
Abstract
Background:
current organization of the prehospital emergency teams, decreasing the prehospital times, given the possibility of working during the patient’s transport and, therefore, the consequences that may result from the same improving the prognostic.
Objectives:
To explore the opinion of professional healthcare experts regarding prehospital emergencies arising when forced to assist a critical patient in a moving vehicle, based on a high-fidelity clinical simulation, as well as the factors influencing them.
Methods:
An exploratory study of content analysis with qualitative methodology, via semi-structured questionnaires that are self-completed anonymously, before and after the clinical simulation intervention in which participants intubate a mannequin in a moving ambulance. The sample consisted of 36 experts in prehospital emergencies from the province of Alicante (Spain). Codification and assessment of the data obtained was carried out via triangulation, respecting the language and literal expressions of the participants.
Results:
Thirty-two pre- and post-intervention questionnaires were completed. Four different units of meaning or categories emerged which were organized based on two thematic structures, from the perspective of professional and patient needs. Twenty-three participants had never previously intubated in a moving vehicle.
Discussion:
Working in a moving vehicle may be yet another aspect to consider in the specialized teaching–learning process of prehospital emergency medicine.
Conclusion:
Based on the need to decrease prehospital assistance times, a new paradigm has been opened in prehospital emergencies with the possibility of being able to safely assist our patients during their transport on a moving ambulance or helicopter. It will be necessary further research in the future.
Introduction
Prehospital emergency medicine involves the acute phase of any pathology. Numerous studies have focused on the possibility of prehospital emergencies (PE) teams performing certain therapeutic procedures during the patient’s transfer to a hospital center,1–3 maintaining both their clinical safety and the professional’s safety. So, in prior studies, we have analyzed whether or not it was feasible to intubate a critical patient in a moving ambulance and any potentially adverse events. From this we have observed that there are no significant differences in terms of time of intubation, or regarding risks while stationary or in movement. 4
This results in innovation in the current organization of the PE teams, decreasing the prehospital times, 5 given the possibility of working during the patient’s transport and, therefore, the consequences that may result from the same 6 improving the prognostic.
The aim of this study is to explore the opinions of healthcare PE professionals regarding the assistance of critical patients, in our case, when intubating in a moving ambulance, based on a high-fidelity (hi-fi) clinical simulation as well as to determine the factors that may influence the same.
Methods
Setting
The study was conducted in the Department of Health Sciences at the University of Alicante (Spain) where participants responded to a questionnaire before and after undergoing an intervention with a hi-fi clinical simulation, in the care compartment of a moving ambulance. Participants were to intubate a mannequin having a physiological response, initially programmed with different clinical cases, using distinct intubation devices.
Study design
An explorative content analysis study as the qualitative methodology. The sample includes 36 physicians from the prehospital Emergency Medical Service (EMS) in the province of Alicante (Spain), from a total of 93 physicians making up the service, and participating in the study on a voluntary basis. Inclusion criteria were that physicians were to have over 6 months of work experience in the area of PE, as well as prior academic training in the therapeutic procedure to be performed during the intervention, in this case, an orotracheal intubation (OIT).
Data collection
After signing the informed consent form, and in order to ensure maximum participation and heterogeneity of experts, all participants responded prior and post to the intervention semi-structured questionnaire, based on their own experience, with open questions. Given that there were no prior similar studies, the research team agreed on the key questions to cover the relevant fields with regards to assistance in a moving vehicle, as an initial approach: prior experience, prior training, opinions, suggestions for the future.
Analysis
The research team was consisted of clinical experts in PE, experts in the creation of hi-fi clinical simulation scenarios and experts in qualitative research in the health sciences. Thus, data triangulation was enhanced, comparing data from the distinct perspectives involved in the study.
The responses obtained were transcribed from the questionnaires defining the segments. All members of the research team were involved in the analysis of each segment, using analysis files and alpha-numerically coding each of the appraisals expressed in them. Therefore, coding and assessment design was carried out from the obtained data using triangulation between the team of researchers, in order to create the general units of meaning or categories, as well as relevant units of meaning or sub-categories, ordered by topic. The study was approved by the Ethics Committee of the Vice Chancellor of Research, Development and Innovation of the University of Alicante.
