
Abstract
Introduction:
Patients with palliative care needs seek support from paramedics in instances of unexpected worsening of symptoms associated with their primary diagnosis, but often do not desire conveyance to an emergency department. Despite this, up to one-quarter of patients with palliative care needs will experience an avoidable admission to the emergency department. British Columbia Emergency Health Services, in collaboration with Canadian Virtual Hospice and regional health authorities, developed the Palliative Care Assess, See, Treat and Refer (ASTaR) Clinical Pathway, with palliative clinical practice guidelines and education to support paramedics minimising avoidable admissions to emergency departments.
Aim:
To describe the paramedic management of patients enrolled in the palliative care ASTaR clinical pathway, supported by paramedic-specific education and clinical practice guidelines.
Methods:
This study was a retrospective descriptive cohort study of the first 100 patients enrolled by paramedics in the palliative care ASTaR clinical pathway following its introduction in October, 2019.
Results:
The median age of patients was 78 years (IQR 70–88), they were more often male (n = 58) and in a private residence at the time of 911 call (n = 91). Calls for assistance were in the work week (n = 73), but often out of business hours (n = 61). Primary care paramedics provided the majority of care (n = 64), most frequently contacting paramedic specialists for clinical advice (n = 32, 47%). The most common patient complaints were dyspnoea (n = 25), altered conscious state (n = 16), mobility assistance (n = 14), and pain (n = 13), with pharmaceutical intervention required in less than half of cases.
Conclusion:
Paramedics continue to play a critical role in supporting patients with palliative care needs, particularly during out-of-hours periods. When supported by robust clinical practice guidelines and integrated systems of care, this cohort study demonstrates that paramedics may be able to manage the requirements of patients with palliative care needs and their family, friends, and carers, beyond clinical care and conveyance.
Introduction
There is a growing demand worldwide for community-based palliative care and home-based deaths, 1 with up to 75% of Canadians indicating a preference to die at home. 2 Accordingly, paramedic attendance for unscheduled palliative care needs in the out-of-hospital (OOH) setting is increasing. 3 By definition palliative, or end-of-life (EoL) care involves providing patient-centred support to alleviate suffering and allow a ‘good death’ for those with life limiting conditions. 4 This necessitates an interprofessional, holistic, and non-curative approach to manage physical, psychological, social, and spiritual suffering for patients as well as their families. 5 Palliative care can be initiated at any stage of disease progression, with clinical strategies to manage pain or worsening physical symptoms common for EoL patients such as respiratory, cardiovascular, or neurological deterioration. 6 Acute symptom crises often involve severe pain, nausea, vomiting, delirium, agitation, and dyspnoea, and can be very distressing for both patients and caregivers. 7
Often, patients with palliative care needs seek support from paramedics in instances of unexpected worsening of symptoms associated with their primary diagnosis but do not wish for conveyance to an emergency department. 8 Despite this, some studies report up to one-quarter of patients with palliative needs will experience an avoidable admission to the emergency department, 9 with paramedics often facilitating conveyance. 10 The need to improve the paramedic approach to patients with palliative care needs is widely accepted.11,12 Previous literature has identified multiple complex barriers to providing goal-concordant care. These have included fear of reprisal if patient EoL wishes are not clearly documented 13 and feeling under-prepared to manage EoL situations,14–16 resulting in paramedics defaulting to a traditional ‘treat and transport’ approach to care. 14
To address these barriers, British Columbia Emergency Health Services (BCEHS) in collaboration with Canadian Virtual Hospice and regional health authorities in British Columbia (BC) developed the Palliative Care Assess, See, Treat and Refer (ASTaR) Clinical Pathway. 3 The introduction of this clinical pathway was supported by palliative care clinical practice guidelines for common palliative care presentations, such as delirium, pain, dyspnoea, nausea and secretions, 17 as well as paramedic-specific palliative care education. The goal of this clinical pathway was to reduce patient conveyance to the emergency department in suitable patients and support patients wishing to receive care in the home after contacting paramedic services.
