
Abstract
Background
Cardiopulmonary resuscitation (CPR) and defibrillation markedly increases survival following out-of-hospital cardiac arrest (OHCA). Members of the public can perform both before the ambulance service arrives. However, bystanders use a public-access Automated External Defibrillator (AED) in around 5% of cases. Using Unmanned Aerial Vehicles (‘drones’) to deliver AEDs may overcome many of the barriers preventing public-access AED use.
The study team investigated how quickly and easily bystanders performing CPR could use drone-delivered AEDs.
Methods
The study team developed an AED-capable drone between May and November 2020 and conducted 18 OHCA simulations in July and September 2021. A single participant found a simulated patient inside a building and made a 999-call to a Welsh Ambulance Services NHS Trust call-handler. Once cardiac arrest was confirmed during the 999-call a nearby drone launched, reached hovering altitude and delivered the AED immediately outside the building. The participant retrieved the AED when instructed to do so, attached it to the patient and delivered a single shock.
The primary outcome was hands-off CPR time. Secondary outcomes included ease of AED retrieval, by using a questionnaire adapted from the System Usability Scale and exploring participant behaviours via post-simulation interviews and reviews of audio and video recordings of the simulation.
Results
Hands-off CPR time was (median) 109 s (interquartile range 87–130 s). Participants spent 19 s (16–22 s) away from the patient's side when retrieving the AED. Participants found it easy to use the AED but often sought the call-handler's reassurance that it was appropriate to retrieve it.
Conclusion
Participants found it easy to retrieve and use an AED delivered by drone in simulated OHCAs. Hands-off CPR time was potentially clinically relevant in this lone bystander simulation, but there was only a small increase in hands-off time caused by retrieval of the drone-delivered AED.
Introduction
No more than 10% of patients who sustain an out-of-hospital cardiac arrest (OHCA) generally survive to hospital discharge or to 30 days after the event.1–3 Good quality cardiopulmonary resuscitation (CPR) and prompt defibrillation using an Automated External Defibrillator (AED) substantially increase survival rates. 4
Bystander use of public-access AEDs before the arrival of the ambulance service is associated with increased survival to hospital discharge (OR 1.73) and survival with good neurological function (OR 2.12). 5 However, bystander use of an AED occurs in a small minority of OHCA cases.1,6 Improving bystander AED use to enhance survival to hospital discharge is a key aim of resuscitation strategies in many countries, including all four home nations in the United Kingdom.7–10
Many barriers to timely AED attachment relate to a bystander's ability to promptly locate, access and retrieve a public-access AED: a systematic review in 2017 reported that only 5–22% of people knew the location of their nearest AED when surveyed, 18–59% of AEDs were poorly accessible and only 3–25% of OHCAs occurred within 100 m of a public-access AED. 6
One way of overcoming this may be to deliver AEDs by Unmanned Aerial Vehicles (‘drones’). Studies have modelled optimal drone location11–13 and flights for simulated OHCAs.14–18 These studies demonstrate that a defibrillator could potentially be attached to a patient substantially sooner than with a standard Emergency Medical Services response, with the benefits being higher in rural areas.11,12,15 In 18 test flights in Sweden (October 2016), an AED-equipped drone reached the site of historical OHCAs in rural areas 16.4 min sooner than an ambulance (mean) had managed to arrive during the actual events (which occurred between 2006 and 2014). 14
A network delivering AEDs via drone for real-world OHCAs is now operational in Sweden. Between June and September 2020, drone-delivered AEDs were available for OHCAs in three regions. Once an emergency call-handler identified an OHCA, there was an alert to a drone pilot. The pilot sought permission to fly from air-traffic control and remote-piloted the drone to the scene. In 12 drone flights, a drone arrived at the scene 11 times and arrived before the ambulance seven times (median time saving 1:52 min). However, on no occasion was a drone-delivered AED actually attached to a patient. 19 There has, subsequently, been a case report of survival to hospital discharge in a patient defibrillated by a drone-delivered AED in this system. 20
The Swedish experience 19 represents a commendable effort by researchers and policy makers, but demonstrate that there is more work to be done to optimise drone-delivery of AEDs. A simulation study in Germany similarly demonstrated that much of the time between receipt of an emergency call and arrival of a drone-delivered AED was due to delays before and after the drone flight itself. 21 There are many process issues to address.
A drone-delivered AED system does not exist in the UK, nor has there been any simulation work. The aim in this study was to develop a drone-delivery system for an AED and determine whether a lone bystander performing CPR on a simulated patient could effectively retrieve and use a drone-delivered AED in the UK setting.
