
Abstract
Domestic and intimate partner violence are significant causes of mortality and morbidity worldwide. The act is usually serial in nature and tends to amplify in severity if not intervened. The first interaction a victim-survivor has with the healthcare system may be through a paramedic. Paramedics are opportunely placed for early violence intervention. Previous research sought to assess the impact of domestic and intimate partner violence education on healthcare professionals, primarily with in-hospital staff, however, there has been relatively minimal inquiry concerning paramedic education and practice. This study aimed to investigate evidence regarding domestic and intimate partner violence educational interventions for pre- and in-service paramedics. Additionally, we describe the nature and extent of interprofessional training and the relevant practice guidelines/policies for paramedic responses. A scoping review, utilising an a priori piloted search strategy (Medline via PubMed, Scopus, and EBSCOhost), was used to identify literature published from 2002 related to paramedic domestic and intimate partner violence interventions. Academic literature including research produced by organizations outside of conventional academic publishing were searched. A total of 1713 records were identified, and 36 were included for descriptive analysis. Major topic domains identified included teaching content and methods, professionalising best practices for public protection, intersectionality calls for interprofessional training, and the impact of educational interventions. With reports increasingly highlighting the potential role of the paramedic response to violence, there is a paucity of studies related to its improvement. Reported teaching strategies across multiple settings have some consistency. Though interventions may improve behaviour and actual/perceived knowledge and competence, there is no evidence suggesting an impact on victim-survivor experiences and outcomes. Interprofessional collaborations between out-of-hospital services, police, social workers, and in-hospital staff may be useful but remains underreported/underutilised. Future research should focus on domestic and intimate partner violence victim-survivor stakeholder engagement and intervention implementation.
Introduction
Domestic violence (DV) and intimate partner violence (IPV) are significant causes of mortality and morbidity worldwide. 1 IPV is defined as ‘behaviour within an intimate relationship (current or former) that causes, physical, sexual or psychological harm, including acts of physical aggression, sexual coercion, psychological abuse and controlling behaviours’. 2 DV is similarly defined however victim-survivors may include a child, other relatives, or any other household member. 3 Women are the most common victim-survivors of DV/IPV which is primarily perpetrated by men. 4 The act of DV/IPV is usually serial in nature and tends to amplify in severity if not intervened. 5
The first interaction a potential victim-survivor has with the healthcare system may be through a paramedic. 6 Globally, the majority of emergency medical services (EMSs) are historically positioned and currently primed to manage emergencies post facto. 7 Notwithstanding the contemporary literature on emerging extended roles and community paramedicine, 8 the traditional model of paramedicine does not typically encompass primary intervention (prevention) efforts in its ‘narrow’ ambit. It is thus essential that more sustainable solutions are investigated. Paramedics are positioned for early identification, treatment, documentation, education, and referral of victim-survivors. 7 The integration of these functions alongside contextual cues from the scene may enable the paramedic to become a significant role-player in a DV/IPV response. Despite this, there are limited data describing the pre- and in-service education and professional practice of paramedics regarding DV/IPV.
Previous studies including systematic reviews have sought to assess the impact of education on multiple healthcare professionals, notably physicians, nurses, social workers, and dentists. 9 However, there has been relatively minimal insight from the paramedic perspective. The World Health Organization (WHO) clinical and policy guidelines Responding to Intimate Partner Violence and Sexual Violence Against Women provide healthcare workers with much needed guidance. Unfortunately, the guideline and its supporting evidence are not fully representative of the paramedic or out-of-hospital context.2,10 The authors believe that there may be critical nuances between the in- and out-of-hospital DV/IPV response which are not being investigated.
Objectives
The aim of this scoping review was to investigate the existing international evidence of DV/IPV educational interventions for paramedics. The research question was ‘What DV/IPV educational interventions are currently in place for pre- and in-service paramedics responding in the out-of-hospital environment?’ The objectives were (1) to document DV/IPV training for paramedics, (2) to identify professional practices, protocols, and guidelines currently in place when managing out-of-hospital DV/IPV cases, and (3), to document how and to what extent interprofessional training is used in the DV/IPV education of paramedics.
Population: Consisted of ‘paramedics’ defined as any out-of-hospital non-physician healthcare provider with any educational level or experience.
11
Concept: Domestic violence educational materials including practice guidelines and operational policies. Context: ‘Out-of-hospital’ consisted of paramedic responses on-scene and/or during transport to hospital.