There is a paucity of evidence examining paramedic palliative care once key barriers are combatted. As paramedic services globally continue to develop and implement palliative care clinical pathway and clinical practice guidelines, research is needed to evaluate their suitability and efficacy. 18 To address this gap in the literature, this retrospective descriptive cohort study aimed to describe the characteristics, and subsequent paramedic management, of patients enrolled in the palliative care ASTaR clinical pathway, supported by paramedic-specific education and clinical practice guidelines.
Methods
Study design and participants
This descriptive observational study was a retrospective cohort study of the first 100 patients enrolled by paramedics in the palliative care ASTaR clinical pathway between October 24th, 2019, and January 24th, 2021. Patients are eligible for enrolment in the palliative care ASTaR clinical pathway if they have been diagnosed with an advanced, life-limiting illness, their care is currently focussed on comfort and symptom management, or the patient has pre-established goals of care consistent with treatment in place. In accordance with the clinical pathway, none of these patients were conveyed to the emergency department as a component of their management plan. Due to data constraints, it was not possible to identify the number of patients who paramedics attempted to enrol but were subsequently conveyed to hospital. Patients were selected using non-probability convenience sampling. No exclusion criteria were applied.
Study setting
BCEHS is the largest paramedic service in Canada, covering 944,000 km2 and responding to over 700,000 911 calls each year. 19 BCEHS provides an Anglo-American model of OOH care, utilising paramedics in the delivery of clinical care. 20 The majority of care is delivered by emergency medical responders (EMRs) and primary care paramedics (PCPs), supported by advanced care paramedics (ACPs) and critical care paramedics (CCPs) in complex cases. BCEHS provides remote clinical support via the CliniCall service, which gives frontline clinicians 24/7 access to paramedic specialists (ACPs or CCPs) for ad hoc clinical advice and support, or escalation to emergency physician support (EPOS) where required. 21
The scope of practice and clinical practice guidelines for each level of clinician within BCEHS are available open-access, online. 17
Data sources
BCEHS paramedics utilise Siren™ (Medusa Medical Technologies, Halifax, NS) to document electronic patient care records (ePCRs), which was interrogated to identify the variables of interest. A purpose-built data collection tool and protocol was developed to extract variables from ePCRs during the study period.
Variables
The variables of interest included: patient characteristics, medical priority dispatch system (MPDS) coding during 911 call, response priority, day of the week, incident location, patient palliative diagnosis, patient chief complaints, bystanders present, 911 caller, specialists contacted from scene, documented goals of care, management provided by paramedics, crew clinical level, and overall case times. Codes were developed to categorise any non-pharmaceutical interventions such as positioning and education.
Data were analysed using Statistical Package for the Social Sciences (SPSS), Version 29 (SPSS Inc., Chicago, IL). Categorical values are described using frequencies (n) and percentages (%). Continuous data are reported using mean, median and standard deviation or interquartile ranges, dependent on normality of distribution, which was assessed using the Shapiro–Wilk test.
Bias
We aimed to ensure trustworthiness in our data and findings. The data collection tool was developed collaboratively by three members of the research team (GM, TJ, NB) with input from two external paramedic researchers with extensive experience in chart review. It was then pilot tested by a fourth member of the research team (JH) and suggested changes were incorporated into the final version. One researcher collated the data (GM) and 25% of data from the ePCRs was randomly audited by a second reviewer (TJ) for accuracy. We report the findings of this study in accordance with the STROBE reporting guidelines. 22
Ethics
Ethics approval for this study was granted by the University of British Columbia Clinical Research Ethics Board (H20-01906) and by the Human Research Ethics Committee of Charles Sturt University (H21066). This research was also reviewed and supported by the BCEHS Pharmacy, Therapeutics, Research and Practice Advisory Council (PTRPAC).
Results
Patients in this study ranged in age from 38 to 100 years of age (median 78.3, IQR 18 (70–88)) and had cancer as the most common palliative diagnosis (n = 61). Calls to paramedic services primarily occurred during the work week (n = 66), but outside of business hours (n = 61). Patients with palliative care needs ultimately enrolled in the clinical pathway were overwhelmingly in their private residence (n = 91), with family or friends most frequently contacting paramedic services (n = 78). Patients were assigned an emergency response in 75% of cases. Patient and incident characteristics are presented in Table 1.
