
Abstract
Objective
To explore paramedic students’ understanding and experience of the perceived facilitators and barriers to implementing person-centred care in urgent and emergency practice-based placement situations.
Aim
To explore paramedic students’ understanding of this concept and how it may be applied to clinical practice.
Methods
A non-probability convenience sample of participants was drawn from a second-year undergraduate Bachelor of Science (Hons) programme in Paramedic Science, at a United Kingdom university. The programme was underpinned by the Person-centred Practice Framework. Undergraduate paramedic students participated in face-to-face, audio-recorded, semi-structured interviews. A qualitative reflexive thematic analysis was then conducted to identify themes arising from the data.
Results
Ten participants were interviewed. Four key themes emerged from the data: (1) realising person-centred prerequisites which have two sub-themes – curriculum and reality of practice, (2) challenge of high-acuity calls, (3) developing a rapport with vulnerable people and, (4) factors in the macro environment.
Conclusion
Paramedic students witnessed moments of person-centred practice and were enabled to reflect on their learning experiences in positive ways, by working with paramedics/practice educators. However, their person-centred ideals were constantly challenged as students negotiated to work in complex, dynamic situations and in a health system under pressure.
Introduction
Paramedicine has reached a critical juncture, both globally and nationally, as it evolves alongside the ongoing whole-system approach to safe and effective healthcare.1–3 In recent years, pressures on the healthcare system, including concerns about overcrowded emergency departments, and undignified care facilities for patients, 4 have led to significant changes in paramedicine and the role of paramedics. 5 This role has developed from that of a humble stretcher bearer 6 to a critically thinking registered autonomous practitioner. 7 Contemporary paramedics are required to develop their professional identity and demonstrate professionalism in all aspects of their practice. In the United Kingdom (UK), new approaches to pre-hospital healthcare delivery 8 and professionalisation to an all-graduate profession are providing opportunities and challenges for paramedics to expand their practice and work with people in more collaborative ways.
One approach to increasing collaborative, respectful paramedic professionalisation is drawing on the principles of person-centredness. The seminal work of McCormack and McCance9,10 outlines a robust philosophical and theoretical framework for PCC that is increasingly becoming embedded into strategic documents and practice across healthcare. 11 Person-centredness is an approach to healthcare delivery that places the person at the centre of all decision-making, through informed choice 12 at the individual, family, and community levels, while also considering the organisational culture in which people are receiving healthcare. Frequently, PCC is understood as focusing only on the patient, leading to debate regarding the interpretation and transferability of a shared language of person-centredness and many misunderstandings of the terms and concepts. 13 For example, the terms ‘patient-centred’, ‘relationship-centred’, and ‘person-centredness’ are used interchangeably, though they mean different things. McCormack and McCance 7 argue that person-centredness is all-encompassing and focuses on all people who use or work in healthcare settings. Thus, all people have the right to be respected as a person for the individual choices they make and enabled to make informed decisions, through the fostering of healthful relationships. This includes ensuring that staff have the necessary prerequisites to support patients’ decision-making. Such aspirations are mirrored in the World Health Organisation's 14 conceptual framework, which emphasises building systems where people are provided with education and knowledge to make informed decisions.
In its drive towards professionalisation, paramedicine is required to build renewed education programmes that will equip the next generation of paramedics with enhanced skills to practice effectively. 15 While professional standards 16 and guidelines facilitate this transition, the true skill of professionalism may not be so much in ‘knowing what to do’, as ‘when to do it’. 16 This means embracing new ways of working while remaining cognisant of the unique skills paramedics already possess. Givati et al. 17 suggest undergraduate programmes play a significant role in shaping professions. Furthermore, in academic discourse, universities are commonly conceptualised as a space where individuals engage in the construction of professional knowledge as a fundamental aspect of their academic journey while simultaneously developing shared professional characteristics. 18 One way for paramedicine to achieve this is by drawing on the concept of person-centredness and examining the ways in which it has been integrated into nursing curriculum development. According to Cook et al., 15 the development of person-centredness through curriculum design offers a way of aligning curricula with the healthcare practice environment.
The new paramedic science undergraduate programme in a university in the UK is based on the Person-centred Practice Framework (PcPF). 10 The curriculum's philosophy ensures, that as well as learning about medical-technical interventions, graduates acquire the knowledge, skills, attitudes, and values necessary to provide person-centred, professional, competent, safe, and effective care. 19 This equips the new paramedic graduate to be emotionally intelligent and capable of managing their own health and well-being, as well as empowering individuals and communities to exercise choice and assume responsibility for their health and behaviours.10,15,20,21 Currently, the value of PCC in improving the quality of healthcare and service user satisfaction is widely recognised as the cornerstone of nursing theory and practice.10,22 However, McCormack and McCance argue that the PcPF offers a multi-professional framework that can be applied across the spectrum of care. 10 Nevertheless, there is a dearth of international research linking person-centred care to pre-hospital care (paramedicine). This study aims to explore paramedic students’ understanding of this concept and how it may be applied to clinical practice.
Methods
Qualitative approach
A qualitative exploratory cross-sectional methodology was adopted to explore the understanding and experience of PCC among second-year paramedic students during their practice-based placement (Table 1). This strategy offered an efficacious methodology for elucidating the facilitators and barriers of PCC in practice placements and is particularly pertinent when there is limited knowledge regarding this concept in the field of paramedicine. 23 A codebook approach which aligns with reflexive analysis when it comes to emphasising a qualitative philosophy in coding was considered. 24 The proponents of codebook approaches acknowledge the interpretive nature of data coding and do not rely on positivistic conceptions of coding reliability. 25 However, a reflexive thematic analysis approach was selected as the framework for this study owing to its versatility and theoretical adaptability. Braun and Clark's 26 methodology utilises a qualitative approach with the objective of identifying patterns and comprehending the experiences, perceptions, and understandings of various participants regarding this new phenomenon within paramedicine.
Research objectives.
Research question
To explore paramedic students’ understanding of the perceived facilitators and barriers to implementing person-centred care in urgent and emergency practice-based placement situations.
