
Abstract
This study aims to investigate and describe the relationship between acquired leadership capability and clinical performance in the out-of-hospital environment (OOH) and to identify and explore those key themes that might influence a relationship between paramedic leadership aptitude and patient safety. This study employed a qualitative descriptive design using a combination of purposive and convenience sampling. Data collection occurred via semi-structured interviews conducted over teleconference. Qualitative thematic analysis was chosen with an inductive orientation, semantic focus of meaning, and experiential framework taken to coding and theme generation. This methodology facilitated the discovery and analysis of the participant's personal experiences with the interconnectedness of leadership and clinical skills and the associated implications to patient safety. Data was collected from seven registered paramedics, all of whom were working for public sector ambulance services as specialist, advanced care paramedics. Five primary themes emerged: (1) discovery of human factors, (2) knowledge growth is formal and informal, (3) working smarter, (4) leadership expectations and usefulness and (5) transparency of errors. These themes underpin the importance of, and provide constructive insights into, the relationship between leadership and clinical skills in paramedicine and the impact on patient safety. This research has identified that those non-technical skills (NTS) including that of leadership employed in paramedicine are inextricably linked and of equal importance to those technical clinical skills The assessment of a paramedic's NTS against a required standard in a similar way to a technical skill, is important when considering practice competency policies moving forward.
Introduction
Since the turn of the century paramedicine has transformed from what was considered a trade to that of a pre-hospital healthcare profession that required registration to practice. This was initially led by the United Kingdom (UK) then followed by Australia and New Zealand with the USA and Canada also introducing state or provincial based licencing requirements during this time. 1 This has been in part driven by a scarcity of primary healthcare resources and a growing and ageing population requiring a much broader scope of practice with particular reference to that of low-acuity presentations.1,2 In many jurisdictions, paramedicine has an expanded out-of-hospital (OOH) scope of practice and has clinicians specialising in both high and low acuity presentations. 3 Furthermore, the burgeoning field of community paramedicine is evolving to support primary healthcare providers, 3 all of which are required to align with the various registration authorities’ mandated focus on patient safety. 1
The nature of the OOH environment limits ready access to a senior clinician or manager requiring paramedics to routinely assume and demonstrate leadership capability contemporaneously with that of clinical competency, ensuring patient safety and minimising incidence of clinical error. 4 A paramedic's operating environment is also decidedly uncontrolled, resource limited and requires a wide array of clinical skills when compared to that of a better resourced and more controlled in-hospital operating environment. 4 There is limited evidence mapping a relationship between the transferability of a paramedic's leadership capability to that of their clinical skill set, other than the identification of non-technical skills (NTS) that are highly desirable for individual paramedics, and indeed all healthcare professionals. 5 Leadership is a key NTS along with other skills and attributes such as decision making, communication, empathy and ethics.5,6 A paramedic will also work in constantly changing teams, placing an even greater necessity on NTS. 6 Should these cognitive and social skills be desirable within the clinical practice of a paramedic, it would be in the interest of all ambulance services to further investigate any associated links to clinical performance. 5
In contrast to paramedicine, physicians and nurses in Australia have a long history as registered professions and have evolved clinically to meet changing patient needs with an expanding scope of practice and that of specialisation such as the recent development of the nurse practitioner role. 7 Both medicine and nursing have identified strong associations between individual and team leadership capability with an improvement in patient safety, including an increase in the reporting of patient safety issues within a hospital environment.8,9 It is not unreasonable to suggest that parallels may exist within paramedicine as it in turn evolves as a registered healthcare discipline.
The relationship between nurse and physician leadership and patient outcomes has been well documented in the literature with systematic reviews identifying linkages between both senior and frontline leadership to that of clinician wellbeing and patient safety, including the incidence of adverse events over the short and long term.9–12 This is in addition to the ongoing psychological state of nurses and physicians and the resultant impact on organisational culture.8–10 Conversely, there is very limited evidence examining these linkages within paramedicine.
Recent research has also identified a strong correlation between self-aware authentic leaders with that of improved healthcare organisational performance and the development of strategies to reduce both inevitable and preventable medical errors.12,13 The promotion of this ethically driven leadership approach helps to reduce the incidence of hospital medical error rates, maintains patient safety and increases the incidence of medical error reporting. 14 The reporting of adverse events by clinicians has been shown to be heavily influenced by ethical leadership practices that promote psychological safety and reduce any perceived power distances between fellow clinicians. 15 These correlations are worthy of further investigation within paramedicine.
Clinical leadership programs have been prevalent in contemporary healthcare for some time, emerging as a result of sub-optimal clinical environments such as crises or unpredictable situations that would have directly affected patient care.16,17 Clinical leadership is seen as interactive and transformational rather than a transactional process that evolves and develops over time for the purpose of improving patient safety. 16 The interchangeability of clinical and leadership skills is an important element in this process and one highly applicable and sought after in the OOH environment of paramedicine. With a lack of current evidence in this space, this research has been designed to explore the perceptions of paramedics as to the role of leadership within their clinical practice.
