
Abstract
The paramedic role is physically demanding, yet limited attention has been given to how paramedicine students are physically prepared for practice within tertiary education programmes. The extent to which physical fitness standards and training are embedded in curricula, professional registration requirements or pre-employment testing remains unclear. This review explored how paramedicine students are physically prepared within tertiary education and whether student fitness levels meet the demands of the paramedic role in Australia, New Zealand, South Africa, the United Kingdom (UK), Ireland and Canada. A scoping review was conducted and reported following guidelines from the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR). Electronic databases (Medline, CINAHL, Scopus, ERIC, Emcare and Informit) and grey literature sources (university handbooks, policy documents and online domains) were searched, with searches completed in June 2025. Curriculum documentation from 51 universities, two organisation or college documents and nine relevant studies were analysed. Four universities (one in Australia and three in South Africa) in the six countries (Australia, New Zealand, United Kingdom, Ireland, Canada and South Africa) included in the review clearly embedded physical fitness training in their curricula. Most Australian institutions addressed fitness only as a requirement of work-integrated learning (WIL), typically mandated by placement providers. Internationally, South African programmes integrated sequenced physical preparation within curricula, while UK and Irish programmes applied entry screening prior to enrolment with manual handling training integrated within curricula. One study found that student fitness levels were comparable to the general population, but there is inconsistent data whether they meet all of the essential job demands of the paramedic role. There is limited and inconsistent integration of physical fitness information and preparation in paramedicine education. Embedding structured physical readiness frameworks into curricula may improve student support and preparedness for WIL. Future research should investigate validated physical fitness standards and strategies to ensure student readiness for the physical demands of the paramedic role.
Keywords
Introduction
The paramedic role is widely recognised as physically demanding, involving tasks such as lifting and carrying patients across varied terrains,1–4 as well as performing cardiopulmonary resuscitation (CPR). 3 In addition to physical demands, paramedics experience significant psychological stress resulting from long working hours, staffing shortages, critical decision-making responsibilities and repeated exposure to traumatic incidents.5,6 These factors contribute to a high incidence of injury,7–10 as well as high prevalence of elevated stress, depression, cardiovascular disease11,12 and obesity.13–15 The economic burden of work-related injuries in Australia exceeds AUD$60 billion annually, 16 with musculoskeletal injuries – particularly from manual handling – being a common concern among paramedics due to the physically intensive nature of their work. 17 Since the 1950s, it has been known that physical inactivity leads to poor health, risk factors like cardiovascular disease and a variety of chronic diseases such as diabetes mellitus.18–20 In other health professions, poorer clinician health has been associated with adverse care outcomes. By extension, maintaining physical health is likely important for a paramedic's ability, as a healthcare professional, to perform their duties safely and effectively.21,22 It is therefore critical that paramedics and paramedicine students be suitably physically prepared for the role. The current review was conducted to inform developments in this area in Australia, though the findings will have relevance for a range of other countries.
Research has increasingly described the physical demands of paramedic work3,23–27 and the importance of physical fitness, including components such as cardiorespiratory endurance, muscular strength, muscular endurance, flexibility and body composition,28,29 for paramedics to safely and effectively perform their duties30–32 and maintain their health. Despite this professional expectation around fitness to practice, 33 there is limited guidance on whether and how tertiary education programmes could support the physical readiness of paramedicine students. This is further complicated by the limited evidence available around validated and specific pre-employment physical fitness requirements and testing.
The primary pathway to becoming a paramedic in Australia is through the completion of an accredited 2- to 4-year bachelor degree programme, 34 similar to other countries such as the United Kingdom (UK), New Zealand (NZ), Ireland and South Africa (SA). However, during these lengthy periods of study, students may experience a decline in their physical activity and mental well-being,35,36 which could result in inadequate preparation for the physical aspects of paramedic work, particularly during work-integrated learning (WIL) placements or post-graduation. When completing WIL or upon employment, there is an expectation that patient care be delivered effectively and safely, in challenging situations that involve assessing, treating, lifting and moving patients, often with limited resources, 33 but it is unclear how tertiary education centres support paramedicine students for this.
Further adding to the complexity, the role of a paramedic is not standardised internationally, or even across Australian states and territories, with significant variation in role titles, scopes of practice and required competencies.
In response to these knowledge gaps, this scoping review aims to answer the following research questions:
To what extent and through what approaches are paramedicine students physically prepared before and within their tertiary education for the role of a graduate paramedic, in Australia, NZ, the UK, Ireland, Canada and SA? To what extent do paramedicine students’ physical activity and fitness levels in Australia, NZ, the UK, Ireland, Canada and SA meet physical demands and fitness requirements of the paramedic role, represented by ‘pass’ levels of job-specific physical fitness tests and the physiological demands of paramedic tasks?
Methods
This scoping review was conducted in accordance with the Joanna Briggs Institute (JBI) methodology for scoping reviews 37 and was registered with the Open Science Framework on 30 January 2024 (https://doi.org/10.17605/OSF.IO/6GQBV). Following the searches, the scope was narrowed from that outlined in the original protocol due to the unexpectedly large volume of relevant literature. Specifically, the review focused on student paramedics and state or territory services, while evidence pertaining to qualified paramedics will be reported separately. In addition, the contexts of NZ and Ireland were added to the review scope due to their similarities in systems to Australia and the UK. Search strategies were revised accordingly to ensure comprehensive coverage of the refined topic.
