
Abstract
Introduction
Background
Leadership may be something of a contentious concept in academic literature. Published research addressing the character of leadership has been permeated by – and grounded in – an extraordinary range of different understandings of what it is to ‘lead’ in many practical contexts, and especially in healthcare.1–4 Leadership frequently defies routine or abstract definition in any given substantive sphere. With direct reference to paramedicine, Johnson et al. note an appropriate single definition for leadership is highly unlikely to emerge. 5 This paper argues, however, that this should not be viewed as an obstacle to research in leadership in the paramedicine domain, but rather a facilitating one. In this paper, paramedic leadership is addressed essentially as a phenomenological matter, ultimately rendered meaningful within the everyday experiences of working paramedics.
In England, where the research was undertaken, issues of healthcare leadership in the twenty-first century have become particularly salient. The consequences of a National Health Service (NHS) Trust not getting leadership ‘right’ are, for example, vividly outlined in the 2013 Francis Report into the Mid-Staffordshire Crisis. Cited throughout this inquiry's work is an account of poor leadership, amongst other failings, including wide cultural issues which ultimately led to preventable deaths. 6 The report led to a campaign run by the families of those who had died and, two years later, a comprehensive evidence-based review further underscored the importance of leadership in the NHS, with a clear link to its influence on outcomes such as patient satisfaction, mortality, financial performance, staff well-being and retention. 7 The standing NHS 10-year plan similarly recognises the key role of leadership in improving patient outcomes and organisational performance. 8 Current evidence further emphasises the importance of nurturing psychologically safe cultures where leaders can ensure staff are valued, supported, respected and cared for. Such a constructive approach has been shown to positively impact upon patient care and organisational performance.7,9,10
Following from the Francis Report, the NHS recognised the need to support and develop its leaders. The NHS Leadership Academy, active since 2012, aims to help leaders reach their full potential and promotes the highest standards in health and social care. 11 Despite Paramedicine in the UK having been a registered profession for nearly two and a half decades, there remains a relative paucity of paramedicine-focused research in this space. A recent report commissioned by the Association of Ambulance Chief Executives (AACE) into paramedic leadership recognised the trans-disciplinary relevance of many wider Allied Healthcare Professions (AHP) studies in the domain. The report confirmed a widespread need to support leadership development opportunities. 12
Despite strategic drivers being formulated to enhance leadership within the NHS,7,11,13–17 the Care Quality Commission (CQC) and the Office for Standards in Education, Children's Services and Skills (Ofsted) identified concerns when undertaking government regulatory inspections of ambulance services. The inspections recurrently documented issues of unsatisfactory, unproductive or actively dysfunctional leadership.18–21 In aggregate, these reports demonstrate higher-level leaders are often (a) out of touch with what happens ‘on the ground’ in their organisation, (b) neglectful of safeguarding responsibilities around staff and, in the worst cases, are (c) accountable for the growth of ‘toxic’ workplace cultures that actively condone bullying, harassment and sexual misconduct. The latter is further documented by the AACE and Office of the Chief AHP Officer in their joint report on reducing misogyny and improving sexual safety in the ambulance service. 22 Additionally, ambulance staff in England are now reporting poor mental health and well-being due to a lack of support from senior leaders, as opposed to the impact of clinical incidents 23 with bodies such as The Ambulance Staff Charity being founded to help staff navigate a variety of such challenging contexts.
The National Guardians Office was set up in the shadows of the Francis Report and has established avenues within the NHS to support staff in speaking out against negative experiences when they might otherwise feel unable to do so, known as ‘networks of freedom’. A Speak Up Review of ambulance trusts in England found many staff were routinely experiencing discrimination, bullying and harassment, with a continuing reticence to speak up at all. 24 ‘Command and control’ decision-making was reported in environments where favouritism and cliques were observed, with senior leaders reporting a varied understanding of ‘speaking up’. When staff did speak up, they reported inconsistencies with how cases were managed. Of note, these concerns were cited to be negatively impacting staff well-being and patient safety. 24
These finding are consistent with the 2024 NHS staff survey, 25 which highlighted that the English ambulance services mean score fell below the national average in all ‘people promise’ elements, that is, areas influenced by leadership and culture which relate to staff experiences at work. 26 Furthermore, a recent cultural review of ambulance services built upon these issues, further highlighting the challenges being faced by frontline staff. 17 Echoing the 2022 Messenger Review of leadership and management in the UK's health and social care sectors, 27 it was noted that effective leadership was highly salient in shaping a positive work culture, instrumental in improving patient outcomes and supporting individual staff facing a range of challenges. However, it was also observed that ambulance service leaders often prioritised operational performance measures over people and culture.