Patient and incident characteristics.
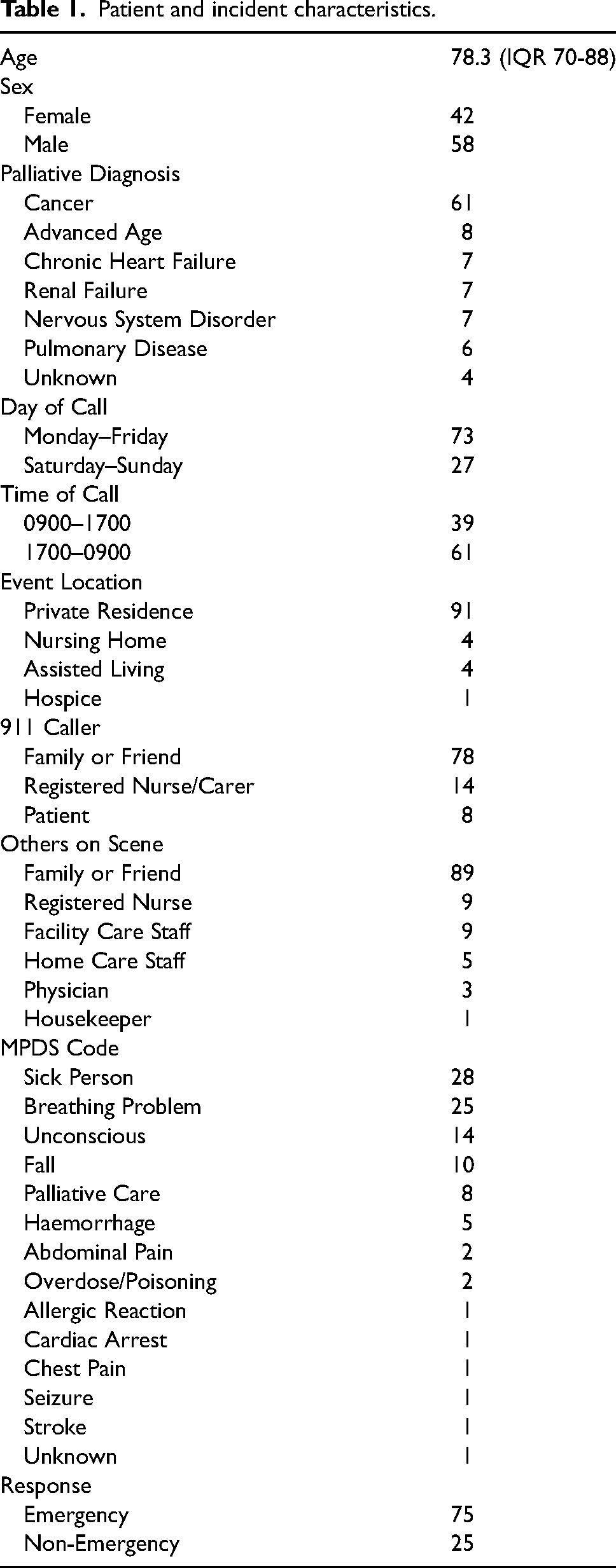
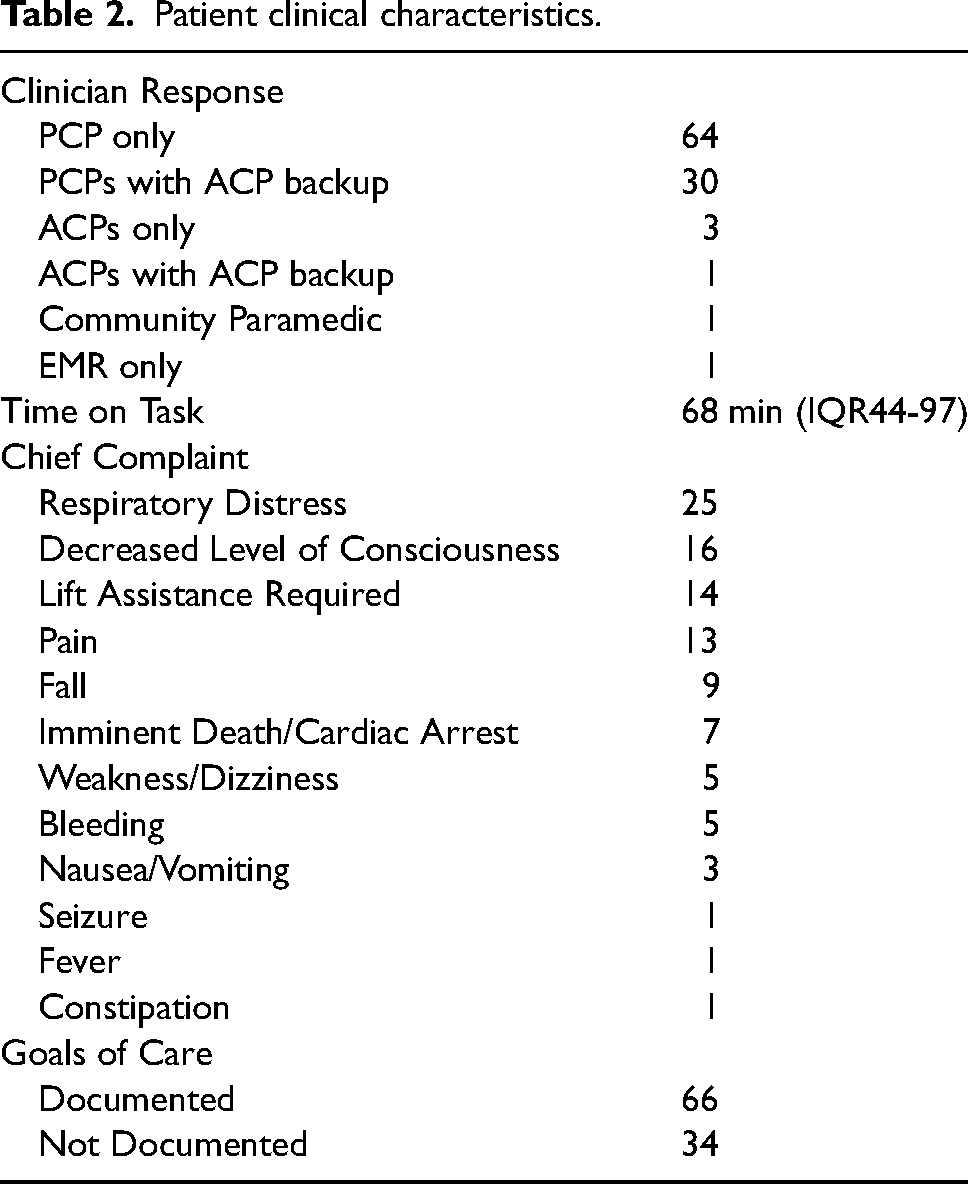
A PCP response was the most common paramedic crew configuration (n = 64), with ACPs frequently supporting PCPs as backup in a tiered response model (n = 30). Common chief complaints reported to paramedics included respiratory distress (n = 25), decreased level of consciousness (n = 16), lift assistance required (n = 14) and pain (n = 13). Goals of care, determined prior to paramedic attendance by patients and their family physician or palliative care team, were only documented and available at the scene for two thirds of patients (n = 66). Clinical characteristics of patients are detailed in Table 2.
Patient clinical characteristics.
Paramedics most often contacted the CliniCall service from scene to consult with paramedic specialists for support (n = 32). Paramedics also contacted the patient's own palliative care team (n = 14) or family physician (n = 7) for guidance.