Results
Of the 36 questionnaires that were sent, 32 were completed (88.88%) before and after the intervention. Of these, 19 (59.37%) were completed by men and 13 (40.63%) by women, having a mean age of 44 years (SD 8.05) and mean prior experience in the area of PE of 8 years (SD 5.15). Participants came from distinct medical specialties, with all of them coinciding in having post-graduate training in PE.
Of these, nine had previously intubated in a moving vehicle in their daily routine, declaring that “when it is an easily accessed airway, no problem, and on the other hand, I have used supraglottic devices that are easy to handle and maneuver.”
In general, positive opinions expressed in the questionnaire given prior to the intervention were “I think that it should be performed when, due to circumstances, the vehicle cannot be stopped and the patient requires it”; “I think that we should care for the patient’s safety in all senses, before getting him in the ambulance and/or helicopter but, since we cannot predict everything, sometimes, we must open the airway while moving.”
Negative opinions expressed by the participants, prior to the intervention included, “it should only be performed in exceptional cases. It is almost always possible to perform the maneuver while not moving”; “I don’t consider it to be recommendable. It would always be preferable to look for a place to stop, halting the OIT for a few minutes and performing it calmly.”
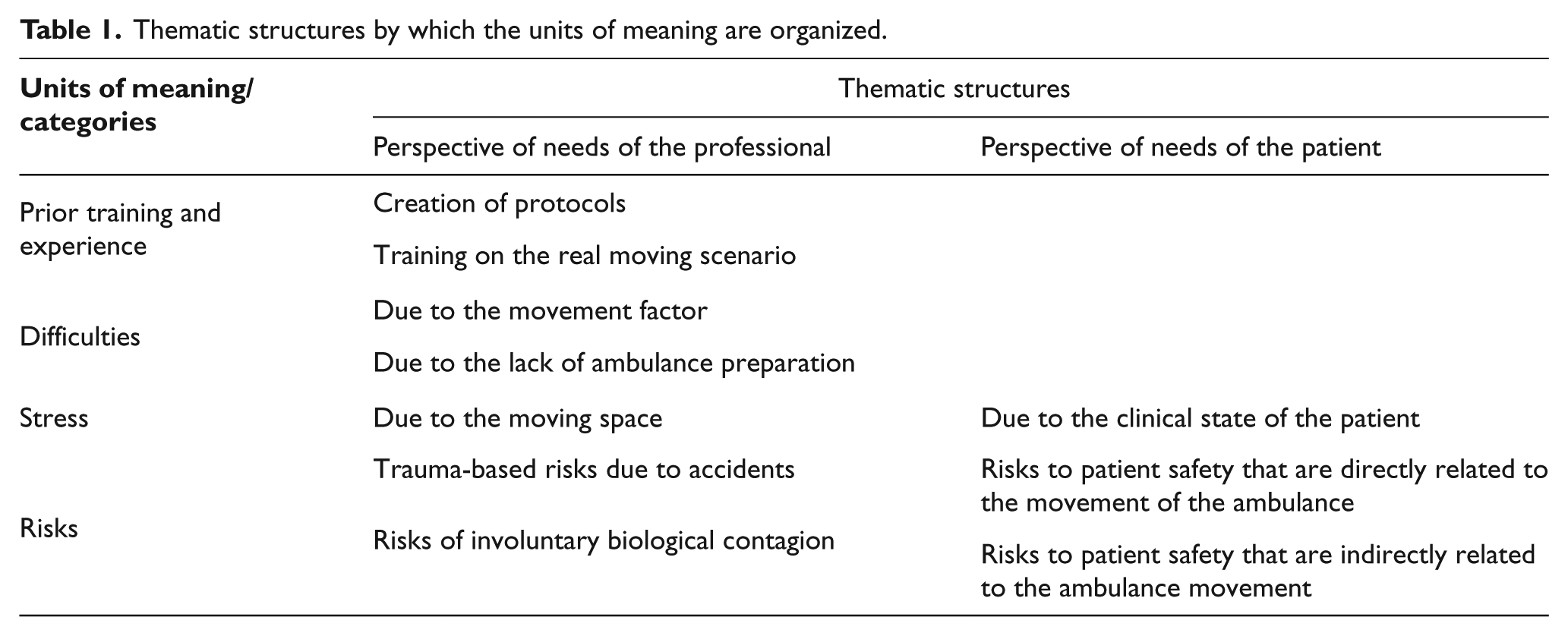
As for the analysis of the factors that influence their opinions, four different meaning units or categories emerge (Figure 1) which have been organized in two topic-based structures: from the perspective of the professional needs and of patient needs (Table 1).