Researcher characteristics and reflexivity
The lead researcher LMcA has experience in both clinical practice and as an educator, working as a registered paramedic and clinical support officer employed by the Northern Ireland Ambulance Service. DB is widely recognised for her research and practice, and expertise in person-centred practice. Additionally, DB holds the position of Senior Lecturer, in the university supervising MSc and PhD students. The research team has a background that gives them first-hand knowledge of the complexities and challenges that paramedic students may have to navigate in this new concept in pre-hospital care situations. Throughout the research process, the team consistently maintained an open and reflexive stance towards competing ideas and was careful to consider any potential bias that might have resulted from their personal experiences and preconceived notions. The significance of reflexivity in research is well recognised, as it serves to augment understanding of the setting context and enhance the validity, trustworthiness, and credibility of the research findings. During the study, the researchers embraced their collective experience in person-centred practice, paramedicine, education, and research, both before data collection and during data analysis. This enabled the researchers to gather and identify significant insights and opportunities to enhance PCC. The researcher's unique perspectives and reflexivity played a crucial role in expanding the research scope and ensuring that the findings were relevant to the lived experiences of paramedic students.
Research paradigm
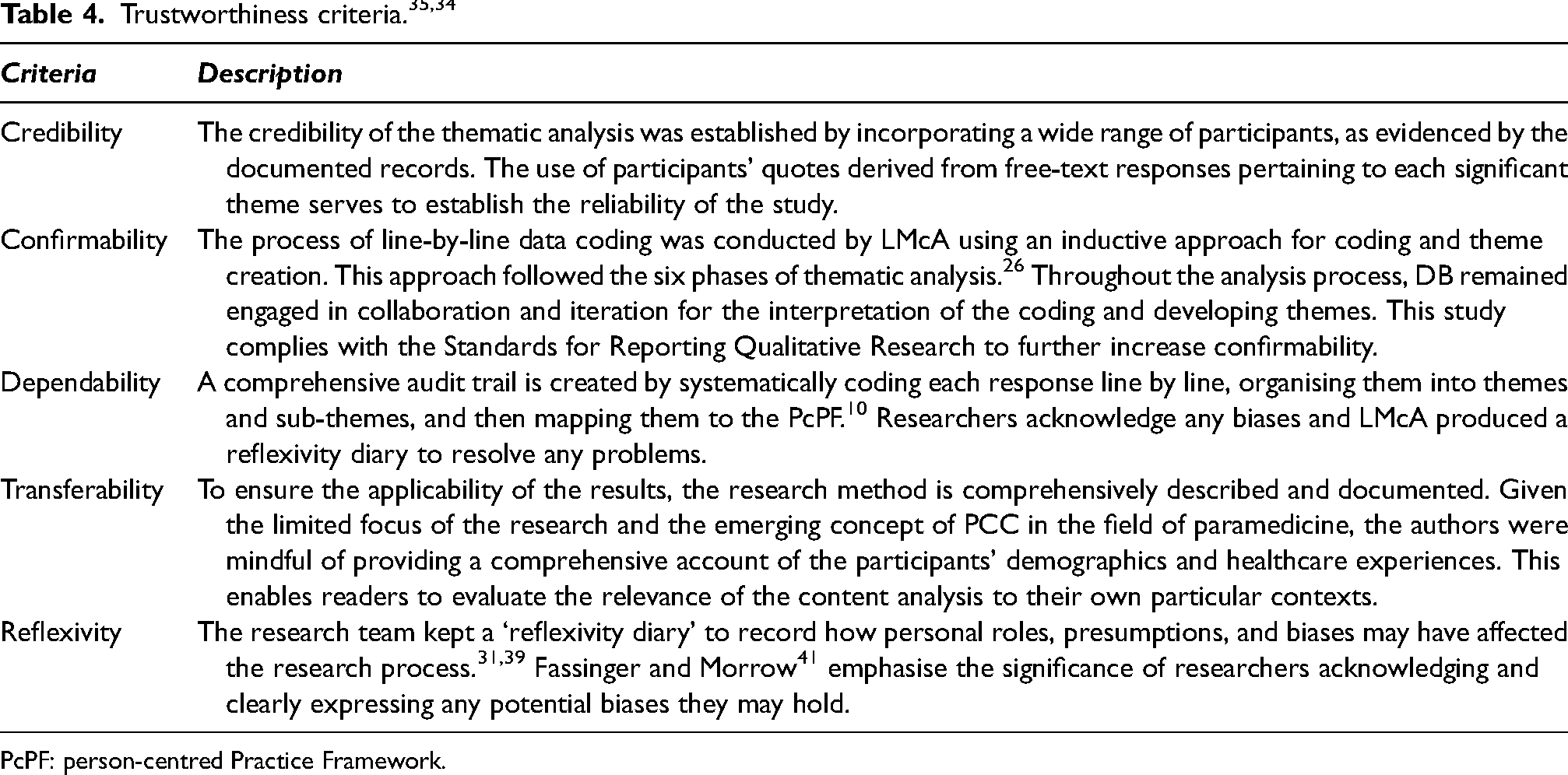
In this research, the lead researcher utilised an interpretivism approach and a constructivism theory to analyse the data. These perspectives acknowledge that knowledge is constructed through human experiences. Constructivism asserts that knowledge is constructed through scientific enquiries. It also challenges the notion that a singular methodology for generating knowledge exists. By employing constructivism theory in the healthcare field, researchers and participants endeavoured to critically consider facilitators and barriers to PCC in paramedicine. The combination of this epistemological stance and the interpretivism approach represents a philosophical perspective rooted in the belief that multiple realities exist. This worldview holds that each individual constructs their own unique version of the world based on their life experiences, perceptions, and beliefs. 27 For that reason, trustworthiness and rigour28,29 are essential aspects of qualitative research, as they depend on the confidence placed in the data, interpretation, and procedures used to ensure research quality.28–30 To achieve this, researchers have established protocols and methods which readers can review to ensure transparency, 28 such as reflexive journaling, triangulation, supervisor coding and data tables.30–33 These methods provide evidence of reliability and validity, as well as diminishing bias26,34,35 (Tables 3 and 4). Adopting this approach enabled the researchers to acknowledge the presence of multiple layers of reality while also recognising the complex interplay between theoretical 28 knowledge and its application to paramedicine clinical practice.
Setting and sample
A non-probability convenience sample was employed to capture a wide range of different perspectives. 36 Participants were recruited from the pre-registration database of second-year paramedic students who were undertaking a 3-year BSc (Hons) degree in paramedic science, at a UK university. The course director acted as the gatekeeper, and paramedic students who met the eligibility criteria were sent an invitation email with a participant information sheet attached (Table 2). If interested and willing to participate voluntarily, paramedic students were instructed to contact the researcher to gain further information and to consent to proceed with the interview. The study had an estimated n = 40 participants, with the first 10 being included in the research on a first-come, first-served basis. This number offered a reasonable representation of the target population and aligned with a sample size used in other studies involving nursing students on this topic. 37 This study aimed for ‘data saturation’, which can be considered ‘information power’.26,38
Inclusion and exclusion criteria.
