as a distinct profession. This distinction becomes critical when examining the tensions between person-centred ideals and emergency practice realities. Table 4 synthesises these tensions across conceptual, relational and ethical-practice domains, revealing a complex landscape that existing evidence, generated predominantly within nurse-trained contexts, has not adequately addressed paramedics as a distinct professional group.
Tensions between person-centred ideals and practice realities.
This matters critically for international applicability. In the United Kingdom, Ireland, Australia, North America and many other countries, paramedics are trained through dedicated paramedicine programmes distinct from nursing. These educational pathways emphasise different philosophical foundations, often prioritising emergency medical intervention, rapid decision-making and protocol-driven care over the relational, holistic emphasis characteristic of nursing education. 65 The absence of person-centredness research in paramedicine contexts suggests that PCP has not been studied in traditional paramedic training systems or that research has not kept pace with emerging educational innovations. 66 Ulster University in Northern Ireland represents a notable exception. The paramedic science degree is explicitly underpinned by the PcPF, 22 demonstrating that person-centredness can be intentionally embedded within paramedic education, independent of its nursing heritage. 13 This makes Northern Ireland a unique research context, a paramedic-led system with person-centredness formally integrated into professional formation. To date, this innovation remains largely absent from international literature.
Discussion
This review reveals a fundamental paradox: paramedics instinctively provide relational care yet fail to recognise these practices as person-centredness. Despite person-centredness representing the global standard for healthcare delivery, 10 its conceptualisation and implementation in paramedicine remain poorly understood. Analysis identified six conceptual tensions between person-centred ideals and practice realities, exposing critical gaps in how person-centredness translates into out-of-hospital emergency care.
The literature consistently integrates PCC with person-centredness by treating patients with respect, dignity and compassion, involving them as equals, and affirming self-determination.50,55,63 The studies frequently highlight the pivotal role of the patient and their SOs in the therapeutic relationship with paramedics. 51 They articulate attributes that foster a supportive and reassuring environment through empathy, dignity and calm communication. However, in the general literature, patient-centredness does not fully incorporate the roles of families and SOs. In contrast, the paramedic profession explicitly includes these individuals in its practice. Consequently, while discussions may centre on patient care, actual delivery of care demonstrates a commitment to person-centredness. 22
The lack of clarity in the literature regarding how PCP differs from PCC, as well as the implications of these terminologies, often leads to them being considered interchangeable. However, this presents a challenge. Person-centredness is increasingly being defined by only one or two of its more popular or appealing elements. 67 Nevertheless, this perspective fails to encompass the comprehensive nature of person-centredness by endorsing a constricted interpretation of the iterative mid-range theoretical model of the PcPF, 22 which was developed from practice for use in practice. 68 The PcPF conveys the dynamic nature of person-centredness, acknowledging the intricacy present at various levels within the wider healthcare systems. It defines healthfulness as the primary outcome of fostering person-centred workplace cultures. Healthfulness refers to creating an environment in which individual health and the well-being of everyone are central.
Evidence suggests that PCP remains little more than a catchphrase in paramedicine. Practitioners view it as offering no meaningful practice enhancement, dismissing it as a ‘trendy concept’. 60 Without adequate paramedic input, PCP feels like another checklist, inauthentic and imposed from outside the profession. This resistance reflects a historical identity crisis in paramedicine. The profession's core identity remains rooted in its origins as a trauma-focused emergency service, 9 creating tension between public perceptions and practice realities. Paramedic competencies have evolved slowly, failing to match the changing landscape of out-of-hospital care. 69 The profession has evolved from ‘humble stretcher bearers’ 70 to autonomous, critically thinking practitioners, 71 yet education and mindset have not evolved. The PcPF 22 offers a different approach, a multi-professional framework enabling authentic engagement with people's beliefs and values. Crucially, this framework encompasses not just patient interactions but collaborative work with colleagues across organisational levels. It requires paramedics to understand knowing self, their values and the importance of strategic leadership.22,27 Research has yet to explore how paramedics may undervalue these attributes, potentially rendering person-centred implementation superficial or context-dependent. 3
Person-centredness emerged partly as a response to the limitations of traditional biomedical models, particularly in practitioner-patient interactions. 72 The reviewed studies confirm that paramedic assessments remain primarily biomedically driven, particularly in emergency situations.55,62 These assessments prioritise systematic, rapid surveys to identify time-critical issues and facilitate transport to definitive care.73,74 The biomedical model reduces patients to collections of signs and symptoms, criticised as paternalistic and system-centred rather than patient-focused. 75 This critique extends beyond paramedicine to medicine, radiography, occupational therapy and physiotherapy. Killingback et al. 74 found that physiotherapists engage in critical reflection about their roles and language in shaping care experiences. Like paramedicine, physiotherapy lacks a singular definition of person-centredness but shows consensus on fundamental principles.