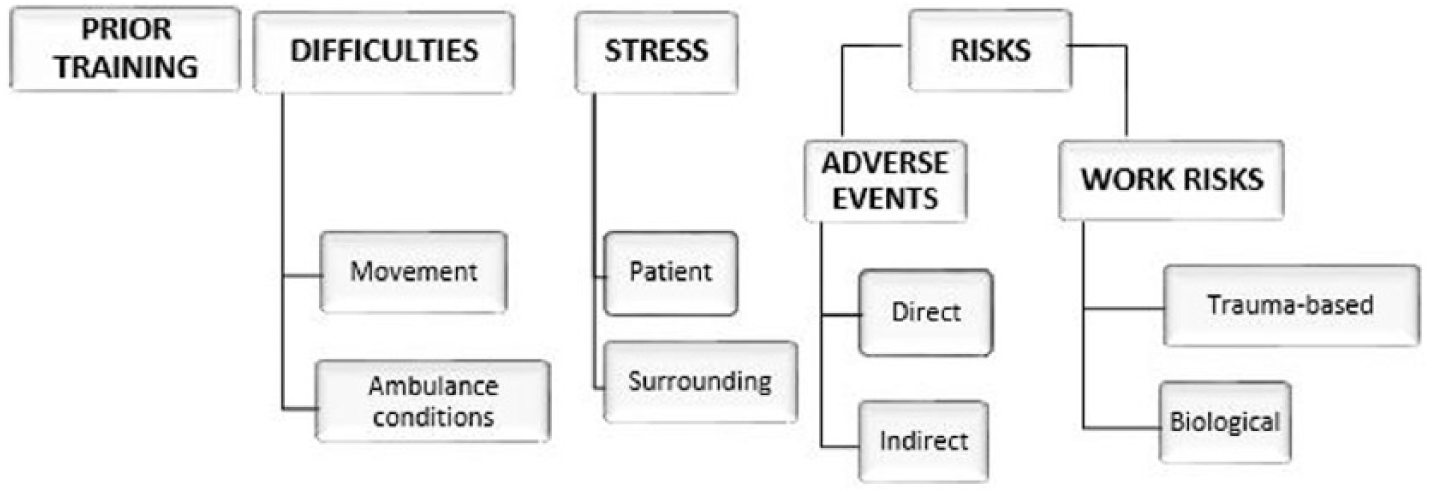
Map of meanings.
Thematic structures by which the units of meaning are organized.
Prior training and experience
Opinions were expressed regarding the use of the technique while moving, and the need to create specific new protocols and practical training for the same. “It is important to have procedures and trainings so that, when necessary, there is the necessary skill and experience.”
Difficulties
The relevant units of meaning, with regard to the perceived difficulty, are the added difficulty to the technique due to the movement factor and the difficulty derived from the lack of preparation of the ambulance.
Prior to the intervention, opinions were offered, both positive and negative, regarding the difficulty of performing OIT while moving. “I think that it must be more difficult to perform while moving”; “harsh movements of the vehicle are always a great inconvenience, especially turns. It isn’t more complicated than performing it while stationary if the vehicle travels at an appropriate velocity and avoids sharp turns.” After the intervention, the perceived difficulty changed for some participants. Expressions such as “I thought it would be more difficult; after completing the simulation I see that it isn’t as difficult as I imagined it would be, as long as it doesn’t move too fast”; “actually, I didn’t even notice the movement.” Others, however, maintained that the movement added increased difficulty to the technique. “Harsh movements of the ambulance while visualizing the airway”; “verification of the endotracheal tube due to external noise, which prevents proper auscultation.”
As for the difficulty resulting from the lack of preparation of the ambulance, opinions such as the following were expressed: “difficulty in preparing and displaying the materials necessary to intubate, added problems to a technique that even under ideal conditions may be complicated and difficult, it is more difficult to visualize the airway structures.” Others, on the contrary, declare that they do not find any differences in terms of perceived difficulty, “because there are devices that greatly facilitate the maneuver.”
In the post questionnaire, five individuals expressed their change of opinion with expressions such as “I thought I would have more difficulty, after completing the simulation I don’t see as many problems as I did prior to completing it”; “difficulty due to the reduced space for performing the techniques.” Ten participants commented on the added difficulty due to the “lack of stability for performing the technique”; “the falling of materials during the turns and speed bumps, unexpected braking.”