Data collection
Semi-structured interviews were conducted in person and recorded using audio equipment. At the commencement of each interview, participants provided confirmatory verbal consent to proceed with the interview. The research team LMcA and DB developed an interview schedule through an iterative process. The interview questions follow Parahoo's 39 six primary questions. These questions were designed to align with the research objectives and were presented in a semi-structured format, with additional prompts to guide the interview process. The preliminary interview served as a pilot to facilitate learning and confirmed that no modifications were needed for the interview schedule. Recruitment was ongoing until the predetermined sample target was met, based on pragmatic considerations. The richness of the data collected also influenced the sample size to guarantee sufficient information power to address the research question.38,26
Analysis
Data analytic strategies
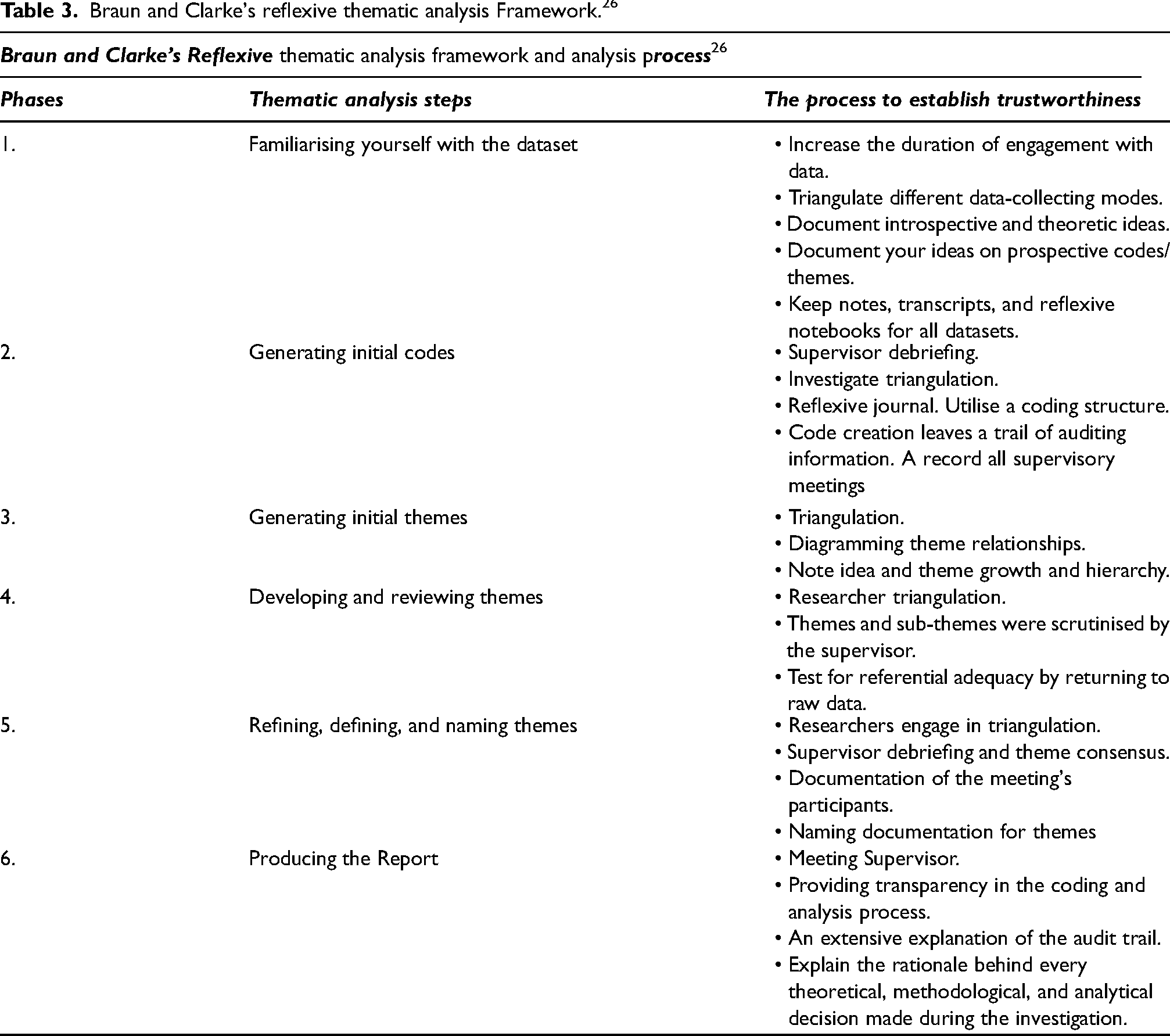
Interviews were transcribed verbatim by LMcA, compared with audio recordings to ensure accuracy, and subsequently anonymised and coded. Data was analysed using Braun and Clarke's 26 Reflexive Thematic Analysis Framework (Table 3) and mapped to the PcPF 10 (Figure 1) Data analysis was led by LMcA. The process of data analysis involved using an inductive approach for coding and theme development. Given the specific research question, the researchers focused on identifying themes at the semantic or explicit level. 