Methods
Qualitative design and approach
This study has employed a qualitative descriptive design framework investigating whether those paramedics with an acquired leadership capability, have had their clinical practice influenced as a result of their training. A qualitative approach was chosen to facilitate the inductive exploration of the possible relationship between paramedic leadership and patient safety. 18 This qualitative descriptive design utilised reflexive thematic analysis to facilitate the discovery and analysis of the participant's personal experiences with the interconnectedness of leadership and clinical skills and the associated implications to patient safety. It was used to explore and describe experiences in a free and unstructured form from participants who have been emersed in this phenomenon.19,20
Researcher characteristics and reflexivity
As a mature age and newly qualified registered paramedic working for an Australian ambulance service, the lead researcher's prior experiences in organisational leadership have provided a basis for understanding how NTS might support the technical skills in the setting of the OOH environment. The researcher is a practicing paramedic and as such has experienced firsthand the clinical leadership and patient safety challenges being faced in Australia. This, when considered with the researchers’ previous background as an academically credentialled executive leader across small and large non-healthcare-related corporate entities, has influenced their perspectives upon the role of leadership in the relatively nascent field of paramedicine in Australia.
The supporting research team comprises a recently retired Australian state ambulance service senior executive leader, academic and practitioner as chief researcher, and a senior university academic and researcher who have provided subject matter expertise in the shaping and guiding of thematic development whilst ensuring contemporary academic oversight of the project.
Throughout the research project, there were regular diarised discussions to openly debate and discuss those themes and views generated from the data whilst maintaining a reflexive outlook. Given the diverse background of the research team consideration was consistently given to the potential for predispositions associated with the experiences and presumptions influencing the interpretation of the data.
Research paradigm
This research was undertaken with an interpretive lens as an analytical guide, the methodology of which is to understand phenomena via the meaning assigned to them on behalf of the participants. 21 The foundation of this assumption is that interpretive epistemology is subjective in nature in that external reality may only be accessible to those observers after the shaping or influence of their own worldviews, perceptions and experiences to date. 22 With this guiding lens the researcher is afforded the opportunity to understand the phenomena from the viewpoint of the participant rather than themselves. 22 The goal of this research is to attempt to understand the interpretations of phenomena by the individual participants rather than attempt to discover a universal and knowledge-free truth. 22
In applying this paradigm to the research at hand it was required to understand the participant's perspectives as to which leadership characteristics are portrayed, and the processes by which those characteristics influence patient safety. With the interpretive lens of a belief in socially constructed multiple truths and realities being created rather than discovered, 22 the iterative process of revisiting and reconsidering ideas and viewpoints irrespective of the time of formation drove the process of data collection. With subsequent analysis, themes were either abandoned or expanded. This approach allowed the researchers to recognise those multiple constructs and the influence they have on paramedic practice.
Study participants and recruitment process
Australian and New Zealand registered paramedics who self-identified as having leadership training within the last 3 years, either directly or indirectly, were deemed eligible to be included in the research project. These paramedics were eligible regardless of public or private sector employment; however, they were required to be currently employed within a paramedic role within Australia or New Zealand. Convenience sampling was used with recruitment advertisements disseminated via an approved electronic flyer using researcher professional networks and the Australasian College of Paramedicine platform. In addition, purposive sampling was employed with paramedic authors of recently published work in the area of leadership directly contacted. Expressions of interest (EOI) were sought from all potential participants to ensure eligibility. Recruitment of participants occurred between June and August 2023 with eight (8) potential paramedics responding and seven (7) meeting the eligibility criteria. If eligible, participants were sent a videoconferencing invite with an attached explanatory statement and a participation consent form. Participants were assigned a randomly generated alphanumeric code for deidentification purposes in addition to redacting any data that might identify a participant.
Data collection
The collection of data was undertaken by way of semi-structured and in-depth one-on-one interviews between the lead researcher and each participant utilising the videoconferencing and transcription platform, Zoom. This platform was chosen to both alleviate the geographical spread of participants whilst preserving the strength of face-to-face communication. 23
The semi-structured interview question prompts are provided in Appendix 1. The interview guide is composed of nine questions with additional sub-questions designed to align themselves with our research aims and questions. The question prompts were created by the lead researcher after a thorough systematic review of the current literature and subsequent review of the question prompts by the research team. The intent of the interviews was to encourage the participants to freely express their own experiences and perceptions of the relationship between leadership, clinical skills, and patient safety in a confidential and psychologically safe environment.
Before undertaking the interviews, a trial interview was conducted on 25 August 2023, to test question validities and establish whether call quality and reliability would suffice for the study as a research tool. Following this test interview data collection occurred between 11 and 30 September 2023. Before analysis and subsequent data interpretation and with chief researcher oversight, the interview transcripts were reviewed to ensure accuracy and clarity of content. In addition, the authors considered data collected from these participants to be of sufficient depth to provide valuable insight that addressed the study's aims and no further recruitment was attempted.