Methods
This was a cross-sectional study using multiple methods. Direct observation of the simulations allowed the study team to record important time intervals related to retrieval of a drone-delivered AED, and the use of surveys, brief interviews and direct observation allowed us to pragmatically explore the qualitative nature of the interactions between the bystander, the drone and AED and the call-handler.
This article is reported as per STROBE (The Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for observational studies, 22 referring to an extension for simulation studies. 23
Developing the delivery system
The study team compared two systems to deliver an AED by drone in controlled, closed-test conditions (October–November 2020).
The drone hovers over the delivery site (at a height of 7–10 m) and lowers the AED by winch. Once the AED is on the ground, the winch is retracted and the drone hovers above the AED to indicate its location. The drone lands on the ground at the delivery site, the AED detaches and the drone hovers above the AED to indicate its location.
There were five test flights for both delivery system configurations – so the drone operator developed sufficient experience – and recorded time for AED delivery. Timings started when the drone was at the delivery site and began to (a) extend its winch or (b) descend to the ground, and ended when the drone had returned to its hovering position, with the winch fully retracted again in scenario (a). The study team considered that this endpoint was when it would be safe for a bystander to retrieve the AED.
TETRA Drones Ltd (https://www.tetradrones.co.uk/) developed the drone delivery systems, and it carried a Lifepak CR2 AED Training Unit (Physio Control).
Simulations
Setting: Out-of-hospital cardiac arrest simulations took place on 10 July 2021 and 04 September 2021 at the Sussex Police Training Centre in the UK – a controlled-access site with mocked-up buildings and roads. There was a CPR manikin (Laerdal Medical) placed in a single-storey building from which one could get outside via a hallway and an external door. Immediately outside was a pavement and road.
Participants: The aim was to recruit 20 participants. Non-pregnant adults (≥18 years) who felt physically capable of performing CPR in the simulations) were eligible. For reasons of pragmatism this was a convenience sample of (non-healthcare) personnel known to local police, search and rescue operations or members of the study team. None had previous knowledge of the drone or the AED delivery system. Study participants received a Participant Information Leaflet and Consent Form via email at least 48 h in advance. Participants had an opportunity on arriving at the simulation (in a separate holding area) to read a hard copy of the Participant Information Leaflet and ask questions, before reading and signing the Consent Form.
Outcome measures: The primary outcome was ‘hands-off CPR time’ – the time between stopping chest compressions to retrieve the AED to starting chest compressions again after the AED delivered its shock. Secondary outcomes were time spent away from patient retrieving AED; time from start of 999 call to first shock; ease of AED retrieval (after analyses of ‘System Usability Scale’ [SUS] scores, findings from post-simulation interview and findings from video and audio call analyses).
Format of the simulations: Participants were informed that they: would find a simulated patient in the building who was unconscious and not breathing; should indicate when wishing to make an emergency (999) call and help the patient as they saw fit; would have an AED delivered by drone; and should retrieve the AED when indicated that it was safe to do so.
A study team member observed the participant but did not intervene, other than to hand them a mobile phone with a pre-programmed number for the simulated 999-call. The participant was connected to a Welsh Ambulance Services NHS Trust (WAST) call-handler. The call-handler was operating at a training centre but handled it as if it were a ‘live’ 999-call, using the Advanced Medical Priority Dispatch System (AMPDS) to prioritise the call.
Once the call-handler recognised a potential OHCA there was an automatic allocation to a mobile device (Terrafix Ltd, http://www.terrafix.co.uk/) allocated to a study team member (CP) from WAST. This team member was situated with the drone operator and then cued them to initiate flight. For these simulations, the drone was situated out-of-sight of participants, approximately 50 m away. It flew to the delivery site and delivered the AED.
The study team indicated when it was safe to approach the drone by sounding a loud siren. Additionally, the 999 call-handler gave the following instruction: ‘A defibrillator has been dispatched to your location by drone. When it has arrived, and it is safe to approach a horn will sound allowing you to retrieve it safely. Please let me know as soon as it is right next to the patient.’
Analyses: Simulations were timed: starting when participants entered the building and ending once participants resumed CPR after attaching the AED and delivering a shock. Key study timings were recorded manually and subsequently checked against the video recording of the simulations. There were two fixed position video cameras: one inside directed at the manikin, and one outside directed at the drone delivery site. Welsh Ambulance Services NHS Trust made audio recordings of the 999-call on the first study day, but this did not happen (inadvertently) on the second day. The phone audio on the second study day was audible via the video recording.
