
Abstract
A key component to the continued development of any profession is a strong research culture. For paramedicine, a research culture that acknowledges the uniqueness of the out-of-hospital setting allows clinical practice to develop. Recent international publications investigating paramedicine research outputs demonstrated that Ireland was not strongly represented in the production of paramedicine-based research. The aim of this scoping review was to identify and evaluate the quantity and quality of the research published to date in the Irish out-of-hospital literature, and to identify research gaps that may need to be addressed. A scoping review was conducted using the Joanna Briggs Institute guidance. All studies that reported on out-of-hospital care in the Republic of Ireland were included. MEDLINE, CINAHL, EMBASE, Cochrane Library, and grey literature sources were searched from 2000 until 2022 for relevant articles in March 2023. Key authors were contacted to identify missing articles and data were extracted to present the final publication yield. Scientific quality was assessed using Clarivate Average Journal Impact Factor Percentiles. Over 3200 research outputs were identified from the databases with a final yield of 294 research outputs included in this review. Research outputs were identified for most years included in the review period, with outputs published in a large range of journals. Research heavily focused on areas linked to the Clinical Practice Guidelines, and predominantly used quantitative data collection methods. Most authors identified in this review were named on only one output. However, diversification in research topics and methodologies, a concerted effort to ensure practitioners are leading research and support to ensure that conference presentations are continued to peer-reviewed publication would strengthen this resolve.
Introduction
Health services benefit from integrating research findings through an overall improvement in the quality of patient care. 1 To produce such evidence, health services need to support a strong research culture and invest in increased research capacity to improve outcomes for service users and professionals. 1 Research culture relates to the research environment, including how organisations value research, as indicated by factors such as leadership, resources, technologies and incentives. Research capacity building is defined as a process of developing sustainable abilities and skills enabling organisations and individuals to perform high-quality research. 2 This capacity within the workforce can facilitate knowledge translation to close the gap between theory and practice. 3
The out-of-hospital setting is a challenging environment for research, particularly related to limited resources and infrastructure, participant recruitment, and protocol deviation. 4 Consequently, research capacity and research culture in out-of-hospital care internationally remain underdeveloped.5,6 Paramedicine as a profession also historically relies on ‘heirloom knowledge’ (passed down from one generation to the next) or on evidence generated by other health professions. 7 Paramedic education was traditionally vocational ‘on the road’ training which had a limited focus on academic and research skills. 8 However, many international jurisdictions have evolved to higher education models, and paramedics are now more engaged with research and scholarly contributions.5,8,9 For example, 242 paramedics have registered their doctorate degree with the international paramedic PhD registry as of January 2024. 10 However, in addition to other knowledge translation strategies, it is acknowledged that the translation of research into peer-reviewed publications and conference presentations is of great importance to the continued professionalisation of paramedicine. 11
The Irish out-of-hospital context
In Ireland, out-of-hospital care is predominantly provided by Pre-Hospital Emergency Care Council (PHECC) registered practitioners who practice autonomously, with support from other health professionals. Public ambulance services are primarily delivered by the National Ambulance Service, and Dublin Fire Brigade with additional support from auxiliary, private, and voluntary providers of out-of-hospital care. Out-of-hospital care has progressed significantly in Ireland over the past two decades, as evidenced by the regulation of practitioners, the publication of national evidence-based clinical guidelines, and the emerging professionalisation of paramedicine.12,13 For the purposes of this manuscript, when we use the term ‘paramedicine’ we are referring in the Irish context to the overall profession. When we use the term ‘practitioners’ we are referring in the Irish context to the individual PHECC registered practitioners, which include emergency medical technician, paramedic, advanced paramedic, and specialist paramedic. Although definitions of out-of-hospital care vary in the literature, we use the term ‘out-of-hospital’ in this manuscript to encompass all aspects of pre-hospital emergency care and community clinical care provided by practitioners and other health professionals (e.g., physicians and nurses who provide clinical care in support of practitioners and ambulance services), and related non-clinical aspects of paramedicine such as education, professionalisation, and leadership.
The establishment of the statutory regulator, PHECC in the year 2000 marked an important milestone in the professionalisation of Irish out-of-hospital care. One of the strategic priorities of PHECC is to support research in out-of-hospital care. As such, to guide and inform research capacity building, in 2008 a National Prehospital Research Strategy was published, 14 which was highly innovative at the time as national-level out-of-hospital research agendas were rare internationally. 15 Another important milestone was reached in 2016 with the graduation of the first degree-educated paramedics in Ireland. 16 This education has extended to postgraduate level research training with many masters degrees conferred, and six doctorates from Ireland registered on the paramedic PhD registry (four graduates and two current PhD candidates). 10 Although these measures are important for the profession, ensuring that the research completed in Ireland is disseminated to policymakers, stakeholders, education institutions, and clinicians is a vital step to improve research culture and ultimately result in translation to impact patient-oriented health service outcomes. This includes the need to disseminate these findings in publications that are used as sources of evidence for policymakers and decision-makers. 17 This is proving a challenge for Ireland. For example, in two recent investigations of bibliometrics and research outputs in paramedicine, Ireland was not a place of origin for any work in the top 100 most cited paramedicine papers, nor named in the top 10 countries for publications.5,11 This suggests a lack of a research culture and measurable outputs, but also a potential opportunity to improve the culture and therefore better inform policy and service design and implementation.
Therefore, the primary aim of this scoping review was to map and identify characteristics of the evidence published to date in the Irish out-of-hospital literature. A secondary aim was to inform future needs for out-of-hospital care research in Ireland.
