
Abstract
Introduction
Following the declaration of COVID-19 as a global pandemic, significant challenges were introduced to many sectors of the healthcare system, including paramedicine. Understandably, concerns that a surge in healthcare system utilisation could overwhelm resources and compromise patient safety led to the development of innovative strategies to address these concerns. For example, at the hospital level in Canada, strategies included cancellation of elective surgeries and accommodation of alternate level of care patients in alternate settings. 1 In Germany, visits were made to COVID-19 patients in their homes to monitor whether they required hospitalisation. 2 At the community level, strategies included utilisation of telehealth in the United States, 3 a web-based self-triage system in Denmark, 4 and a telephone triage system in Israel with home-testing conducted by paramedics. 5
Also, because the severity of symptoms varies significantly among COVID-19 patients, 6 and a proportion presenting with low-acuity complaints do not require immediate assessment and treatment in hospital, strategies were implemented in the United States7,8 and Denmark 9 to identify and not transport to hospital individuals calling 9-1-17,8 or a general practitioner 9 who presented with low acuity symptoms suggestive of COVID-19 who could be left at home.
For several years preceding the COVID-19 pandemic, paramedic practices around the world have developed varying options for patient disposition including alternate destinations and discharge of low acuity patients from the scene,10–14 although concerns for patient safety have been expressed.15–19
In Ontario, Canada, however, provincial legislation has required all patients accessing 9-1-1 to be transported to a hospital emergency department unless the patient or substitute decision-maker refuses transport. But in the face of the COVID-19 pandemic, to reduce the potential burden on hospital services as well as avoid unnecessary risks of contagion to hospital staff, patients and visitors, a medical directive, novel for Ontario, was approved by the Ontario Ministry of Health. This medical directive authorised paramedics (following telephone consultation with and approval of an EMS physician) to manage patients with confirmed or suspected COVID-19 infection who met pre-defined criteria at the scene without transportation to hospital. The objectives of this study were to measure compliance and patient safety associated with the use of this medical directive. Specifically, we aimed to:
Determine, among patients who were not transported under the COVID-19 medical directive, the proportion for whom paramedics and EMS physicians complied with the requirements of the directive. Determine the proportion of patients not transported who called 9-1-1 again within 7 days.
Methods
Study design and setting
This was a retrospective descriptive study employing a record review of 9-1-1 calls to paramedic services under medical delegation of the Sunnybrook Centre for Prehospital Medicine, which includes Halton Region Paramedic Services, Muskoka Paramedic Services, Peel Regional Paramedic Services, Rama Paramedic Services, County of Simcoe Paramedic Services, and Toronto Paramedic Services. These paramedic services responded to 597,033 calls in 2021 where patient care was provided. These services collectively employ approximately 3100 paramedics providing service to approximately six million inhabitants. Records reviewed were patients’ ambulance call reports and recorded telephone consultations with EMS physicians.
Paramedics in Ontario, Canada, are not self-regulated. Their practice is governed through legislation, specifically the Ambulance Act. 20 Paramedics complete a 2-year college diploma programme. Advanced care paramedics complete an additional year of study, which enables them to perform advanced cardiovascular life support resuscitations and advanced medical procedures as per the Ontario Advanced Life Support Patient Care Standards (ALS PCS) published by the Ontario Ministry of Health. 21 The ALS PCS are reviewed and developed based on evidence by a medical advisory committee that makes recommendations to the Ministry of Health.
The Assessment of Patients with Possible COVID-19 Medical Directive (COVID-19 medical directive) was created by the Ontario Base Hospital Medical Advisory Committee and published on 23 November 2020, by the Ontario Ministry of Health for use by paramedics (see Supplemental Appendix 1). 22 The goals were to decrease the number of low acuity patients with suspected or confirmed COVID-19 transported to the emergency department while providing appropriate and safe care, which included providing a leaflet to non-transported patients with follow-up advice and instructions to phone 9-1-1 again if symptoms worsened.
Prior to implementation of the COVID-19 medical directive, 100% of paramedics successfully completed a 1-hour provincially developed online asynchronous education module with a minimum passing score of 70%. The 60 physicians who participate in the patch system were not required to complete the mandatory online course that was designed for paramedics; however, all EMS physicians received a memo outlining the new directive and were offered two optional online question and answer sessions. In addition, 23% attended additional patch rounds related to the COVID-19 medical directive, and reminders were provided quarterly at patch physician meetings.
Study population
Paramedics were directed to assess all patients who phoned 9-1-1 on scene for suspected or confirmed COVID-19 as per the COVID-19 screening tool for paramedics (Supplemental Appendix 2) 23 and (Supplemental Appendix 3). 24 For patients considered by paramedics as meeting the COVID-19 medical directive criteria and who consented to non-transport, paramedics were required to obtain approval through a telephone consultation (known as a ‘patch’) with an EMS physician.
All cases where paramedics applied the COVID-19 medical directive and patched to an EMS physician were included during the data collection period, 1 January 2021, through 31 March 2022. However, paramedic services activated the medical directive and enrolled patients at different times within the study period based on the assessed need within each community. Cases were identified from the electronic patch (ePATCH) database housed at the Sunnybrook Centre for Prehospital Medicine.
We were not able to identify patients who might have screened positive for COVID-19 and met the COVID-19 medical directive criteria for release on scene if the paramedic did not screen the patient for COVID-19 or initiate a patch to an EMS physician for authorisation to release the patient from care. Thus, we could not identify cases where the patient was stable and the patient or the substitute decision-maker either (1) requested transport, (2) requested release from care before the paramedic patched to the physician or (3) the paramedic made a decision to transport the patient (Figure 1).