Our study employed multiple methods including positivist and interpretivist enquiry. The positivist elements sought to describe certain concepts such as speed within the specific operation of use drone-delivered AEDs in OHCA. Concepts such as bystander experiences and ease of retrieval of AED in OHCA required an interpretivist epistemological approach. 24 This approach acknowledges that such experience and meaning is subjective, varies and is dependent on context and environment.
We reviewed simulation video and audio and administered a post-simulation questionnaire and conducted brief post-simulation interviews (described below) in an attempt to capture information about participants’ experiences. There was a recognition that interactions between humans and their environment are complex and often unpredictable and that there should be no pre-set hypothesis about how study participants would react as the simulation unfolded. 25 The study team recognise the limitations of our pragmatic approach and make no claims as to the generality of the findings related to bystander experience; indeed, other AED drone delivery systems could yield different findings. By employing such multiple methods however, this study sought to add to the body of knowledge: providing important positivist insights about what occurs during bystander retrieval of AEDs and interpretivist insights to explain how bystanders experience retrieval of AEDs.
The short post-simulation questionnaire was based on the SUS. This was developed in industry to assess the usability of a new device or system and has been made freely available for usability assessments 26 and has been validated in this setting. 27 The brief (<5 min) interview asked participants about their experience of retrieving the AED. Interviews were based on the ‘Learning Conversation’ used in resuscitation courses to evaluate behaviours during mock cardiac arrest simulations. 28 CMS administered the questionnaire and conducted the interview. The questionnaire and interview topic guide are available in the Electronic Supplementary Material.
The results section details study timings and post-simulation questionnaire scores (1: strongly disagree to 5: strongly agree) as median (interquartile range, IQR). JP directly observed participants in simulations and made notes between simulations. CMS performed post-simulation interviews and also made contemporaneous field notes based on the observations of the study team during simulations. CMS transcribed these contemporaneous handwritten notes and added further information after reviewing audio and video of the simulations.
CMS and JP manually reviewed the summated information from the questionnaire, post-simulation interviews and review of simulation audio and video to identify key themes relating to the participants’ interaction with the AED, drone and 999-call-handler. Both then added their reflections, independently considered important issues and grouped them into relevant themes, and decided final themes by consensus.
There was an iterative approach to understanding and synthesising information to make it accessible to those reading, which is common to thematic analyses. 29 Efforts to improve reliability of findings were made by triangulating data from multiple sources and organising it into written notes before analysis and presentation, 30 generating themes inductively with little pre-determined ideas about what these might be. However, it must be acknowledged that both CMS and JP are medical professionals with clinical experience and academic interest in the management of OHCA. The guiding principle was the study's research aim and so there was a focus on information about the participants’ interaction with the AED, drone and 999-call-handler.
Ethical considerations
The study received ethical approval from the University of Warwick Biomedical and Scientific Research Ethics Committee (ref: BSREC 109/19-20) on 02 June 2020.
Simulations were COVID-safe, in line with UK government guidelines at the time. 31 Participants performed compression-only CPR on the manikin.
All study data were stored electronically on an encrypted University of Warwick device running Windows 10. Paper-based data collected on study days were scanned onto the computer within 48 h and shredded the originals.
Patient and public involvement
There were no patients in this project. The project had a ‘patient and public involvement’ representative, who contributed to review and re-draft of project protocol and all participant-facing documents; observed and offered feedback to the study team on study days; reviewed and co-authored this published article.
Results
Developing the delivery system
There were five test flights in November 2020. Timings for the two delivery system configurations are recorded in Table 1.
Timings for delivery system configurations (seconds, median value in bold).