Methods
We conducted a scoping review using the methods outlined by the Joanna Briggs Institute (JBI). 18 A scoping review was considered the most appropriate methodology for this review as we sought to identify key characteristics of out-of-hospital publications, and we wished to draw upon data from any source of evidence and research methodology. 19 Informed by a recent publication 11 that identified minimal peer-reviewed journal publications from Ireland, engaging stakeholders was considered essential to identify emerging and unpublished research. We utilised the PRISMA extension for scoping reviews (PRISMA-ScR) checklist (Appendix A) and explanations in reporting this review. 20 A literature search for studies that investigated out-of-hospital care in Ireland was performed, and the JBI scoping review methodological framework was applied to facilitate the identification of gaps and methodological deficiencies in the existing literature. The protocol was registered on the Open Science Framework for transparency (https://osf.io/n6zf7/) in February 2022.
Inclusion and exclusion criteria
We utilised the Population, Concept, Context (PCC) Framework to draft the search strategy for the scoping review in consultation with the project sponsor, PHECC. The key areas of the framework were: Population – All patient populations; Concept – Out-of-hospital research (encompassing all aspects of pre-hospital emergency care and community-based out-of-hospital care provided by practitioners and other health professionals (e.g., physicians and nurses who provide out-of-hospital care in support of practitioners), and non-clinical aspects of paramedicine such as education, professionalisation, and leadership); Context – Ireland (based on Irish data, or related to the Irish out-of-hospital system). All studies that reported on out-of-hospital care in the Republic of Ireland were included, in line with the PCC explanation above. Where a study was reported in more than one form (e.g., a peer-reviewed article and a conference abstract), all forms were included to acknowledge the multi-faceted nature of knowledge translation.
Studies were excluded if they were not related to out-of-hospital emergency care (such as in-hospital studies), or not conducted in or including data from Ireland. Research that was completed by an Irish researcher relating exclusively to out-of-hospital care in another jurisdiction was not included (e.g., an Irish author working in and publishing about out-of-hospital care in Australia or Canada). Outputs based on European-wide registry data that included Irish data AND had an author from Ireland involved were included. Studies that were written in languages other than English were included; however, the interpretation of the context of the research may be limited. All patient age groups were included as were all research designs/sources (e.g., randomised control trials, systematic reviews, case studies, quasi-experimental studies, mixed-methods studies, clinical guidelines, qualitative studies, audits, or quality assessment reports). Scholarly pieces that did not have a research component (i.e., opinion pieces or commentaries) were excluded.
Search strategy and information sources
For this study, we developed a search strategy and searched electronic databases MEDLINE, CINAHL, EMBASE, Cochrane Library, and Google Scholar from 2000 until 2022 for relevant articles in March 2023. The start date of 2000 was in line with the establishment of PHECC. The search strategy was peer-reviewed by an information specialist to ensure accuracy and sensitivity. The search strategy was iteratively edited to ensure sensitivity based on their review and expertise. Subject headings were used where appropriate, and keywords and subject headings were adapted as required for individual databases. A previously developed search strategy 21 modified to the parameters of this study was employed. Identified journals in Ireland that are not indexed were also searched. Key stakeholders were included in this developmental stage. Stakeholders reviewed the search terms to ensure they were inclusive and were encouraged to suggest any terms we may have missed. When no additional terms were suggested by the team, the information scientist, or the key stakeholders, we considered this to represent saturation. Stakeholder engagement at this early stage also allowed for knowledge exchange throughout the scoping review process. 22 The base search strategy used in OVID Medline was as follows with truncations and Boolean operator included (subject headings were not used in this database as none were deemed appropriate for the search strategy):
Ambulances OR Emergency Medical Technicians OR Air Ambulances OR emergency medical services OR paramedic* OR ems OR emt OR prehospital OR pre-hospital OR first responder* OR emergency medical technicians OR emergency services OR Ambulance* OR HEMS OR field triage OR out-of-hospital
AND
Irish OR Ireland OR ‘PHECC’ OR ‘National Ambulance Service’ OR ‘Dublin Fire Brigade’ OR ‘OHCAR’ OR ‘Pre-Hospital Emergency Care Council’.
The database search was supplemented by examining published conference abstracts from relevant conferences held in Ireland (identified by the research team, sponsor, and expert stakeholders), and contacting experts in the field to identify difficult-to-locate or unpublished material. We also searched for grey literature in Google Scholar, Google, TROVE, national health websites (PHECC, Health Service Executive, Dublin Fire Brigade, Lenus, OHCAR Registry), and health professional and scientific associations’ websites (Irish College of Paramedics, Irish College of General Practitioners). We screened the first 300 results for both Google Scholar and Google. 23
All search results were imported into Covidence systematic review management software 24 where duplicates were removed. Each title and abstract were screened independently by two reviewers for inclusion using the eligibility criteria (Level 1 screening). This was followed by an independent full-text review of potentially relevant articles by two reviewers to determine inclusion using the same eligibility criteria (Level 2 screening). Conflicts were resolved by discussion or involvement of a third reviewer. Once the final listing of publications was established, the citation lists of each included article were checked via citation chaser. 25 This process collated all reference lists of included articles (backward citation chasing) as well as future publications that cited the included articles (forward citation chasing). The titles of all articles in this list were also screened to ensure potential work was not missed.
Stakeholder consultation
Authors who had five or more research outputs as the first or senior (i.e., last) author in the review were consulted. Authors were provided with the inclusion and exclusion criteria of the scoping review and were asked to assess their personal list of included outputs and to suggest items that were in-progress or missing from the list.
Extraction of results
A data extraction table based on the key output characteristics was developed by the research team in Covidence. Iterative updates to the extraction form took place until the research team reached a consensus on the final form. General study characteristics extracted included the following variables: authorship, year of publication, type of output (i.e., peer-reviewed publication, conference proceeding, or grey literature), journal or venue of publication, study design, and area of research.