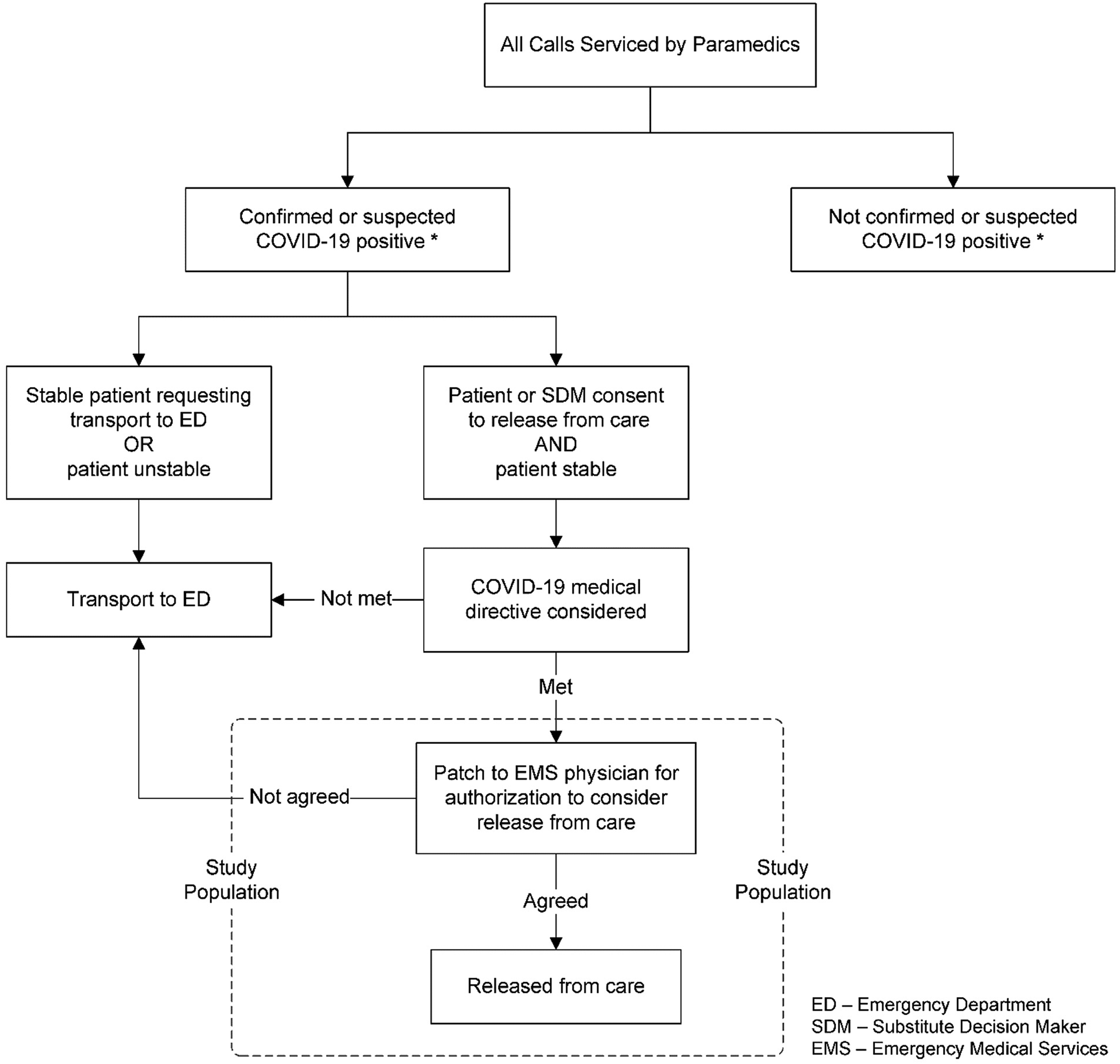
Study population.
Data sources
Eligible patients were identified from the electronic patch (ePATCH) database maintained by the Sunnybrook Centre for Prehospital Medicine. This database includes all patch conversations between paramedics on scene and EMS physicians. These are audio recorded, catalogued and stored electronically. Corresponding electronic patient care records (ePCRs) completed by the attending paramedic were matched with each identified patch recording.
Outcome measures
The primary outcome of our study was the proportion of patients where the paramedics and EMS physicians appropriately applied the COVID-19 medical directive. Appropriate application was defined as patients meeting all criteria of the medical directive within the specified parameters, all of these having been verbally reported by paramedics to the EMS physician and the patch physician agreeing that the patient can be left at home. If any criteria were not reported or were not consistent with the medical directive, the patient did not meet criteria for non-transport.
The secondary outcome was the proportion of patients considered to have met the directive and were not transported who subsequently called 9-1-1 again within 7 days. The COVID-19 screening tool was again administered by the responding paramedics for patients who accessed 9-1-1 again within 7 days.
Data abstraction and analysis
A single data abstractor (JS, manager, professional standards and compliance) listened to each patch audio recording of included cases and entered study information into a standardised data extraction template. Abstracted data included the following objective measures: patient age, sex and the following parameters as specified in the medical directive: respiratory rate, blood pressure, heart rate, Glasgow Coma Scale, oxygen saturation (SpO2), level of awareness (LOA) and patient acuity designation utilising the Canadian Triage Acuity Scale (CTAS) 25 as reported by the paramedic to the EMS physician. Additionally, patient demographics, call characteristics and last documented vital signs were abstracted from the corresponding patient's ePCR. It was also recorded whether the EMS physician agreed to apply the medical directive for non-transport of the patient to the emergency department, and, if so, whether the patient had continued to agree to remain at home. In cases where the patient was to be left at home, the abstractor documented whether the paramedic had reported the patient's ability to self-isolate, access food, phone and other necessities, as well as the presence of an appropriate caregiver, as needed.