Inclusion criteria
Consistent with the framework of populations, concepts and contexts (PCC) 38 employed in developing the search strategy for the review, the following inclusion criteria were used.
Populations: The definition and role description of a paramedic appear to vary broadly, within ambulance services internationally, and the literature shows a lack of consensus. 39 This scoping review uses the term ‘paramedic’ to include various related roles such as ‘ambulance officer’, ‘first responder’ and ‘emergency medical technician (EMT)’. This review included studies and other eligible documents (see below) that considered student paramedics or individuals described by other terms or labels for this role (provided the documents met other eligibility criteria). Terms included combined the concept of ‘student’ with ‘paramedic’, ‘EMT’, ‘emt’, ‘Emergency Medical Technician’ or ‘paramedicine’.
Concepts: The scoping review employed the definitions for the concept terms physical activity, exercise, physical fitness and physical health listed in Appendix 1. It is important to clarify the definitions to be used, as these terms are often confused or used interchangeably. 40 Studies and other eligible documents (see below) that considered these concepts in relation to the populations mentioned above were included in the review provided they met other eligibility criteria.
Contexts: The contexts of interest in this review included several geographical locations in which ambulance systems and student education in paramedicine are considered broadly comparable, particularly in their Anglo-influenced structures and clinical governance models. These are Australia, NZ, Canada, the UK, Ireland and SA. Otherwise-eligible documents focused on these contexts were included in the review. These countries share common features such as English-based legal and health systems, university-level paramedic education, professional registration requirements and models of ambulance service delivery that combine emergency response, clinical assessment and patient transport.
Types of sources: Where they met other eligibility criteria, the review included studies that employed qualitative or quantitative research designs, including secondary research conducted in a systematic manner. Authoritative documents describing university curricula and related content and activities, ambulance service fitness and testing requirements and standards, and fitness requirements and standards of governing organisations responsible for the registration or accreditation of paramedics, as well as policies, position statements and procedures relating to any of these, were included as key additional sources of evidence for the review.
Exclusion criteria
The following were excluded: opinion pieces, study protocols, non-systematic secondary research (such as narrative literature reviews) and research reports lacking sufficient methodological detail to confirm their status as primary or robust secondary research. Studies conducted outside the six focus countries were also excluded, as was any curriculum content not part of an undergraduate paramedicine or paramedic science bachelor's degree. Research focused on special operations roles or industrial and private-sector paramedic roles was similarly excluded. The databases were searched without any date restrictions; the grey literature manual searches were limited from 2020 to 2025.
Search strategy
A diverse list of relevant databases and search platforms was accessed and searched to identify eligible peer-reviewed studies and grey literature relevant to the review aims. The electronic databases searched include MEDLINE (via Ovid), Emcare (via Ovid), Informit Health Collection, Scopus, ERIC (via EBSCOhost) and CINAHL (via EBSCOhost). Additional searches were conducted using Google and Google Scholar, including advanced manual searches of grey literature. Reference lists of included studies and citation tracking via Scopus were used to identify additional sources. Relevant professional standards, policies and curricula were sourced directly from university programmes and ambulance services, with additional contact made to Australasian universities to seek such documents through the Australasian Council of Paramedicine Deans (ACPD).
An initial exploratory search was conducted to identify a range of relevant documents. Titles and abstracts were screened to extract keywords consistent with the PCC framework guiding this review. These keywords and equivalent thesaurus terms were then used to develop a comprehensive search strategy (Appendix 2), optimising both sensitivity and specificity through Boolean operators (AND, OR, NOT) and relevant controlled vocabulary (e.g., MeSH terms). This iterative development of the search, screening and selection strategies ensured alignment with the research questions and literature mapping 38 (Table 1). The search strategy was peer-reviewed by a librarian with expertise in conducting systematic literature searches, using the PRESS (Peer Review of Electronic Search Strategies) checklist, 41 to ensure the search strategy was comprehensive and risk of bias in the search was minimised.
PCC framework showing search terms and concepts for the scoping review.

Advanced manual grey literature searches were conducted via Google using domain-specific limits (e.g., *.edu.au and *.gov.au) as outlined in Appendix 2. These manual searches targeted education and curriculum documentation from 2020 to 2025 in all six countries and involved screening the first five pages of search results. The searches were completed in June 2025.
Screening and selection of studies and other sources of evidence
Following the searches, citations of all identified documents from databases were collated and uploaded to Covidence (Veritas Health Innovation, Melbourne, Australia – available at www.covidence.org), and duplicates were removed. Records sourced via manual advanced Google searches of curriculum and organisation documentation via direct sourcing via ACPD were added. A pilot test of the planned screening and selection process was conducted. Titles and abstracts were screened by three independent reviewers (S.S., L.R. and H.S.) against the eligibility criteria. To ensure a consistent approach to screening, three meetings were conducted: one to commence the pilot test to clarify the process, one on conclusion of the pilot to inform the screening and selection process and a final meeting during the selection process to address any issues or questions.