Summary and analysis
We performed high-level quantitative and qualitative analyses. The quantitative analysis comprised simple frequency counts of study characteristics and the Average Journal Impact Factor (JIF) Percentile at the year of publication. Further summative analysis was completed on overall counts for each listed author. The results are presented in narrative and graphical form. We performed a high-level descriptive qualitative content analysis of the area of research. These findings were grouped deductively in line with the PHECC 2021 Clinical Practice Guidelines where applicable, 13 and inductively via basic level coding of the main focus of the output.
Scientific quality analysis
We determined the scientific quality of the peer-reviewed research outputs by assessing the Average JIF Percentile through Clarivate, as this is deemed a more meaningful approach to allow cross-category comparison, compared with category-based journal quartiles. 26 As targeted journals in the area of out-of-hospital research are considered in a diverse range of categories, and many journals are considered in more than one category, this was deemed the most appropriate measure to represent scientific quality in this review. Within the Clarivate system, the Average Journal Impact Factor Percentile takes the sum of the JIF percentile ranks for each category under consideration for that journal and then calculates the average of those values. This percentile was matched for the journal name and the year of publication for each included output and with the ‘All categories average’ extracted.
Ethics approval
As this research is a scoping review of published works, no ethical approval was required.
Results
The combined database searches resulted in a yield of 3202 publications. Once duplicates were removed, 2801 publications underwent title and abstract screening. A total of 2633 publications were removed in-line with the predetermined exclusion criteria and 166 publications were available for full-text review. The main reason for exclusion at the full text review level was the research that was not completed in the out-of-hospital setting. This review process resulted in 137 outputs for inclusion. Citation chasing of the included outputs, along with searches of grey literature added an additional 157 research outputs. This resulted in 294 research outputs meeting the inclusion criteria for this review as outlined in Figure 1.
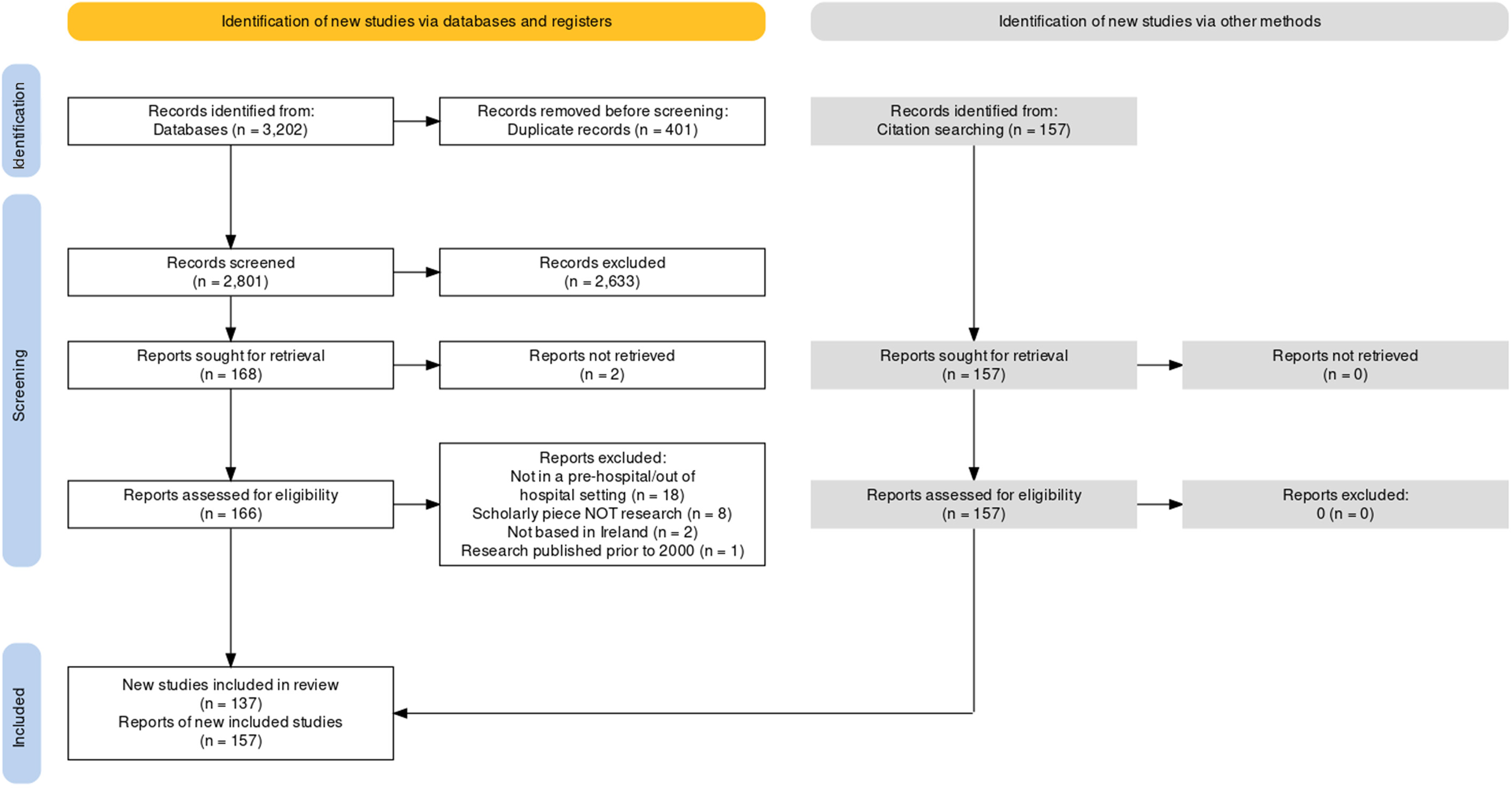
PRISMA flowchart of included publications.