The hybrid scoping/methodological review identified patterns in how existing research has conceptualised the centrality of the patient and SOs in interactions with ambulance services. The studies highlight the internal turmoil experienced during these encounters, emphasising the heightened emotional states associated with physical or emotional anxiety. Terms that encapsulate these feelings include distress, fear, anxiety, frustration, helplessness and powerlessness.56,61,62 This is evident in the broader literature, which indicates that paramedics possess a heightened awareness of the complexities involved in entering the lives or homes of patients during times of significant suffering and distress. 76 The current undergraduate curriculum for paramedics and the accompanying in-house education primarily focuses on accidents and emergencies, such as trauma and cardiac arrest. However, these incidents account for only a small proportion of the calls to which paramedics respond. 77 Therefore, it is essential to emphasise that the relational aspect of care is intrinsic to the paramedic profession, even in the absence of formal education. Paramedics unwittingly cultivate connections by aligning with individuals’ beliefs and values, engaging authentically, being sympathetically present, and facilitating SDM. This approach promotes a psychologically and physically safe environment. 78 These person-centred processes, described by McCance and McCormack, 22 are foundational to delivering PCP.
In these brief encounters, an implicit power dynamic emerges, suggesting that paramedics may inadvertently assume a greater degree of responsibility. It can be characterised as a paradoxical situation. 13 McCann 79 posits that paramedicine is a crucial component of public safety in dynamic and unpredictable environments, necessitating attributes such as discretion, autonomy, emotional intelligence, situational awareness and the ability to make adaptable, real-time decisions. Eaton 80 argues that paramedics’ inherent ability to establish rapport and cultivate trusting relationships alleviates anxiety merely through their presence, creating a space for a ‘harmonious relationship’ that fosters collaboration between the patient and paramedic. 81
Contradictions in the paramedic-patient relationship are present across the literature. Researchers suggest patients seek self-determination and involvement in decision-making, but instead experience acute powerlessness.52,63 This creates an unusual dependency wherein patients trust paramedics completely while remaining uncertain about their own role in care decisions. In contrast, paramedics face the flip side of this dilemma. They constantly navigate what's ethically correct versus medically appropriate within their scope of practice. However, the broader literature challenges any suggestion that relationship-building should compete with clinical competence. 82 Brooks 83 argues that biomedical expertise remains fundamental to effective paramedic care. Gage et al. 84 assert that the primary objective of EMS is to ‘preserve life and limb’. This must take precedence over therapeutic relationships. Actual professional competence requires two types of knowledge working together: Declarative knowledge of concepts and theories, and Procedural knowledge, applying skills in practice. Neither alone creates competence; paramedics require both. 85
This creates a persistent tension paramedics may know precisely what clinical protocols demand but struggle to balance these requirements with individual patient needs. 13 The situation becomes more complex when considering patient preferences. Warner et al. 86 argue that patients often avoid difficult conversations, preferring to let situations unfold naturally while deferring to medical expertise, which challenges the ideal of SDM. In high-pressure situations, patients often lack the medical knowledge necessary for truly informed choices. 87 Paramedics should facilitate decisions rather than make them, but what happens when patients can’t or won’t engage?. To manage these challenges, paramedics rely on safety strategies: crew resource management, optimised procedures and structured communication protocols. 1 These approaches reduce errors and provide measurable performance standards. However, standardisation comes at a cost. Systematic protocols may overlook individual needs, particularly for persons with complex, multiple conditions. Lydahl 88 warns that excessive standardisation strips away individuality, creating homogeneous care that fails to recognise what makes each person unique.