We calculated descriptive statistics for our population, using mean (SD) or count (%) as appropriate. All data analysis was done using SPSS Statistics version 27 (IBM SPSS, Armonk, NY). We used the STROBE cross sectional reporting guidelines. 26
Ethics statement
Permission to conduct the study was granted by the Research Ethics Board of Sunnybrook Health Sciences Centre, Ontario, Canada.
Results
Overall, 122 patients were considered by paramedics to meet the COVID-19 medical directive, and, therefore, contacted an EMS physician via a patch. These patients had a mean age of 46.8 years (SD 17 years), range 5 to 96 years, and 53.7% (65/122) were female. A total of 73.8% (90/122) of the patients had tested positive for COVID-19 prior to contact with paramedics, while the remainder screened positive according to the COVID-19 screening tool. The 90 patients with COVID-19 contacted 9-1-1 an average of 5.3 days (SD 3.4 days) after testing positive.
The proportion of patients for whom paramedics had verbally reported all criteria in the COVID-19 medical directive for non-transport was low. All required patient assessment findings were verbally reported and within ranges specified in the medical directive in only 20% (25/122) of cases (Table 1). When examining the same assessments that had been documented on the patient's ePCR, the proportion of patients who met the specified criteria for non-transport in the medical directive was much higher at 49% (60/122) (Table 2).
Patient assessment findings as specified in the COVID-19 medical directive and verbally reported to the EMS physician that were within the specified range.
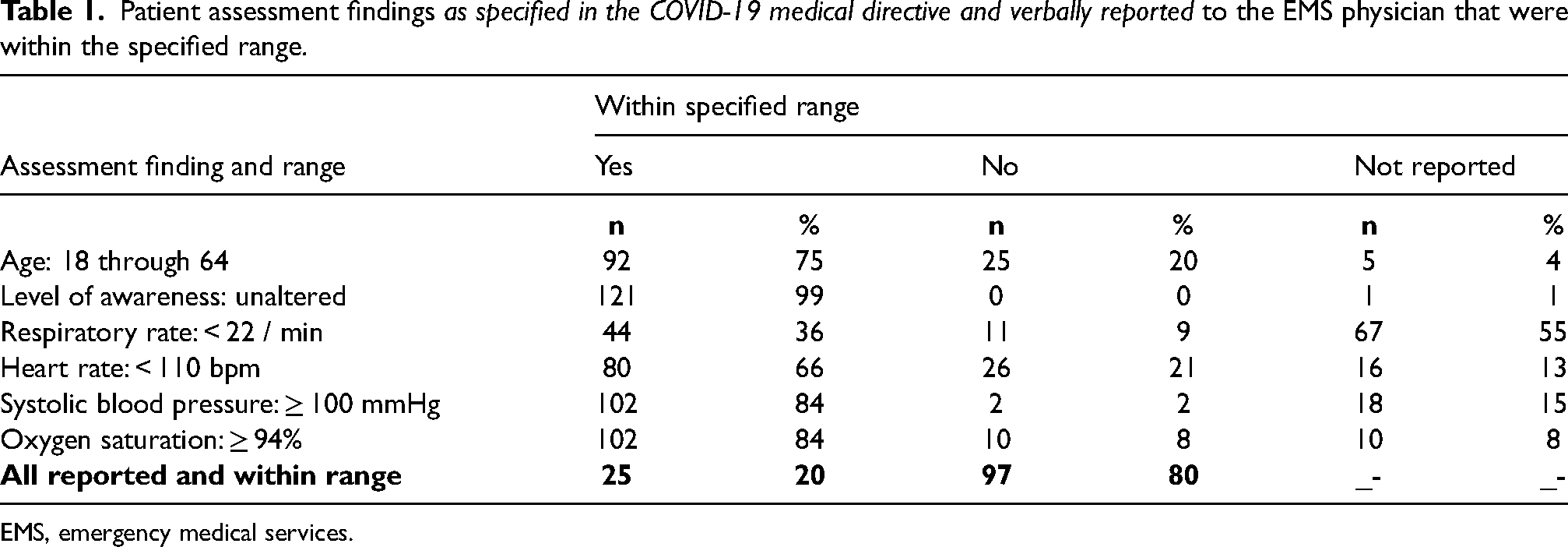
EMS, emergency medical services.
Patient assessment findings as specified in the COVID-19 medical directive and as documented on patient's ePCR that were within specified range.