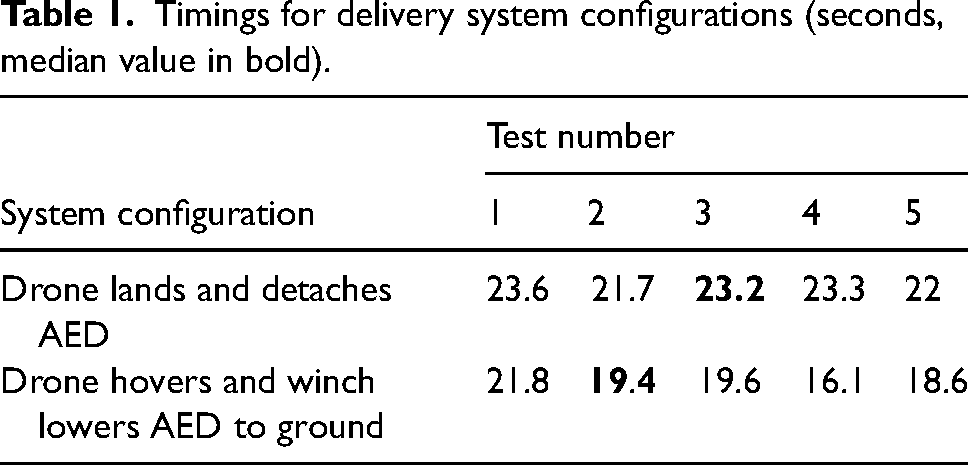
Using the winch was slightly faster. The development team inferred this was largely because the winch lowered the AED faster than the drone could descend to the ground. This and additional concerns about people prematurely approaching a landed drone whose rotors were still operating meant that the study proceeded using the winch mechanism.
Out-of-hospital cardiac arrest simulations
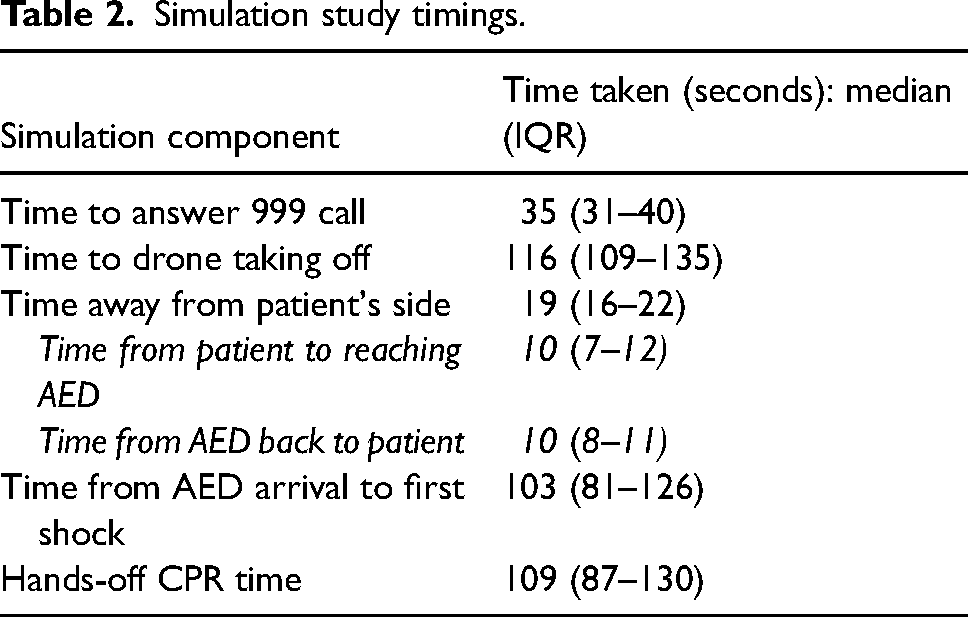
The study recruited 18 participants (n = 10 female, n = 15 previous CPR training); all attended. All participants successfully retrieved the AED, attached it to the patient, delivered a shock and resumed CPR. The median hands-off time was 109 s (87–130 s). The call-handler answered the 999 call in a median of 35 s (31–40 s), and the drone took off a median of 116 s (109–135 s) seconds after the simulation started. When retrieving the AED, the participants were away from the patient for a median of 19 s (16–22 s). Table 2 has full timings.
Simulation study timings.
The post-simulation questionnaire (Table 3) indicated that participants were confident interacting with the drone and did not find it difficult.
Post-simulation questionnaire.