25 The transcripts were thoroughly reviewed several times to become familiarised with the data. The initial codes were then organised into potential sub-themes and themes. The interpretation of the findings involved collaboration and discussion with DB throughout the analysis process. The trustworthiness of the approach proposed by Graneheim and Lundman 35 is characterised by five key elements: credibility, confirmability, dependability, transferability, and reflexivity (Table 4). Consequently, this article follows the Consolidated criteria for reporting qualitative research (COREQ) 32-item checklist as outlined by Tong et al. 40
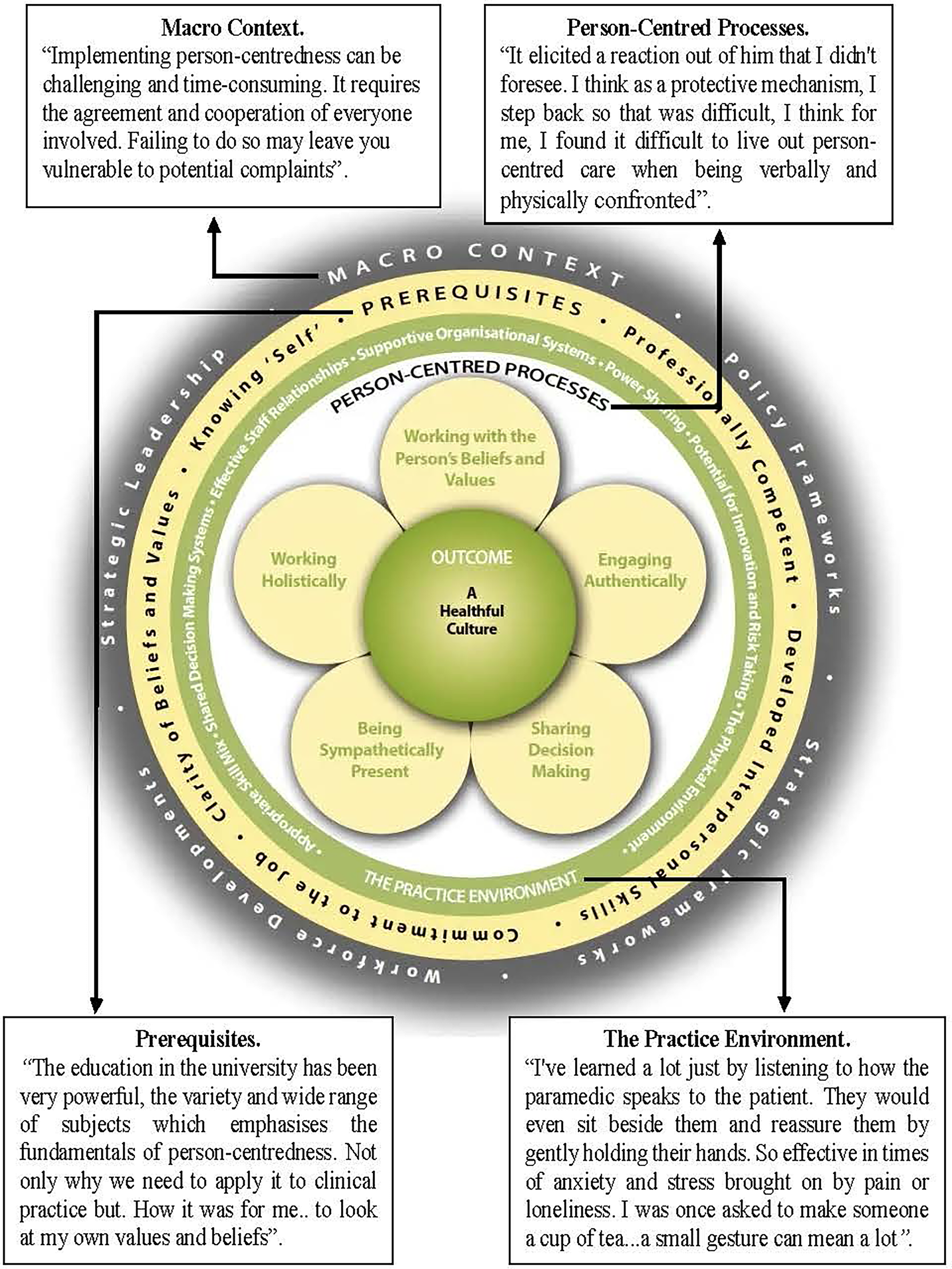
An example of data mapping to the person-centred practice framework. McCormack and McCance (2021 p.27).
Braun and Clarke's reflexive thematic analysis Framework. 26
PcPF: person-centred Practice Framework.
Ethics
Ethical approval was received from the Ulster University Institute of Nursing and Health Research Ethics Filter Committee (FCNUR-23-028). The Senior Leadership Team in the School of Nursing and Paramedic Science granted access to the paramedic students.
Results
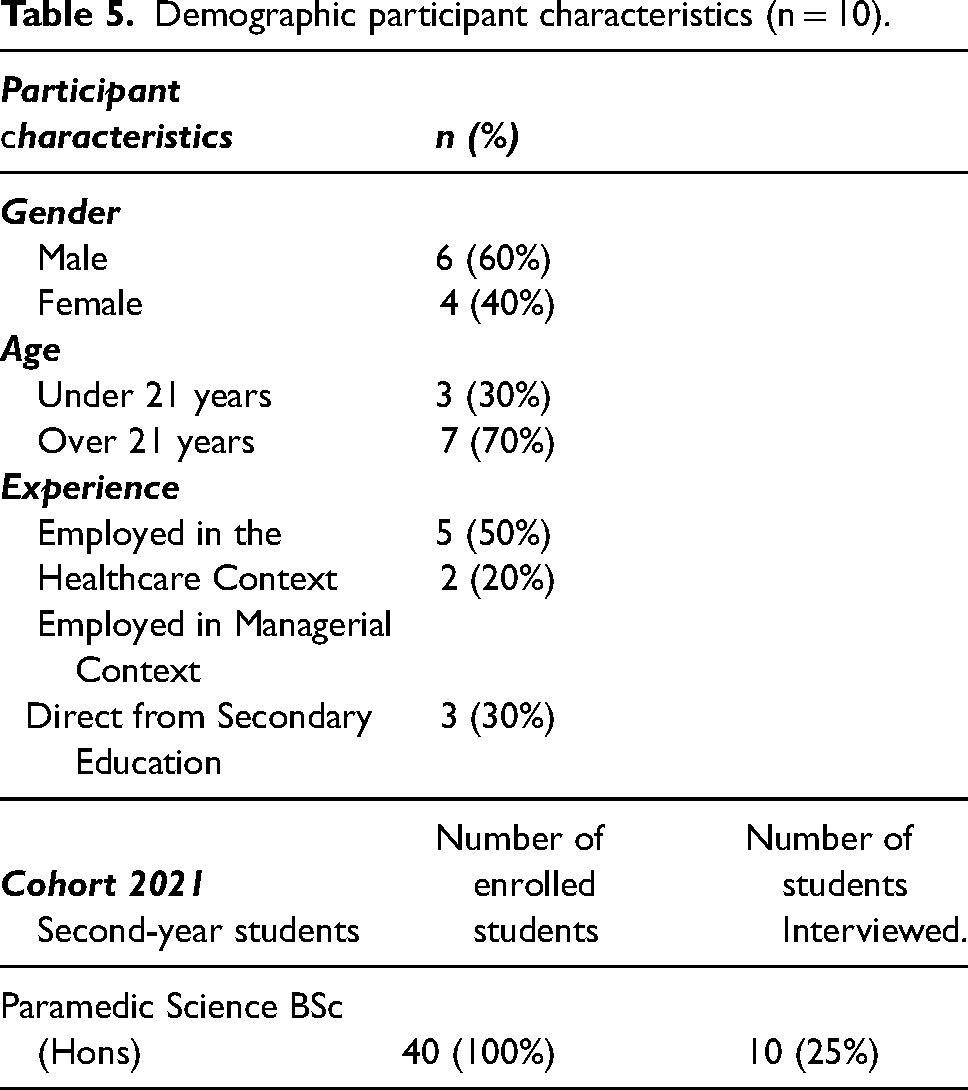
Data obtained through 10 face-to-face, audio-recorded, semi-structured interviews between June and July 2023, exploring the facilitators and barriers to implementing PCC in urgent and emergency practice placement situations, are presented below. The duration of the interviews ranged between 33 and 62 min, with a mean length of 46 min. The demographic characteristics of study participants highlight the variation in participants’ experience prior to undertaking the paramedic degree programme (Table 5).