Data analytic strategy
Data analysis was undertaken by way of Braun and Clarke's six steps of thematic analysis,24,25 where each transcript was coded and collated into potential themes for further review. The lead researcher was responsible for steps one to four of the data analysis utilising a manual methodology. An inductive approach facilitated this process beginning with specific observations to generate potential theories and ideas. A semantic focus on meaning and experiential framework was taken to the coding and theme development. 26
The lead researcher and chief researcher met at steps four to six to assess the initial fit of the proposed themes and review the practicability of the analysis. Furthermore, the themes were reviewed for clarity and strength of core concepts before reviewing the appropriateness of the findings in answering the research aims and questions. This research adheres to the Standards for Reporting Qualitative Research (SRQR). 27
Ethics
Ethical approval was granted by Monash University (MUHREC Project ID: 38635). Signed consent forms were obtained from all participants.
Results
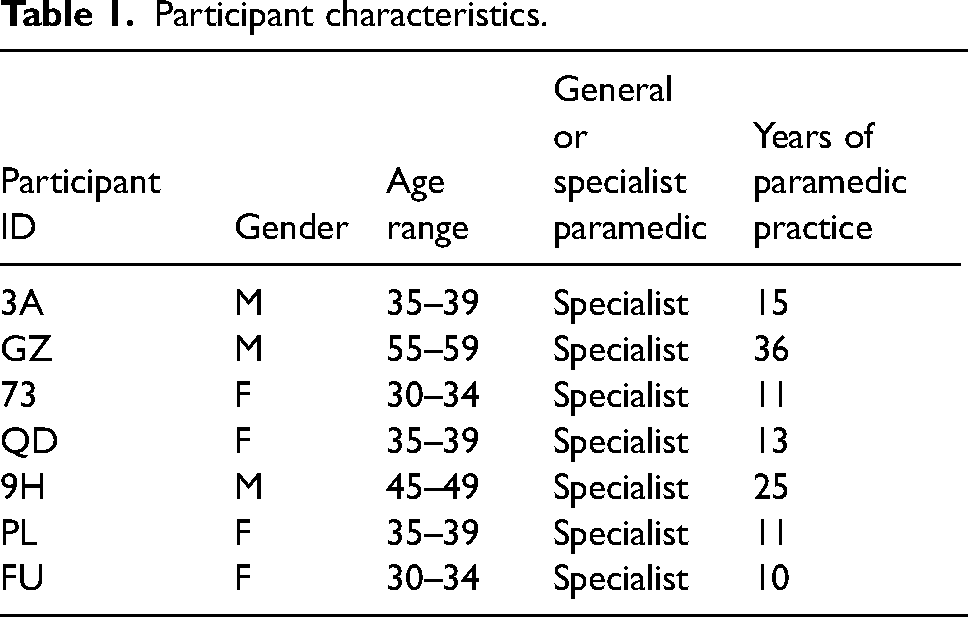
As shown in Table 1, of the seven participants who were interviewed for this study 43% (n = 3) were male and 57% (n = 4) female providing a balanced gender representation. The age range varied from those in their early 30s to those in their late 50s. When combined with 10–36 years of paramedic practice, this cohort represents a relatively extensive level of paramedic practice experience. All respondents were advanced-level specialist paramedics who have undertaken additional clinical training to obtain a wider scope of practice compared to the general duties’ paramedics. After the seventh interview, the data did not reveal any new ideas and the authors considered that the strength of the data collected to date once analysed would enable the generation of the themes. As such, recruitment was halted at this point.
Participant characteristics.
The thematic analysis generated five themes, each of which has associated subthemes. These five themes and associated subthemes are presented in Figure 1, and are: ‘discovery of human factors’, ‘knowledge growth is formal and informal’, ‘working smarter’, ‘leadership expectations and usefulness’ and ‘transparency of errors’.