Publication characteristics
All included outputs were published in English. Outputs were identified from 2000 to 2022. Overall, there were 123 conference/symposia abstracts, 160 peer-reviewed journal articles, and 11 grey-literature outputs published. Figure 2 quantifies the output numbers per year and illustrates the type of output. Prior to 2012, less than 10 relevant peer-reviewed publications were published most years; however, this number nearly doubled for most years from 2012 onwards. The year 2013 produced the most research outputs overall (n = 37), while the year 2016 produced the largest number of peer-reviewed publications (n = 20).
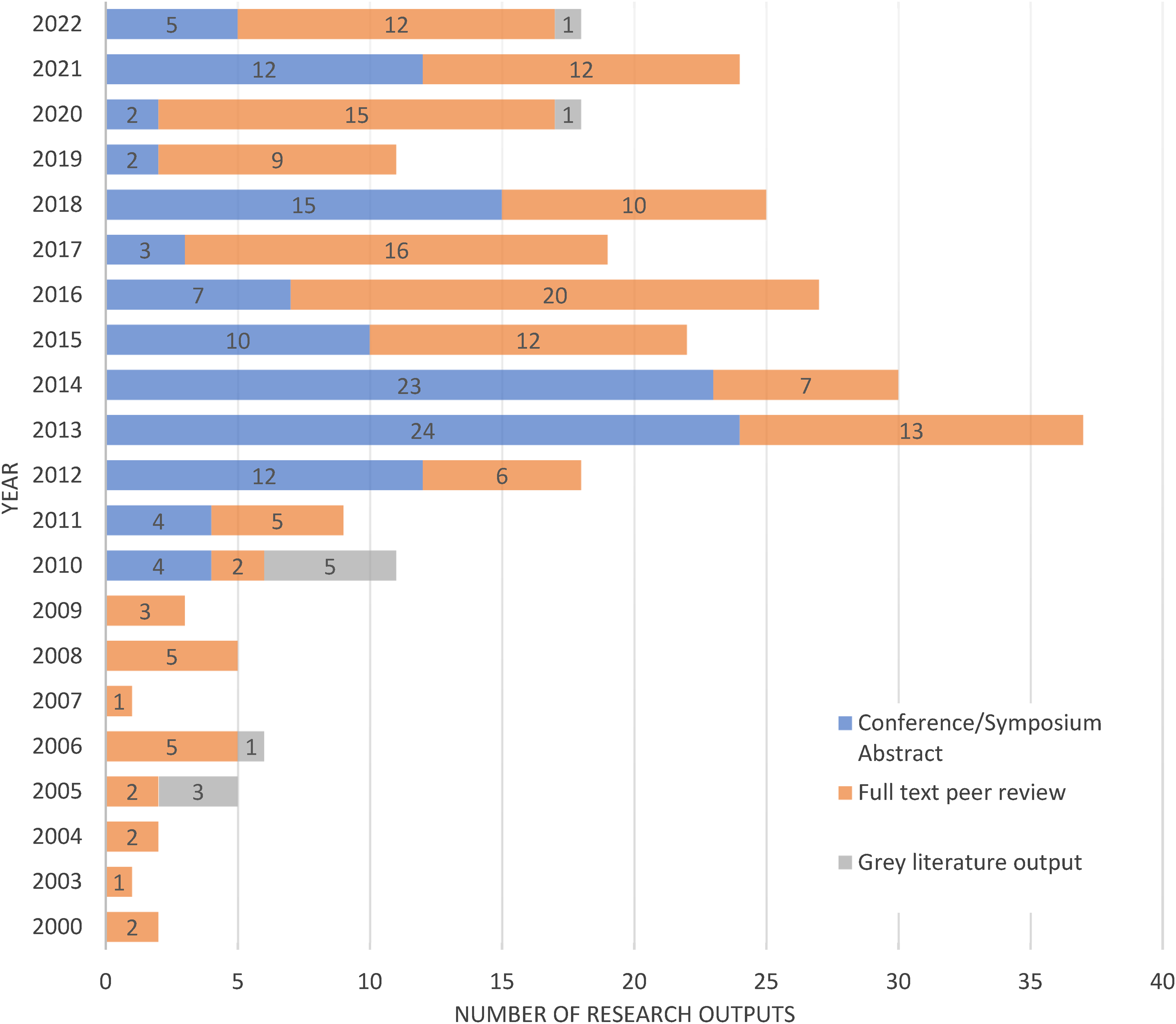
Publication outputs per year over the review time period.
Figure 3 illustrates the journals in which included peer-reviewed outputs were published. Over the period of this review, 203 of the 294 research outputs (peer-reviewed articles and conference abstracts) were published in 58 different journals. The remaining conference abstracts were made available in books of abstracts but not published in journals. For ease of interpretation, journals that included less than five research outputs over the time period were combined into an ‘other’ category. The journal name was coded to chart by the type of research output. Several conferences and symposia publish their abstracts in supplementary editions of journals as evidenced in Figure 3. The top three journals for included outputs were ‘Resuscitation’, the ‘Irish Journal of Medical Science’ and the ‘Irish Journal of Paramedicine’. These three journals include conference abstracts, and if counting peer-reviewed article publications alone, the ‘Emergency Medicine Journal’ is the second most utilised journal.