Language
The authors acknowledge that an individual's movement from victimhood to survivorship is not a linear process following DV/IPV. The term ‘victim’ is an accepted legal term for describing someone who has been adversely affected by a force or agent. 12 However, this term conveys connotations of powerlessness and weakness. Alternatively, the term ‘survivor’, often adopted by civil society, has more positive connotations related to strength, capability, and healing.13–15 Unfortunately, not all victims may survive DV/IPV. Furthermore, individuals may identify as ‘victim’ or ‘survivor’ depending on their perceptions of self-empowerment or secondary victimisation at a given time (i.e. their experience of the health or legal system). 16 In lieu of these binary representations and in the interest of inclusive practice, we adopt the hyphenated medico-legal term ‘victim-survivor’ to describe all individuals who have experienced violence.
Methods
We adhered to the updated scoping review methodological guidance from the Joanna Briggs Institute (JBI). 17 The uncontested protocol for this scoping review was published a priori through the Open Science Framework (https://osf.io/zcdtm/). 18 As an added measure to ensure the quality of this study, we consulted an editorial concerned with scoping review quality within the field of paramedicine. 19 The process and findings were reported in accordance with the PRISMA extension for scoping reviews. 20
Identification of relevant studies
With the assistance of a health sciences librarian (GM) at the University of Cape Town (UCT), a three-step search strategy was employed to identify all literature in a systematic and inclusive manner. 21 A search string was developed for each of the PCC elements using appropriate keywords, their synonyms, and MeSH (where relevant). The population (paramedic) element was informed by a validated filter which was optimised for sensitivity. 11 The search was conducted using Medline (via PubMed), Scopus, and EBSCOhost (Africa-Wide Information, CINAHL) databases. The search strategy was adapted for each database (Supplemental Appendix 1). The most recent search was executed on 31 January 2024.
Non-research evidence and grey literature from government and non-governmental organisations, conferences, and academic institutions were included. The open access dissertation databases from South African universities offering postgraduate courses in emergency care were searched for outputs relating to this topic. Additionally, outputs from international paramedic training institutions, workshops, and regulatory bodies were considered. Policy briefs from advisory institutions such as the WHO and the National Institute for Health and Care Excellence were also considered. The search strategy was completed through manual hand-searching of databases, article reference lists (snowballing), and editorials.
Study selection
Sources of evidence were not limited by study design. Publications outside of the DV/IPV, paramedic, out-of-hospital, and intervention/training discourse were excluded. Sources outside of the timeframe (before 1 January 2002), in languages other than English, or where the full text was not obtainable, were excluded. The timeframe limit was a pragmatic imposition to isolate more contemporary evidence on education and professional practice in the context of legislative maturity. Finally, sources simply highlighting the lack of DV/IPV-specific training for paramedics, without providing recommendations or without describing ongoing teaching practices, were excluded. Sources related to child abuse and sexual violence educational interventions were included if the study population consisted of paramedics.
After the removal of duplicates, an eligibility assessment was conducted independently by two reviewers (WC, NH) at the title and abstract level. Disputes were included in the next phase. Two reviewers (WC, NH) then assessed sources of evidence for inclusion based on the full manuscript, with any uncertainties or ambiguity handled by consensus (with NN and LA as arbiters).
Data charting and analysis
Data were extracted by the principal author (WC) into a novel a priori-designed extraction matrix on an Excel spreadsheet (Microsoft Corporation, Washington, United States). The matrix was piloted on the first 10 studies by two authors (WC, NH) independently. The matrix variables included bibliographic details of the full texts reviewed, study aims, country of origin, study population, methods, main findings, and sources of bias or potential limitations. The authors of the included sources of evidence were contacted for additional information if the review identified missing or poorly reported data. As is commensurate with scoping review methodology, notwithstanding heterogeneity, a formal risk of bias assessment was not performed. 20 The extracted data were descriptively analysed.
Ethics statement
This study was reviewed and approved by the UCT Human Research Ethics Committee (HREC REF: 708_2022).
Results
Search results
A total of 1721 records were identified through database searching. The first search was conducted on 14 October 2022 and yielded 1638 records for initial review. Due to delays in the research process, additional searches were conducted on 22 November 2023 and 31 January 2024 to incorporate the latest literature. These searches yielded an additional 83 records. After the removal of duplicates and titles, and after the abstract screening of a total of 1721 records, 57 full-texts were assessed for eligibility. Thirty-six sources of evidence were included for analysis (see Figure 1). The authors of the included sources of evidence were not contacted, as the review did not identify missing or poorly reported data.