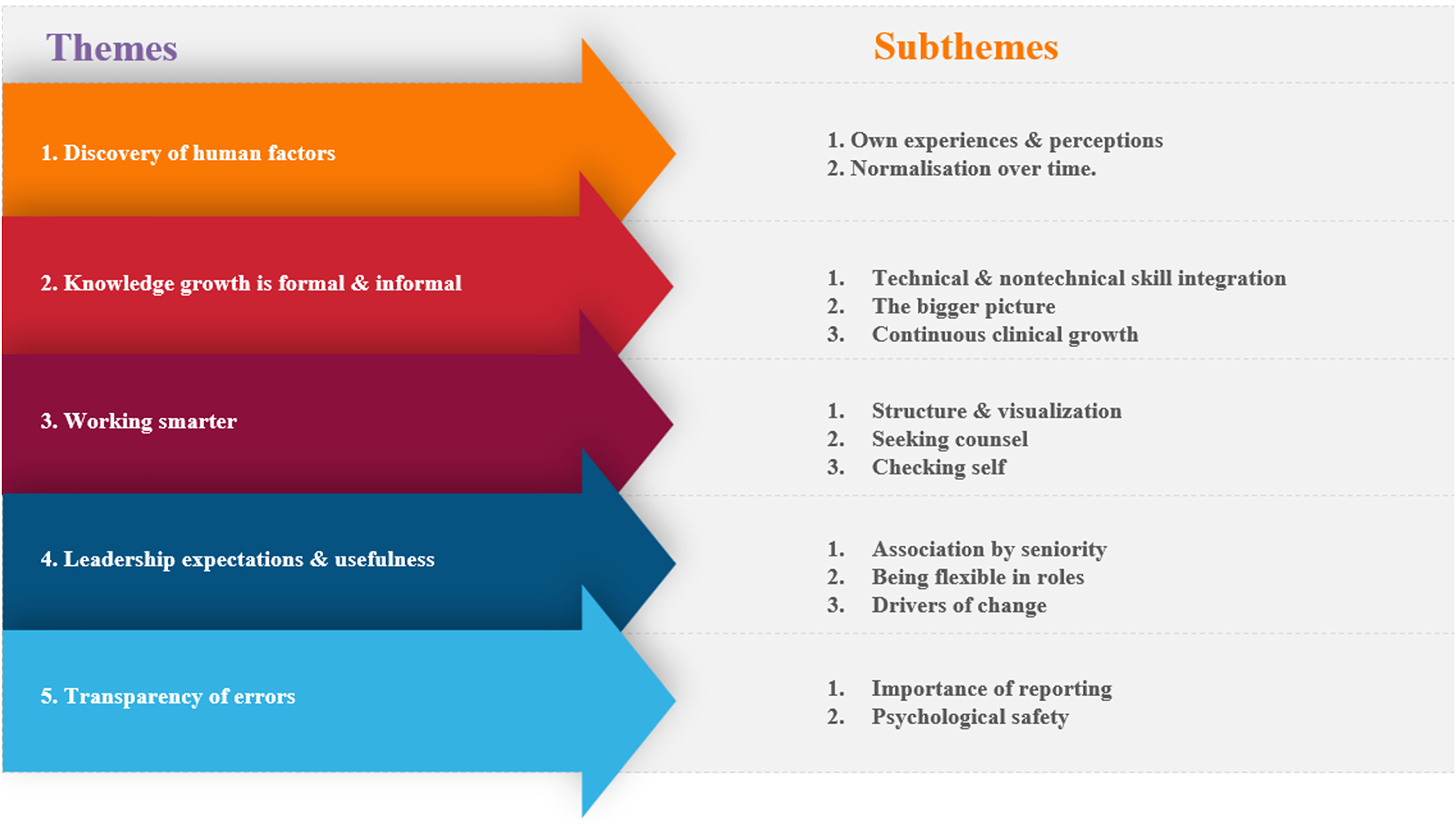
Theme and subtheme generation.
Theme 1: Discovery of human factors
This theme outlines the current perceptions of the role of leadership in paramedicine and the source of its body of knowledge. The data elucidated subthemes where contemporary awareness was built upon the individual paramedic's previous experiences and the normalisation of leadership practices over time.
A consistent reflection within the data told of the self-discovery rather than the teaching of the non-technical paramedic skillset which incorporated such human factors as leadership and communication. This knowledge was furthered with experience and time becoming an embedded part of paramedic practice. 3A – I don't recall ever having something that just talked about leadership within the program when I started to be in intensive care. Transitioning from ALS into intensive care with ahead full of knowledge, but no application … It took (me) time and practice and reflection as well, on things that went well and didn’t go well. QD – I think the only leadership training I had as a non specialist paramedic was related to leadership training relating to on scene management and interaction with other health agencies, and in particular scene leadership you know, at a multi, either a multi agency or multi casualty scene. G2 – There's [now] a heavy emphasis on team leadership and crisis management, clinical crisis management and things like that. So, they are finally introducing those concepts which I think are widely important. FU – It definitely built your confidence up a bit, they talked a lot about the new styles of leadership. You know the [importance of] vulnerability during a debrief and the responsibilities that we have now, and stuff like that. QD – I've ended up going into you know, roles that have management opportunities which you know you can extend to being a leader within. A personal philosophy for me is that if I'm gonna be a leader in one place, then that probably needs to extend more broadly throughout. 9H – that [leadership] was just something that I saw as an important part of my own development, whether that be consciously or subconsciously so, it was just these roles I kind of found myself in. PL – I'd always sort of pictured leadership as like role modelling and setting examples for others around you. So not just junior crews, but sort of others around you, even if they're at the same sort of qualification level. So it's a lot about role modelling and encouraging people to do their best in their roles, and like trying to better themselves. FU – the way that they want us to lead or engage with others and be part of the team [has changed]. You know. They don't want this like stick bashing idea. They want this, you know, team-based focus towards treating a patient. 3A – it was something I actually struggled with in the first 6 months. With transitioning from a [general duties] paramedic into the intensive care space, with a head full of knowledge, but no application, and having the confidence to turn up to these bigger jobs. Now, whereas you know, being the [general duties] paramedic on scene, when the intensive care [paramedic]comes you hand over and they assume leadership, and you play an auxiliary role, whereas now the shoes on the other foot and you were the one that was [providing] the leadership things, and it just took time and practice and reflection as well, on things that went well and didn't go well. And still to this day I think one of the most difficult things that intensive care paramedics do. 73 – I don't think I truly had an understanding or appreciation of the importance of leadership until I started on road as [a specialist] paramedic when you're attending really complex high acuity cases with lots of moving parts. And you're the senior clinician at a scene, and you've gotta manage a large number of paramedics and usually just the one patient who's critically unwell with so many things [that] need to be done, and so many uncontrollable scene factors. It wasn't until I was actually a [specialist] paramedic where I think I gained a true and more accurate understanding of how important it is and what it means.