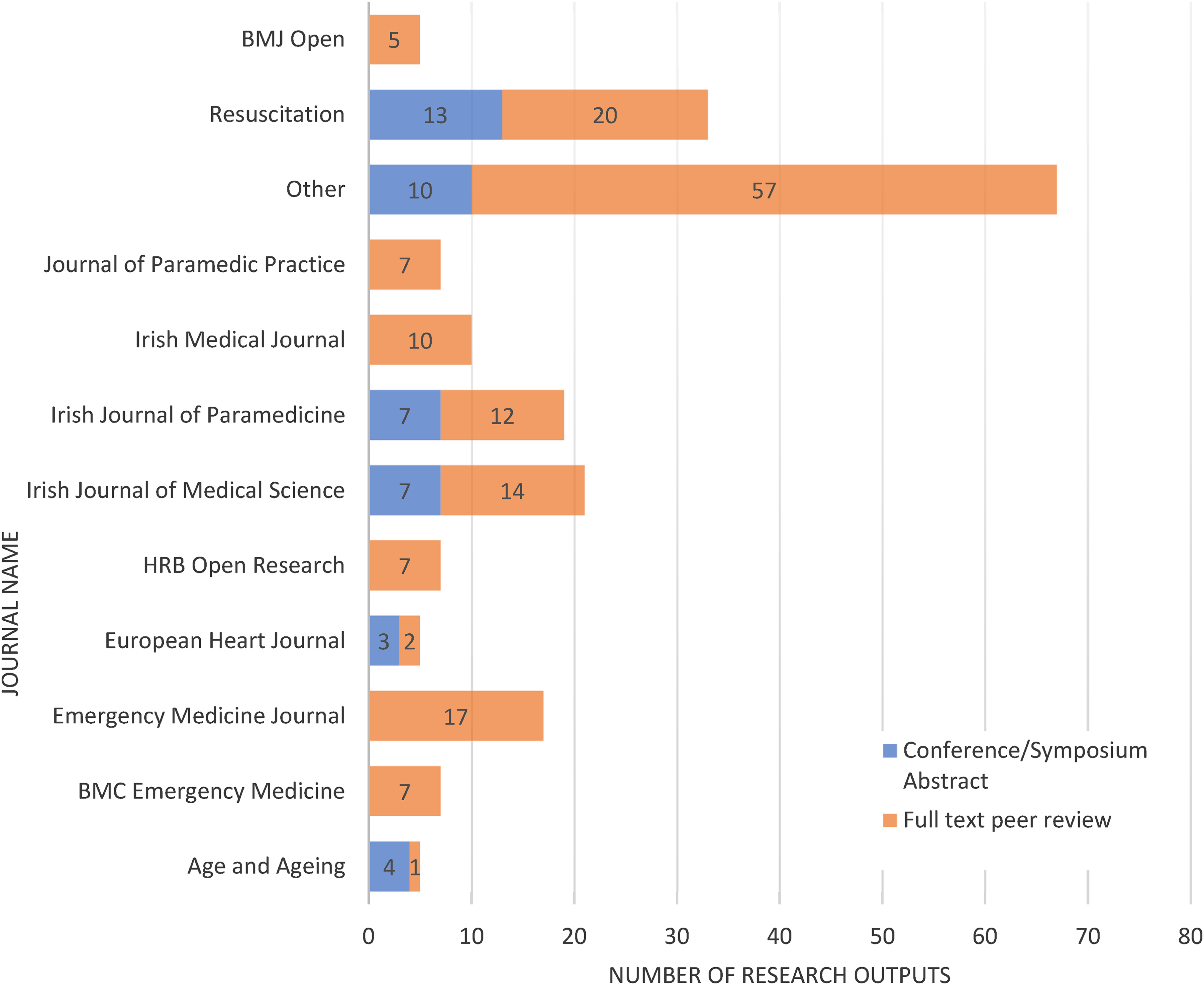
Publication outputs per journal over the review time period.
Of the 203 research outputs that were published in a journal, 118 were published in journals that had a JIF Percentile in Clarivate. The remainder were published in journals that are not contained within the Clarivate database. As outlined in Figure 4, the Average JIF Percentile of outputs included in this review was skewed towards the higher percentiles, indicating the high quality of journals in which the work is published. We were unable to accurately calculate how many conference abstracts were followed through to publication given challenges raised by differing titles, multiple presentations, author teams, and abstract content changes.
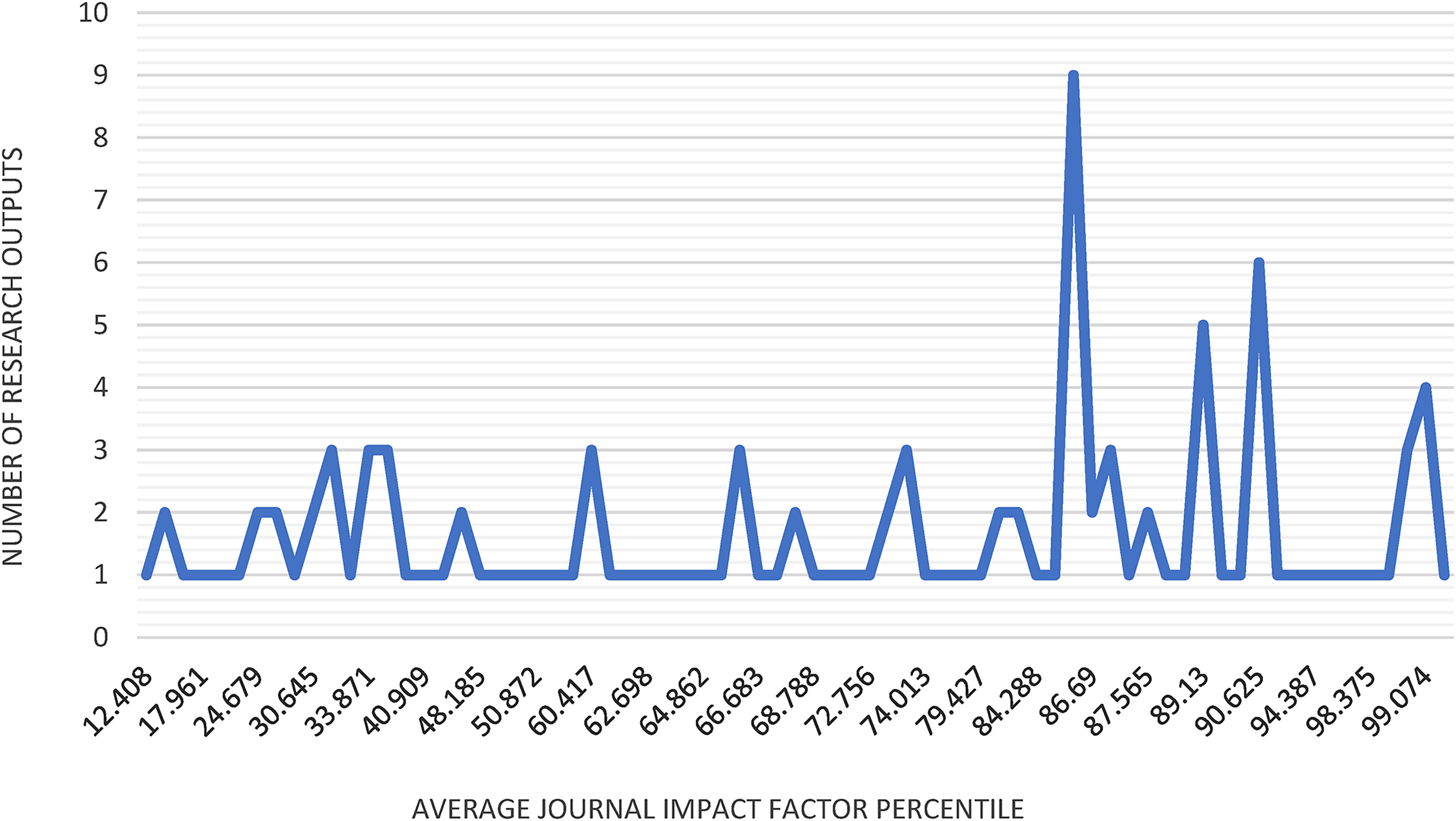
Number of outputs for each average journal impact factor percentile.
From 2000 to 2020 in Ireland, research outputs were produced across a wide variety of out-of-hospital research areas (see Figure 5). The most frequent area of research was ‘Resuscitation’ research with almost 30% of all