Stress
Stress is a factor mentioned by our participants, with regard to the emotions that, generated by the clinical state of the patient or by the circumstances surrounding 7 the completion of the work in a moving ambulance, make the technique more complicated. In our analysis, two sources of stress were detected: stress caused by the patient’s clinical state: “Stressful, since if I decide to do it during the transport it is because the patient’s state is poor, to require making that decision” and stress due to the moving space: “I have not done it, it would have caused a lot of stress.” Following the intervention, the participants did not describe an actual or perceived sensation of stress during the procedure.
Risks
According to our participants, in the adverse events that were directly related with the technique undertaken while in movement, they expressed opinions that were both positive as well as negative: “I believe that it is less safe than “without movement,” therefore we should choose to perform the safest choice; I believe that the movement may increase the number of intubations in the esophagus and oral pharyngo-laryngotracheal lesions; with sufficient experience, the negative effects of the maneuver while moving are minimized; there are devices to perform it without risks.”
As for the indirect risks of OIT while on route, opinions such as the following were offered: “It may extend the time of the maneuver”; “it may increase the number of attempts”; “increase of the time of apnea”; “optimize the transport time, increase the time of the OIT and therefore, of the apnea”; “speed of transport, increase in number of erroneous intubations.”
With regard to the potential risks, from the professionals’ perspective, relevant units of meaning emerged regarding the potential trauma-based risks caused by accidents within the ambulance chamber, as well as biological risks caused by involuntary contagion. Expressions such as, “it is more complex and favors accidents in healthcare workers”; after the experience, participants described having experienced instability during the maneuver within the ambulance.
As for the biological risk of involuntary contagion, opinions such as the following were offered: “risk of contamination with patient fluids, risk of accidents.”
Discussion
In our study, the patient safety is the most relevant topic for our participants. The occurrence of adverse events, when the procedure is carried out while in movement. They thought the probable risks solely to movement, risks that are directly linked by scientific literature to OIT performed in hospital contexts, such as regurgitation of gastric content with risk of bronchoaspiration, 8 hypoxemia, 9 bradycardia, hypotension 10 and, finally, cardiorespiratory arrest. The scientific production in regard to patient safety in PE is limited. According to Tejedor Fernández et al., 11 it is necessary to increase our studies in our context, not only in distinct scenarios but also studying the effects on the patient when applying our care during the transport.
As with our participants, Atack and Maher 12 suggested that the prehospital emergency physicians are not specifically prepared to work within this context since they do not receive training and education according to the specific circumstances of their work. Thus, working in a moving vehicle may be yet another aspect to consider in the specialized teaching–learning process of prehospital emergency medicine.
As for the stress mentioned by some of the participants prior to the experience, according to Valentin et al., 13 learning and regular practice with hi-fi simulation may reduce this stress as a response to specific situations and the development of the clinical practice may be improved with the use of this powerful tool.
Finally, regarding the difficulty of therapeutic treatment in a moving vehicle, and the risks of working under these conditions that were explained by our participants, as in the study by Fournier et al., 14 they express that the care chamber of the vehicle should in the future include the integration of methods of secure anchoring for the professionals and the patient, to make this a safe space for both. We declare that there are no conflicts of interest, that there have been no financing sources from private or public agencies or foundations.
Conclusion
Based on the need to decrease prehospital assistance times, a new paradigm has been opened in PE with the possibility of being able to safely assist our patients during their transport on a moving ambulance or helicopter. This is an original study with preliminary results because of small sample size so it will be necessary further research in the future to analyze with a qualitative method influencers factors and its consequences for having the decision to assist on movement.
Footnotes
Acknowledgements
To all the voluntary participants of the Emergency Medical Service from Alicante (Spain) whose opinions were needs to explore for this initial study. Thanks to the technicians of the Department of Nursing and the Faculty of Health Sciences of the University of Alicante without whose collaboration there would be no possible this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
All the questionnaires submitted are available.
Informed consent
All the participants accepted voluntary participate and signed an informed consent before.
Ethical approval
This project was approved by the Ethical Committee of the Research and Knowledge Transferring Vice dean of the University of Alicante on 19 June 2013. We have the Spanish document at your disposal.
Human rights
We declare that we have covered all the human rights during our study as the participants anonymity.