Clearly, ineligible documents were excluded in the screening process and the remaining, potentially relevant sources were retrieved in full and imported to Covidence for further assessment of eligibility. The full text of each of these documents was assessed in detail against the eligibility criteria by three independent reviewers (S.S., S.F. and H.S.). Differences between these reviewers in eligibility decisions were resolved through discussion and consensus via three online meetings. The results of the search, screening and selection processes were recorded in a flow diagram, showing counts at each stage and reasons for exclusion, following guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for Scoping Reviews (PRISMA-ScR).37,42 Reasons for exclusion of documents reviewed in full text were recorded as part of this process. Further manual searching for curriculum and organisation documentation was conducted by the first author and checked by a second reviewer (L.R.).
Data extraction
Data were extracted by two independent reviewers (S.S. and L.R.) using an adapted data extraction tool in Covidence (Veritas Health Innovation, Melbourne, Australia – available at www.covidence.org) (Appendix 3) and a curriculum mapping framework (Table 2). The data extracted from documents included, where relevant, specific details about the authors, publication year, participants, concepts, contexts, study methods and key findings relevant to the review questions, including findings regarding the following:
-physical preparation approaches for paramedic students; -physiological demands of paramedic tasks and/or the role; and -existing physical activity and fitness levels of paramedic students.
Mapping of physical fitness preparation and testing within undergraduate paramedicine bachelor degrees as a part of work-integrated learning (WIL) (2020–2025).
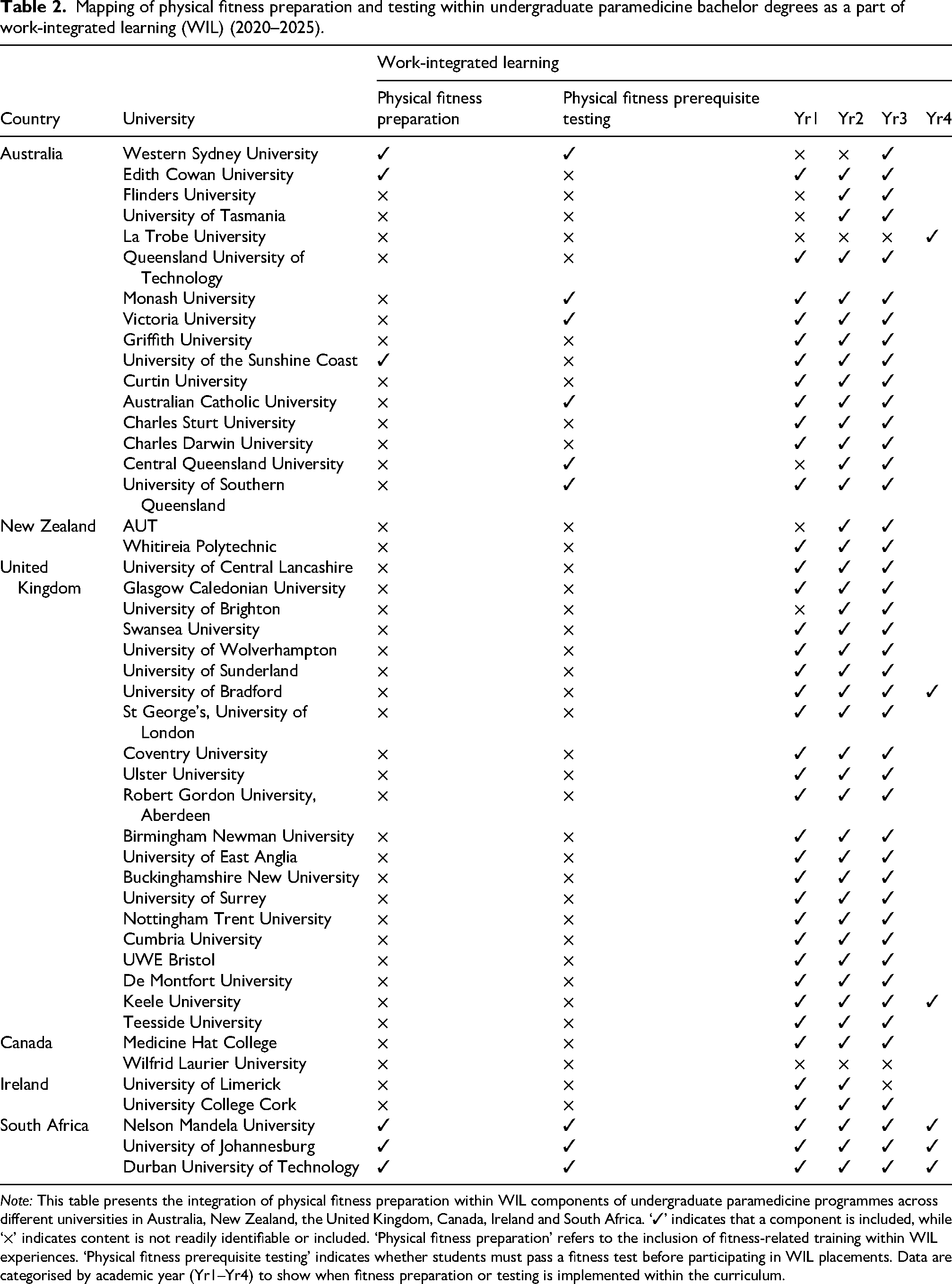
Note: This table presents the integration of physical fitness preparation within WIL components of undergraduate paramedicine programmes across different universities in Australia, New Zealand, the United Kingdom, Canada, Ireland and South Africa. ‘✓’ indicates that a component is included, while ‘×’ indicates content is not readily identifiable or included. ‘Physical fitness preparation’ refers to the inclusion of fitness-related training within WIL experiences. ‘Physical fitness prerequisite testing’ indicates whether students must pass a fitness test before participating in WIL placements. Data are categorised by academic year (Yr1–Yr4) to show when fitness preparation or testing is implemented within the curriculum.