research outputs linked to this category (see Appendix B). Figure 5 illustrates the variation in outputs for each of the categories and research methodologies over the period of the review. As outlined in Figure 5(a), although research related to ‘traditional’ clinical out-of-hospital presentations dominated outputs, the last 5 years have seen outputs engage with ‘evolving’ clinical research such as alternative care pathways. Additionally, the last 10 years have resulted in an increase in research outputs in non-clinical spaces (e.g., education, professionalism, and interprofessional collaboration). Methodological choices have also evolved throughout the period in this review. Quantitative research designs were dominant prior to 2012; however, we observed an increase in methodological diversity over the last 10 years, with several qualitative and mixed or multiple methods research designs published (see Figure 5(b)).
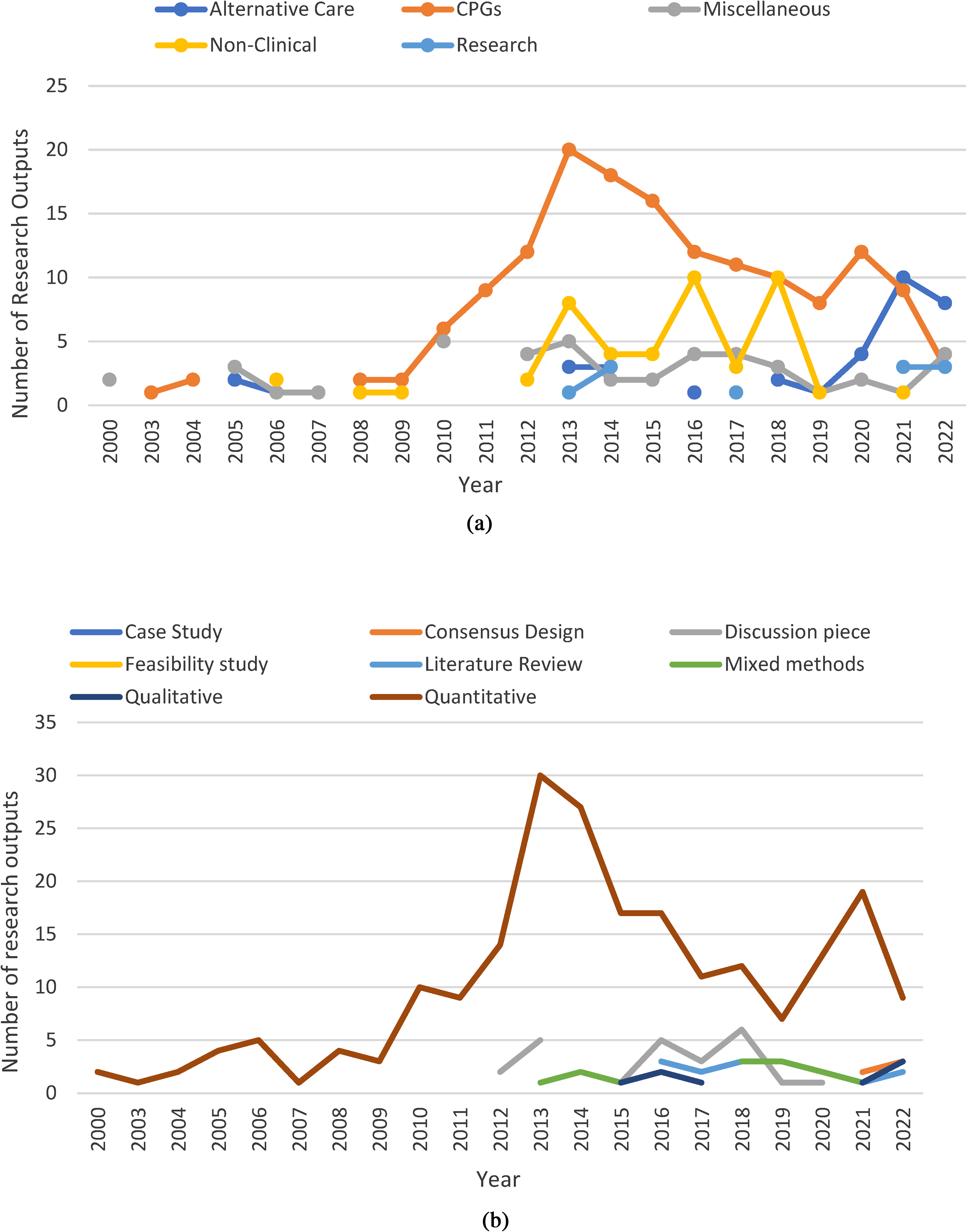
Variation in research outputs by categories (a) and research methodologies (b) for each year included in the review.