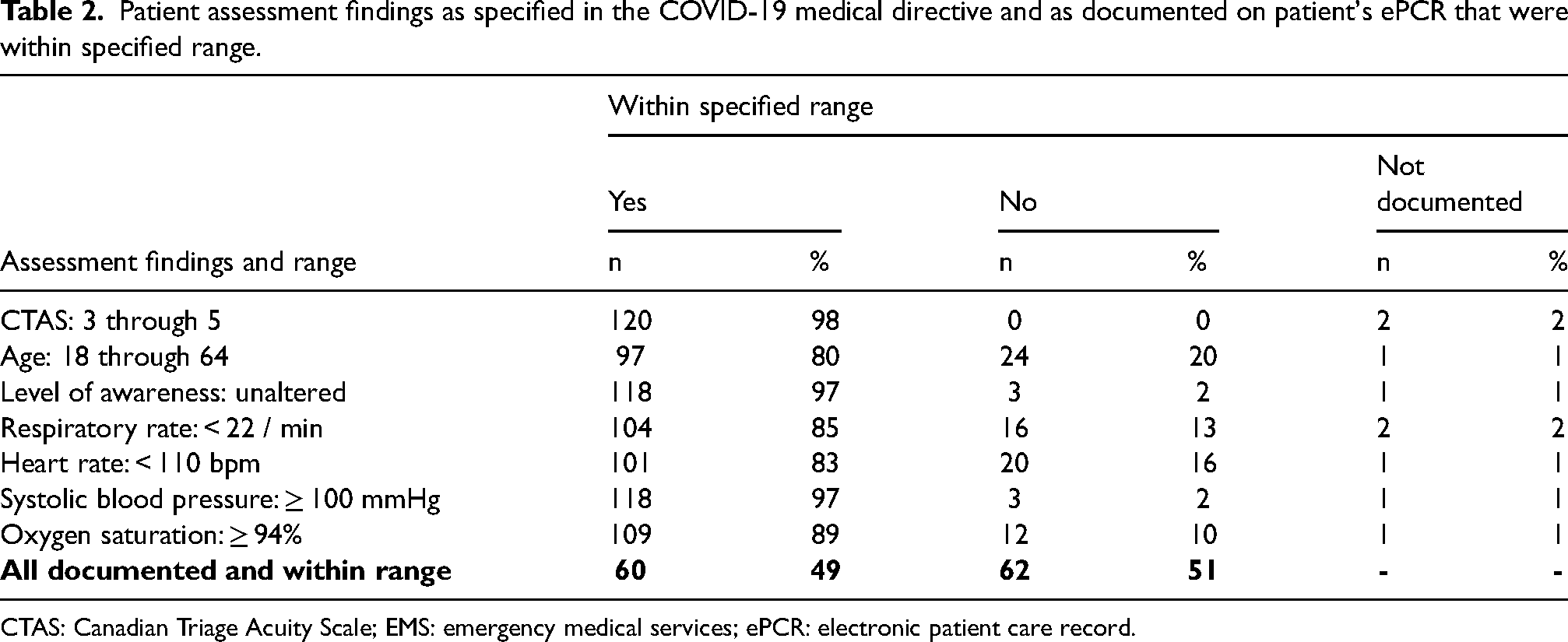
CTAS: Canadian Triage Acuity Scale; EMS: emergency medical services; ePCR: electronic patient care record.
There was considerable variability among paramedic reported and documented assessment findings. For example, LOA was reported during the patch to have met the criteria for 99% of cases, but respiratory rate was only reported and within the specified range for 36% of cases. In comparison, according to documentation on the ePCR, LOA was within the specified range for 97% of cases and respiratory rate was within the specified range for 85% of the cases.
In 83% of cases (101/122), the EMS physician authorised non-transport (Figure 2). Ninety-nine of these patients were released from care at the scene by paramedics and two were transported to hospital, one because of patient preference and the other at the request of the patient's family doctor. Of these patients, a total of 55% (55/101) met the COVID-19 medical directive criteria for non-transport as documented on the ePCR, and a total of only 25% (25/101) met the directive as verbally reported to the EMS physician.
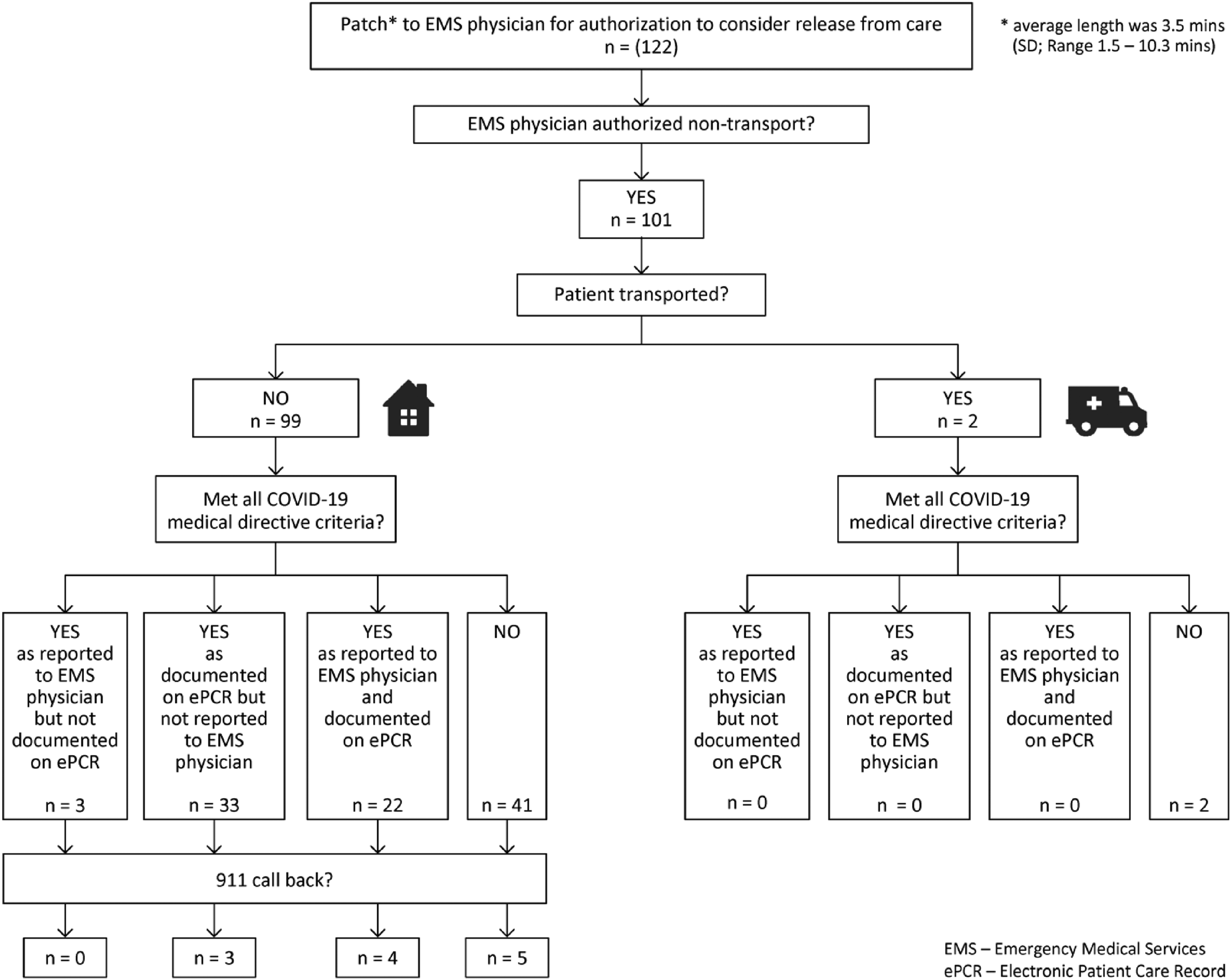
Patient disposition after emergency medical services (EMS) physician consultation, non-transport authorised.