Any disagreements between the reviewers were resolved through discussion and consensus.
Curriculum documentation data were extracted to map the minimum length of the degree and whether physical fitness content was easily identified as embedded within module(s) and sequenced throughout the course. In addition, information regarding each course was examined to identify whether the respective course included any physical fitness preparation and testing as a part of WIL.
Data synthesis
The research questions that were the focus of the scoping review were answered descriptively, with relevant evidence from the included documents categorised and mapped by topic area: physical preparation approaches for paramedic students, physiological demands of paramedic tasks and/or the role and existing physical activity and fitness levels of paramedic students.
A deductive basic qualitative analysis approach was undertaken to describe and summarise evidence in each pre-existing category, guided by JBI scoping review recommendations. 43 A three-step approach was used, as described by Elo and Kyngas, 44 preparation, organisation and reporting,43,44 using the pre-existing categories based on the research questions. Once the researchers were familiarised with the data, the data were then organised based on the categories and summarised. Reporting of the analysis for this scoping review was conducted as per the PRISMA-ScR checklist and explanations. 37
Ethics
As all data were drawn from previously conducted research and other existing documents that did not include sensitive or personal data regarding individuals, this scoping review was exempt from any requirements for ethics approval.
Results
The systematic literature searches retrieved a total of 1785 records. After the removal of 325 duplicates and the addition of 286 records identified through manual searches, a total of 1746 records were screened by title and abstract or title and description. Of these, 288 records met the initial eligibility criteria and were retrieved for full-text review. Following full-text assessment, 226 records were excluded, resulting in 62 records included for data extraction (Figure 1).
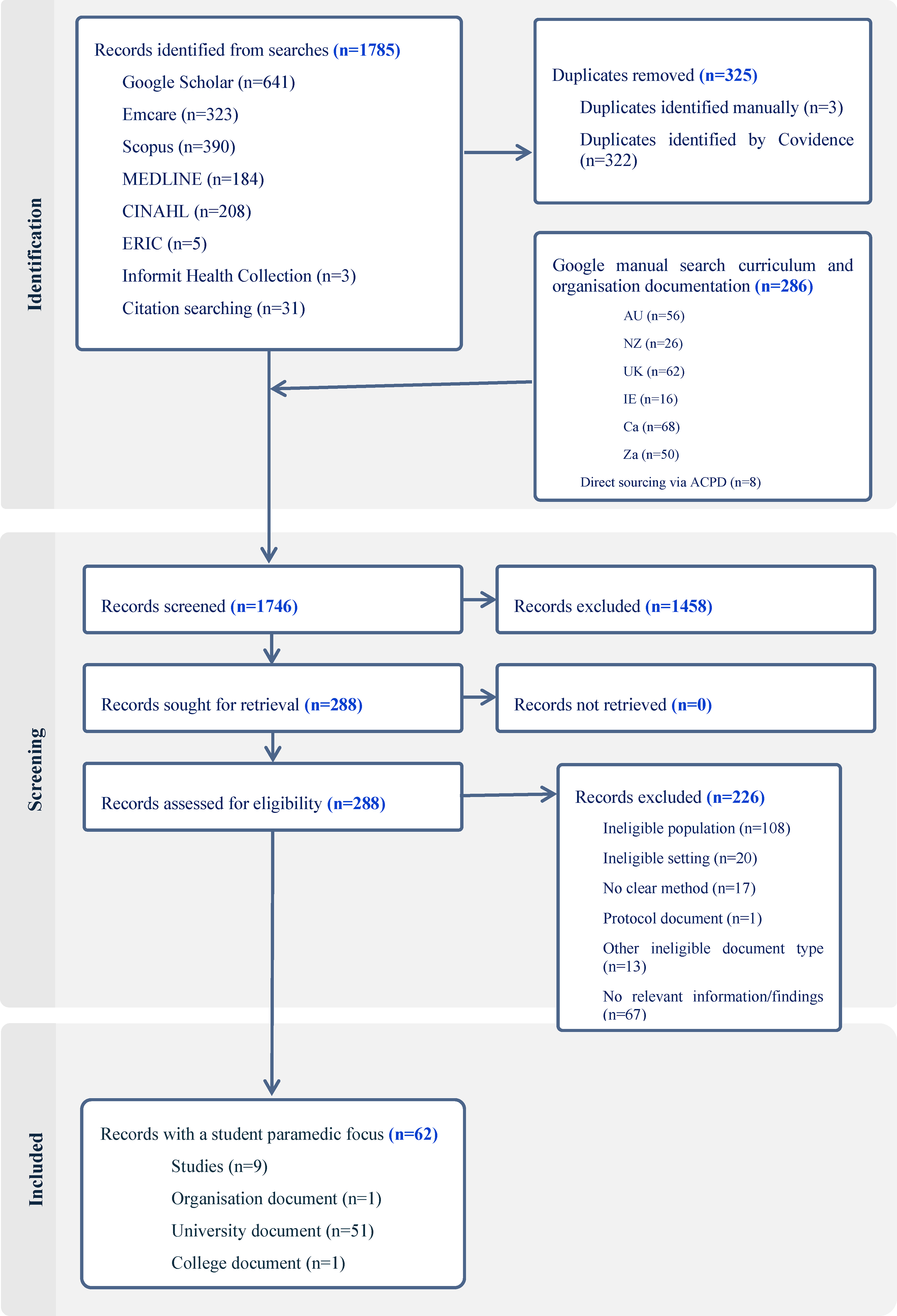
PRISMA flow diagram, based on the Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for scoping reviews (PRISMA-ScR). 37
Record characteristics
Data from all 62 records were extracted. Data from studies and some documents with a student paramedic focus were extracted as per the extraction template (Appendix 3). Detailed data from published articles and information directly received via ACPD are presented in Appendixes 4 and 5. Data from 51 university documents identified through grey literature sources were extracted and mapped as shown in Table 2.
