
Abstract
Background
Advanced airway interventions, including endotracheal intubation (ETI) and supraglottic airway devices (iGel®), are used for airway management. Advanced airway proficiency is critical to maintain patient safety. Airway registries are commonly used quality assurance tools that can drive system-level improvement. This study analyses the first two years of data from a new prehospital airway registry.
Methods
This is a retrospective review of the first two years of an airway registry for Intensive Care Paramedics in New South Wales Ambulance spanning 8 August 2020 to 8 August 2022. Changes in airway management effectiveness were examined as a time series and analysis proceeded regression using Newey–West standard errors. Additionally, a machine learning algorithm (generalised boosted model) was used to predict successful ETI.
Results
There were 872 unique advanced airway episodes suitable for analysis. Of 705 patients that had received ETI, 655 were successful resulting in an overall success rate of 92.9%. Intubation was achieved on the first attempt in 573 out of 705 (81.3%) patients. Supraglottic airway insertion was successful in 193 of 222 patients (86.9%). The first-pass success for the iGel® supraglottic device was 183 of 222 (82.4%). Considerable increases in ETI and iGel® first-pass success were observed over time. A machine learning analysis demonstrated that factors predicting success for endotracheal intubation included airway-grade, patient age, the use of video laryngoscopy, patient weight and the use of external laryngeal manipulation/bi-manual laryngoscopy.
Conclusions
This prehospital airway registry analysis demonstrates increasing advanced airway success over the first two years of registry implementation. These increases may be explained in part by the reflective feedback and awareness of airway management that results from the registry, training and the increased use of video laryngoscopy.
Introduction
Advanced airway techniques, including endotracheal intubation (ETI) and supraglottic airways (iGel®), are used to protect and maintain the patency of the airway; enabling oxygenation, ventilation and preventing aspiration. 1 Advanced airway techniques can also be associated with adverse events, including oesophageal and endobronchial intubation, unsuccessful placement and interruptions to chest compressions in cardiac arrest.2,3 Endotracheal intubation use by paramedics has been controversial.4,5 Studies show that paramedic ETI is generally associated with a lower success rate and more adverse events, compared to physician ETI.2,6,7 Recent randomised trials of ETI versus supraglottic airways in cardiac arrest found low success rates for the advanced airways used, especially for ETI.8–10 If it is true that many paramedic systems have sub-par success and more adverse events, then strategies to improve the success of advanced airway interventions and avoidance of adverse events are imperative to patient safety and outcomes.
An important strategy in improving successful advanced airway use is regular review, using standardised high-quality data. 11 Airway registries are used to prospectively record advanced airway interventions and enable the analysis to support feedback and quality improvement.11–13 New South Wales Ambulance (NSWA) commenced an airway registry for specialist Intensive Care Paramedics (ICPs) in 2020. The purpose of this new registry was to monitor service-wide airway proficiency and to enable the identification of opportunities for quality improvement. This new registry is comparable to registries in other jurisdictions in terms of information collected but does differ in that many other registries limit their collection to adults and have a large focus on rapid sequence intubation (RSI). 14 An analysis of the first year of the registry identified that video laryngoscopy (VL) was associated with increased success compared to direct laryngoscopy (DL), which led to practice changes in NSWA. 15 However, that analysis only compared video and DL and did not measure other factors such as time trends. The objective was to describe the findings from this new airway registry for the two years since its inception, with a focus on changes over time. Such trends could elucidate the factors that led to improvements in successful advanced airway placement, making advanced airway management safer.
Methods
This study followed the STROBE reporting guidelines. 16
Design and study setting
This is a retrospective review of prospectively collected registry data. NSWA has 6536 staff of which 81% are frontline paramedics and is one of the largest ambulance services in the world. This service responds to over 1 million emergency calls per year, with an average response time of 7.5 min to cardiac or respiratory arrests. 17 The service has a two-tiered structure, employing Paramedics and a smaller group of ICPs. Some ICPs have additional training and work in aeromedical teams as Critical Care Paramedics. Only ICPs are credentialed in ETI and both tiers are credentialed to insert supraglottic airways using the iGel® (a second-generation device made by Intersurgical). ICPs perform ETI without induction or paralysis medications.