Demographic participant characteristics (n = 10).
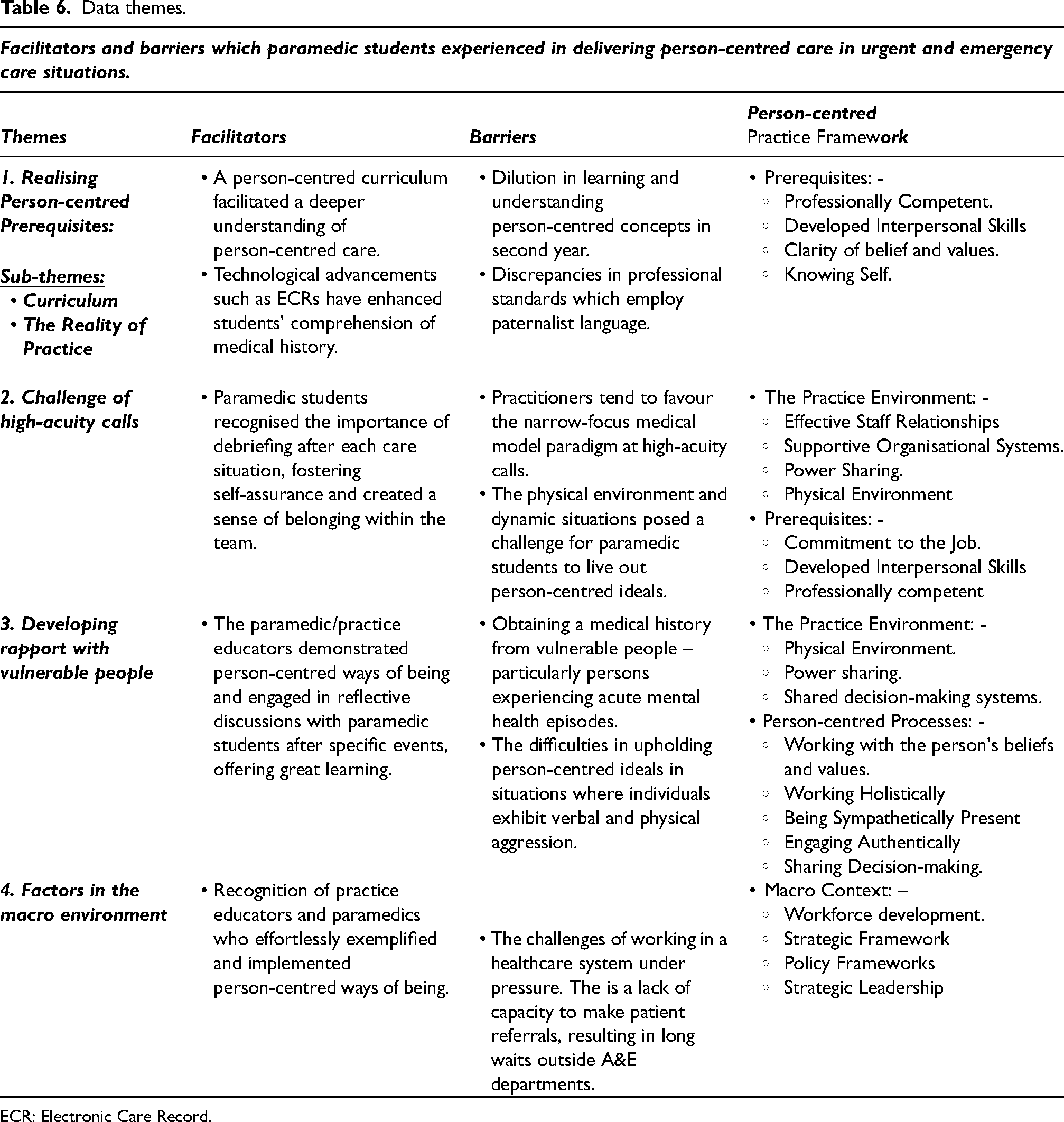
Thematic analysis of the data initially revealed 13 tentative themes. On further re-reading of the data analysis and discussion with the academic supervisor, four key themes emerged from the interview transcripts. Mapping the data findings to the PcPF 10 revealed that the arising themes linked to the concepts’ prerequisites, the practice environment, and person-centred processes (Figure 1). Findings revealed that the facilitators and barriers to implementing PCC into practice were realising person-centred prerequisites, the challenge of high-acuity calls, developing a rapport with vulnerable people and factors in the macro environment (Table 6).
Data themes.
ECR: Electronic Care Record.
Overall, while most participants reported that they understood the term and possible nuances of person-centred practice, there was some confusion about how person-centredness is related to all aspects of care, and paramedicine in particular. All paramedic students referred to patient rather than person-centred care. Their primary objective was to meet patients’ healthcare expectations and preferences during a specific episode of care. They emphasised the need to deliver adequate care for patients’ illnesses and injuries, regardless of how urgent or emergent the situation may be. However, none of the student participants articulated that person-centredness included the importance of the multi-disciplinary team and all those who work in healthcare, as well as having a patient focus. They only discussed the inclusion of all individuals involved in the care situation, including family, relatives, and the team, when prompted.
Realising person-centred prerequisites
Curriculum
Having experienced almost 2 years of a 3-year undergraduate degree course for paramedic education, all participants recognised that the degree programme facilitated the development of their knowledge and skills both theoretically and practically and was highly informative, with a particular focus on person-centred practice. The programme content was tailored to the participant's level of understanding. The written assessments were designed to incorporate person-centred practice and align with the learning outcomes.