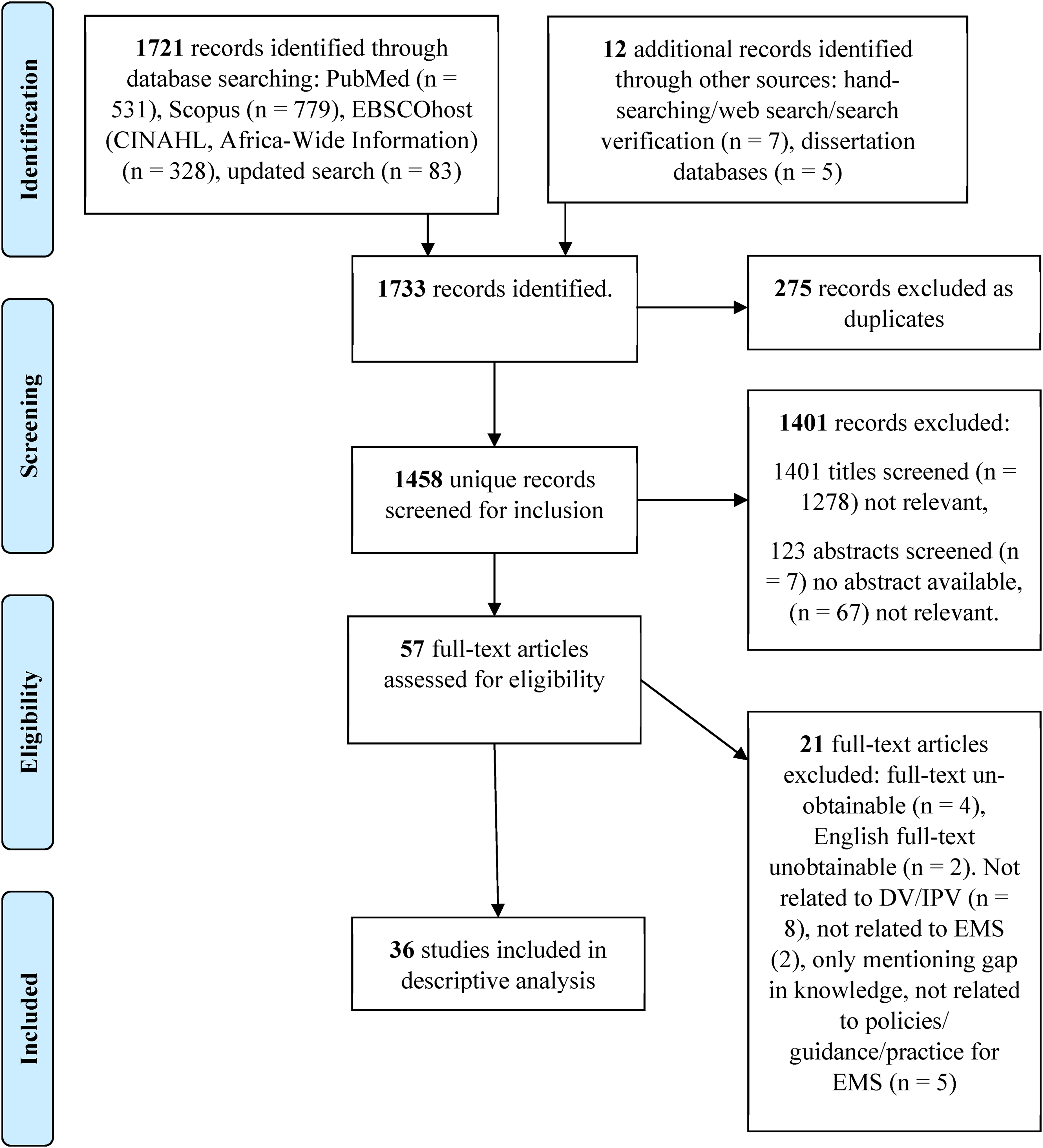
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) extension for scoping review flow diagram.
Study characteristics
The publication dates ranged between 2002 and 2022. The majority of the included sources originated from Australia (n = 12, 33%), South Africa (n = 10, 28%), and the United States of America (n = 9, 25%). Low- and middle-income countries were represented in (n = 11, 31%) of the included literature (ten originating from South Africa and one from India). Full study characteristics can be found in Supplemental Appendix 2. This appendix also indicates the main and additional topic domains noted for each of the included sources. The most common study design was cross-sectional survey (n = 8, 22%), followed by reviews of literature (n = 7, 19%) and mixed-method approaches (n = 5, 14%). A small number of sources spoke to paramedic-specific DV/IPV guidance (n = 4, 11%). There are no included sources published between 2003 and 2009. Most of the included sources were published after 2010 (n = 35, 97%) (see Figure 2, and Supplemental Appendix 2).