Of the patients who were not transported to hospital and where the EMS physician had authorised non-transport, 12% (12/99) called 9-1-1 again within 7 days of the index event. All of these call-backs were for COVID-related symptoms and complaints (Table 3).
Patients who called 9-1-1 within 7 days after initial non-transport at index visit.
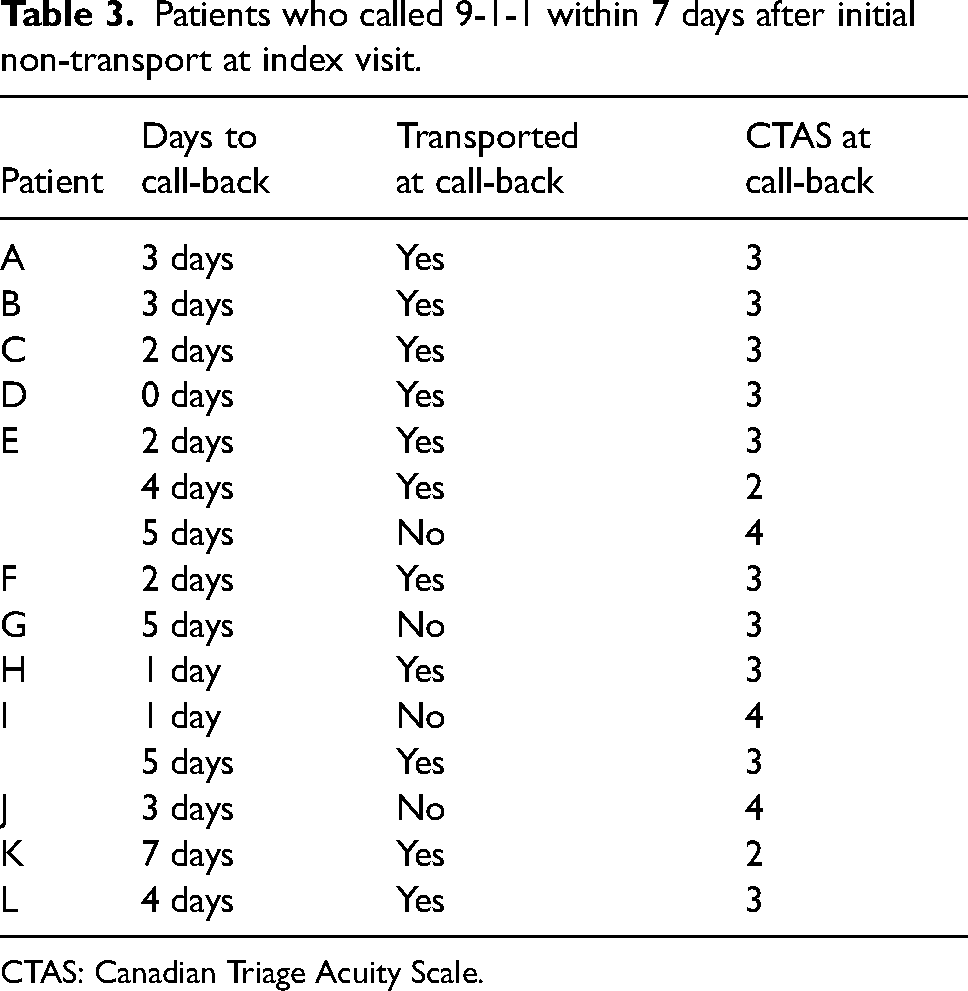
CTAS: Canadian Triage Acuity Scale.
Of the 17% (21/122) of patients who were not authorised for non-transport by the EMS physician (Figure 3), 14 were transported to hospital, and seven refused transport and were released from care at the scene (see note, bottom Figure 3). Of these 21 patients, five met the COVID-19 medical directive criteria as documented on the ePCR, and none met the criteria for non-transport as reported to the EMS physician via the patch. There were no repeat calls to 9-1-1 among the seven patients not transported.