Eight of the records with a student paramedic focus were peer-reviewed quantitative studies12,35,45–50 and one a mixed-methods study, 51 with years of publication ranging from 2012 to 2024. Areas of interest and concepts within the evidence are reviewed here with a student focus. The 51 university documents were reviewed with a focus on information they provided regarding the preparation of paramedicine students and the physical fitness requirements of the paramedic role within the curriculum and as a part of WIL. These documents included published student handbooks, WIL documents and subject documents where available via advanced manual Google searching or provided directly by universities and organisations following contact through the ACPD.
Curriculum mapping
Information regarding the extent to which and through what approaches paramedicine students are physically prepared and tested before and during their tertiary education for the role of graduate paramedic was sourced from curriculum documentation provided directly by six universities and organisations in Australia and NZ (with data extracted in Appendixes 4 and 5). Additional information of this type, reported in Table 2, was derived from documentation from 16 tertiary education organisations in Australia offering an undergraduate paramedicine degree and two in NZ, through the online grey literature searches of paramedicine course descriptions, handbooks and related curriculum documentation. Further international evidence was obtained from institutions offering undergraduate paramedicine degree courses in the UK (n = 21), Canada (n = 2), Ireland (n = 2) and SA (n = 3), through the advanced manual searches outlined in Appendix 2.
At most Australian and NZ institutions, physical fitness preparation is neither embedded nor consistently addressed within undergraduate paramedicine curricula. Physical fitness education and preparation is not clearly or consistently integrated or sequenced throughout the coursework of most paramedicine programmes. Table 2 outlines whether physical fitness requirements or assessments were integrated as part of WIL. Where physical fitness testing was required, it was typically mandated by the placement organisation rather than the university. For example, in the state of Victoria, Australia, fitness testing was a prerequisite for WIL placements with Ambulance Victoria. In isolated cases, preparation activities were evident but not embedded within the curriculum itself; instead, they were delivered by external providers. One university in Australia, for example, engaged the Australian Paramedical College (APC) to support fitness preparation.
In the UK, Ireland and SA, interviews are conducted as part of assessing student eligibility, followed by standard occupational health screening. These screens include health declarations and immunisation checks in courses across the UK and Ireland. Universities in SA (n = 3) were the only universities identified where physical fitness preparation is embedded and sequenced within each year of the bachelor's degree programmes.
In Canada, paramedicine remains predominantly a vocational or diploma-level qualification, although a transition towards degree-level education is underway. Two Canadian undergraduate paramedicine degrees were identified; however, enrolment in both is restricted to currently practising paramedics, and thus, physical preparation for entry-level students could not be assessed in this context.
Physical preparation approaches for paramedic students
University documents
Fifty-two university documents were reviewed, comprising online course descriptions and handbooks for undergraduate paramedicine degrees across Australia, NZ, SA, Canada, Ireland and the UK. Of these, only four universities – one in Australia and three in SA – clearly documented physical fitness preparation within their course materials. The three SA universities were the only institutions to demonstrate sequenced physical fitness preparation across the full duration of the degree programme.
In Australia, physical fitness requirements were referenced in the context of WIL, with three universities referencing general fitness preparation and six universities referencing physical fitness testing. However, in all cases, these requirements were mandated by the placement organisation – typically state ambulance services – rather than the university itself. For instance, both Ambulance Victoria and the Queensland Ambulance Service require students to complete a fitness assessment prior to WIL placements. Three universities in Australia provided course-specific or supplemental documents detailing these expectations. One university in New South Wales (NSW) provided the Readiness for Work-Integrated Learning (R-WIL) and Paramedicine Physical Capacity Assessment guide, which specified the procedures and criteria used to ensure students are physically prepared for clinical placements.52,53 Another in Western Australia (WA) provided a general resource outlining fitness expectations across multiple Australian ambulance services, with a focus on student well-being and pre-employment readiness. 54 One university in South Australia and the Northern Territories (SA/NT) included a dedicated course unit (PARA1007) that summarised physical fitness tests and task simulations across Australian ambulance services, while emphasising manual handling safety and injury prevention. 55
In the UK and Ireland, a more standardised approach was observed. Entry into paramedicine programmes typically requires applicants to undergo an interview and occupational health screening, including reviews of medical history and immunisation status. However, no evidence was found of formalised or ongoing physical fitness preparation embedded within the curriculum.