Common non-pharmaceutical interventions provided by paramedics included lift assistance, bed transfers, or repositioning (n = 45), education regarding palliative care plans (n = 44), education regarding patient's own medications (n = 16), as well as specific discussions relating to goals of care and documentation (n = 25). The pharmaceutical interventions most frequently required were oxygen (n = 23), morphine (n = 19), dimenhydrinate (n = 8) and patients’ own just-in-case medications (n = 8). Paramedic treatment decisions were primarily supported by the General (n = 100), Dyspnoea (n = 28) and Pain (n = 16) clinical practice guidelines. Paramedic management and clinical practice guidelines utilised are detailed in Table 3.
Paramedic management.
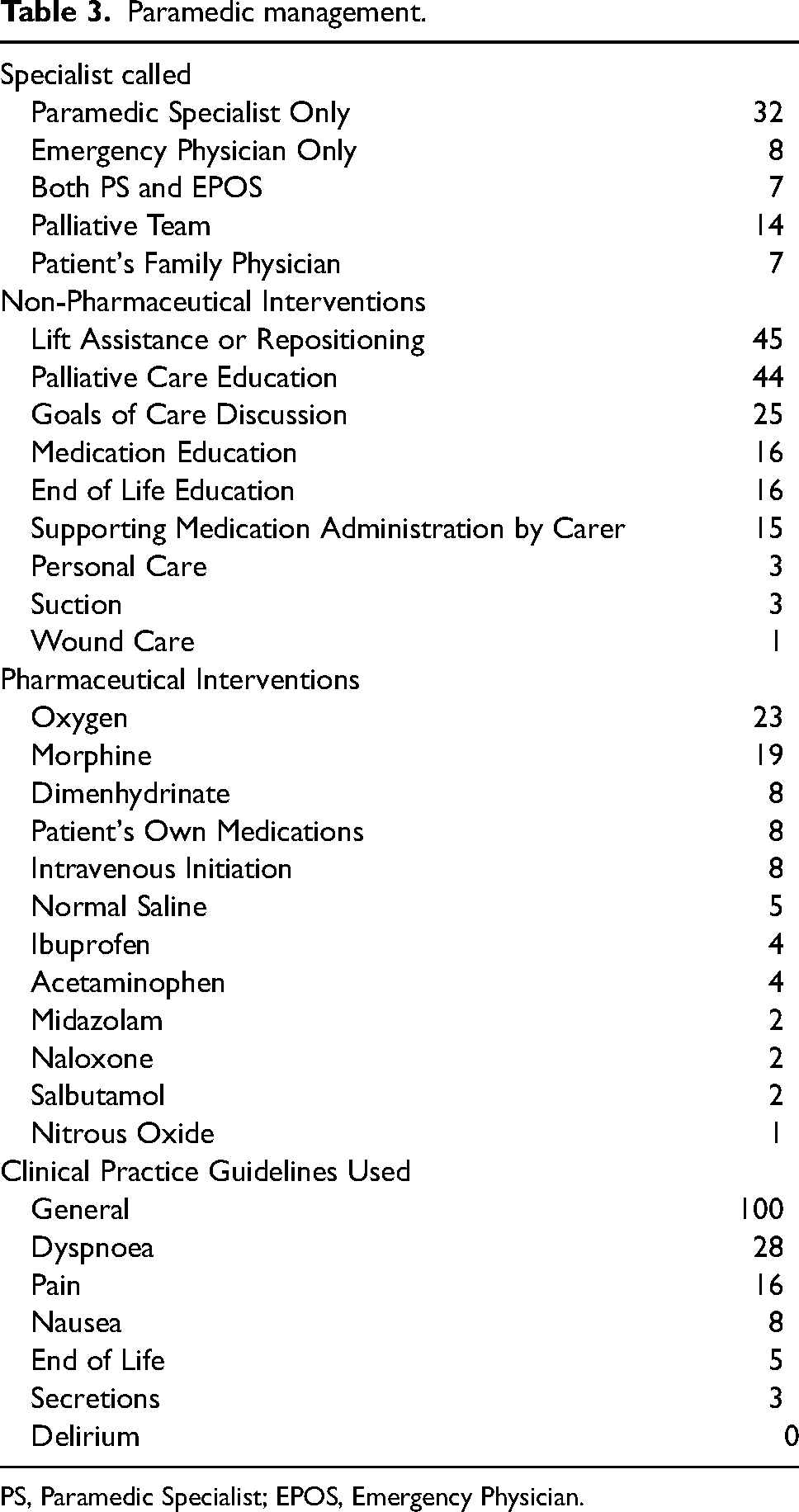
PS, Paramedic Specialist; EPOS, Emergency Physician.