Although the current study (and the literature above) is situated within an English context, ambulance services in Finland have been reported to experience similar challenges relating to ineffective and/or dysfunctional leadership, ‘toxic’ cultures impacting staff well-being and morale and staff who feel unsupported, undervalued and reticent to raise concerns. 28 Furthermore, a recent Australian inquiry into complaints about discrimination and human rights breaches in Ambulance Victoria, found a range of drivers behind the breaches. These included a culture of power imbalance, tolerance of incivility, a focus on achieving key performance indicators over staff well-being and a culture of silence or not speaking up, within the organisation. 29
Rationale
Given the above triangulation of research, reports and reviews regarding leadership in English ambulance services, it is essential to better understand how frontline ambulance staff have experienced, and consequently come to perceive, leadership itself. This ensures any measures implemented by organisations, and their leaders, respond directly to their staff's real-world concerns and mandates in an evidence-based approach.
While the evidence above addresses leadership at every level within the NHS, the focus of this study is on senior leaders who have the specific ability to implement strategic change to effectively respond to the widespread issues reported. Senior leaders take greater responsibility for the performance of the organisation and receive greater financial reward for doing so. This is the group of staff explicitly cited in CQC reports as being most disconnected from frontline paramedics.18,19 For the purposes of this study, senior leaders are defined as those working at a senior operational level or higher, often associated with at least an NHS salary grade of band 8a, that is a leader who is responsible for a service or department. 30
At time of writing, there remains a dearth of peer-reviewed literature addressing leadership in the paramedic domain, a view supported by Wankhade and Murphy, 31 notwithstanding Wankhade's own contributions to this area.32,33 The authors recognise research directly addressing paramedics’ experiences of learning to be leaders and identifying/acquiring effective leadership skills.34,35 The authors also note previous contributions by McCann, 36 which explore the evolving profession of the paramedic and the challenges faced leading to stress and burnout, reflecting upon the role management and leadership has within this space. Additionally, Mildenhall's Thesis explored some of the psychological dynamics within social relationships of ambulance leaders and employees through the COVID-19 pandemic. 37 Whilst some of the pre-existing literature has a focus on first line and middle management, this study aims to directly explore the experiences of frontline ambulance staff regarding their senior leaders.
Some international research has begun to explore the experiences of frontline ambulance staff regarding their leaders28,29; however, limited published evidence directly relating to the English paramedic ambulance context exists.
Methods
Investigative framework
An exploratory-descriptive qualitative (EDQ) methodology, grounded in online semi-structured interviews, was used to understand English ambulance staff's perception of experiences with senior leadership. The EDQ offers a suitable framework for use in contexts where there is limited research and understanding. This approach goes beyond simply reporting upon observations and findings surrounding a phenomenon and instead seeks to examine the phenomenon itself through rich insights of participants’ experiences obtained via open-ended interviews. 38 This framework guided the research methods utilised by the authors and aligned to the research paradigms employed by the authors. While the well-established EQUATOR SRQR standards were used as primary guidance in the reporting throughout, the recent intervention of Braun and Clarke around values-based reporting in qualitative research is acknowledged. 39 In line with some of the key concerns therein, the authors have endeavoured to avoid framing the worth or trustworthiness of the research in terms of typically positivist or postpositivist evaluative criteria such as data saturation or participant validation.
Aim
To understand the perceptions of front-line staff about their experiences with senior ambulance leadership in the English NHS.
Question
What are the experiences of frontline ambulance staff in relation to senior leadership in the English NHS?
Research paradigm
The authors utilised an interpretivist and constructivist approach to data analysis, allowing the researchers to gain deeper insights into participants’ perceptions about their experiences. Interpretative work takes reality to be subjective, and that individuals’ interpretations of phenomena are shaped through the lens of experience.40,41 Constructivism, meanwhile, is grounded in the position that humans coordinatively construct knowledge in line with their negotiated experiences of, and reflections upon, local realities. 42 In combination, these perspectives underscore that qualitative researchers are themselves embedded in the social world and are subject to the same matters of positionality as the participants in their research; this is an issue that the adopted EDQ methodology will aim to reflect. 43
Sampling
A purposive sampling strategy was utilised which is commonplace in EDQ research, where finding samples exposed to the phenomenon being explored is imperative to obtaining rich data.
43
Participants were recruited via online social media adverts which identified key information, and a link to a JISC consent collection instrument, which contained full participant information. The sample size was dictated by pragmatic issues such as the recruitment window set and resource and funding limitations. Participants (N = 10) were recruited from frontline ambulance service staff who met the study's inclusion criteria:
Ambulance staff working in clinical roles in the English NHS. NHS Band 7 or below.
44
3 + months of active clinical experience.