Theme 2: Knowledge growth is formal and informal
This theme recognises that clinical leadership knowledge may be derived from either formal or informal means. The integration into paramedic practice of this knowledge requires both deliberate practice and capacity for self-reflection and recognition of personal strengths and weaknesses. PL – it's been data collation, really, of observation and seeing what I have observed to work really well, and what I liked from leaders. 3A – good technical skills, complement, non-technical skills, and vice versa like, I suppose the more practiced you are at a skill, whether that be leadership or intubation for instance the more brain space you're gonna have to be able to do the other. 73 – And when you tell people about this job, all they ask you about is the skill [of the procedure], which you know is understandable. But it's funny how small the importance of the skills seemed or felt compared to the whole job of all the non technical skills that were going on. PL – What most people think is when you come up clinically. From general duties paramedic to specialist everyone thinks about the clinical jumps. So, the you know, the new guidelines, the new toys that you get to play with new medications. And I sort of saw that as the biggest big component of it. But what I came to realize is that the more important part and the more challenging part is the leading, leadership and mentoring role that comes with these advances in your in your role.
QD – there is an expectation that intensive care paramedics will be the clinical leader at these scenes, and you know, if there's a mica (mobile intensive care ambulance) team manager then they’ll probably be the clinical leader, but if it's a CSO (clinical support officer) they’ll probably be the clinical leader. So to some extent, having a hierarchy like that is quite protective (of the patient) because you always know who it's seen as likely to be. If they are delegating it to someone else like a mica student its because they are giving them the opportunity to try, develop their leadership in a supported environment.
FU – you know, you walk in, and everyone just looks at you. And all of a sudden, all that expectation is on you, and you know you can’t take that all on and be expected to do everything. And then, all of a sudden, you find yourself in a situation where you have 800 things going on, and you can't possibly do them all. And you just become very overloaded. 73 – as a leader, the non-technical skill of taking [for] lack of a better phrase, the clipboard approach, so, standing back and being less involved, less physically involved in all the skills and having better oversight to increase the situational awareness of the job. I think that was probably one of the biggest shifts in the way I behave at a job as a leader is taking that step back and observing and task delegation and only getting, you know, getting your hands dirty if it if it's required so to improve that situation, because as soon as you start doing a task you can get task focused. So that would probably be the biggest change in behaviour for me. G2 – I'm an old dog, but I’ve certainly been taught new tricks over the last few years. I think it's a good thing. QD – [I have] motivation to seek out good leadership from people above me, and probably more comfort in questioning things that I don't think are particularly well done, because I see there are opportunities for improvement. So that's probably a key thing for me. G2 – I feel a lot more confident now than what I used to, especially talking with other staff like at other clinical levels and being less judgmental and understand that we all do make errors, clinical errors from time to time. And yeah, I feel a lot more comfortable in my own skin talking through these matters with other people of other clinical levels. FU – But I think this idea of vulnerability was a good one. I love that, you know, we can turn around and say, hey, you know what I stuffed up on this job, and this is why, and this is what I'm gonna learn from that, and I think showing that to other people, was phenomenal. The changes that came from that one moment, you know, was incredible to see.