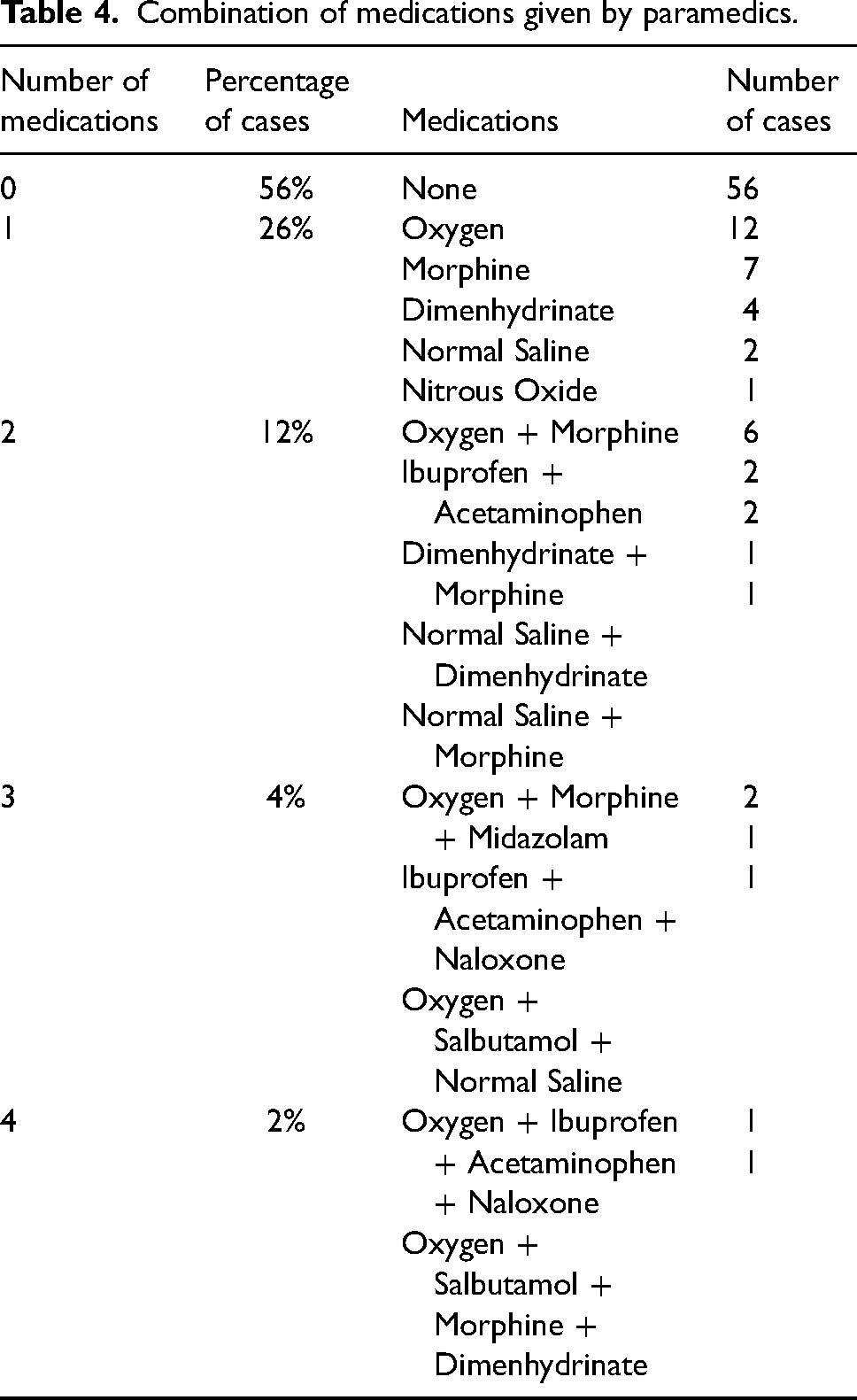
Pharmaceutical interventions were not required in over half (n = 56) of cases, with a single pharmacological intervention provided in 26 cases. The combinations of medications provided as a component of patient management are detailed in Table 4.