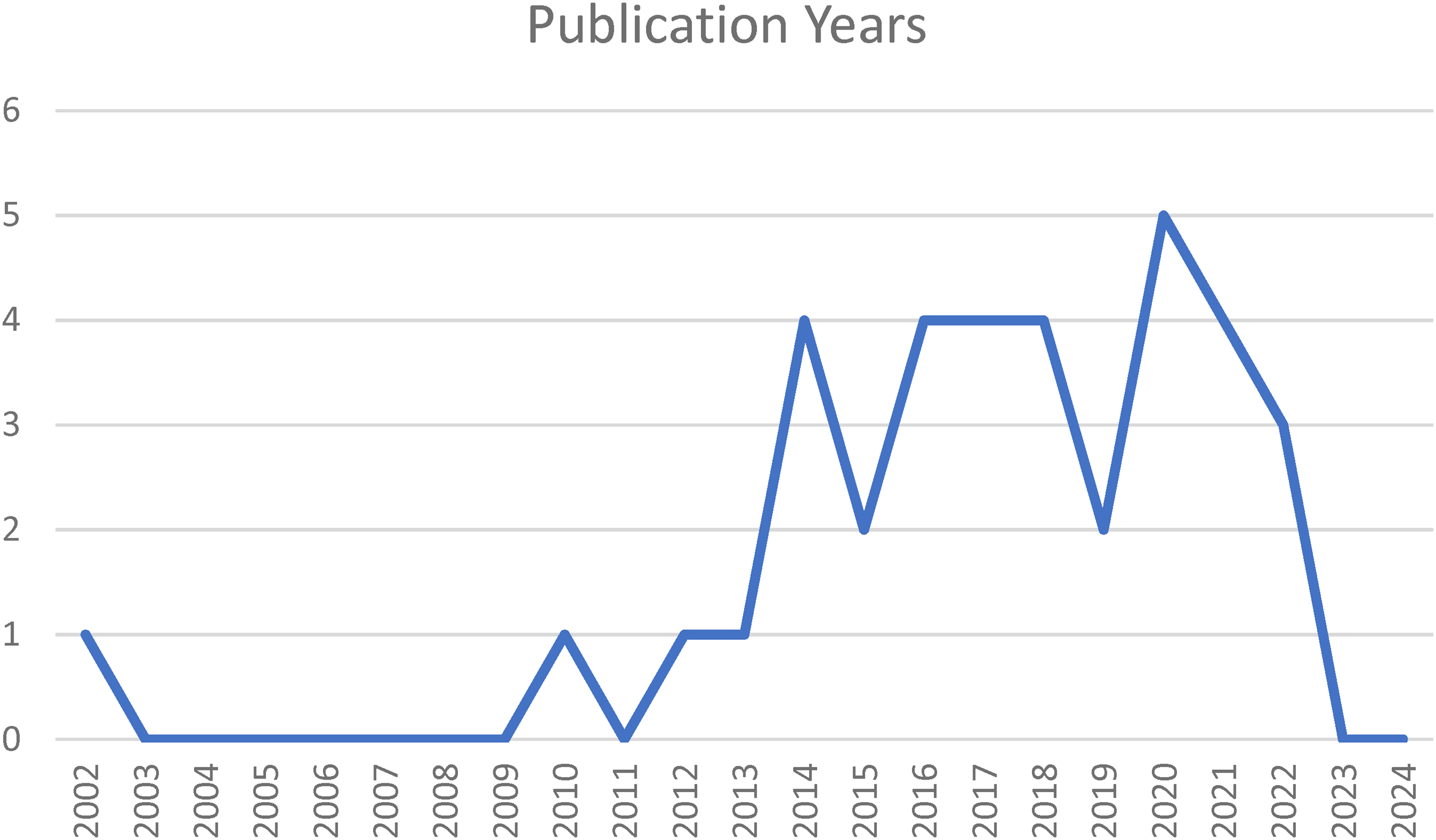
Publications by year.
Likely due to the research objectives and related search strategy, most sources included in this review speak to adult DV/IPV cases (n = 28, 78%), and the remainder spoke to child abuse cases. The discourses in most sources were aligned towards female victim-survivors and male perpetrators.
Four topic domains were derived after descriptive analysis: (1) DV/IPV teaching content and methods; (2) professionalising best practices for public protection; (3) DV/IPV intersectionality calls for interprofessional training, and (4) the impact of DV/IPV educational interventions. Supplemental Appendix 3 indicates the topic domains, sub-domains, and key messages identified during descriptive analysis of the included literature. A file indicating how the various sources contribute to the topic domains can be shared by the authors on request.