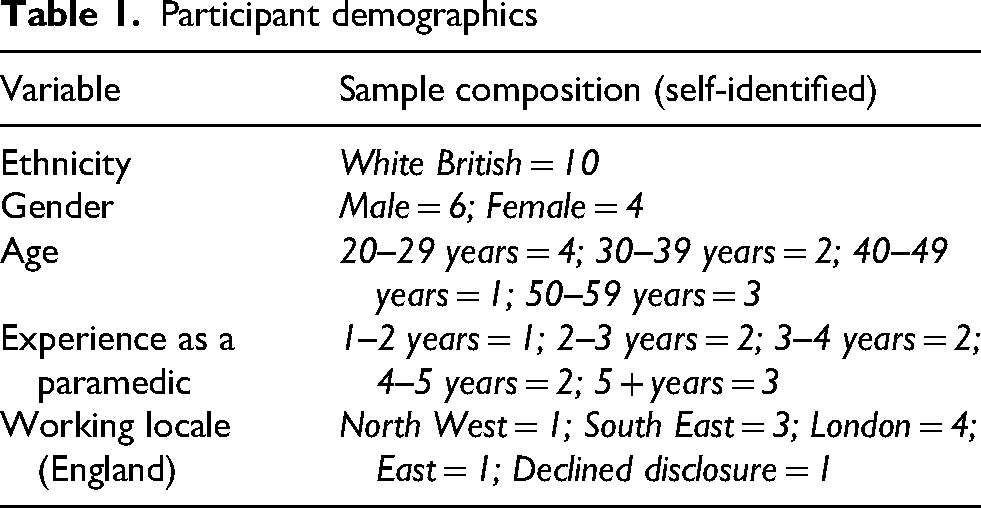
It was further stipulated that participants should not presently have significant leadership responsibilities of their own, nor currently be subject to disciplinary procedures, or have submitted a grievance against senior leaders. The demographic composition of the final sample is shown in Table 1. It should be noted that conditions of ethical approval negate these demographics being reported with any greater connectivity pertaining to individual participants, given the prospective sensitivity of the salient topic.
Participant demographics
Data collection
Semi-structured interviews were chosen as the data collection method for rich and detailed data to be collected about participants’ perceptions and experiences and manifestly designed to allow for flexibility and pursuit of any topical novelties that may arise. 43 An adaptable interview guide, available as a supplemental file, was developed by the first author (an experienced paramedic and academic) and the third (a veteran social psychologist and qualitative healthcare researcher). The first author conducted all interviews, ensuring consistency of application and strength of in situ capacity to understand and develop upon participants’ positions and experience. Interviews were conducted and recorded using Microsoft Teams. Collected data was transcribed verbatim, using the recordings, by a trusted agent, signed up to the full ethical conditions of the project. Data was collected between January 2023 and May 2023.
Data analysis
Reflexive Thematic Analysis was chosen as the core analytic approach, given its native integration with the paradigmatic concerns outlined above. 43 The authors followed the recommended six-step process, the inductive character of which is well suited to exploratory studies wherein sensitivity to unexpected analytic directions and outcomes is key. The first author conducted the initial coding and theme development, with their approach to coding identifying both semantic and latent codes within the literature, considering the participants interpretation of the question in their response and the researcher's interpretation of that response. 43 The third author then discussed this interpretation with the first, periodically verifying it with reference to the original transcripts, until a mutually agreeable thematic structure was reached. Finally, the second author (an experienced paramedic and researcher) reviewed the internal consistency of the emergent analysis and proposed key modifications that were integrated into the final presentation of findings.
Reflexivity
With extensive experience and knowledge of the sector, both in England and Australasia, the researchers were able to use reflexivity to bring key insights into ambulance leadership. A reflexive and opened minded stance was essential in recognising and mitigating potential biases stemming from their own professional backgrounds. Reflexivity, a well-established principle in qualitative research, was instrumental in enhancing the credibility and contextual relevance of the findings. By remaining critically aware of their positionality, the researchers were able to engage more deeply with the nuances of leadership as experienced by ambulance personnel. This reflexive engagement not only enriched the data analysis but also ensured that the emerging themes were grounded in authentic operational contexts.
Ethics
Ethical approval for this study was obtained via the research ethics committee at the lead author's institution (ref: 22/13). Informed consent was provided electronically by all participants in advance of interviews taking place, and the first author additionally reviewed the inclusion criteria, summarised the participant information sheet and verbally confirmed consent at the start of each interview. At the end of the interview, participants were reminded of how to withdraw their consent post-hoc should they wish to do so and were sent an electronic debrief sheet containing information and support.
Findings
Analysis of data yielded three major themes:
Function and dysfunction in a top-down professional culture Everyday ethics in hierarchical structures Influence by leaders and influence on leadership
These are schematised with relation to the major subthemes from which they are assembled in Figure 1 and described with respect to direct data.