Combination of medications given by paramedics.
Discussion
This descriptive cohort study characterises emergency paramedic palliative care patient encounters and management of these patients when treated under a novel ASTaR non-conveyance clinical pathway and associated palliative care clinical practice guidelines. This study addresses a gap in the literature, providing data on patients managed with paramedic-specific palliative care clinical practice guidelines following tailored education.
Our findings align with previous work which demonstrated that patients with advanced illness and palliative needs who contact paramedic services are most often categorised under MPDS as ‘Breathing Problems’, ‘Sick Person’ and ‘Falls’. 23 Notably, patients in this study were also commonly identified as ‘Unconscious’, possibly signalling higher acuity needs or variable application of MPDS compared to other jurisdictions. Our study adds to existing literature by highlighting that these presentations are commonly coded as ‘Delta’ or ‘Charlie’ responses, which often correlates with a response using warning beacons and sirens. Although patients with palliative care needs often require expeditious care from paramedics to alleviate suffering, the utility of an emergency response rate as high as 75% is questionable in patients with pre-identified life-limiting illness when emergency responses are associated considerable risk to paramedics and the general public.24,25 Given the under-utilisation of the ‘Palliative Care’ MPDS card in this case series future research should focus on original strategies for early identification of patients with palliative care needs who are likely suitable for care in the community, as were the patients in this study. This would facilitate an expedited response to palliative related events without imposing unnecessary risk to paramedics and the public.
Most patients in this case series contacted 911 during the working week, yet out-of-hours for many community-based palliative care teams. Paramedics responding to patients with palliative care needs outside of regular hours is consistent with previous research, 26 and highlights how paramedics provide an after-hours bridge to support these patients with unscheduled care needs. Notably, former apprehension towards assuming this role is shifting as paramedics adopt a holistic approach to palliative care and see this as aligning with their professional identity. 27
The patient management findings in this study offer valuable insight into the nature of palliative-related 911 calls and the subsequent care paramedics provide. The most common documented patient symptoms involved problems breathing, changes in consciousness, or worsening pain. This aligns with other research that identifies symptom management for breathlessness and pain as primary reasons for emergency calls to patients with palliative care needs.11,26,28 In response to these chief complains, paramedics primarily managed patients’ palliative care needs under the ‘Dyspnoea’ and ‘Pain’ clinical practice guidelines. Importantly, effective management of these two symptoms is thought to prevent unnecessary conveyance to hospital. 29
Broadly, it appears that most patient needs were met by treatments within the PCP scope of practice, with over half of the cases managed without the need for any pharmacological interventions. In the 44 events where medications were given, 59% (n = 26) of patients only required a single intervention, primarily oxygen or morphine. During the study period, administering opioids, benzodiazepines and antimuscarinic medications were beyond the PCP scope of practice. These findings have important implications for paramedic systems across Canada and internationally who utilise clinicians with a similar scope of practice, as they signal that PCPs may be able to successfully manage uncomplicated palliative care needs in a model with strong remote clinical support. As the paramedic approach to palliative care continues to mature, it is important for paramedic systems with similar scopes of practice to consider expansion of PCP education and medication formularies to better align with patient needs and reduce reliance on ACP crews for symptom management. 28
The study finding that 68% of cases involved some type of remote clinical consultation highlights the important role that remote clinical support can have in mitigating risk, especially for non-conveyance when goals of care are absent or unclear. 30 Research has also shown that paramedics are positively inclined to confer with a paramedic colleague, especially if they have a pre-existing professional relationship. 31 While this study did not investigate the nature of the phone consults, it is possible that the ability to contact a paramedic specialist gave paramedics additional confidence to leave patients at home following clinical care. With most encounters occurring outside of normal office hours, and only 14% of cases involving direct contact with palliative care teams, this study highlights the importance of specialised remote clinical support for paramedics providing unscheduled palliative care. 32