DV/IPV teaching content and methods
There was considerable overlap between the different sources regarding the teaching content that should be included in DV/IPV education for paramedics. Teaching content at the forefront of paramedic educational interventions were key definitions,9,22–25 relevant legislation,2,9,25,26 addressing of DV/IPV-related myths,24,27,28 victim-survivor referral,9,25,29,30 and documentation.9,22,24–26,31–33 Management of safety concerns (for both the paramedics and victim-survivors) was also a common teaching point.2,9,23,27,34 The concept of forensic evidence collection/preservation was mentioned, particularly within the context of sexual offences.2,9,24,25,33 Moving to broader competencies, the concepts of communication, interpersonal skills, and attitudes were mentioned in several sources.2,6,9,22 The details regarding these broader competencies were not routinely publicised, therefore the consistency between ongoing teaching could not be reported. From the included literature, relatively less emphasis was placed on victim-survivor safety planning,2,9 risk assessments and the potential for vicarious and direct traumatisation of paramedics.24,25 Defining of role definitions between paramedics and the other services available to victim-survivors (police, social workers, and in-hospital staff) was mentioned twice.22,31
Aside from medico-legal documentation, medical treatment, and reporting, emphasis is required on the essential skills of communication, empathy, and appropriate referral.2,9,22,25,35 Knowing how and when to speak to a victim-survivor presents a nuanced skill in communication.9,25,26 This includes knowing which information to provide and how to assess when it is safe to do so. 27 The included literature presented a need to redefine communication methods/techniques, provide opportunities for pre- and in-service paramedics to hone these skills, and find a way to robustly evaluate this learning.9,22,35,36
Data was mostly related to the pre-service context, particularly for undergraduate qualifications. Teaching methods varied substantially, there was, however, a common desire and shift towards multimodal learning.27,37 Teaching methods ranged from student-led, asynchronous online modules to the use of simulation training with standardised patients.9,22,31,34–38 Didactic lectures, victim-survivor stories, expert interviews, and clinical discussion focussing on the patient assessment were all examples of reported teaching strategies.9,31,39 Mentorship programmes between those experienced and skilled in DV/IPV responses and their colleagues were also recommended. 22
Although the importance of adequate training is universally stressed there is a risk that DV/IPV-specific content may be included in paramedic curricula as a token. The duration of the reported DV/IPV paramedic educational interventions was diverse, ranging from minutes to weeks. Lovi et al., 40 discovered through their investigation in Australia, that paramedicine programmes, including nursing and midwifery, may intentionally or unintentionally limit the coverage of IPV to a ‘couple of hours’. Some reasons for this were cited as curricula overcrowding, lack of prioritisation with more focus on the biomedical model of health, and the belief that the form of violence is not central to the role of the healthcare professional. 40
While there are multiple proposed teaching methods for the settings of both pre-and in-service education there is limited efficacy data to support one method over another. 41
The impact of DV/IPV educational interventions
Reported outcomes assessing the impact of DV/IPV educational interventions include changes in attitude, behaviour, and actual/perceived knowledge and competence. The heterogeneity of study designs, populations, training methods, and assessment made it challenging to compare interventions.
Sawyer et al. 42 sought to develop a new tool to measure the readiness of healthcare practitioners and students when encountering patients experiencing IPV. The 27-item scale, demonstrated a good reliability and validity when delivered to a cohort of Australian healthcare students. 42 The results of such a scale may also provide insight into the educational needs of those completing it.