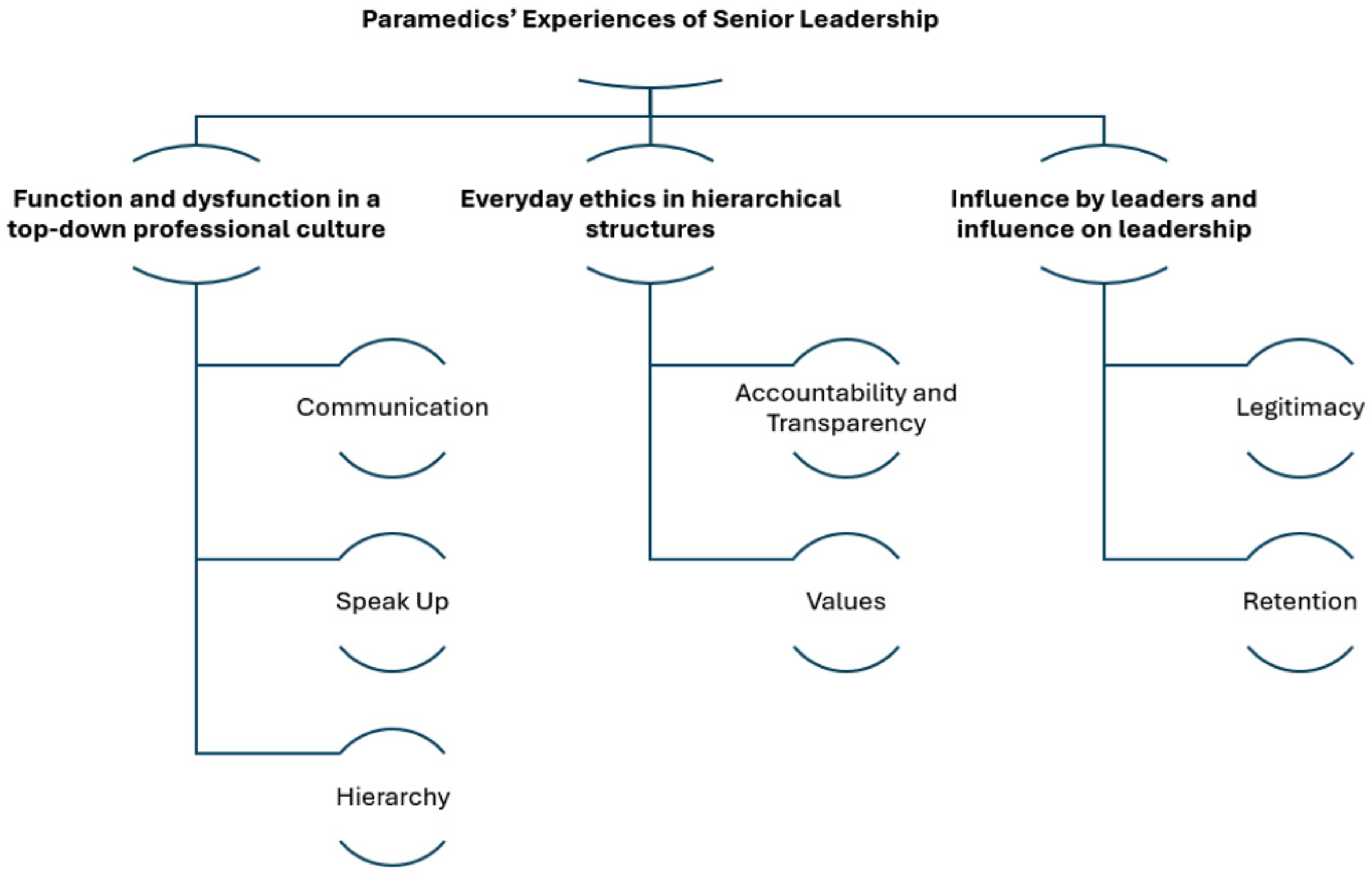
Schematic of relationships between themes and major subthemes.
Function and dysfunction in a top-down professional culture
Data suggested senior leaders who communicate effectively are more able to lead their teams and earn their staff's respect. The study's participants recurrently emphasised the root of ‘effectiveness’ was embedded largely in the capacity of a senior leader to show they had listened to and understood their staff, thereby facilitating the building of genuine connections. Where this was the case, it was reported to have helped establish a clear and morale-boosting vision, which aided staff in better understanding their roles, with benefits for the workplace environment and patient care. ‘I think we engage better with those more visionary leaders…who set out where they think the ambulance service should be going…so we can buy into that and feel part of that journey and we can see a role for ourselves in this future’. (T2) ‘I think the influence is where you feel a connection with that leadership or leadership team that you’re naturally going to be feel more passionate about the role. If you’re more passionate about the role, you’re probably going to deliver a better service to your patients…You’re going to start giving ideas’. (T2) ‘If I’m completely honest, it's an organisation that I won’t stay with. I have difficulty explaining it because I feel like as if senior management aren’t tackling things or they’re trying to, but there's no communication…you have an element of there's too much ambiguity within just day-to-day working…ambiguity within healthcare, it equates to risk’. (T3) ‘It often feels you have to jump up the management levels to get a response. So, I’m acutely aware that you’re adding to people's burdens, their inbox, when they shouldn’t have to be dealing with that but you’ve had to go to that level because nothing else is working’. (T2) ‘[I] raised this…they were “you need to come in, we need to have a chat with you about you being more positive”. This sort of thing had been threatened before…’ (T1) ‘Yeah. I mean some real good people that have just been worn down, come into roles so enthused…And they’ve challenged, for the right reasons for staff and or patient care and just been worn down by it. But of course, it's a system, especially if senior leaders are playing the system and the politics, because you’ll never break that system. You’ve got to find other ways of dealing with it. And when I’ve mentored, I just say to people “Just play the long game. You are going to be here a lot longer as a registrant than most of these senior leaders”.’ (T4) ‘I’ve noticed that with the younger staff, with social media, it's information overload. And because a lot of them are thinkers now, they’re trying to reconcile so much information, so many messages, that it leaves them in conflict of which direction to go’. (T4) ‘I feel sorry for the guys that are coming straight out and never had a job before and they just think that's the norm. So, they probably accept it’. (T3) ‘It's change. I mean they go through them like you wouldn’t believe. I can’t remember how many CEO's and senior people have been through in the seven years I’ve been here…they seem to come and do a little bit and then they go’. (T6) ‘I don’t think I’ve ever actually seen them. I don’t think I could tell you who they are…’ (T7) ‘And with quite a few of the more senior managers, it's a case of “my door is always open” why are you in my office again? They talk a great game about these things but the reality when you start pointing things out…tends to be an awful lot different. To the point where you even get what could be seen as idle threats…’ (T1) ‘In our ambulance service, we have team-based working, so each of us are assigned a team leader…And we specifically work under that manager. So, any sort of issues we have with regards to disciplinary, appraisals, supervisions anything like that is all with that specific manager’. (T7)