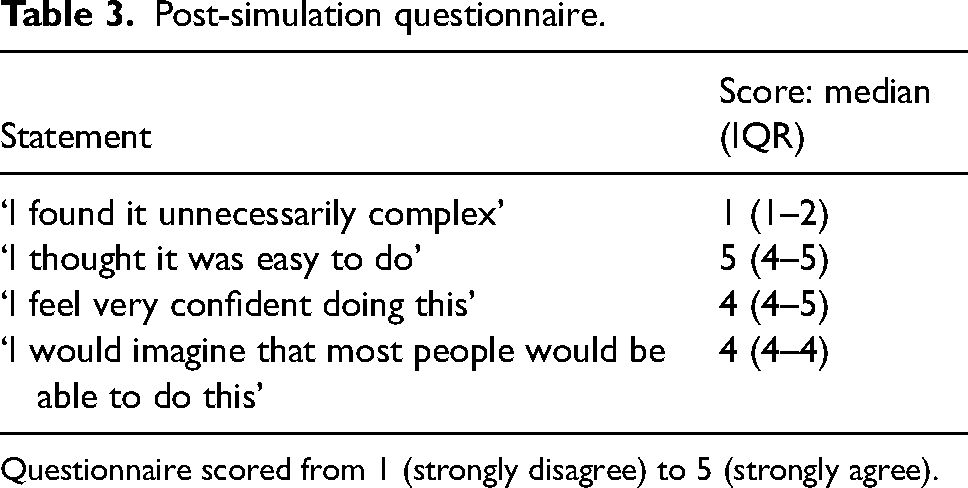
Questionnaire scored from 1 (strongly disagree) to 5 (strongly agree).
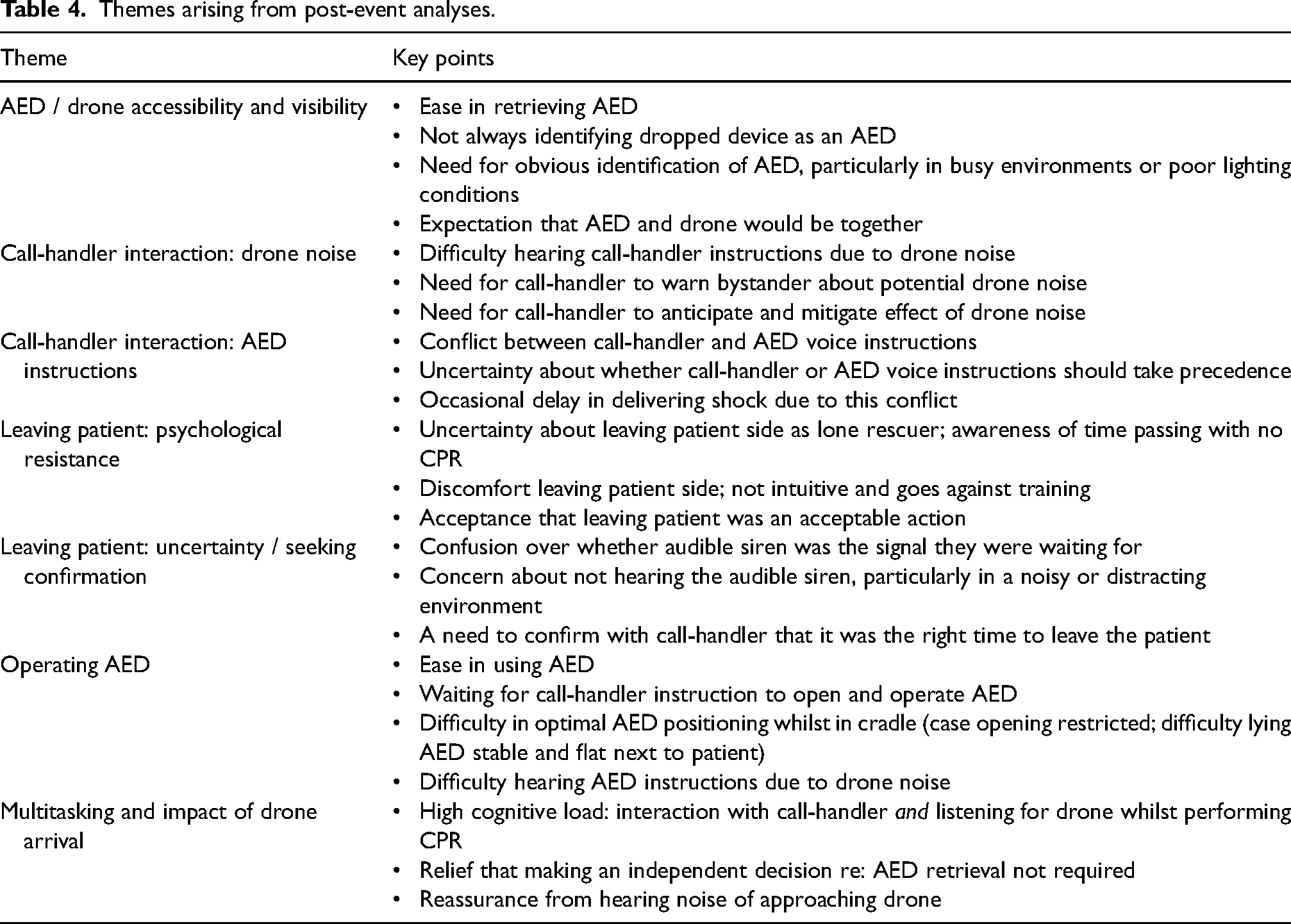
Eight participants reported that they did not immediately identify that the device on the ground was the AED they were looking for, although video analyses revealed negligible delays in moving towards the AED in any simulation. The drone noise (arriving and departing) made hearing call-handler and AED instructions difficult. Participants were sometimes uncertain about when it was safe for them to leave the patient to retrieve the AED, even after hearing the siren. Several participants directly asked the call-handler if they could leave the patient before doing so.