Reported improvements to general learning and confidence were seen through the use of image-based cases of injury patterns, 43 standardised patients,35,37 and interactive, mixed-methods interventions. 9 Mackey found that increasing the length and ‘robustness’ of DV/IPV training may not necessarily translate into increased benefits when comparing a 2-h university module with a routine continuing professional education course. 41 There is some evidence to suggest that even after completing DV/IPV-specific training, paramedics still endorsed, or were neutral, when asked about common negative stereotypes associated with DV/IPV.27,28 There is consistency found here, as Edlin et al. 44 report that even with improvements to knowledge levels, there is still evidence suggesting that this does not immediately translate to the screening and reporting ability of professionals following training. This discrepancy in learning was further highlighted by Sawyer et al., 32 noting that even when they controlled for any potential confounders (age, gender, year of study, and lifetime IPV experience), previous training was significantly associated with higher ‘perceived’ knowledge but not ‘actual’ knowledge. Regarding behaviour changes, in South Africa, Naidoo et al. 6 determined that DV screening training could improve the paramedic detection rate of domestic violence three-fold, with the most stringent assumptions, and nine-fold if widespread mandatory adoption of practice policy occurred. This data subsequently highlighted a paramedic missed detection rate of 42.8 per 1000 patients (for female patients, 14 years and older). A ‘Risk-Need-Responsivity’ practice model was proposed. 6
Professionalising best practice for public protection
The lack of clear policies was found to be a key challenge in implementing successful DV/IPV interventions in low- and middle-income country (LMIC) healthcare systems. In settings where policies, protocols, and procedures are clear and integrated, services for DV/IPV victim-survivors have become an effective part of routine healthcare. 29 For EMSs without DV/IPV guidelines, Artz et al. 29 highlighted that healthcare professional guidance, screening tools, risk assessment, and safety planning guidelines already exist, and these can be easily adopted and reconfigured to suit the needs of the given organisation. Ideal guidelines should (1) be as brief as possible, (2) be based on the paramedic’s observations, (3) be easily incorporated into their existing standard operating procedures and (4) provide them with guidance when reporting. 45 In 2013, the Health Professions Council of South Africa Professional Board for Emergency Care, a regulatory body, released a DV-screening protocol for paramedics, 46 based on Naidoo's et al. 7 research translation. These guidelines outlined the importance of biopsychosocial care, screening, and risk assessments. Unfortunately, the uptake of this protocol by registered professionals obligated to do so was minimal, 47 with no evidence suggesting implementation through public and private EMSs or training institutions. 35 Naidoo et al. 6 argued that it would be unreasonable to expect practitioners to implement a clinical guideline that they have never been trained on.
In Australia, Sawyer et al. 48 sought to address the unsolved need for paramedic DV/IPV guidance by using current evidence and recommendations from various health agencies finalised through consensus methods. This guideline was significantly informed by the WHO clinical and policy guidelines Responding to Intimate Partner Violence and Sexual Violence against Women. 2 The produced guideline has four sections titled ‘recognise’, ‘respond’, ‘refer’, and ‘record’; outlining the major actions to be performed when managing potential DV/IPV cases. 48
DV/IPV intersectionality calls for interprofessional training
Only two sources spoke directly to interprofessional training.31,33 Johnson et al. 31 referred to the development of three interprofessional educational modules based on trauma-across-the-lifespan. Participants in these modules included students of dentistry, paramedicine, nursing, occupational therapy and pharmacy amongst others. The programme was reported to be largely positive with most students valuing the overall learning experience and the opportunity to interact with other disciplines. 31 Additionally, Pelucio et al., 33 sought to develop an interagency approach to non-fatal strangulation. Here investigators co-developed training tools, forensic documentation, and referral processes between the sectors of law enforcement, EMS, emergency department staff, forensic nursing teams, and prosecuting attorneys. The team was successful in improving both the rate of forensic nurse examinations for non-fatal strangulation and police arrests for felony assault by strangulation within their county. Unfortunately, the investigators could not assess the programmes impact on successful prosecutions, 33 yet it can be assumed that improved forensic documentation can improve the chances of successful prosecutions.2,49
Additionally, while not specifically an educational intervention, there was support for the paramedic collaboration with other specialty services. 22 Through consistent and accurate completion of medico-legal documentation, valuable information may be relayed to investigative staff (social workers and police) narrowing the knowledge gap between services. 22 In the same light, value may also be found in having paramedics serve on interdisciplinary femicide/child death review boards. 22
Discussion
The findings of this review provide a foundation for further research on the paramedic approach to DV/IPV, the development of training methods, and the initiation of practice policy development where gaps currently exist.
The advancement of multimodal learning, environments that allow instructional elements to be presented through more than one sensory mode (visual, aural, and written), 50 was pronounced in this review.6,22,27,32,34,35,37,38,41,51 The pedagogy of multimodal learning shifts the emphasis from the delivery of instruction to methods that, in a more participatory manner, engage the student in ways that best suit their learning styles, strengths, and practice potential.52,53 By doing this, students are exposed to experiences otherwise unavailable in standard didactic education, focussing on reflection, communication, action, and response. 54 This approach is justified since it is known that a range of educational, linguistic, and socio-cultural factors affect the likelihood that healthcare professionals will discuss potentially sensitive topics with their patients. 30 Multimodal learning requires intensive consideration through content development and assessment of student preferences, ultimately favouring programmes with greater resources and time allowances for content delivery.