Everyday ethics in hierarchical structures
Connecting to the issue of communication, participants made it clear they valued senior leaders who had been open and honest with them and who had taken active accountability for their actions. Even where a leader had made a decision with which a participant disagreed, or that decision transpired to be simply wrong, that leader maintained respect if they were transparent about the decision process itself and held themselves accountable for the outcomes. Conversely, inferred dishonesty or avoidance of culpability was viewed as hugely damaging to all aspects of the workplace and relationships therein. ‘If we can understand the pressures they’re under and the constraints they have to work in, it will set expectations better’. (T2) ‘But I think it's understanding and honesty. I think there's just too many mixed messages and there's too many changed messages. They just need to be honest, stick to a line and deliver on that product’. (T4) ‘Within the Trust they do have a…platform where each week they do discuss issues…I think they try to be fairly transparent and fairly open and honest, pragmatic and realistic about why something's been put in place or what it does. So, I think generally when they try to explain stuff or discuss stuff, it is quite good’. (T5) ‘[T]hey need to stamp out the bullying and the favouritism and just make it an equal playing field for everybody’. (T6) ‘It seems to be the certain few that get the development opportunities rather than it be a transparent and open process available for everyone’. (T8) ‘I think there was some parts of [previous Trust's name] where there was a reputation of some areas being sort of boys’ clubs and jobs going to their mates’. (T9) ‘I guess just a bit of empathy, “We understand what you’re going through and we’re working on it”. And again, it's that open communication…I would rather somebody come down to me and say “What can we do to change it?” Rather than “Well this is what we’re doing…”’ (T10) ‘I found everyone in the meeting was a Band 8 and above. It was quite intimidating as someone who was a Band 6, and you go into a meeting and on screen there's four Band 8 managers there. And they did say the whole “If you need anything let us know” [but] there was no follow up to it and I felt a little bit disheartened…But a simple follow up and simple contact would have been really beneficial in that circumstance and made it a lot more positive when my whole work life was just changing’. (T8) ‘They were really diplomatic. My manager wasn’t on shift but they chose the manager that was closest to me on shift to break that bad news. The [senior leader role] was there as well and he was really supportive. I’d never met him before that point, but they were really good there, like he even gave me a hug and things like that. So, it wasn’t like, “Oh, I’m a manager. I’m just here for formalities”. He was really, really involved. And I had a really good follow up with them’. (T7)
Influence by leaders and influence on leadership
Influence emerged as a complex concept within the findings. Some participants could recognise that Senior Leaders often were influenced by boards or key performance indicators. Furthermore, influence could go two ways, that is, the paramedic voice itself could be influential in terms of self-determination, and it was not always a top-down approach.