Alongside symptom relief, our findings also revealed how patients and families needed assistance to lift, transfer or simply re-position patients in almost half of cases. In some instances, paramedics were called specifically to facilitate a transfer onto a hospital bed in the home. There were also many situations wherein the family or carers were not able to move the patient from the toilet or back into the bed. Additionally, the paramedics often documented spending time repositioning patients with dyspnoea to ease symptoms and maximise comfort. While not directly reported in similar studies, this serves as a reminder that manual handling and lifting or moving techniques are foundational professional competencies in paramedicine and a valuable, but potentially undervalued skill set that paramedics contribute to interprofessional care of the patient with palliative care needs. 33
Our results also demonstrate how paramedics routinely perform teaching, a non-clinical intervention requiring strong communication skills. Paramedics in this study documented educating family and patients in various aspects of palliative care plans, including how to prepare and administer the patient's own medications. They also documented teaching family members what to expect as the patient neared EoL, other supports available in the healthcare system, and the importance of having clearly documented goals of care (absent in over one third of cases). These findings raise questions regarding paramedic readiness to fulfil the role of an after-hours educator in palliative care. Previous studies suggest that paramedics may lack confidence in their knowledge of support available in the wider healthcare system and speaking to family about EoL care. 34 Despite this, paramedics are increasingly identifying patient education and advocacy for patients with palliative care needs as a core component of their role. 28 Previous literature has highlighted that education can reduce paramedic anxiety, increase confidence and better prepare them to support family members, 26 particularly education targeting communications skills. 35 Effective communication with those on scene has been correlated with higher non-conveyance rates, allowing more patients to remain at home following management. 1 The findings of this research suggest that providing paramedic-specific palliative education along with the release of clinical practice guidelines supports paramedic confidence in acting as an educator for patients with palliative care needs and their families.
Limitations
This study has a number of limitations which are important to recognise. Our study was observational in nature and suffers from the usual limitations of this methodology, specifically that the manually extracted data from ePCRs relies on the information supplied by attending paramedics. Our conclusions are limited in that they do not evaluate patient satisfaction or re-contact rates for similar symptoms. Additionally, only patients not conveyed to hospital within the clinical pathway were assessed and not those with palliative needs who were ultimately conveyed to hospital, which limits our ability to identify features associated with failed attempts at enrolling patients in the clinical pathway.
Conclusion
This descriptive cohort study describes patient characteristics and management of patients with palliative care needs enrolled in a novel assess, see, treat and refer clinical pathway by paramedics in Canada. Paramedics continue to play a critical role in supporting patients with palliative care needs, particularly during out-of-hours periods. When supported by robust clinical practice guidelines and integrated systems of care, this case series demonstrates paramedics can manage the needs of patients with palliative care needs and their family, friends and carers beyond clinical care and conveyance. Further research should consider strategies for earlier identification of patients with palliative care needs during the emergency call-taking process, as well as the optimal scope of practice for primary care paramedics in Canada to best support the symptom-based management of patients with palliative care needs.
Supplemental Material
sj-doc-1-pam-10.1177_27536386231178965 - Supplemental material for Characteristics and paramedic management of patients enrolled in a novel assess, see, treat and refer palliative care clinical pathway: A retrospective descriptive cohort study
Supplemental material, sj-doc-1-pam-10.1177_27536386231178965 for Characteristics and paramedic management of patients enrolled in a novel assess, see, treat and refer palliative care clinical pathway: A retrospective descriptive cohort study by Tania Johnston, Richard Armour, Gamonluk Muinoi, Jennie Helmer and Natalia Bilton in Paramedicine
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article
Supplemental material
Supplemental material for this article is available online.
Correction (June 2023):
This article has been updated to replace XXXXXXXXXXX with CliniCall in the Result section since its original publication.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.