“The education in the university has been very powerful, the variety and wide range of subjects which emphasises the fundamentals of person-centredness. Not only why we need to apply it to clinical practice but also…how it was for me… to look at my own values and beliefs”. [PS5]
“I feel we haven’t done as much with person-centred care this year. Person-centred practice should be woven through the whole paramedic BSc degree course. There has been little or no consolidation in the second year”. [PS3]
Reality of practice
All participants acknowledged that successfully completing practice placements, whether in community settings or emergency vehicles, enabled person-centred learning and was of great value. A majority of respondents considered that time constraints were not a factor in the community setting. The students considered that having access to Electronic Care Records (ECR) or referral documents prior to meeting with the patient enabled them to adopt a more person-centred approach to care. ECR access was valuable as it provided a more comprehensive understanding of the patient's background and medical history facilitating students to build a therapeutic relationship. On the other hand, emergency vehicle placement participants who did not have ECR at their disposal were surprised by how quickly therapeutic relationships developed with little information. Words such as ‘mutual respect’ and ‘professional demeanour’ were used to describe these relationships. All participants commented that paramedicine is not only about responding to high-acuity calls and saving lives but also about being there for patients who need guidance and support.
“I've learned a lot just by listening to how the paramedic speaks to the patient. They would even sit beside them and reassure them by gently holding their hands. So effective in times of anxiety and stress brought on by pain or loneliness. I was once asked to make someone a cup of tea…a small gesture can mean a lot.”. [PS2]
Challenge of high-acuity calls
Interviews revealed that the participants considered the practice environment related to high-acuity calls, such as major trauma, cardiac arrests, actively convulsing patients, and time-critical patients, presented significant difficulties in upholding the core principles of PCC. Participants described the experiences as hectic, crowded, noisy, demanding, and stressful. All agreed that their main objective was to ensure the safety and physical well-being of all individuals. In these situations, the participants acknowledged the importance of taking a systematic approach, based on the medical model of care. They realised the importance of having a comprehensive understanding of the pathophysiological processes involved in each situation, in order to make effective decisions. They acknowledged that the approach focuses on technical interventions and relies on established guidelines, protocols, algorithms, and mnemonics. Alongside these interventions, they spoke of an awareness of the time constraints and the need to consider, concepts such as the ‘golden hour’, the saying ‘time is brain’, and ‘time is muscle’. The participants described this approach as a task-focused activity.
“You're extremely resource-focused and protocol lead – to ‘keep on-scene time to a minimum”. [PS2]
“It requires a very quick decision, very structured and in an uncontrolled environment”. [PS4]
“When dealing with a major trauma, a time-critical call… once the intervention has been done – the paramedic resumes the person-centred approach…not alone with the patient but in some cases the family or relatives… always remaining calm.” [PS7]
Participants found high-acuity calls as anxious and tense experiences in which it was difficult for them to find their place or understand how they contributed positively to the team. Nonetheless, they spoke of how paramedics and practice educators gave them opportunities to reflect on and discuss these situations. This enabled them to develop insight into the rationale for the order in which each intervention was performed which provided enhanced learning. Additionally, paramedics and practice educators praised the students’ actions offering them clarity on their role. The participants were surprised by this, as they were made to ‘feel like an integral part of the team’, ‘enabling self-assurance’ in their clinical practice. “I have learnt so much from my practice educator, always willing to give me advice on how to tweak my cannulation skills.” [PS9]
Developing a rapport with vulnerable people
For this research, the definition of vulnerability as developed by Tavaglione et al.
42
(2015 p. 98) was used: ‘In healthcare, particularly vulnerable individuals are those who are more likely to have their interests unjustly considered’. All participants expressed the significant challenges they encountered when interacting with individuals whom they perceived as vulnerable. This includes individuals who are experiencing an acute mental health episode, those who have a dependency on alcohol, and individuals who misuse illicit drugs. All participants expressed difficulties with accurately assessing and managing people in acute mental health crises or those who were considered vulnerable people. In particular, students struggled to see how they could live out person-centred ideals and work with the person-centred processes when vulnerable patients were being aggressive.
“I believe that maintaining a person-centred approach becomes impossible when you or your crewmates are subjected to an assault”. [PS5]
“It elicited a reaction out of him that I didn't foresee. I think as a protective mechanism, I step back so that was difficult, I think for me, I found it difficult to live out person-centred care when being verbally and physically confronted”. [PS6]
All participants described how the paramedic/practice educators possessed the natural ability to intervene and safeguard the student while also deescalating the situation and working effectively with the patient. Even when patients were verbally aggressive and confrontational, the paramedic/practice educator's ability to read the situation and communicate succinctly and clearly in these circumstances impressed the participants. Role modelling person-centred ways of being paramedics/practice educators remained mindful of the patient's background and history, which may have led to these events. Watching how experienced staff managed situations and reflective discussions after specific events offered paramedic students great learning.
“My mentor assumed control and effectively assessed the situation, promptly separating the intoxicated patients. Afterwards, we discussed the importance of situational awareness, the challenges associated with managing volatile environments, and the duty of care”. [PS3]
Factors in the macro environment
Participants were aware of a healthcare system that is facing significant challenges, and how the role of contemporary paramedics is evolving to include the ability to assess, treat, refer, and discharge patients at scene. In situations where there was no urgency, student participants were not focusing on algorithms or guidelines, therefore facilitating them to fully embrace their person-centred principles and collaborate with the person's values. Under the supervision of the practice educator, students were given the opportunity to discuss the referral of patients to other services, such as direct assessment units or acute care at-home teams, therefore, enabling the students to actively participate in the decision-making process. However, the rigorous nature of the pathway's inclusion and exclusion criteria, the significant time investment required, to obtain verbal acceptance of the referral and the transfer of the duty of care for that patient, insufficient capacity available, and the implementation of risk mitigation through safety netting posed challenges to the participants.
“Implementing person-centredness can be challenging and time-consuming. It requires the agreement and cooperation of everyone involved. Failing to do so may leave you vulnerable to potential complaints”. [PS2]
“Sitting outside A&E departments for hours, you feel like you’re wasting resources. Because you hear over the radio, “Is anyone available to respond to Cat One emergency call”? You are aware that there's a cardiac arrest call in your area”. [PS8]
From a broad perspective, the participants were impressed by paramedics’ ability to work with person-centred principles, despite not having received formal education on the PcPF. 10 Some participants queried whether providing, paramedics and practice educators with a formal understanding of person-centredness and the PcPF 10 would impact clinical practice and enhance PCC.
“I believe that giving current … paramedics, who have been in the service for far longer than we have, the same kind of lecture that we received would have a significant impact on patient care”. [PS5]
Discussion
This study set out to explore second-year paramedic students’ understanding of person-centredness and what facilitated or hindered their ability to work in person-centred ways. The study found that paramedic students have a broad understanding of the theoretical principles of person-centredness and wish to work in person-centred ways. However, in placement, they experienced unpredictable and challenging environments, working with patients who were vulnerable and had complex needs. The findings will be discussed under the themes of a person-centred curriculum, a practice-based learning environment and person-centred ideals.