In contrast, SA undergraduate paramedicine degrees incorporate comprehensive physical fitness training, including search and rescue components, across all years of study. This structure suggested that the entry-level paramedic role in SA may encompass more specialised operational tasks than equivalent roles in Australia or the UK.
In Canada, paramedicine education remains largely vocational or diploma based, though a transition to degree-level programmes is underway. Two Canadian undergraduate degrees were identified, both of which are currently limited to practising paramedics, preventing assessment of student fitness preparation at the entry level.
College documents
One college document from Canada 56 provided guidance and recommendations for physical health and fitness preparation for undergraduate paramedicine students, based on existing testing requirements within ambulance organisations. The document serves as a comprehensive resource for paramedic students, covering fitness assessment, exercise programme development and stress management. It included a detailed description of the physical employment test (PET) adapted from the City of Greater Sudbury Paramedic Services, Canada. The PET simulates common physical demands of the paramedic role, including strength, agility, anaerobic capacity and flexibility. The second college document, from the APC, 57 a private training provider, details fitness requirements for each state or territory ambulance organisation across Australia. One university in Australia outsourced physical fitness education to the APC.
Studies
Four of the included studies explored physical fitness preparation approaches and standards among paramedic students or candidates.45–47,51 Armstrong et al. 45 evaluated the impact of a 4-week strength and conditioning programme on performance in the Ontario Paramedic Physical Abilities Test (OPPAT™) using a pre/post design. Participants demonstrated improved mean completion times, decreasing from 905 to 816 s following the intervention. However, the study did not include a control group or account for potential learning effects, so it cannot be concluded that the improvement was solely attributable to the intervention itself. In a related study, Malone et al. 47 examined predictors of OPPAT™ success and identified significant associations with gender, employment status and body mass. Female students from public colleges were more likely to pass the test than those from private colleges (OR = 2.41), while employed participants also had higher odds of success (OR = 1.87). Each 1-kg increase in body mass was associated with a 5% increase in the probability of passing (OR = 1.05).
Gayton and Lovell 46 investigated the relationship between resilience, general health and well-being among 219 participants, including 146 qualified paramedics and 73 students in Queensland. They found significant associations between resilience and both general health (r = −0.259, p < 0.002) and well-being (r = 0.369, p < 0.001). Additionally, age and professional experience were positively correlated with resilience.
The doctoral thesis by Muhlbauer 51 focused on task-oriented physical preparedness among emergency medical care (EMC) students in the 4-year Bachelor of Health Sciences in Emergency Medical Care (BHSc EMC) programme in SA. Although the EMC role differs from that of paramedics in Australia due to its rescue-focused components, the thesis demonstrated that EMC students must maintain adequate physical fitness to safely complete programme requirements, including physically demanding tasks such as CPR, patient lifting and high-risk rescues. In response to the absence of validated fitness assessments in EMC education, Muhlbauer 51 developed and piloted an occupation-specific preparedness assessment at three SA universities. The assessment included a 5-km timed run (aerobic capacity), a 200-m swim (total-body endurance), a flexed-arm hang (upper-body endurance), a sit-and-reach test (flexibility) and push-up and abdominal strength tests (muscular endurance). Results indicated a wide variation in student fitness profiles and highlighted sex-based performance disparities. The thesis recommended that EMC programmes adopt validated fitness assessments, integrate structured physical training and support students with lower baseline fitness levels to mitigate injury risk and improve clinical readiness.
Existing physical activity and fitness levels of paramedic students
Five studies specifically assessed physical activity and fitness levels among paramedicine students.12,35,48–50 Micalos et al. 35 compared physical activity (measured via the International Physical Activity Questionnaire, IPAQ) across paramedicine, nursing and double-degree students. Paramedicine students reported significantly higher physical activity than did nursing students (p = 0.009) and double-degree students (p = 0.044). Activity levels also varied by year of study, with third-year students being more active than first years (p = 0.007). No significant differences were observed based on gender or living arrangements. 35 Similarly, a study conducted by Le Rossignol et al. 48 investigated the health-related physical activity of first-year students at an Australian metropolitan university campus and found that male students reported significantly higher physical activity levels than their female peers, while age, living arrangements, commute mode and hours of paid work had no significant associations with physical activity levels. The authors concluded that universities, especially those training future health professionals, have a responsibility to foster environments that support lifelong physical activity – a key component of their future roles as health behaviour role models.
Thornton and Sayers 12 reported that paramedic candidates generally demonstrated fitness levels comparable to general population averages based on a pre-employment screening protocol. While the study did not assess how these fitness levels relate to paramedic job performance or injury risk, the average level of fitness may be insufficient for some operational demands in paramedicine, which can require sustained work above the anaerobic threshold during emergency tasks.