Theme 3: Working smarter
This theme encompasses the data explaining participants’ perspectives as to how acquiring leadership knowledge and capability has influenced their approaches in maximising patient safety and perceptions as to whether these approaches are likely preventing or reducing the incidence of clinical error. Whilst adherence to clinical practice guidelines and procedures and drug therapy protocols was without question, this theme explored those individually derived NTS that were complementary as such. Employing a shared, structured and systematic approach with visualisation techniques, seeking counsel from peers and the recognition of bias were all found to be essential components. QD – So I think probably one component is adherence to guidelines which are written to promote patient safety. You know, that's a really key form of doing things right. Is to have an evidence base for what we're doing. In the first place. 73 – Yes, I think it's a massive factor that helps reduce error, absolutely huge. You know, just thinking about the times where I have made mistakes. I would say more often than not it's because I've neglected my standard of assessment and I've neglected or ignored my biases and haven't checked myself, I think, its huge yeah, I think that's massively reduces errors. 73 – I know that sticking to a structured approach works because you don't really miss anything when you do that but the times where I have missed things is when I haven't done that. QD – I think that is a really key thing for me with regards to patient safety, but also with regards to leadership. [If] I'm not sure I'll pull out my phone and check the guideline and make sure that the dose that I'm giving is right, you know, is this particular thing indicated at this point in time, and confirm what I think. FU – Talking to your partner on the way to the job. Really important. So, you know, talking about you know, what's our approach to this patient, what role are we each gonna have, you know, at the job? And what skills do I think I'm going to need? And then, if I'm feeling unsure about a particular skill, just a quick look to have a look at the skill. 9H – visualisation of what you anticipate is going to be happening. So not only visualizing what a scene might be, I've taken in all the information on the way to a job and started to put some things together, also having ability to seek out information that isn't there, so if there's, you know, voids of information, trying to fill them, but also preparing the team that you're with. So, if that was a two-person ambulance crew preparing them beforehand just saying, okay, when we get there, what we can expect is this, and these are the roles that we are going to perform. G2 – I always jump on my phone and check the protocol, check the contradictions which I never particularly routinely did, but because of the constant changes of our protocols, I think that's an important thing, and to include my partner as well more in the assessment of the patient and ask them, you know, are you comfortable with this treatment, you know, you're welcome to have your thoughts on it, and to work more as a team. PL – I learned to take my ego out of it, and share my thoughts and observations amongst myself and the other paramedics on scene because I try to create an environment where they, the other paramedics, feel empowered to communicate back to me and tell me what they see, and I say to them, am I missing anything? This is what I'm thinking because of X, Y, and Z. Can you think of anything that I’ve forgotten. I just wanna make sure like we're doing the right thing. Or, this is my plan, we're going to start by doing this. Can you think of anything. So, I try and involve the other people to and take the I'm the senior paramedic, so I know what I'm doing, so I'm more experienced than you - just have to take that out of it, because it's not safe for the patient to keep that all to yourself, because we're not infallible. We're human, and we can miss things and make mistakes. 9H – Please ask questions if you're not sure what's going on or not, always take that time when we've laid out our plan to say, is everyone okay with the plan? Is there anything I've missed? Is there anything that we think we can do? Is there anything you are concerned about? And generally, you know the answers, but occasionally it's like you haven't got the end tidal [CO2] plugged in, or something [and] you're like Oh, thanks! Great! What that comes down to is humility and leadership. If you don't have that, you'll find yourself in a hole very quickly. QD – I have a very key focus when driving to a scene about the potential impact of you know, clinical, and cognitive bias and how that can affect my assessment of a scene, my assessment of the patient, the care provided to a patient. 73 – If I was to you know, deviate from those strategies in front of a [general duties] crew they're less likely to uphold the good standard at their next case versus if I do uphold my standards, I think they're more likely to continue that for their next case
Theme 4: Leadership expectations and usefulness
This theme considers the data relating to how participants believe an OOH service or organisation perceives their roles once they have acquired leadership knowledge and capability. The data reveal subthemes describing both formal and cultural sources of leadership expectations, the broader and potentially beneficial leadership roles that result from an acquired capability and its perceived importance in driving organisational change. 73 – I don't think there's a true understanding or appreciation of just how much leadership skills we need to be able to run a complex job. Well, I don't think they're appreciated. I don't think they're understood, and I don't think they place any importance over them. QD – there is an expectation that intensive care paramedics will be the clinical leader at these scenes, and you know, if there's a team manager then they'll probably be the clinical leader. 9H – I think that the organization has an expectation that you perform a clinical leadership role in those roles, yeah. 9H – Yeah, look, I think [about] stages of the hierarchy, you would be expected as a senior paramedic, to lead a job as the senior paramedic, and that would largely be chronological, you know how long you've been a paramedic. 3A – it's a lot of money spent on a lot of people sitting idly for a long period of time. QD – I think there's probably an expectation, even with, you know [general duties] stuff who will see us as paramedic educators. There is that expectation with that additional training. FU – The management in my local area, has an expectation that as a [specialist] paramedic, and being lots of new ones on our station, that we will provide education in our role, and we will do that extra work. G2 – Every paramedic should be able to access to a clinical leader or clinical support person. And not necessarily only on the phone, someone can turn up and help. PL – I think the sections of the organization that either haven't worked operationally at all or haven't for a long time sometimes don't understand how much of the [specialist paramedic] role is leadership and not just intubating and you know the technical stuff. You do find more people that are freshly out of operational roles or have come from come up through the clinical pathway themselves tend to understand it a bit more. There is, of course, you know, the really old school ones that just don't get it. FU – I think that they sort of are placing a bit more of an expectation on you now. And I do think that they want you to be the drivers of a cultural change. 73 – There's too much emphasis and importance placed on KPI's in the service, such as arrival of a paramedic crew to a case. I don't think there's enough emphasis on what skill level certain patients need. FU – Sometimes you do just feel like that they just want to be able to script the idea that they have [specialist] paramedics. So, they can just tell the media that they are in the community, you know, sometimes it does feel that way. But I think the culture is changing. I think it's slow, but I do think it is changing.