A key concern among all participants was the practical influence of senior leaders who had no direct experience in the domain of emergency medicine and had a limited capacity to fully comprehend the working lives of those for whom they were making crucial decisions. These typically ‘top tranche’ leaders were widely perceived to not understand the paramedicine culture and were concerned only with spreadsheets and targets. ‘The very senior leaders, they’re not clinical and quite often they give the impression that all they’re worried about are the figures…the problem with the senior managers is that they just don’t get us…Particularly those who come from outside, other parts of the NHS and they don’t realise that our job is so different…’ (T1) ‘There's people that are in management positions that shouldn’t be management positions. There's elements of they’re not being trained correctly. The [senior leader role named] has told me that [Trusts’ name] frontline management have not had training in ten years’. (T3) ‘So, in fairness, for all my bad points about senior leaders, I’m not convinced they are given the tools or the foundation to do the job’. (T4) ‘I think the other massive thing in the background is this demand piece and we are so wedded to our targets. So, when I talk about this actually it's not a criticism of our senior leaders. I genuinely believe that they’re trying to do the right things for services, colleagues and patients. But our politicians, our stakeholders, the NHS is so wedded to these targets because it's easy to measure, isn’t it?…It's really difficult to measure quality but this gives us a measure…But actually has that enabled us to change our culture and change our operating model, and become this visionary leading ambulance service?…It drives those behaviours. It plays into that command and control nature because now we have to control everything so tightly, we need to understand right at the top that these changes are the most important things to focus on’. (T2) ‘I think the other thing is that our service has had a bad CQC report for a number of years. We’ve had Ofsted where we’ve lost our accreditations to apprentice training. There were some behaviour stuff obviously, but a lot of that was around leadership and engagement. So, the regulatory impact has also helped us’. (T2) ‘[T]he ambulance voice is, my perception is, it is quite weak. It's not like other sectors that have a really strong voice, and I know we’re actually a really small player in the NHS’. (T2) ‘I think we’ve come on a very long journey very quickly as an ambulance paramedic. profession, let's say from the late 40 s, fifties onwards…Whereas nursing and medicine is hundreds or thousands of years old. And I think we’ve got a real opportunity to cut out a lot of that time, as long as we have better structures. And it's the senior leaders that have got an opportunity to make sure we’ve got the right structure for our staff’. (T4) ‘[Y]ou’re making other people's job more difficult in which case they’re just going to leave…I’ve got at least ten good mates who’ve left the ambulance service to work in primary care…and every single one of them says “You just get treated so much better”.’ (T1) ‘[I]t's hard to watch and I think we’re definitely losing staff because of that feeling that the management are just not involved with us’. (T10) ‘I think that has negatively impacted me because now I’m thinking “well, I’ve got to get out of here before they try to push me out the door in some kind of way”.’ (T3)
Discussion
The study aimed centrally to explore the experiences of frontline ambulance staff and their interactions with senior leaders. The qualitative analysis revealed three major themes, relating to culture, ethics and influence. Key issues arising from these are discussed with reference to their relationship with literature in paramedicine and the broader allied health domains.
Within the broader theme of function and dysfunction in a top-down professional culture, communication emerged as a key and often problematic, aspect of contemporary leadership for participants. Failings in communication, and the negative impacts of these upon patients, staff and wider organisations, have been a prominent feature of many reports exploring leadership within the NHS in recent years.6,18–21 The findings above broadly confirm similar results to those emergent of recent staff surveys.9,25 The latter similarly suggest that ineffective and/or ambiguous top-down communication practices are still a persistent feature of England's ambulance Trusts, and that a lack of ‘connection’ between senior leaders and on-the-ground staff was often present. The findings did, however, highlight how some senior leaders had shared their vision with staff, and transparently communicated how feedback had reshaped, with positive impacts on performance and morale. The value of this order of inclusion within the NHS has been strongly emphasised in key literature,7,9,45 as has the cost of its absence, not least in fomenting dysfunctional and even toxic workplace cultures. 10 Walsh and Sarandy 45 were commissioned by the Kings Fund to explore collaborative leadership within the NHS, recognising the value this approach to leadership could have in and across complex healthcare systems. This is a behaviour led approach which focusses on bringing diverse groups of people inside organisations together. The report identifies the need to create safe and inclusive forums for transparent conversations and shared decision making. Creating open environments such as this manages power dynamics and conflict, challenges how people think, leading to more effective outcomes for organisations and the people within them. Such an approach may address the cultural and communicative issues being reported by participants.
With respect to the latter, participants reported experiences of having ‘spoken up’ about problems within the ambulance service, with variable consequences. While some positive experiences emerged, it was also described how, due to a variety of structural and interpersonal obstacles to ground-up communication, issues often had to be ‘needlessly’ escalated to receive any form of response.9,24 Perhaps a greater matter of concern was a reported reluctance to speak-up at all, which for some had become a mundane feature of their workplaces – a need to ‘play long the game’ – with attritional consequences for their sense of psychological safety within the workplace. This order of dysfunctional coping mechanism is well-noted to be a routine outcome of unhealthy leadership, and senior leaders who are more focused upon ‘comfort-seeking’ than ‘problem solving’, in healthcare contexts in England and elsewhere.9,10,24,29,46 If senior leaders were to create safe spaces where concerns could be addressed openly and collaboratively, then more positive outcomes could be achieved. 45
An important underpinning theme in the study was the regularly voiced confusion about organisational structures themselves, the lack of which was typically seen to hinder access to senior leaders (and their messages) rather than facilitate it. This was in part attributed to a high-turnover of senior-level leaders in ambulance services, itself connected to a perception that these leaders were often ‘politicians’ for whom the role was functionally a stepping-stone for their broader ambitions. The emergent sense of ennui in the analysed findings regarding the order of support participants could therefore expect to receive ‘from the top’, itself then connected to staff attrition issues, speaks plainly to ongoing staff well-being concerns documented in a raft of pertinent literature.7,9,17 However, the findings of the present study did not indicate a unilaterally bleak landscape. The findings reported some senior staff implemented a team-based working approach, which offered local leaders increased autonomy and a more supportive operational model through which to lead staff. This model was recommended in the cultural review of UK Ambulance Trusts, 17 and the findings above underscore its prospective facility.