Given the reported teaching methods and content, the findings from Lovi et al. 40 describe the potentially token inclusion of DV/IPV training in paramedic curricula. Notwithstanding the limited transferability of these results to other programmes, the risk of this phenomenon is still very probable. A study investigating tokenistic DV teaching at UK-based medical schools cited ‘lack of time’, ‘the perception that DV is not a medical problem’, and ‘the assumption that the knowledge can be learnt elsewhere’ as potential reasons. 55 The observed lack of training institution accountability combined with healthcare provider discomfort in handling DV/IPV cases underscores a significant disparity between ongoing medical education and the needs of healthcare workers.
Victim-survivors may be hesitant to disclose violence due to its repetitive, retaliative, and psychologically harmful nature.56,57 This coupled with healthcare professionals’ reluctance to screen patients highlights a need for guidelines and training on questioning practices. 29 This is particularly crucial when investigating non-fatal strangulation 33 Alone, this form of violence is associated with greater than seven-fold odds (OR 7.48, 95% CI: 4.52–12.35) of becoming a completed homicide. 58 Critically, only about 50% of non-fatal strangulation victim-survivors present with visible physical injuries. 59 Universal screening and education entails the screening of all patients regardless of the healthcare professionals’ suspicions. 60 While this reduces the number of missed cases and normalises the conversation, 60 it is not recommended by WHO due to limited evidence indicating reductions in violence reoccurrence. 2 Additionally, victim-survivor trust may be eroded where there are limited referral options. 2 The caveat is that none of the evidence underpinning that position includes out-of-hospital research. Alternatively, the WHO recommends selective screening, enquiring about violence when assessing patient conditions that may be caused or complicated by DV/IPV (e.g. depression, substance use, unexplained medical, or traumatic complaints).2,61 Sprague et al. 62 and Naidoo et al.6,7 argued that the emergency care patient cohort is already at higher probability of experiencing DV/IPV than the general population, making screening both selective and universal in nature.
Through empathetic questioning, paramedics can counter the professional indifference, and hesitancy to intervene that is commonly associated with DV/IPV. 60 A change in paramedic reporting of DV was found through the training and use of a screening tool in South Africa. 6 Unfortunately, in this study setting, there is no evidence that the tool, nor training, were adopted after the research efforts. Nonetheless, this observed change in paramedic behaviour is promising and suggests that the industry is merely waiting for policy development, proactive implementation, and compliance monitoring. Due to the nascency of the Australian guideline developed by Sawyer et al., 48 we are unable to report the extent of adherence and overall impact. Though outcome data is lacking, this evidence-based guideline should be embraced by EMSs as it offers the opportunity for local modification to meet contextual requirements. 48
An unsupported rationale for the limited development/uptake of DV/IPV guidance is the assertion that paramedics are too encumbered with the prevailing life-threatening emergencies to manage DV/IPV-related cases appropriately.6,47 This notion comes into direct scrutiny with a finding from the Western Cape Province in South Africa, well-renowned for its high trauma burden. 63 Binks et al. 64 found that of all patients transferred to the hospital via ambulance (between October 2018 and September 2019), 82% (n = 199,062) received no medical treatment. Additionally, of all patients seen to by paramedics and not transported to the hospital, 84% (n = 4388) also did not receive any medical treatment. While the findings may not be immediately generalisable to other settings, they do speak to the latent capacity within a typical paramedic response for meaningful DV/IPV interventions, little of which calls for medical care through the biomedical health model. 65 Useful DV/IPV interventions appear to be centred on more holistic approaches, potentially actionable through pre- and in-service interprofessional training. Collaborations between paramedics, police, social workers, and in-hospital healthcare workers can highlight the specific function of each stakeholder, a current knowledge gap within most systems.22,25,31,45 At present there are no well-described systems of paramedic referral pathways for DV/IPV victim-survivors; interprofessional collaboration can be leveraged here.24,33
The overlapping forms of oppression faced by victim-survivors of DV/IPV relate to intersectionality. 66 This phenomenon refers to the synergism between gender, race, ethnicity, language, sexuality, education, culture, and the societal bias to each, in creating barriers to care. When evaluating paramedic attitudes to DV/IPV, post-intervention improvements are noted however some sources state that participants may still hold false beliefs and negative stereotypes despite the focused training.6,27 Attitudes are not cemented, and modifications may be seen through training. There is an argument to be made that confidence and perceived knowledge of DV/IPV are just as important as actual knowledge, as these are the factors driving paramedics to act based on their suspicions or a disclosure of DV/IPV.