Theme 5: Transparency of errors
This theme underscores participants' perceptions as to how acquiring leadership knowledge and capability has influenced their opinions as to what behaviours promote the growth of a patient safety culture in paramedicine. The subthemes emphasise the importance of reporting and understanding sources of individual and system errors and highlight the importance of providing a psychologically safe environment for paramedics to discuss patient safety concerns. 3A – If things don't go as planned then stepping back and pointing the finger is not a healthy way to learn or to practices as a paramedic. 9H – It's very easy to blame an individual when it's likely to be a systems error. PL – you know it's natural if you do something wrong, like, you know, and you don't want to say anything, and you want to try and pretend that nothing happened. But that is so dangerous for our patients. 73 – Like it would be phenomenal like how much better we would be and how much better [we] would be at our jobs because of these learnings and if everyone was more open and transparent about mistakes and learning from each other's mistakes. I think like people's skills and knowledge would be huge, would be so much bigger than what it is now, with being able to have open genuine conversations about, you know, knowledge gaps, etc. 9H – especially when you start working as a [redacted] paramedic you go I can't afford to stuff up, whereas today, If I did, I'd go. Oh, I messed this up, you all need to learn from me, Look! Look what I did, what I messed up. FU – I think if you're self-reporting, I think that shows a lot of self-awareness. 9H – I think patient safety and ambulance is absolutely enhanced when the staff are safe as well. So, I think when the staff feel that they have compassionate governance, that they're supported, you know that the staffing stuff is taken care of, you get better patient outcomes. And I think this is a really key thing for ambulance. If you can provide that safe work environment, and that's physically safe, but also psychological safety, and make sure that you will be looked after you hopefully will have less burnout, less patient safety issues. PL – Just accepting that mistakes do happen, and then actually being open about reporting them stops people from hiding their weaknesses or things that they could improve on, because as soon as you then highlight something that could be improved, then you're going to actively try and improve it.
Discussion
The results from this study provide constructive insights into the relationship between leadership and clinical skills in paramedicine and the impact on patient safety. The five themes generated provide pertinent points of discussion describing the nuanced and complex associations between leadership capability and that of patient safety. All of these promote the notion that high-performance paramedicine embraces both technical and NTS as having equally pronounced importance.
The first theme describes the current understanding of the role that leadership plays as a function of NTS utilised in daily paramedic practice. The changing cultural paradigm of both the importance of those NTS and the sources of acquiring them in the first place. That is, the reliance of the paramedic's own life experiences, where they may have recognised the value of leadership practices prior to their training and subsequently cementing those practices as normalised behaviour.
These findings are aligned with existing literature where the recognition of leadership and those other NTS deemed as desirable for paramedic practice have been identified with recognition of a conceivable link with patient safety. 5 The importance of these NTS has been well considered and applied in practice to other complex and high-risk fields such as aviation and medicine, where parallels may be drawn with paramedic practice, suggesting potential links with improved patient safety and clinical error avoidance. 28 This is in addition to the suggestion that the engagement of those leadership practices adds value to a paramedic's individual technical strengths to promote better patient outcomes over time. 4
This theme poses the question as to whether the inclusion of formal leadership and/or NTS development programs should be considered when drafting educational and practice competency policies moving forward.
The ongoing formal and informal growth of a paramedic's body of knowledge over time is highlighted in the second theme of this study. The recognition of an inextricable link between those technical and NTS notes the greater challenge in acquiring the latter. The data describes and acknowledges the importance of prioritising leadership when paramedics are faced with a complex presentation where multiple clinicians may be present on scene, and the integration of clinical skillsets to avoid cognitive overload is required. This is in addition to the informal and formal growth of knowledge in a safe learning environment.
The wider healthcare literature describes the growth of knowledge occurring formally with the adherence to correct protocols by the individual clinicians, whilst also suggesting the informal growth in knowledge be at least in part the responsibility of those senior staff and managers.9,10,29 There are limited similarities within the paramedic literature other than the recognition that the adoption of approaches such as crew resource management used in other high-risk industries would benefit patient safety and capture of knowledge/learning opportunities in those team environments.6,28
This study highlighted that paramedics were employing individually derived leadership strategies in their attempts to work smarter with those clinical guidelines, procedures, and protocols to maximise patient safety. The participants adopted risk minimisation techniques before patient engagement and sought real-time performance feedback from peers whilst on the scene, in addition to reflective review from those individuals they considered as clinical leaders. It was revealed that the success of those leadership strategies was heavily reliant upon the paramedic's capacity to recognise the presence of and then address those clinical or cognitive biases whether they had become apparent by themselves or by their peers.