Experiences were routinely reported where senior leaders had not appeared open and honest with staff about key decisions, with serious consequences noted for workplace trust and confidence. Conversely, cases were also documented where senior leaders had openly and transparently consulted with staff, even where the decisions subsequently made did not inherently align with the preferences of the participants themselves, the openness of the process itself was lauded and the decisions viewed as ‘reasonable’. These observations connect those above regarding leadership communication with a sense of ‘everyday ethics’ in healthcare 47 ; that is, those actions which are ultimately viewed by stakeholders as ‘fair’ and/or ‘decent’. Above, transparency in decision-making was widely seen as ethical in this sense, irrespective of outcome; even when the ultimate outcome was personally (or more broadly) favourable, which can improve staff experiences at work.9,10,45
It has been well-established that senior leaders providing staff an opportunity to influence strategy and understand decision-making rationale is typically valued by those affected, and often leads to higher levels of staff satisfaction, which by extension can result in improved patient satisfaction and clinical outcomes.9,10 In this respect, the embedded and hierarchical ‘command and control’ culture in the English ambulance service arguably accentuates a lack of transparency encountered by many working paramedics. 17 A consistent matter in the findings above related to a particular lack of clarity around career development and opportunities within participants’ services, with some referencing ‘cliques’ and ‘boys clubs’. This is an issue reflected in a recent report which documented how English ambulance staff had experienced a lack of fairness and/or transparency regarding career progression, and that this was particularly true for those from a minority background, 48 and confirms allied findings in broader research literature.49,50
In terms of more direct ethicality, experiences reported in this study highlight some senior leaders had been actively accommodating and supportive. Incidences where senior leaders had demonstrated a lack of compassion and empathy were, however, more commonly described, with serious implications for individual confidence and, where more widely apparent, collective morale. The absence of demonstrable integrity and fairness from senior leadership is well-recognised to be a major factor in mental health and well-being challenges among paramedics in England and elsewhere.17,23 Indeed, it has been identified that such occupational stressors are more likely to have serious impacts upon mental health and well-being in emergency services, where situational stress is inherently higher, than in many other professions. 51
Authentic leadership theory has attracted much research within the healthcare context, alongside transformational leadership. Authentic leadership is a values driven and ethical style of leadership where leaders demonstrate openness, transparency and integrity with their approach, often showing vulnerability while doing so. Transformational leadership is about creating a compelling vision, inspiring others and encouraging professional growth aligned to organisational objectives. In combination, these leadership approaches are associated with higher levels of staff morale and productivity, as well as enhanced patient outcomes. 7 Senior leaders within the ambulance services could respond to concerns being raised by participants and the associated literature by adopting these leadership theories within their own practice in the future.
In alignment with the previously described concern regarding the high turnover of senior leaders, and their allied ‘political’ ambitions, a lack of direct clinical experience within their senior leadership was addressed in the findings, complicating the leader's manner of direct influence. A key outcome of this was an understanding that not only were many senior leaders concerned exclusively with measuring performance through abstract data, but that a lack of front-line experience rendered them largely unable to address performance in any more sympathetic way. This perception of senior leadership viewing the complex working lives of ambulance staff entirely in terms of descriptive statistics was reported to further concretise a sense of being broadly disconnected from hierarchy, and to stimulate a ‘them versus us’ mindset. A similarly reductive approach to professional healthcare performance, prioritising nominal/response targets over real-world pragmatic activity, has been well-evidenced to impact negatively upon healthcare workers’ well-being and, indeed, performance in a range of contexts.52,53 The English cultural review of ambulance services also mirrors the participants’ overshadowing focus on how operational performance measures can work to the detriment of people and culture. 17
In terms of explanation, the findings did not universally address these issues in ad-hominem terms regarding ambulance senior leaders. Rather, it was recognised that senior leaders may not have received the support and training they may have needed to undertake their roles effectively, a matter further underscored in the cultural review. 17
Findings further indicated a key perceived interaction between the character of senior leaders and its direct influence on the retention of staff. This links to the issues noted above regarding workplace culture and communication, though it was (once again) clear that issues of transparency and everyday ethics prevailed in the assessments made by the study's participants. Predominantly, accounts of colleagues leaving the ambulance service were framed in terms of terms of ‘greener grass’ where leaders were more focused upon worker-oriented values, found within more authentic leadership styles. 7 Key internal reasons given for such departures were largely reported to be inflexible senior leaders denying workplace alterations, and colleagues even being told to find alternative employment when asking for such adjustments. These observations both mirror and develop upon the nuance of some of the key concerns regarding staff retention detailed in existing literature.17,22–24 Key workforce data indicates attrition is improving in the UK ambulance service, although one in ten paramedics left their job in the 2021/2022 period, 54 with attrition maintaining at 10% in 2023. 55
Limitations
While sample size and generalisability are not typically key concerns within qualitative work, 56 recruitment via social media may have attracted participants with particularly strong views regarding leadership, possibly limiting diversity of perspectives across the broader ambulance workforce. Moreover, while a strong age range and relatively even gender divide was represented in the sample, all identified as white British people. Given the concerns noted above regarding how dysfunctional leadership can disproportionately disadvantage staff from minority groups, this is a clear limitation and a matter that mandates further research.