Although the literature highlights key interventions to be performed by paramedics, there is limited evidence describing what will make paramedics competent in performing these functions. Competency-based health professions education is, broadly, a framework for preparing health professionals for future practice. 67 It includes the practice standards that articulate the knowledge, skills, attitudes, and capabilities of a profession.67–69 One of the strengths of this approach is through the inclusion of relevant and diverse stakeholders (patients, end-users (paramedics), and policymakers) during programme development. Unfortunately, there is no evidence indicating causation, or even association, between DV/IPV training of paramedics and victim-survivor health outcomes. At present, we can only assume that the improvement of educational outcomes (knowledge, competence, practice readiness) are helpful for victim-survivors and negates the learnt helplessness among providers of care.
Limitations
This scoping review has some limitations. While efforts were made to include globally published literature from three databases, grey literature, and theses/dissertations from South African universities offering postgraduate programmes in emergency care it is possible that relevant sources were missed. Attempts at searching international theses repositories (NDLTD Global ETD and Open Access Theses and Dissertations) resulted in inconsistent results with several omissions from multiple countries. South African theses repositories were then searched for pragmatic reasons, what with the countries femicide rate being five times the global average. 70 Although the search has no restrictions on study origin, the exclusion of all non-English works is a notable limitation. A diverse range of studies were included, and a formal risk of bias assessment was not performed. Readers should be aware that this may have adversely affected the reliability and validity of the finding interpretations.
Conclusion
In the presence of reports suggesting the role of paramedics in DV/IPV cases, there is a paucity of studies related to its development. Reported teaching content and methodologies appear consistent between different settings. There are data indicating that educational interventions can improve paramedic confidence, behaviour, competence, and knowledge, but we are unsure of its overall impact on the well-being of the victim-survivor. Future studies should evaluate victim-survivor perspectives on paramedic interventions to promote the theme of victim-centred care within education and practice policy. The review revealed significant gaps in knowledge regarding intentional interprofessional collaboration. The value may be found here through outlining role definitions and by sharing information and knowledge between sectors. An intentional and comprehensive design in paramedic education and professional practice may significantly influence a victim-survivor journey to health and justice.
Supplemental Material
sj-pdf-1-pam-10.1177_27536386241265416 - Supplemental material for Paramedic educational interventions for out-of-hospital domestic and intimate partner violence cases: A scoping review
Supplemental material, sj-pdf-1-pam-10.1177_27536386241265416 for Paramedic educational interventions for out-of-hospital domestic and intimate partner violence cases: A scoping review by Wesley Craig, Natalie Hartnady, Navindhra Naidoo, Lorna J Martin and Lillian Artz in Paramedicine
Supplemental Material
sj-docx-2-pam-10.1177_27536386241265416 - Supplemental material for Paramedic educational interventions for out-of-hospital domestic and intimate partner violence cases: A scoping review
Supplemental material, sj-docx-2-pam-10.1177_27536386241265416 for Paramedic educational interventions for out-of-hospital domestic and intimate partner violence cases: A scoping review by Wesley Craig, Natalie Hartnady, Navindhra Naidoo, Lorna J Martin and Lillian Artz in Paramedicine
Supplemental Material
sj-docx-3-pam-10.1177_27536386241265416 - Supplemental material for Paramedic educational interventions for out-of-hospital domestic and intimate partner violence cases: A scoping review
Supplemental material, sj-docx-3-pam-10.1177_27536386241265416 for Paramedic educational interventions for out-of-hospital domestic and intimate partner violence cases: A scoping review by Wesley Craig, Natalie Hartnady, Navindhra Naidoo, Lorna J Martin and Lillian Artz in Paramedicine
Supplemental Material
sj-docx-4-pam-10.1177_27536386241265416 - Supplemental material for Paramedic educational interventions for out-of-hospital domestic and intimate partner violence cases: A scoping review
Supplemental material, sj-docx-4-pam-10.1177_27536386241265416 for Paramedic educational interventions for out-of-hospital domestic and intimate partner violence cases: A scoping review by Wesley Craig, Natalie Hartnady, Navindhra Naidoo, Lorna J Martin and Lillian Artz in Paramedicine
Footnotes
Acknowledgements
The authors are thankful to Gill Morgan, a UCT health sciences librarian, who kindly gave her time to this project.
Authors contributions
Authors contributed to the conception and design of the work (WC, NN, LA); the acquisition (WC, NH), analysis or interpretation of data (WC, NH, NN); and drafting the manuscript or revising it critically for important intellectual content (WC, NN, LJM, LA). All authors approved the version to be published and agreed to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Navindhra Naidoo is an associate editor of Paramedicine. The authors have no other competing interests to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.