Intensive Care Paramedics receive advanced airway training in didactic, manikin and simulation settings. As part of their training, all ICPs complete an operating theatre placement with anaesthesiologists and an on-road clinical internship prior to being credentialed in ETI. Equipment available to ICPs to facilitate ETI includes bougies, stylets and suction. Physiologic monitoring includes ECG, pulse oximetry and non-invasive blood pressure monitoring. Waveform ETCO2 use is required to confirm endotracheal tube placement. Colorimetric CO2 detectors are available as a backup device to waveform capnography. Confirmation of iGel® placement with ETCO2 technologies is not mandatory currently as only ICPs carry waveform and Colorimetric CO2 devices. Bimanual laryngoscopy with external laryngeal manipulation is taught to optimise glottic view during laryngoscopy as required.
In 2020, NSWA introduced a VL device with standard Macintosh blade geometry (McGrath® MAC VL). A video-assisted technique was encouraged when the DL view was inadequate despite optimisation. During the SARS-COV-2 pandemic, paramedics were encouraged to adopt a VL first approach to maintain clinician safety. This approach is still recommended for confirmed or suspected COVID-19 patients.
Registry eligibility and data sources
Any advanced airway attempts by ICPs (ETI or iGel®) are required to be documented in the Airway Registry. Only ICPs entered data in this registry during the study period. The registry is a REDCap (Research Electronic Data Capture) database, which is a protected web application. 18 Registry data was extracted for the dates ranging 8 August 2020 and 8 August 2022 and included pre-airway, airway and post-airway variables.
Predictors and outcomes
The primary outcome was successful advanced airway management. Endotracheal intubation success was defined as confirmation of tracheal tube placement by clinical means, supported by waveform or colorimetric ETCO2 detection. iGel® success was defined as adequate chest expansion being possible after insertion, with confirmation ETCO2 if available. The secondary outcome was first-pass success. First-pass success is defined as the placement of the ET tube on the first attempt, such that an endotracheal tube passes beyond the vocal cords and is seated correctly. 19 For iGel®, first-pass success is defined as instances with successful airway placement in one reported attempt. 20 An intubation attempt was characterised as the insertion of laryngoscope into the mouth with intent to intubate, and for iGel® an airway insertion attempt where the passage of the distal end of the iGel passed the patient's teeth. 20
Data analysis
Stata version 18 (Stata Corp, College Station, Texas, USA) was used in this analysis. Descriptive statistics were calculated for all variables. Categorical variables were presented as frequencies, and continuous variables as means with standard deviations, or medians and interquartile range. Categorical variables were compared with the χ2 test and continuous predictors with the t-test and analysis of variance or nonparametric equality-of-medians test. Hypothesis tests were two-sided, with a significance level of P < 0.05. The unit of analysis for this study is the individual patient. Therefore, success and first-pass are calculated at the individual patient level. This analysis reports odds ratios (ORs). An OR is a measure of the association between an exposure and an outcome. The OR measures the probability of an outcome occurring given a particular exposure, versus the probability of the outcome occurring in the absence of that exposure. An OR greater than 1 indicates a positive association between the exposure and the outcome, while an OR less than 1 indicates a negative association. 21
This study also analyses changes in success as a time series. The authors utilised an ordinary least squares regression on complete observations only and estimated Newey–West standard errors to account for autocorrelation heteroskedasticity in this time series. 22 A machine learning algorithm (generalised boosted model) was used to predict successful ETI. This model implements the boosting algorithm described by Hastie, Tibshirani and Friedman and is a re-interpretation of adaptive boosting, which was modified into the likelihood framework. 23 The machine learning algorithm produces estimates of ‘influence’, which is the measure indicating the relative importance of each variable in the final model. The machine learning analysis was limited to ETI because iGel® use was less common and therefore lacked statistical power. To further quantify factors that have a meaningful impact on success, the authors used logistic regression. All regression analysis was univariate, and no multivariate adjustments were made, as the authors reported descriptive statistics and causality was not the focus of this study. The authors reported findings as a point estimate with 95% confidence intervals where appropriate.