Retrieving the AED was easy. However, the cradle at the end of the winch in which it was held (see Figure 1) interfered with lying the AED down flat and made it more difficult to access the button required to open the case. There was sometimes conflict between call-handler instructions and AED voice instructions about how to use the AED. Table 4 summarises the main themes emerging during post-event interview and audio-visual analyses.

The drone, AED and its cradle.
Themes arising from post-event analyses.
Discussion
Main findings
Lowering an AED from a drone via winch was quicker and felt by the study team to be safer than the drone landing and the AED detaching during the development of the drone delivery system. Participants in the lone-rescuer simulations had a median of 109 s ‘hands-off CPR’ when retrieving the drone-delivered AED but spent only 19 s away from the patient's side retrieving the AED from the drone. This means that, in the current study, an AED delivered directly to a lone rescuer by drone would only increase hands-off CPR time by an extra 19 s compared to a (hypothetical) scenario involving delivery of an AED directly to a patient's side. Participants found it easy to interact with drone and AED and were willing to do so despite some expressing discomfort at having to leave patient.
Simulations revealed issues about AED visibility and AED stability in its cradle when positioned next to a patient. Drone noise had a substantial impact on participants’ interactions with the call-handler, and there was sometimes conflict between call-handler and AED voice instructions. Whilst the arrival of a drone-delivered AED gave participants an extra thing to consider, some recognised that delivering an AED to their location relieved them of the decision to retrieve one.
This current study saw an AED lowered to the ground via winch using a rotary wing drone. In a previous UK study, researchers used fixed-wing aircraft to carry an AED a total of 92 km in six test flights in a coastal air corridor. The AED was dropped by parachute from a height of 120 m, and it landed within 50 m of the target location. 17 This is the first UK study to demonstrate safe AED delivery immediately outside the target location and a subsequent effective interaction between bystander and drone/AED and is an important first step to establishing effective drone-delivery of AEDs in the country.
The study demonstrated a median hands-off CPR time of 109 s. In a 2018 simulation study in Sweden, four untrained participants in lone-bystander scenarios retrieved a drone-delivered AED with a hands-off CPR time ranging from 75 to 110 s. That study also reported, like this current study, that participants found drone/AED interaction easy, felt relieved when the drone arrived and perceived that effective communication with the call-handler facilitated AED use. 16
To minimise time delays during drone delivery of an AED, it is just as important to optimise processes before flight (i.e., from time of OHCA recognition to the time that the drone is ready to fly) as it is once the drone has arrived and bystanders interact with it.
In Germany, researchers performed end-to-end simulations, fully integrating a drone delivery network with local ambulance service systems, for 46 simulated OHCAs across five flight paths. Unlike the current study, these simulated OHCAs allowed testing of the whole process from the start of the emergency call to AED attachment and use. Mean time to defibrillation (from time of emergency call) was 6:02 min for the shortest route (only 0.4 km), suggesting substantial delays before and/or after the drone flight itself. 21
Automated External Defibrillators were dispatched via drone for 12 real-world OHCAs in Sweden (June–September 2020), arrived on scene on 11 occasions, and before the ambulance service seven times. However, a drone-delivered AED was not attached to a patient on any occasion. There was a median time delay of 3:10 min from the emergency call starting to the initiation of drone flight. 19 Shortening this delay may improve the effectiveness of the system, and this current study suggests that the call-handler may have a role in encouraging the bystander to leave the patient briefly to retrieve the AED. This needs further exploration.