These findings are in line with previous studies that had found that leadership strategies were used to reduce preventable medical errors and increase the clinician's commitment to improving patient safety. 13 In addition, it was noted that those clinicians who operated in environments that promoted these leadership strategies maintained a greater degree of clinical competence which in turn again promoted patient safety.9,11
A greater understanding as to how these strategies might be developed, and the positive influence they could have in paramedic practice, is worthy of further investigation. Identification of the expectations that an OOH service or organisation has of its paramedics post acquiring leadership capability and the perceived sources of leadership are an important finding in this study. The positive correlation between time of service and perceived leadership, whilst not unremarkable, was found to be considered as a disconnect in some circumstances, whilst the positive correlation between clinical level and perceived leadership was readily expected. It was also anticipated that those clinical leaders would both take the lead in educational excellence and driving organisational change. Within the wider literature, there is strong support for the notion that leadership development is strongly correlated with both individual and team level advancements across all NTS and, as a result, the caregiving process. 17
There is emerging evidence in support of a significant relationship between those authentic leadership qualities and that of a patient safety culture including that of improved patient outcomes within hospital-based organisations worthy of further investigation in the OOH environment. 8 The challenge to both drive change whilst maintaining sound clinical practice individually and organisationally cannot be understated.16,17 An understanding of how these leadership skills are both developed and applied to paramedic practice might not only influence current practice but also the overarching body of paramedicine knowledge.
Our findings have promoted the proposal that identification and reporting of clinical errors in a non-punitive, psychologically safe environment is crucial to the success of future policies, procedures and guidelines that will enhance patient safety. The development of individual paramedic leadership traits within this environment will promote ongoing clinical growth in day-to-day practice.
The results of this study add to a growing body of research that supports the notion that sound leadership practices in healthcare environments will contribute to both the reduction of clinical errors and as such improve patient safety overall.12,14,15 The central theme of this association is the linking of leadership practices to organisational culture and its shaping or orientation of the working environment as to error management and the resultant behavioural practices of employees. 12 The wider literature has found that the provision of psychological safety and the reduction of perceived power distances between operational/management tiers will heavily influence the willingness of clinicians to report adverse events. 15
These findings offer some consideration to OOH organisational management practices around those policies and procedures that are aimed at preventing errors. That is, the promotion of leadership practices facilitates transparency of those inevitable clinical errors and recognises the opportunity for knowledge growth that will shape the paramedic's behaviours around patient safety.
Limitations
A number of limitations should be considered when interpreting the results of this study. Firstly, the design is observational focussing on the recollections and understanding of the leadership experiences of a small cohort of specialist paramedics. This design in the absence of a control group allows the researchers to consider the prevalence of a possible relationship between leadership and clinical skills with that of patient safety.30,31 Notwithstanding this, these limitations should not be considered unique or inherent to this study and as such will still provide insights to the causal effects of this relationship, which in turn contribute to a more nuanced future understanding and assessment. 31
As described in Table 1, all the participants were of a ‘specialist’ paramedic clinical level. This cohort represents only a minority, with the majority being general-duty paramedics, of the total population of paramedics targeted for the study. As such, the interpretation of the results and the consideration of external validity to the wider population will need to be reflected upon with care. This is in addition to the investigation as to why those generalist Paramedics did not respond to the request for EOI and whether a perceived NTS knowledge gap exists between these cohorts.
The development of the semi-structured interview guiding questions asked of participants were developed after a systematic review of the literature and reflective consideration by the lead researcher and an additional review with the chief researcher as an expert in the area. Notwithstanding that the questions were both open ended and used as a guide, the risk of potential bias that might unintentionally skew responses will remain. Whilst a noteworthy limitation, this observation is not unique to this study. 32
Conclusion
Paramedics are often patients’ first point of contact and set the scene in their journey through a health care system. The importance of leadership development and other NTS within paramedic practice is key to the growth and promotion of a patient safety culture within this setting. This study has explored the perceptions of paramedics and the role of leadership within their clinical practice and its influence on patient safety. As there have been very limited previous investigations specific to paramedicine, this research has sought to seek out those lived experiences of registered paramedics and in doing so contribute to this body of knowledge. The participants in the study have identified that those NTS are inextricably linked and of equal importance to those clinical skills. The awareness of those human factors by either formal or informal means provides a basis for clinical growth, driving organisational change and the promotion of patient safety.
Footnotes
Acknowledgements
The lead researcher would like to acknowledge the Frederick (Ric) Bouvier family for generously awarding the lead author a full scholarship for completion of this honours program.
Data availability statement
The deidentified data supporting the findings of this research project are available upon request from the lead investigator. The data will not be made publicly available to maintain participant confidentiality.
Declaration of Conflicting Interests
Kelly-Ann Bowles is an associate editor of the Paramedicine Journal.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Appendix 1. Semi-structured interview questions asked of participants.
How would you describe your recent leadership training and how did your recent leadership training come about? How did you perceive the role of leadership in the out-of-hospital environment before your recent training? What aspects of your recent leadership training resonated with you as a paramedic and what aspects challenged your thinking? Do you believe this training will contribute to your skillset as a paramedic, why? What strategies do you currently employ when treating a patient to maximise their safety?
a. How did you identify these strategies? b. Have these strategies changed over time and if so, why? c. How do you know if these strategies are effective? Do you feel that these strategies are effective in preventing or reducing the incidence of medical errors?
d. If so, why? e. If not, why? What are your thoughts on how the ambulance service perceives your role as a clinical leader on the road? What strategies do you employ after treating a patient with a challenging clinical presentation? Do you have any other thoughts or information that could provide greater insight into the promotion of a patient safety culture in the out-of-hospital environment?