Ethics
This was a quality assurance project, and no identifiable data was used. Therefore, no formal ethics approval was sought. Research governance approval was granted by the research unit at NSWA.
Results
Success rates
During the study period, 999 entries were recorded in the registry, of which 872 were suitable for analysis (Figure 1). Of 705 patients that had received ETI, 655 were successful, resulting in a success of 92.9%. For ETI, the first-pass success was 573 out of 705 (81.3%) patients. Of 222 patients that had an iGel® inserted 193 (86.9%) were successful. The first pass success for iGel® was 183 of 222 (82.4%). ETI success was stratified by DL versus VL. The DL overall success was 101 out of 122 (82.8%) and first pass was successful for 83 out of 122 (68.0%). For VL, the overall success was 552 out of 583 (94.7%), and first pass for VL was successful in 489 out of 583 (83.9%). In 55 (6.4%) patients, both ETI and iGel® were attempted or successfully placed. Additionally, there were 23 (2.6%) instances where an iGel® was placed successfully, but then removed and an ETI was subsequently attempted, of which 20 (87%) ETIs were successful.
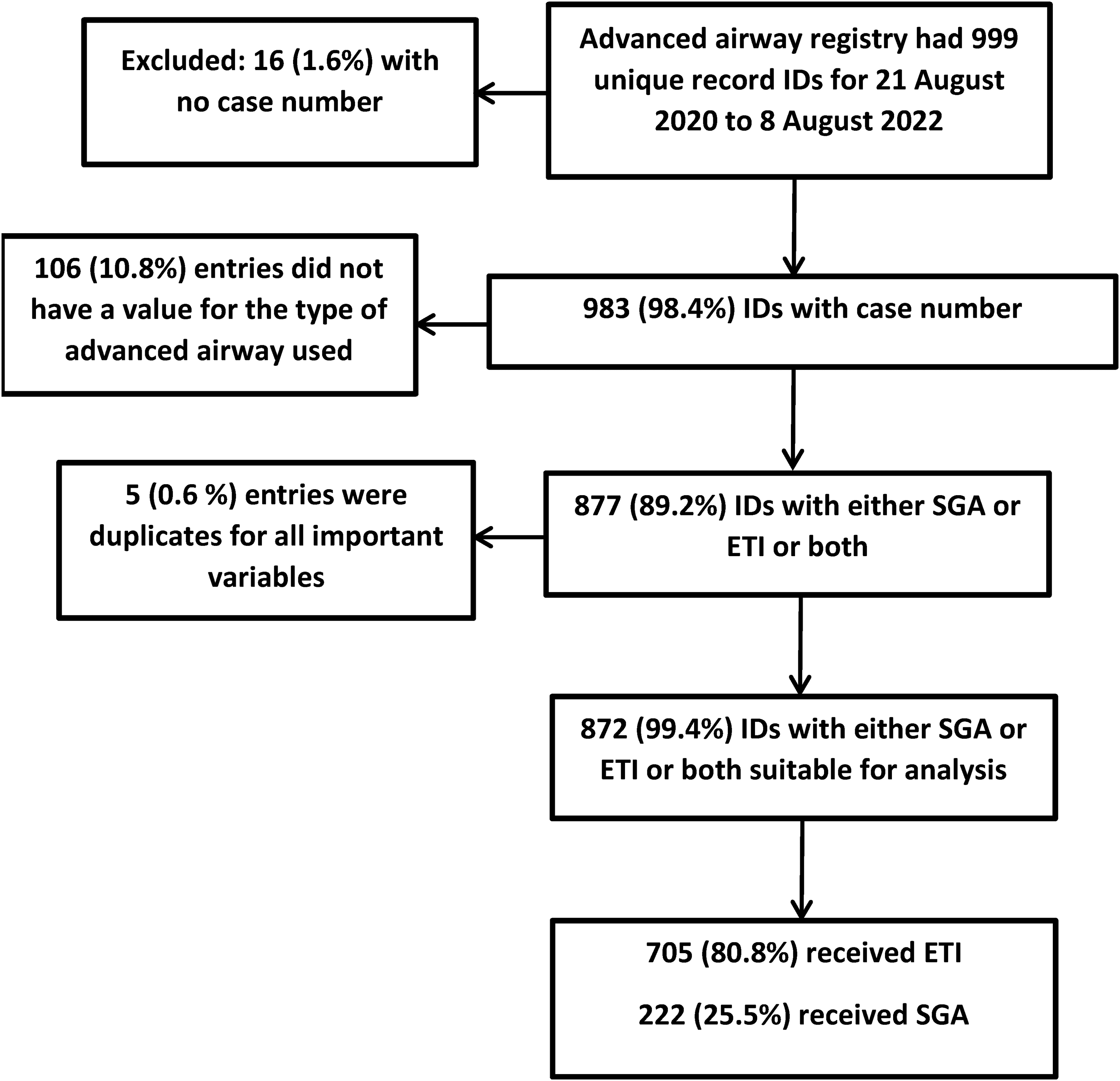
Selection of a cohort that had received paramedic advanced airways.
Demographic factors
Table 1 shows the patient level demographic and pre-advanced airway factors for all patients that received an advanced airway. Two-thirds of the cohort were male, and 96% of advanced airway uses were in cardiac arrest or when return of spontaneous circulation was present. Eight percent of patients were traumatically injured. The most common indications for advanced airway insertion were airway protection, inability to ventilate with an iGel® or bag-valve mask or a contaminated airway. Obese patients and limited neck movement were most strongly associated with difficult advanced airway management.