Person-centred curriculum
The findings from this study illustrate that person-centredness served as a central theme throughout the undergraduate curriculum and that paramedic students had a fundamental level of understanding of person-centeredness. Nevertheless, they showed that they understood the link between values, attributes and delivering safe, compassionate care to patients. However, participants felt that the PcPF 10 seemed very focused on nursing perspectives and were unsure how to enact it in their clinical practice. This suggests that care is required when adopting health models across differing healthcare professions, as one size may not fit all. McCormack and McCance claim that they developed the PcPF 10 with the multi-disciplinary team in mind and argue that it is transferable across healthcare disciplines. 43 The participants discussed the centrality of the patient, though did not grasp fully that person-centredness extended to how they worked with the professional team. Ultimately, the students saw person-centredness as being patient-centred. This finding supports previous research which outlined that generally there is widespread difficulty in discerning the distinctions between person-centred and patient-centred healthcare. 44 Additionally, this adds weight to the necessity of establishing a standardised language for person-centred concepts within all healthcare systems. This standardisation is crucial to achieve comprehensive recognition and understanding among all stakeholders involved in healthcare.45,46 Regardless of the language challenge, Steenbergen et al. 47 argue that the implementation of a person-centred curriculum can help students recognise person-centred concepts before they are exposed to the clinical practice environment. This is important, as the concept of person-centredness is now encompassed in many healthcare policies globally and nationally.14,48 The challenge is that curricula are influenced by a variety of factors across different professions 49 and for paramedicine across higher education institutions and practice settings. For person-centred ideals to be valued by paramedic students and lived out in practice, educators need to work together to develop models of learning that can be meaningfully adapted to suit the paramedic practice environment.
The advent of professionalisation in the field of paramedicine, as discussed by Gallagher et al., 50 has introduced a new paradigm wherein graduates are equipped not only with the necessary skills and competence but also with the ability to assume leadership roles within this evolving profession. The College of Paramedics 51 has advocated the implementation of a spiral curriculum that goes beyond rote learning. This approach recognises the importance of building on existing theoretical knowledge and practical skills. By encouraging learners to establish their own connections between these elements, the curriculum aims to facilitate a deeper understanding. It is understandable that paramedic students, in this study, did not recognise the important role that an explicit person-centred philosophy played in helping them acquire the knowledge, skills, and attributes needed for person-centredness. However, this philosophy is crucial to ensuring that what is learned can be effectively applied in real-world clinical settings. Furthermore, it reflects the broader research by Cook et al. 15 which shows that incorporating person-centred principles into a pre-registration nursing curriculum can effectively help students maintain their core values over time. This study's data illustrates the importance of creating integrated person-centred learning cultures in higher education, organisational, and clinical practice settings. 52
Practice-based learning environment
When second-year paramedic students were faced with challenging practice environments and competing priorities, all students expressed their focus on tasks and prioritised medical-technical competence rather than the provision of compassionate care. This is not unusual, as these findings resonate with research exploring person-centredness in emergency departments. 53 A potential reason for this could be that paramedicine aligns with the philosophy of medicine and is seen as a medically directed profession. According to Moore et al., 54 doctors tend to make decisions for patients rather than collaborate with them, as PCC is often seen as focusing on soft skills. Discrepancies exist where professional standards use paternalist language,55,56 rather than adopt the ideals of PCC and its actual implementation in clinical practice. Alternatively, paramedic students are experiencing the tension that exists due to a lack of readiness among practitioners and organisations to support a prevalence of person-centredness in healthcare, instead favouring a narrower focus on the medical model paradigm aspects rather than a whole-system approach. 57
Student participants considered that the focus on person-centredness in year 1 had reduced by year 2, resulting in a dilution in their learning and understanding of PCC. According to Steenbergen et al. 47 a person-centred curriculum helps students understand person-centred ideals before they pursue, them in healthcare settings. This suggests that there is a need for a consistent focus on person-centredness through all years of a curriculum with enhanced understanding and learning across the years to foster self-awareness among participants and illustrate the importance of gaining insight into one's own identity or knowing self, before being able to effectively care for others. Reflecting on previous research, by McCormack, 49 there is a strong emphasis on the importance of healthcare professionals having the ‘right’ moral attitude. Furthermore, the findings highlighted the importance of the prerequisites within the PcPF 10 that are seen as the cornerstone for the cultivation of proficient interpersonal skills among students. These newly acquired skills enable effective communication across diverse contexts, fostering the growth of practitioners dedicated to holistic approaches in clinical practice.22,58
Fostering productive interaction between staff members [students and practice educators] and people receiving care is problematic. The research findings revealed that students encountered difficulties in consistently implementing person-centred principles during their practice-based learning. In particular, there was uncertainty regarding how the principles of person-centred practice could be implemented when caring for patients in emergency situations. Students discussed moving between working in a technical way to stabilise patients before being able to adopt a more person-centred approach to care. While the PcPF 10 gained widespread acceptance as a professional standard among a significant number of paramedic students, the lack of consolidation of theoretical elements in year 2 of their learning acted as a barrier. Research has demonstrated that the PcPF 10 can have a substantial impact on how students develop their professional identities and beliefs.15,53
When faced with difficult situations in the practice environment paramedic students discussed that they either ‘step in’ or ‘step back’, from their comfort zone during care interactions. This observation aligns with Currie et al.'s 59 findings which are to motivate a more independent and self-assured learner who can ‘step in’ by incorporating strategies that promote active learning and engagement. This also resonates with existing pedagogical theories on active or passive styles of learning suggesting that self-initiated learning through practical application (doing) is more effective than solely relying on reading patient histories. Therefore, as evidenced by the participant's responses, the utilisation of technological advancements, specifically ECRs, has advantages within the paramedicine field to deliver more PCC. For example, participants initially suggested that developing therapeutic relationships was unrealistic due to their limited interactions and time with patients. However, these technological innovations contributed to enhancing students’ comprehension of medical history, promoting effective learning, and fostering the adoption of a patient-centred approach to healthcare provision. In contrast, in an emergency situation, student participants considered that therapeutic relationships were often formed with little background information. These relationships were built on mutual respect, which aligns with McCormack and McCance's 21 humanistic philosophy. This philosophy emphasises person-centeredness as a way of being, achieved through authentic engagement, and mutuality by way of ‘being with’ and ‘doing with’ through active participation. These results suggest that the therapeutic relationship goes beyond the stereotypical image of paramedicine.