The timing of data collection during post-COVID-19 organisational recovery may also have heightened participants’ sensitivity to leadership challenges and impacted upon their accounts of recent experiences. Moreover, the study's focus on English NHS ambulance services inherently limits transferability to other healthcare systems, though findings have been demonstrated to resonate with international evidence, and attention is drawn to international concerns wherever possible.
Conclusion
This study explored how frontline ambulance staff in the English NHS perceive senior leadership, revealing three interlinked themes, culture, ethics and influence, that shape their experiences. Central to these findings was the importance of authentic communication and genuine connection. Staff consistently valued leaders who demonstrated transparency, empathy and accountability, even when decisions were difficult. In contrast, poor communication, lack of visibility and perceived dishonesty contributed to psychologically unsafe environments and defensive coping behaviours, undermining trust and morale.
Ethical considerations were especially prominent in participants’ evaluations of leadership, with transparency and fairness seen as critical to organisational integrity. Reports of favouritism and exclusionary practices were deeply damaging to staff morale. Additionally, the theme of influence highlighted tensions between external pressures and internal realities, with a disconnect between leadership and frontline operations exacerbated by high turnover and the relatively weaker voice of paramedicine within the NHS. Despite these challenges, examples of effective leadership, particularly those rooted in team-based models and open communication, offer promising pathways forward. Ultimately, the study underscores the urgent need for leadership development focused on communication, inclusive decision-making and deeper engagement with frontline contexts to improve staff well-being, patient care and retention. Collaborative, authentic and transformational leadership approaches are also identified within the literature as being crucial to responding to some of the challenges experienced by participants. These approaches must be integrated into workforce training, policies and service design to meaningfully shape and enhance how organisational change impacts frontline staff's perceptions and experiences of senior leadership, a key mechanism to improve patient outcomes.
Participants intermittently spoke about first-line and middle managers alongside senior leaders during their interviews. Perhaps reflective of the lack of clarity around organisational structures and the reported disconnect they have with senior leaders. Consideration does however need to be given to the role first line and middle managers have upon the experiences being reported within this study. Are they merely reflecting behaviours role modelled to them by senior leaders or having to implement strategies with which they may not agree? Or are they in some way part of the problem, reducing senior leader visibility and failing to implement effective leadership approaches. Or is there something else at play? Further research is needed to explore this phenomenon.
Supplemental Material
sj-docx-1-pam-10.1177_27536386251412465 - Supplemental material for The LEAD (leadership experiences and direction) study: Exploring top-down cultures, everyday ethics and mutual influence in UK paramedics’ experiences of senior leadership
Supplemental material, sj-docx-1-pam-10.1177_27536386251412465 for The LEAD (leadership experiences and direction) study: Exploring top-down cultures, everyday ethics and mutual influence in UK paramedics’ experiences of senior leadership by Richard Ward, Scott Devenish and Paul K. Miller in Paramedicine
Supplemental Material
sj-docx-2-pam-10.1177_27536386251412465 - Supplemental material for The LEAD (leadership experiences and direction) study: Exploring top-down cultures, everyday ethics and mutual influence in UK paramedics’ experiences of senior leadership
Supplemental material, sj-docx-2-pam-10.1177_27536386251412465 for The LEAD (leadership experiences and direction) study: Exploring top-down cultures, everyday ethics and mutual influence in UK paramedics’ experiences of senior leadership by Richard Ward, Scott Devenish and Paul K. Miller in Paramedicine
Footnotes
Ethical approval and informed consent statements
Ethical approval for this study was obtained via the University of Cumbria Research Ethics Panel (ref: 22/13). Informed consent for interviews to be recorded and analysed, and extracts to be published in redacted form to protect identities, was provided electronically by all participants in advance of interviews taking place. Participants further confirmed consent at the start of each recorded interview.
Author contribution(s)
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received internal research funding from the University of Cumbria's Internal Research Fund (IRF) to pay for transcription services.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The second author (SD) is an Associate Editor at the present journal. The third author (PKM) is the current Chair of the Research Ethics Panel at the University of Cumbria, the body responsible for ethical oversight of this project, but was not in this role at the time the project was ethically approved.
Data availability statement
Conditions of ethical approval, given the prospective sensitivity of the matters discussed by participants, preclude the public archiving of full transcripts, redacted or otherwise.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.