Patient, demographic, clinician and pre-advanced airway factors in 872 advanced airway uses (missing data excluded).
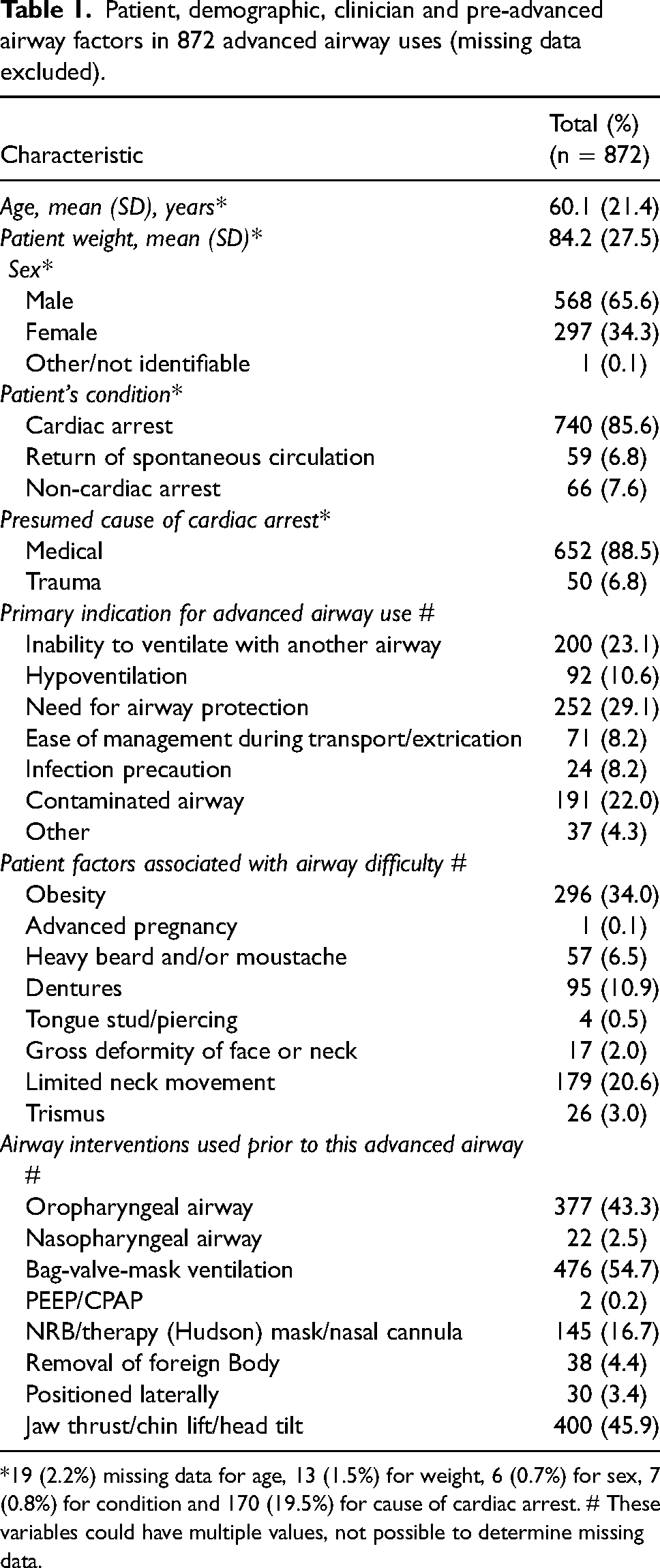
*19 (2.2%) missing data for age, 13 (1.5%) for weight, 6 (0.7%) for sex, 7 (0.8%) for condition and 170 (19.5%) for cause of cardiac arrest. # These variables could have multiple values, not possible to determine missing data.
ETI factors
Supplemental Table S1 tabulates airway factors in a cohort of 705 ETI patients. Sixty-two percent of intubations were performed in the location the patient was found and intubation was attempted in a moving ambulance in less than 2% of the cases. Most intubations were at ground level, with a supine patient and mostly with full access to the patient. Occipital pad and ‘ear-to-sternal notch’ were the most common airway positioning manoeuvres utilised. Nearly all intubations progressed with the use of an assistant. A view of the laryngeal inlet was obtained in 83% of ETI attempts (grade I or grade II), and 82% of intubations were performed using a video laryngoscope. Suctioning, head lift and ELM/bi-manual laryngoscopy use were common. Most clinicians used a bougie, and two-thirds used the video screen to confirm placement. Other methods of confirmation were used. More than 83% reporting the use of end-tidal CO2, and two-thirds reported auscultating for air entry and visualised chest rise. Chest compressions were interrupted in 41% of intubations during cardiac arrest, mostly between 10 and <30 s (as estimated by the paramedic). Almost 60% of clinicians report airway contamination during advanced airway attempts.