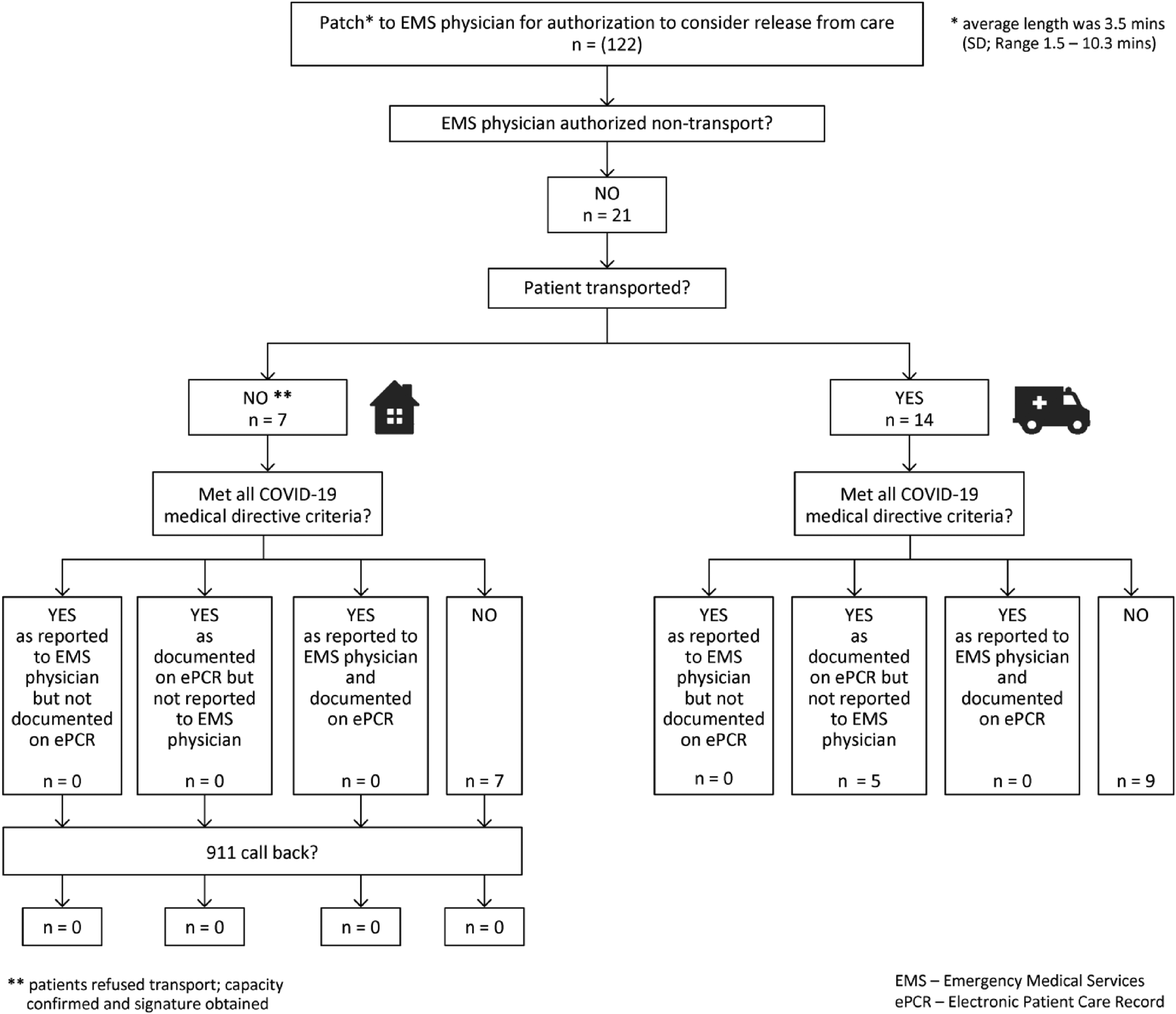
Patient disposition after emergency medical services (EMS) physician consultation, non-transport denied.
Among the 12 patients not transported who called 9-1-1 again within the 7-day period, the average interval to the first 9-1-1 call-back was 2.8 days (range 0–7 days). For the 12 who called back, 10 were transported to hospital. Of these, only two were considered by paramedics to be CTAS 2 (high acuity).
Discussion
Our objectives were to determine the proportion of patients for whom paramedics and EMS physicians complied with the requirements of the directive as well as the proportion of patients not transported to hospital who called 9-1-1 again within 7 days.
We found that compliance with the COVID-19 medical directive was low among both the paramedics and the patch physicians. Nearly half of all patients where the medical directive was applied by paramedics met the non-transport criteria of the medical directive according to paramedic documentation on the ePCR. However, the proportion of calls where the paramedic verbally reported all assessment findings to the EMS physicians was much lower. In addition, physicians authorised non-transport in the majority of cases even though in most of these cases, the patients did not meet the medical directive criteria as reported to them by paramedics.
Our measure of the safety of the application of the COVID-19 medical directive was the proportion of patients not transported who called 9-1-1 again within 7 days. We found that 12% of these non-transported patients called 9-1-1 again. All cases calling 9-1-1 again presented with continuing COVID-19 symptoms and the majority (10/12) were transported to hospital. We could not determine whether these patients had been admitted to hospital nor whether other non-transported patients may have presented to the emergency department on their own.