Gutwirth et al. 49 conducted a pilot study examining the relationship between physical exertion and CPR performance among paramedic students. The study aimed to assess how fatigue influenced compression rate and depth, two critical components of high-quality resuscitation. The pilot study suggests that fatigue developed early in the resuscitation effort, with increases to heart rate and perceived exertion scores. Given fatigue may adversely affect CPR quality, the authors advocated for the integration of physical conditioning into paramedic education to mitigate the effects of fatigue during prolonged resuscitation efforts. 49 MacQuarrie et al. 50 also conducted a pilot study to investigate the effect of acute physical exertion on paramedic students’ clinical performance under high-stress conditions. In terms of CPR performance, there were no significant differences in compression depth or chest recoil, or in clinical performance scores, between the occupational physical activity (OPA) condition and the rest (REST) condition. 50
Discussion
This scoping review explored the current landscape of physical fitness preparation for paramedicine students in Australia, NZ, the UK, Ireland, Canada and SA. The findings have been presented in relation to the two research questions and situated within the broader academic and professional literature.
Physical preparation approaches for paramedicine students in Australia
This review found limited evidence of structured or embedded physical fitness education and preparation in Australian undergraduate paramedicine curricula. At one Australian university, a formal physical preparation subject was embedded in the curriculum. 55 Other Australian universities referenced fitness testing in relation to WIL requirements, driven externally by placement providers rather than the institutions themselves.52–54 The absence of embedded fitness preparation in Australian curricula differs from the models observed in SA, where physical training is integrated throughout the paramedicine degrees; however, these degrees include elements like search and rescue readiness. This suggests that the paramedic role at the entry level in SA may be more complex than in other countries considered and therefore similar to special operations roles in Australia. Further research into these models along with an examination of the paramedic workforce in SA, particularly regarding injury rates, physical health and patient outcomes, would be beneficial. Such studies could help establish the relationship between physical preparedness and the effectiveness of paramedic services, providing valuable insights that could inform curriculum development in Australia.
A structured and standardised approach may better align with appropriate physical capacity preparation of students to be embedded throughout paramedic education and training, 51 and not treated as the responsibility of the individual only.3,58 Previous research suggests that university students, including those in paramedicine and nursing, often experience a decline in physical activity over the course of their studies.35,36 However, whether tertiary education providers should be responsible for students’ physical preparedness is underexplored. Fitness assessments could be used formatively, offering students feedback and opportunities for improvement throughout their degree, or summatively, with predefined standards determining WIL eligibility. While beyond the scope of this review, future research could explore how tertiary education providers in collaboration with state and territory services may balance these considerations in preparing students for the physical demands of the paramedic role. Further investigation is warranted into how formal physical fitness preparation may be conducted and whether it improves paramedicine student preparation for WIL and the physically demanding nature of clinical placements.
To what extent do Australian paramedicine students’ physical activity and fitness levels meet the physical demands and requirements of the paramedic role?
Studies that have directly examined paramedicine student fitness levels reported that paramedic students were more physically active than nursing students 35 and also noted an increase in activity from first to third years, suggesting physical activity levels can vary across the years of a program. 35 Le Rossignol et al. 48 reported that nursing and paramedicine students had a lower self-reported physical activity level than physiotherapy students, for example. Thornton and Sayers 12 found that paramedicine candidates generally demonstrated average fitness levels relative to the general population, based on a pre-employment screening protocol. However, the study did not assess whether these fitness levels were adequate for the physiological demands of paramedic work, nor did it examine outcomes such as injury risk or job performance. 12 Separate research has suggested that certain operational tasks in paramedicine – such as patient handling, prolonged CPR and operating in physically demanding environments – may require exertion that exceeds the anaerobic threshold. 49 In contrast, current physical activity and fitness levels of paramedicine students did not significantly impact performance in CPR.49,50 However, the literature has identified a mismatch between the physical demands of the paramedic role and the lack of preparation students receive.49–51 As well as CPR, paramedics are required to lift and transport patients and work in challenging and unpredictable environments.1–4,51 Without adequate fitness, students may struggle to meet these expectations, increasing their risk of musculoskeletal injury, a leading cause of paramedic attrition.10,17
Variability in fitness requirements across countries and institutions
This current scoping review explored how different universities approach physical preparedness and fitness testing for paramedicine students. The comparative review of undergraduate paramedicine degrees across Australia, NZ, the UK, Canada, Ireland and SA highlights key disparities in physical fitness preparation requirements. While universities in SA embed structured fitness training within the curriculum, others around the world rely on external health screenings or fitness declarations. Australian universities exhibit a varied approach to integrating physical fitness within paramedicine programmes. While one Australian university embeds fitness-related content into the curriculum, 55 most other institutions did not. However, several Australian universities in NSW, Victoria and Queensland, require fitness testing for placement eligibility. In NZ, paramedicine programmes worked closely with Wellington Free Ambulance and Hato Hone St John, requiring students to complete health screening to ensure students are medically fit for the paramedic role.
Universities across the UK and Ireland require occupational health clearance prior to student enrolment into the programmes. Some universities in these countries mandated fitness screenings before placement, while another university conducted manual handling training for assessing lifting capabilities. Still another incorporated stress management as part of its training, but it is unclear if physical-fitness-specific information is included. Overall, universities in the UK advertise an approximate 50/50 split between WIL and in-class or simulation activity. UK students will therefore take part in a significantly higher amount of physical work associated with the paramedic role than students in Australia.