A fundamental contextual factor, the practice environment, was largely overlooked in the reviewed studies. While challenging conditions facing paramedics in pressured healthcare systems were acknowledged, no studies examined how these environments impact care delivery. Paramedics face a dual burden. They must manage complex medical emergencies while simultaneously addressing the emotional distress of patients and their families, a distress often heightened by extended waiting times.52,57 The PcPF 22 reveals why the environment matters so much. Practice environments are complex ecosystems encompassing the environment, people, processes and structures. 22 These elements interact dynamically, directly affecting clinical effectiveness, team performance and patient outcomes. 89 McConnell et al. 90 demonstrated this environmental impact in emergency departments. They uncovered that high-pressure, protocol-driven settings forced practitioners into internal conflicts between professional duties and personal values, resulting in medical technical care consistently winning out over PCC. These pressured environments create what McCormack et al. 91 call ‘person-centred moments’, brief opportunities for authentic connection amid routine tasks. However, Clissett et al. 92 warn that practitioners rarely capitalise on every opportunity. For paramedics in high-acuity settings, the challenge becomes clear: how to synthesise these sporadic moments into consistent person-centred cultures. The solution may lie in enhanced integration of medical interventions with relational care through targeted person-centred education.
Strengths and limitations
This hybrid scoping and methodological review offers important insights into how paramedics conceptualise and implement PCP. The synthesis of diverse research methodologies, including qualitative, quantitative studies and other reviews, strengthens the evidence base and provides a comprehensive perspective on current practice. However, several limitations must be acknowledged. As detailed above, most studies originated from Sweden, where ambulance personnel are nurse-trained rather than paramedic-trained, creating a notable contextual difference. This geographic concentration limits the breadth of contexts and highlights essential gaps in the evidence base across different healthcare systems and cultural contexts. Additionally, the review captures a snapshot of paramedic practice that may not fully reflect the profession's rapidly evolving scope of practice. Future research should examine person-centred approaches across diverse international settings to address these evidence gaps and develop a more contextually nuanced understanding of implementation strategies.
Conclusion
The findings from this rigorous hybrid scoping and methodological review identified that the articulation of person-centredness is largely missing from the available paramedic evidence. Analysis revealed fundamental tensions between person-centred ideals and paramedic practice realities. Paramedics lack a shared understanding of person-centredness principles, leading them to dismiss it as rhetoric whilst instinctively enacting relational care. Structural challenges compound this conceptual gap: the brevity of encounters limits relationship-building, paradoxical power dynamics create vulnerabilities for both patients and paramedics, capacity constraints complicate meaningful autonomy, acute emotional distress demands constant regulation and risk-averse cultures prioritise protocol-driven defensive practice over individualised care. Despite these barriers, the evidence consistently demonstrates that paramedics instinctively provide relational care, they simply fail to recognise this practice as person-centredness.
The evidence base suggests that there is a need to explore ways in which paramedics can enact person-centredness in the reality of everyday practice. This may require examining paramedic practice across multiple jurisdictions, exploring how educational programmes can authentically integrate person-centredness without dismissing the distinctive constraints of out-of-hospital emergency care and ensuring that policy frameworks support working in person-centred ways. Only through such comprehensive research can paramedicine develop a profession-specific understanding of person-centredness, one that reflects the profession's distinct identity whilst honouring the relational care paramedics already instinctively provide.
Footnotes
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.