Finally, nearly 400 researchers produced the research outputs included in this review. Of note, 249 (62%) of these researchers were listed once on a sole research output (see Appendix C). Of the 123 conference abstracts, practitioners were first author on 39 (32%), and senior author on 8 (6.5%). A decrease emerged for peer-reviewed manuscripts (n = 160) with practitioners first author on only 36 outputs (22.5%), and senior author on only 8 (5%). Meanwhile, only one grey literature report featured a practitioner in the first or senior author position (9%). The 17 most prolific research contributors were predominantly non-practitioners with three exceptions. These 17 researchers contributed to 10 or more outputs, with only five researchers listed as authors on more than 20 research outputs over the last 20 years. This review was limited to research related to the Irish out-of-hospital setting, and as a result, some researchers have additional research outputs that were excluded from this review related to other jurisdictions (e.g., Australia, Canada) or other contexts (e.g., in-hospital studies).
Discussion
This review sought to identify and evaluate the quantity and scientific quality of the evidence published to date in the Irish out-of-hospital literature. Almost 300 research outputs were produced by nearly 400 researchers in the 23-year period from 2000 to 2022 inclusively. Most of these researchers appeared on a single output and did not have sustained research output involvement. Out-of-hospital research in Ireland has largely focused on ‘traditional’ clinical areas such as resuscitation. The evidence was produced predominantly by non-practitioners (e.g., physicians, non-clinical researchers), and practitioners were rarely first or senior authors on publications. Finally, the emerging diversity of research topics, while encouraging, suggests that Ireland may benefit from a more strategic approach to identifying, funding, and researching pertinent issues related to out-of-hospital care. We therefore identified four needs to be addressed in Irish out-of-hospital research: a need to focus on contemporary issues; a need to promote practitioner-led research; a need to translate findings to appropriate venues; and a need for a strategic direction that facilitates research capacity building. These needs mirror recent findings in Australia. 27
A need to focus on contemporary issues
A dominant focus on ‘traditional’ out-of-hospital clinical issues (e.g., cardiac arrest) may limit the understanding of other complex health and social care situations that are presented to practitioners and other healthcare professionals working in out-of-hospital contexts in Ireland. For example, with a continued focus on care-close-to-home and reducing emergency transports and admissions, other jurisdictions such as the United Kingdom, Canada, and Australia have produced a wealth of research focused on community paramedicine and alternative models of care.28–30 In addition, international colleagues are producing evidence related to vulnerable and under-served populations including the role of paramedics in substance use disorder and harm reduction, mental health calls, palliative care, and those experiencing homelessness.31–34 While some studies have started the process of researching new roles such as community paramedicine, additional research is required to better understand the role of paramedics in providing health and social care in complex contexts in Ireland. There is an opportunity to further research contemporary issues facing practitioners in Ireland such as mental health calls, substance use disorder, care of older adults, and the disparities of rural health access. Given that some research areas may require less attention to be adequately informed than other areas, we recommend that the findings of this review are brought to stakeholders in Ireland to identify perceived research gaps based on their understanding of the system.
A need to encourage practitioner-led research
The production of out-of-hospital research should seek to engage those who are involved in the work. Of the seventeen most prolific researchers in this review, only three are registered practitioners, all of whom hold leadership positions. In addition, there were a limited number of first and senior-author publications by practitioners, despite an increase in the number of paramedics with honours, master's, and doctoral degrees over the last decade. Graduates must be supported to publish their work in an academic setting, and employer organisations must work to build capacity to support these professionals. Partnerships with universities such as those evident in the United Kingdom supporting research paramedics, 35 and the establishment of conjoint appointments such as the clinician-lecturer in Australia support such developments. 36 Encouraging broad engagement with diverse paradigms and perspectives is also a priority. Without diverse approaches to understanding complex problems (e.g., clinical, sociological, economic, lived experience), out-of-hospital research in Ireland may fail to identify and therefore meet the needs of those who use it, including the practitioners who do the work.