A contributing factor to the low compliance among paramedics with this new medical directive may have been the increased cognitive burden during the early days of the pandemic as healthcare workers in particular may be susceptible to ‘message fatigue’ 27 due to a high frequency of information and changing advice. Also possibly contributing to low compliance was the asynchronous online delivery (e-learning) of the education related to the medical directive that replaced the usual education methodology whereby didactic sessions are followed by an opportunity to consolidate and apply key objectives. However, whether e-learning may be more or less effective than traditional in-person learning is complex and likely confounded by many factors. 28
Although the patch physicians were not required to complete the mandatory online course that was designed for paramedics, all were required to confirm by email that they had received the information regarding this new directive. But indeed, physicians too were burdened by a great amount of changing information and may not have fully remembered the complete criteria. Therefore, this may explain why not all criteria were requested by the physician. Physicians may have relied on the paramedics to highlight the key points and use their judgment to make a patient-centered decision. This may support the notion of a shared mental model 29 between the paramedic and the EMS physician where communication focused on pertinent positive or negative findings.
We identified three reports of EMS-initiated non-transport strategies for low acuity patients either having or suspected of having COVID-19, also initiated for the same purpose, that is, to reduce the burden on hospital services.7–9 Two of these initiatives were put in place during the first three months of the pandemic, one in Denmark 9 and the other in the US state of Indiana. 7 The third took place in the US state of Connecticut during two time periods, one midway in the pandemic and the other early in 2022 during a surge in the incidence of COVID-19 cases in the region. 8
Unlike in our system where physicians authorised all non-transport decisions, in these three jurisdictions, paramedics made all non-transport decisions under specific predetermined protocols.7–9 In the US studies, paramedics responded to patients phoning 9-1-1,7,8 while in Denmark, patients were referred by a general practitioner for at-home assessment by a paramedic. 9 In the studies reported by Glober et al. 7 and Nielsen et al., 9 paramedics could contact an EMS physician familiar with the protocol for a consultation at their discretion.
Similar to our study, Glober et al. 7 and Couturier et al. 8 reported measured compliance with the non-transport protocols and both groups reported non-compliance with their protocols due to specified contraindications, lack of appropriate documentation, or out-of-range patient age or vital signs. A difference in our study is that non-compliance was measured by whether the paramedic had communicated all required information during the mandatory consultation with a physician. In addition, non-compliance was also measured by whether the physician had authorised non-transport in cases where the patient did not meet the criteria. Similar to our reasoning, Glober et al. 7 suggested that lack of compliance, may have occurred because of the increased demands during the pandemic and rapid requirement to implement a new protocol, such that paramedics may not have adequately benefited from the online education they were given concerning the protocol.
Measures of patient safety were reported in all three of these studies, albeit using different definitions of safety and different patient outcome time intervals than used in our study.7–9
Nielsen et al. 9 reported that 76.5% (449/587) of patients referred for paramedic assessment by a general practitioner were not transported. Of these, 13.1% were referred to a hospital within 72 hours. Unlike our study, this group determined 30-day mortality, finding that 11.1% of patients that had been transported to hospital had died, while 5.8% of patients that had not been transported had died.
Glober et al. 7 reported that 27.8% (40/144) of patients not transported where their treat-in-place protocol was actually used were either seen in the emergency department, were admitted to hospital or had died within 30 days, 25.5% (14/55) of patients where the protocol had not been correctly applied, and 29.2% (26/89) of those where it had been. Couturier et al. 8 reported that 11.6% (8/69) of the patients not transported under their protocol were seen in the emergency department within 24 hours.
Our study results in Ontario align with the reported experiences of these three non-transport strategies. Two of the three study groups reported degrees of non-compliance with the protocols or directions on which decisions for non-transport were to be based. However, it is not possible to compare patient safety outcomes among studies because the follow-up time intervals and inclusion criteria were different among the three studies as well as ours.
The COVID-19 medical directive was the first implementation in Ontario of a strategy to reduce the possible burden on hospital resources by allowing paramedics to discharge patients from the scene. Although novel for Ontario, strategies for non-transport of low acuity patients as well as transport to alternate destinations have been utilised over the years in many countries 10 ,14 in response to increasing utilisation of EMS services, emergency department overcrowding, as well as decreasing availability of primary care services in many communities. 30
To compare our study results with other studies of strategies for patient non-transport generally, we found two reviews of EMS patient non-transport in the literature.11,13 A review by Yeung et al. 13 published in 2019 included 10 studies conducted between 1992 and 2016 that measured proportions and outcomes of patients assessed in the pre-hospital setting not transported to hospital. For three of the reviewed studies, only EMS-initiated non-transport was reported; whether non-transport was EMS- or patient-initiated was not specified for six of the other seven. The proportion of non-transported patients who later presented to the emergency department was reported to have varied among these studies from 5% to 46%, although follow-up rates ranged from 16% to 100%. Because the study methodologies varied greatly, the authors felt that definitive conclusions could not be drawn and that further research is needed to broaden understanding of patient outcomes following non-transport.
A review published by Ebben et al. 11 in 2017 included 67 studies conducted between 1990 and 2016. Included were studies of both EMS-initiated and patient-initiated non-transport to hospital as well as non-transport of specific populations and presentations (such as hypoglycaemic and post-ictal patients and patients with acute opioid overdose). Ebben et al. reported rates for general populations of non-transport ranging from 3.7% to 93.7% and a variety of follow-up periods. They further described a variety of re-access locations, such as EMS, the emergency department, general physicians, or walk-in clinics. Finally, the authors noted a gap in the literature related to ambulance professional competencies needed to make non-transport decisions. They cited a need to study such competencies as well as a need to develop supportive tools to guide non-transport decision making such as evidence-based protocols and guidelines for both general and specific populations.
Our medical directive required that paramedics consult with a physician to authorise patient non-transport, but we found no studies addressing paramedic consultations with a physician to support non-transport decision making.