Person-centred ideals
This study found that the majority of students openly discussed situations in which the values and beliefs of patients did not align with their own. All participants demonstrated a moral attitude that involved being sympathetically present 21 with the patient and expressing their understanding patients may be vulnerable because their values or lifestyle choices could be overlooked. Similarly, to previous research, Seedhouse 60 suggested that individuals may have differing opinions, values, and beliefs that healthcare professionals are required to work with. However, Masterson, 61 argues there are instances where it becomes necessary to have ‘challenging’ or ‘courageous conversations’ if a balance between risk management and respecting individual choices and preferences is to be achieved. In this study, there were instances where verbal aggression or physical confrontation arose unexpectedly, taking the student by surprise. As a result, students instinctively stepped back into their comfort zone, observing how paramedic colleagues managed the situation in order to learn from it. Benner's Stages of Learning and Skill Acquisition 62 and Polanyi's tacit knowledge 63 provide an explanation for why paramedic students reacted in this manner. Research has also explored the concept of person-centredness in nursing education, highlighting the fundamentals of tacit knowledge and skills that students acquire during their practice-based placement. 64 Furthermore, this finding reveals that simply teaching theoretical principles is insufficient to bring about a person-centred culture shift and address the knowledge gap in PCC. Instead, active participation in practice-based learning is necessary.21,63,64
All students recognised practice educators and paramedic colleagues as individuals who embodied and effortlessly put person-centred ways of being into action. The students were grateful for their supportive role, which was clearly demonstrated by their professionalism, willingness to share knowledge, and ability to offer protective skills. All students recognised the importance of debriefing after each care situation. They found that this practice had several benefits, such as fostering self-assurance and creating a sense of belonging within the team. Similarly, qualitative research by Gómez and Valdés 65 found that educators should ensure that the feedback they provide is supportive, timely, transparent, and practical. This can be achieved by encouraging students to critically reflect on practice and helping them to gain new perspectives through introspective learning. In Schön's 66 reflective practicum, a broader perspective is emphasised; one of the key aspects of professional practice is the ability to reflect on one's actions, engage in the ‘convergency of meaning’, and embrace the continuous learning process, all of which align with PcPF prerequisites. 10
Limitations
The findings of this research, while valuable, should be evaluated with consideration of various limitations. Firstly, the trustworthiness of the research reported here is an important consideration. The main researcher, who is a paramedic and an educator, may have unintentionally influenced the interview analysis because of her experience with paramedic students. Nevertheless, both researchers were cognisant of the possibility that pre-existing biases could impact the outcomes of the study and implemented strategies to mitigate these concerns. According to Braun and Clarke's Reflexive Thematic Analysis Framework, 26 maintaining a reflexivity diary 31 that documents personal roles, assumptions, and biases that may influence research is recommended. This technique employed a six-phase, iterative, and recursive process that promotes trustworthiness26,31 (Table 3).
In qualitative research, trustworthiness means the level of confidence in the researchers’ integrity in carrying out and presenting the results. 67 Despite Guba and Lincoln's 34 seminal writings related to trustworthiness, the concept has been criticised for the variations in how data may be interpreted. 33 To ensure transparency, the researchers were rigorous in how they analysed and triangulated the data, and offered a clear audit trail (Tables 3 and 4).28-30,32,33
To achieve further rigour, it may have been beneficial to use additional quantitative data sources to further establish identifiable patterns. For example, there are validated person-centred measurement tools available. 68 Introducing the Person-centred Practice Inventory-Staff 68 or the Person-centred Practice Inventory-Service User (unpublished) could offer a more comprehensive perspective of how person-centredness is perceived through a qualitative measure.
Most participants in this study were over the age of 21 years, as indicated by their demographics (Table 5). Therefore, it is important to exercise caution and not make generalisations about person-centred care and the broader population of paramedic students. These research findings should be considered in terms of their applicability to other contexts (transferability), 35 furthermore, by exploring the implications of person-centredness in clinical practice for both pre- and post-registered paramedics. It would be essential to do a comparative analysis of paramedic curricula across different countries and evaluate strategies for advancing person-centred practice. This would offer more insights into the implementation of person-centred care in the field of paramedicine internationally.
Conclusion
Despite an increasing focus on PCC within healthcare professions, there has been a noticeable lack of research regarding paramedic students’ comprehension and exposure to person-centred care in pre-hospital urgent and emergency care. This research explored undergraduate paramedic students’ experiences of person-centredness in practice environments. Participants identified that they witnessed moments of person-centred practice and were enabled to reflect on their learning experience in positive ways by working with paramedic/practice educators. However, their person-centred ideals were constantly challenged as students negotiated to work in dynamic care situations and experienced a mismatch between medical and nursing models of practice. Although the present study primarily focused on paramedic students, it is imperative to acknowledge the necessity of a top-down approach in establishing a strategic direction within paramedicine. Developing a comprehensive shared vision for person-centred care is essential to guiding the development of consultation strategies for policy and practice reform, by aligning person-centred principles to support paramedic practitioners to live out person-centred ideals and foster a healthful culture.
Supplemental Material
sj-docx-2-pam-10.1177_27536386241251499 - Supplemental material for Exploring undergraduate paramedic students’ understanding and experiences of person-centred care while on practice placement
Supplemental material, sj-docx-2-pam-10.1177_27536386241251499 for Exploring undergraduate paramedic students’ understanding and experiences of person-centred care while on practice placement by Lorraine McAteer and Donna Brown in Paramedicine
Supplemental Material
sj-docx-3-pam-10.1177_27536386241251499 - Supplemental material for Exploring undergraduate paramedic students’ understanding and experiences of person-centred care while on practice placement
Supplemental material, sj-docx-3-pam-10.1177_27536386241251499 for Exploring undergraduate paramedic students’ understanding and experiences of person-centred care while on practice placement by Lorraine McAteer and Donna Brown in Paramedicine
Supplemental Material
sj-docx-4-pam-10.1177_27536386241251499 - Supplemental material for Exploring undergraduate paramedic students’ understanding and experiences of person-centred care while on practice placement
Supplemental material, sj-docx-4-pam-10.1177_27536386241251499 for Exploring undergraduate paramedic students’ understanding and experiences of person-centred care while on practice placement by Lorraine McAteer and Donna Brown in Paramedicine
Footnotes
Acknowledgements
We would like to sincerely express my gratitude to all paramedic students who willingly participated in the interviews. They generously dedicated their time and shared incredibly touching and sincere accounts of their experiences during practice-based placements.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.