A need to translate findings to appropriate venues
Getting the information to those who need it is an additional challenge facing researchers in Ireland. While the reported number of conference abstracts (n = 123) and peer-reviewed publications (n = 160) proves that some dissemination and translation is taking place, it is unclear how many conference abstracts were followed through to publication, due to the challenges in identifying such publications. Generally, peer-reviewed publications have increased steadily in Ireland since 2013, the majority of which were published in 2016. The effects of the COVID-19 pandemic may be reflected in the overall reduction in output in the year 2020 and the immediately following years. Strict lockdown regulations in Ireland related to COVID-19 may also be a contributing factor to the decrease in conference/symposium abstracts in the year 2020. This aside, if research is not consistently translated from concept to presentation to peer-reviewed publication, the potential for duplication of work is increased, leading to a waste of valuable resources. This lack of translation may be due to several factors such as a lack of protected time to work on research, a lack of funding to support travel and open-access publication, and a lack of appropriate supervisory capacity to facilitate – all common themes in out-of-hospital research internationally. 27 In addition, without a clear knowledge brokering strategy for the work produced by out-of-hospital researchers in Ireland, research may fail to inform decision-makers and policymakers who would benefit from the findings. 37 A clear strategy for knowledge dissemination from research to policy, service, clinical, and public users is needed.
A need for strategic direction and resource commitment
Finally, and perhaps explaining some of the previous findings, the emerging diversity of research topics without reference to a core concept suggests a strategic approach to identifying, funding, and researching pertinent issues related to out-of-hospital care in Ireland is required. For example, researchers in Canada recently produced a series of principles to guide the future of paramedicine. 38 Several studies since then have anchored themselves in or referenced their contribution related to the principles outlined in this document. 39 As a result, there is now a clearer alignment between the profession and the research informing it, and a clearer link to research outputs and who may benefit from them. Australian researchers have also recently published a research agenda and priorities for Australian and New Zealand paramedicine that outlines priorities aligned with key areas of health service redesign, expanding scopes of practice, worker health and well-being, and systems of care. 40 An overarching strategy for out-of-hospital research in Ireland should be developed, informed by engagement with stakeholders and end-users (i.e., those who expect to use the research) as well as involving patients and the public in a collaborative manner. 41 This strategy will help to identify strategic priority areas for research focus and well as inform funding models, suggest personnel requirements, and inform resources required, with the potential to increase collaboration across researchers and institutions.
Limitations
Although we followed sound methodological approaches there is the possibility that some research eligible for inclusion in the report has been missed. For example, students in Ireland undertake research for academic qualifications but these outputs are not always publicly available. This presents a limitation to the review.
Conclusion
There is an emerging out-of-hospital research culture in Ireland. However, research remains largely focused on ‘traditional’ clinical topics associated with emergency care, it is predominantly conducted by non-practitioners, and is poorly translated to appropriate venues. There is a need to focus on contemporary health and social issues in the Irish context, a need to build capacity within the practitioner workforce to produce and lead research, and a concerted effort to ensure the translation of findings to appropriate venues. A strategic plan that encourages diversification in research topics and methodologies, identifies funding, personnel, and resources required, and promotes the value of research findings to key policy areas would strengthen this resolve. This will help Ireland to move towards a healthy, sustainable research culture in out-of-hospital research.
Supplemental Material
sj-docx-1-pam-10.1177_27536386241263359 - Supplemental material for A scoping review of out-of-hospital research in Ireland from 2000 to 2022
Supplemental material, sj-docx-1-pam-10.1177_27536386241263359 for A scoping review of out-of-hospital research in Ireland from 2000 to 2022 by Kelly-Ann Bowles, Niamh M Cummins, Michelle O’Toole, Shane Knox, Liam Hemingway, Julia Williams, Emilia Ozioma Uzoukwu, Brett Williams and Alan M Batt in Paramedicine
Supplemental Material
sj-docx-2-pam-10.1177_27536386241263359 - Supplemental material for A scoping review of out-of-hospital research in Ireland from 2000 to 2022
Supplemental material, sj-docx-2-pam-10.1177_27536386241263359 for A scoping review of out-of-hospital research in Ireland from 2000 to 2022 by Kelly-Ann Bowles, Niamh M Cummins, Michelle O’Toole, Shane Knox, Liam Hemingway, Julia Williams, Emilia Ozioma Uzoukwu, Brett Williams and Alan M Batt in Paramedicine
Supplemental Material
sj-docx-3-pam-10.1177_27536386241263359 - Supplemental material for A scoping review of out-of-hospital research in Ireland from 2000 to 2022
Supplemental material, sj-docx-3-pam-10.1177_27536386241263359 for A scoping review of out-of-hospital research in Ireland from 2000 to 2022 by Kelly-Ann Bowles, Niamh M Cummins, Michelle O’Toole, Shane Knox, Liam Hemingway, Julia Williams, Emilia Ozioma Uzoukwu, Brett Williams and Alan M Batt in Paramedicine
Footnotes
Acknowledgements
The authors would like to acknowledge Jennifer Bolster for assistance with article screening. The authors would also like to acknowledge the assistance provided by Brendan Cawley from PHECC in the reviewing of the final manuscript. The authors would like to acknowledge the peer reviewers for their in-depth review and feedback which improved the final manuscript. The authors would also like to acknowledge the impact that Irish researchers have on out-of-hospital and paramedicine research in contexts other than Ireland.
Author contributions
All authors contributed to the development of the review protocol. AB conducted the initial and subsequent searches. AB, MOT, SK, KAB, JB, NC, and LH screened abstract and full texts for inclusion, as well as extracting data from the studies included full texts. KAB resolved conflicts in the screening, reviewing and data extraction phases. LH complete the analysis of journal quality, MOT matched research outputs to clinical themes and KAB completed the methodology grouping. KAB emailed key researchers to check current outputs and source additional outputs. KAB, NC and AB drafted the final manuscript. All authors edited the manuscript for intellectual content. AB led the revisions recommended by peer review. All authors have approved the final version for publication and accept responsibility for its content.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KAB, NC, and SK are associate editors, and JW and AB are deputy editors of paramedicine.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Pre-Hospital Emergency Care Council (Ireland).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.