Drone-delivered defibrillation is possible. In the Swedish system (December 2021), a 71-year-old man was defibrillated with a drone-delivered AED and survived to hospital discharge. The drone took off 2:15 min after the emergency call started, and the time from emergency call to first shock was 6:15 min. 20
Clinical implications
If drone-delivered AEDs are to be successful in real-life OHCAs, researchers must optimise multiple processes. These include preparing an effective network (e.g., modelling optimal drone base locations, deciding on response radius and dispatch rules) and optimising both pre-flight (automated processes to activate drone and pilot following OHCA recognition during a 999 call; liaison with air-traffic control about flight paths) and post-flight (safe AED delivery, with effective bystander interaction) processes. 32 Implementing a drone-delivered AED network will have broader implications for the aviation and logistics industries. Currently, routine ‘beyond-visual-line-of-sight’ (BVLOS) drone flight is tightly regulated, in many countries, and work in healthcare settings that demonstrate safe and effective BVLOS flight may potentially facilitate its adoption in other settings.
This study reported a median hands-off CPR time of 109 s. However, participants only spent 19 s away from the patient – this is the additional hands-off time compared to a lone-rescuer having their own AED on site. The study authors have not seen this latter calculation reported elsewhere. This 19 s delay may be acceptable if it can be replicated in a real-world situation. Researchers in an international survey considered that an intervention causing a 5% improvement in OHCA survival was clinically relevant. 33 Following collapse, each minute without intervention equates to an approximately 10% decrease in survival. 34 The study authors would therefore consider that an addition of 30 s (representing an approximate 5% decrease in survival) or more without intervention (caused by retrieving an AED from the drone compared to another method of AED delivery to the patient's side) would be clinically relevant.
This study demonstrated that the 999 call-handler's role is vital, and so there is a need for effective real-time communication between the drone, its operator and the call-handler. The conflict noticed between call-handler and AED instructions and how this might be handled in real-world situations is an important finding that is relevant to every circumstance in which an AED arrives on scene (and not just if delivered by drone). The delay that this might cause was not quantified in this project, but is an area for further exploration. Future researchers can improve usability and visibility of drone-delivered AEDs to make them even easier to use.
The use of drone-delivered AEDs does not fit into a ‘script’ or protocol (such as AMPDS) used by ambulance services. How and where it should fit in – especially as asking a lone bystander to leave an OHCA patient is not usual practice – is an important topic for future research, as is optimising standardised dispatch-assisted AED instructions to reduce conflict between call-handler and AED voice instructions.
Multiple-rescuer situations would result in no additional hands-off time – one rescuer would continue CPR whilst the second retrieves an AED – and so the study did not seek to examine this in the current simulation. The authors know of no ambulance services that would ask a lone rescuer to leave a patient to retrieve a nearby fixed-location public-access AED. The fact that retrieving an AED from a drone does involve a lone rescuer leaving the patient means that examining the time taken and the likely feelings of the rescuer when asked to do that is an important output from this simulation.
Next steps
The current study demonstrated only the ability to carry and deliver an AED via drone, and that study participants could safely and effectively interact with it. This study team are working towards the development of a fully integrated drone-delivery system for simulated OHCAs in the UK (https://fundingawards.nihr.ac.uk/award/NIHR204382). This will involve automated, near instantaneous, activation of a remote drone system by the ambulance service once a potential OHCA is recognised during a 999 call, beyond-visual-line-of-sight flying in dedicated flight corridors and real-time flight path mapping. This current study highlighted that good interaction between bystander and call-handler was vital: developing effective real-time communication between drone and ambulance service systems will allow the call-handler to keep the bystander updated about drone progress and instruct them when it is time to retrieve it. Demonstrating this system will be a pre-requisite to live operations for real-world OHCAs in the UK.
Strengths and limitations
This study reports on bystander interaction with a drone-delivered AED for the first time in the UK. The study examined only the lone-rescuer situation and did not compare this with two-or-more rescuer simulations. It did not consider OHCAs occurring in multi-level buildings or the delay to AED retrieval that this might cause. A scoping review has previously reported lower availability of AEDs, poorer quality CPR and significantly lower survival to hospital discharge and survival with good neurological outcome following OHCA occurring on higher floors in multi-level buildings. 35
This study presents both quantitative and qualitative data, the latter being useful to explore participants’ experiences and behaviours. 36 There is ‘triangulation’ of data from different sources in an attempt to present a richer picture of the participant experience. 37 However, there are some methodological limitations. The SUS has not, to the authors’ knowledge, been used or validated in cardiac arrest research. Similarly, the ‘learning conversation’ approach is usually used in teaching and education settings, rather than having being validated for use in interviews or for data collection. Its use here was pragmatic, although its relevance and suitability as a data collection method can be questioned. The post-event interviews were brief, notes only were taken and they were not recorded, so the study did not capture direct quotes.