Synthesis and implications
This review found no consistent or standardised approach to preparing paramedicine students physically for the demands of the profession. The level of fitness training integration varies widely, with some entry-level paramedicine degree programmes incorporating fitness testing only for WIL and others omitting it entirely. 53 Australian paramedicine students appear to possess fitness levels like those of the general population12,35; however, the role of the paramedic is described as physically demanding.1–4 Furthermore, current pre-employment fitness tests may not accurately reflect the functional tasks required of paramedics.12,17,59–61 These discrepancies highlight the need for validated, job-specific fitness assessments and better-aligned educational strategies. Entry-level programmes may consider integrating structured physical training into their curricula and implementing standardised assessment protocols to support students’ physical readiness for WIL, followed by professional registration and potential clinical practice.
Strengths and limitations
This review contributes to the limited literature on physical preparedness in paramedicine education by mapping fitness preparation within curricula, fitness standards that apply to students and fitness expectations across several countries. It highlights critical disparities and identifies actionable gaps in curriculum design, particularly in Australia. The limited inclusion of physical readiness components in curricula raises broader questions about whether universities should play a more active role in preparing students physically.
However, some limitations must be acknowledged. First, due to the nature of grey literature searches and curriculum documentation, some university materials may have been inaccessible, incomplete or out of date. Second, the lack of standardisation in paramedic education and roles across jurisdictions makes direct comparisons challenging. Also, while some data were gathered via direct correspondence with universities, a lack of response from some may have affected the comprehensiveness of the curriculum mapping. Lastly, due to the reduced relevance of results past the five pages, a limitation was applied to the Google-domain-specific search (searches reduced to the first five pages of results).
Future research should focus on the following:
Developing and validating national physical preparation and readiness frameworks for paramedicine students. Evaluating the feasibility and outcomes of embedding fitness preparation in tertiary curricula. Investigating the equity impacts of physical testing and the efficacy of training interventions across diverse student populations.
Conclusion
This scoping review highlights the variation in how physical fitness preparation is addressed within paramedicine education and professional practice, both in Australia and internationally. While the physical demands of the paramedic role are well recognised, there remains a disconnect between the demands and the preparation provided to paramedicine students within tertiary education programmes.
In Australia, most universities do not embed physical fitness education and preparation within curricula, and fitness testing, when present, is driven by external placement organisations. This contrasts with models observed in countries like SA, where physical training is sequenced throughout paramedicine degrees. The limited research on student fitness levels suggests that paramedicine students generally have fitness levels comparable to those of the general population, which may not adequately support the physical intensity of their future roles.
The findings of this review suggest a need for the development of standardised, evidence-based physical preparation and readiness frameworks for paramedicine students. Embedding clear standards into university curricula and ensuring alignment with evidence-based job-specific PETs would support student safety, graduate and candidate readiness and patient care quality. Future research is required and should focus on whether this is the responsibility of tertiary education providers and how to support and prepare student paramedics for validated physical fitness standards and the essential daily tasks of the paramedic role.
Supplemental Material
sj-pdf-1-pam-10.1177_27536386251405917 - Supplemental material for The physical preparation of paramedicine students for the paramedic role: A scoping review
Supplemental material, sj-pdf-1-pam-10.1177_27536386251405917 for The physical preparation of paramedicine students for the paramedic role: A scoping review by Samantha Sheridan, Rodney Pope, Alexander James MacQuarrie, Renee S. MacPhee, Russell Rayner, Hannah Stack, Lorraine Rose and Steven Fischer in Paramedicine
Supplemental Material
sj-docx-1-pam-10.1177_27536386251405917 - Supplemental material for The physical preparation of paramedicine students for the paramedic role: A scoping review
Supplemental material, sj-docx-1-pam-10.1177_27536386251405917 for The physical preparation of paramedicine students for the paramedic role: A scoping review by Samantha Sheridan, Rodney Pope, Alexander James MacQuarrie, Renee S. MacPhee, Russell Rayner, Hannah Stack, Lorraine Rose and Steven Fischer in Paramedicine
Footnotes
Acknowledgements
This scoping review was conducted as part of the doctoral degree for S. Sheridan (S.S.). The authors acknowledge the support of the Australasian Council of Paramedicine Deans (ACPD) for facilitating communication with Australian and New Zealand paramedicine education providers. We also extend our sincere thanks to the universities, ambulance services and organisations that provided access to curriculum documentation, policy materials and additional insights which contributed to the completeness of this review.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This scoping review is funded as part of a doctoral research degree programme of research by Charles Sturt University. We acknowledge the financial support from Charles Sturt University through its Academic Staff Higher Degree by Research Workload Support Scheme.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The lead researcher is a doctoral candidate at Charles Sturt University, which partially funded this work and was among the institutions included in the curriculum mapping. To mitigate potential bias, the study protocol was preregistered, and selection and data extraction were conducted according to prespecified criteria. Any disagreements were resolved by consensus, and analyses followed PRISMA-ScR and JBI guidance. Charles Sturt University had no role in the study design, data collection, analysis, interpretation or the decision to submit this manuscript for publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.