Paramedic competence and training to independently make appropriate non-transport decisions has been studied. For example, authors of a study in Sweden, in which interviews were conducted with EMS clinicians, reported that clinicians expressed concern with possible inaccuracy of non-transport decisions associated with patient risk. 31 The authors concluded that there is a need for supports such as evidence-based guidelines, revised education curricula, as well as providing learning through clinical feedback following non-transport decisions, 31 a strategy that has been shown to be associated with a decline in the proportion of patients requiring hospitalisation within 24 hours following non-transport. 32
Finally, a review exploring paramedic training to support decision making related to transport of patients with low-acuity presentations was published in 2024. 33 Nine studies were found that met the eligibility criteria. Of these, various types and lengths of training were reported, ranging from a 2-hour training session to extended university training. In addition, five of the studies mentioned the use of protocols and guidelines to support non-transport decisions for low-acuity patients. Although research on this topic was limited, the authors reported finding some evidence that higher level training increases paramedic decision-making confidence and competence. The authors concluded that there is a need to further explore the level of education and training in patient assessment skills that is required to support non-transport and alternate care pathways strategies. 33 The expressed concern with training strategies to increase this paramedic competency suggests that EMS physician consultation may be necessary to support non-transport decision making until the level of appropriate paramedic training can be determined. Along with this, determining best practices with respect to communication between physicians and paramedics during consultations related to non-transport could be helpful.
In general, more research is needed to determine the most appropriate model of care, and it is likely that models of care that allow for safe and appropriate non-transport decisions will vary globally based on structures of paramedic services, education and training. As was discussed some years ago, 34 it continues to be important to standardise measures of patient outcomes in terms of timing and adverse events and to consider what is an acceptable level of under-triage.
Strengths and limitations
A strength of our study was having access to the consultation recordings which were reviewed the same day to monitor the system changes and support the clinicians. Remediation and mentoring were provided to paramedics and EMS physicians within days of the occurrence; thereby, practice could be modified over the course of the protocol implementation period.
A limitation is that we were only able to identify patients where the paramedic patched to an EMS physician, and we were therefore unable to identify patients who met the directive where a patch was not initiated or where the directive had not yet been activated in the community. Also, although we chose a timely and pragmatic approach to monitoring patient safety outcomes, that is, a 7-day window to identify whether a 9-1-1 call-back was initiated, we could only identify patients who accessed further medical care by calling 9-1-1 again within the 7-day period in our catchment area. Patients who utilised their own transportation to an ED or accessed another health care provider were not identified in this study. We were also unable to determine whether returning patients had been hospitalised or had died.
Conclusion
This article presents a novel pathway within Ontario's paramedic regulatory framework. The overall number of cases of use of the medical directive was low; however, there were no instances in which patient safety was known to have been negatively impacted.
Paramedics' written documentation of non-transport criteria was more complete compared with what was verbally reported to the EMS physician. Physicians also varied in compliance regarding authorisation of non-transport in accordance with the medical directive criteria as reported to them.
Further study is needed of other non-transport strategies for low acuity patient presentations with a focus on patient safety and the extent of the resulting alleviation of pressure within the healthcare system. Future research should also focus on training strategies to enhance compliance with decision-making tools and joint decision making between paramedics and physicians regarding patient disposition as well as what training is required for paramedics to independently make non-transport decisions.
Supplemental Material
sj-docx-1-pam-10.1177_27536386241279072 - Supplemental material for Implementation of a strategy to manage EMS COVID-19 patient disposition with physician consultation: A retrospective descriptive study
Supplemental material, sj-docx-1-pam-10.1177_27536386241279072 for Implementation of a strategy to manage EMS COVID-19 patient disposition with physician consultation: A retrospective descriptive study by James Summers, Ian R Drennan, Linda Turner, Maud Huiskamp, W Scott Gorsline, Michael Merko and Morgan Hillier in Paramedicine
Supplemental Material
sj-pdf-2-pam-10.1177_27536386241279072 - Supplemental material for Implementation of a strategy to manage EMS COVID-19 patient disposition with physician consultation: A retrospective descriptive study
Supplemental material, sj-pdf-2-pam-10.1177_27536386241279072 for Implementation of a strategy to manage EMS COVID-19 patient disposition with physician consultation: A retrospective descriptive study by James Summers, Ian R Drennan, Linda Turner, Maud Huiskamp, W Scott Gorsline, Michael Merko and Morgan Hillier in Paramedicine
Supplemental Material
sj-pdf-3-pam-10.1177_27536386241279072 - Supplemental material for Implementation of a strategy to manage EMS COVID-19 patient disposition with physician consultation: A retrospective descriptive study
Supplemental material, sj-pdf-3-pam-10.1177_27536386241279072 for Implementation of a strategy to manage EMS COVID-19 patient disposition with physician consultation: A retrospective descriptive study by James Summers, Ian R Drennan, Linda Turner, Maud Huiskamp, W Scott Gorsline, Michael Merko and Morgan Hillier in Paramedicine
Supplemental Material
sj-docx-4-pam-10.1177_27536386241279072 - Supplemental material for Implementation of a strategy to manage EMS COVID-19 patient disposition with physician consultation: A retrospective descriptive study
Supplemental material, sj-docx-4-pam-10.1177_27536386241279072 for Implementation of a strategy to manage EMS COVID-19 patient disposition with physician consultation: A retrospective descriptive study by James Summers, Ian R Drennan, Linda Turner, Maud Huiskamp, W Scott Gorsline, Michael Merko and Morgan Hillier in Paramedicine
Footnotes
Declaration of conflicting interests
Author Ian Drennan is a member of the Editorial Board of Paramedicine. The author did not take part in the peer review or decision-making process for this submission and has no further conflicts to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Correction (October 2025):
In this article, “Declaration of conflicting interests” section has been updated.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.