Indeed, the study team developed the study pragmatically, intending to gather useful information about drone delivery of AEDs and the bystander experience, but perhaps could have done so with better regard to qualitative research paradigms and theoretical frameworks during analyses. Nevertheless, an understanding of human behaviours is key to the successful implementation of any complex system,38,39 such as the use of drone-delivered AEDs to complement the community response to OHCA, and the study team believe that the approach taken in this project has delivered some genuine insights, and is a major strength of the study.
The participant sample was pragmatic and convenient. There was not a formal assessment of data saturation for qualitative analyses. An appropriate sample size depends on several factors, but will be reduced by the specificity of the situation being investigated (e.g., here, fetching a drone-delivered AED), homogeneity of participants (all performing a standardised simulation), and the briefness of the post-event interview and audio/video clips. 40 Future studies that ultimately try to determine whether or not there is a patient benefit will ideally take the form of a randomised controlled trial. The study team did not consider a priori what a meaningful ‘hands-off’ time would be but future studies comparing AED delivery methods would have to define this to make appropriate sample size calculations. This work is still some way away.
Most of the participants had prior CPR training. Additionally, participants were briefed ahead of the simulation that they would find a patient in cardiac arrest. In the UK (2017), 59% have reported previous CPR training and 19% previous AED training. 41 The study participants may therefore not be representative of the wider public, and their CPR performance and response to the drone-delivered AED may be better than the average bystander in a real-world situation. In the simulations, a siren indicated safe drone arrival because effective communication systems between drone and 999 call-handler did not yet exist. Participants indicated that a direct instruction from the call-handler would be a better option than listening for an audible cue to approach the drone.
Conclusion
Participants in OHCA simulations found it easy to interact with and use drone-delivered AEDs. An AED delivered directly to a lone rescuer by drone only slightly increased hands-off CPR time (by an extra 19 s) compared to delivery of an AED directly to a patient's side. It may therefore be feasible for lone-rescuers at the scene of an OHCA to retrieve a drone-delivered AED with minimal additional interruption to CPR. However, there is much scope to optimise the bystander interaction once a drone-delivered AED has arrived on scene, and the call-handler will have a vital role in this.
Supplemental Material
sj-docx-1-pam-10.1177_27536386241281061 - Supplemental material for Drone-delivered automated external defibrillators for out-of-hospital cardiac arrest: A simulation-based feasibility study
Supplemental material, sj-docx-1-pam-10.1177_27536386241281061 for Drone-delivered automated external defibrillators for out-of-hospital cardiac arrest: A simulation-based feasibility study by Christopher M Smith, Joe Phillips, Nigel Rees, Carl Powell, Anthony Sheehan and Mary O’ Sullivan in Paramedicine
Supplemental Material
sj-docx-2-pam-10.1177_27536386241281061 - Supplemental material for Drone-delivered automated external defibrillators for out-of-hospital cardiac arrest: A simulation-based feasibility study
Supplemental material, sj-docx-2-pam-10.1177_27536386241281061 for Drone-delivered automated external defibrillators for out-of-hospital cardiac arrest: A simulation-based feasibility study by Christopher M Smith, Joe Phillips, Nigel Rees, Carl Powell, Anthony Sheehan and Mary O’ Sullivan in Paramedicine
Footnotes
Acknowledgements
TETRA drones for their work on developing the drone delivery system, and for flying the drone and providing technical support on simulation days. Steven Prince and colleagues at Sussex Police Training Centre for hosting the simulations and the study team. Christopher Shoebridge for videography on simulation days. The call-handler team at WAST for answering training 999-calls on simulation days.
Data availability
Simulation study day timings, responses to the questionnaire based on the SUS, field notes and sorting of these notes into themes are available in the Electronic Supplementary Material.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Christopher M Smith has volunteer roles with Resuscitation Council UK, European Resuscitation Council and the International Liaison Committee on Resuscitation. He is a National Institute for Health Research-funded Clinical Lecturer in Emergency Medicine in the UK. Joe Phillips has volunteer roles with Resuscitation Council UK. Nigel Rees is an associate editor of Paramedicine journal.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by a Resuscitation Council UK Research and Development Grant, awarded on 15th January 2020 (Project ID: 2019-1692778121). The AED was funded through this award but the CPR manikin was not (the study team already had access to this). The views presented in this article are those of the authors and not necessarily those of the funders.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.