SGA factors
Supplemental Table S2 presents prognostic factors in a cohort of 222 iGel® uses. Supplemental Table S3 presents advanced airway factors. Most patients remained severely obtunded after airway management, with almost all having a Glasgow Coma Scale of three. More than 80% of airway attempts had no reported adverse events.
Machine learning analysis
A machine learning analysis and regression shows that numerous factors are associated with success for ETI (Figure 2 and Figure 3). The Cormack–Lehane airway grade influenced 48% of the chance of airway success in this model, with odds decreasing with increasing grade OR 0.21 (95% CI 0.15–0.28, P < 0.001). The patients’ age influenced 8% of the success and regression further showed that the OR 1.14 (95% CI 1.03–1.24, P = 0.007) with each extra decade of patient age. The type of laryngoscope (VL vs. DL) predicted 5% of influence with OR 2.9 (95% CI 1.8–4.6, P < 0.001) in favour of VL. The weight of the patient was influenced by 4% with a OR 0.91 (95% CI 0.85–0.98, P = 0.008) with each increasing 10 kg. The use of external laryngeal manipulation/bi-manual laryngoscopy was the fifth most significant factor explaining 4% with a OR 0.45 (95% CI 0.27–0.76, P = 0.03) against this technique. Finally, occipital padding had almost twice the odds of success, compared to a flat position OR 1.9 (95% CI 1.03–3.45, P = 0.03). Supplemental Figure S1 shows the ETI success stratified by airway grade, showing that this effect is more pronounced for grade III views.
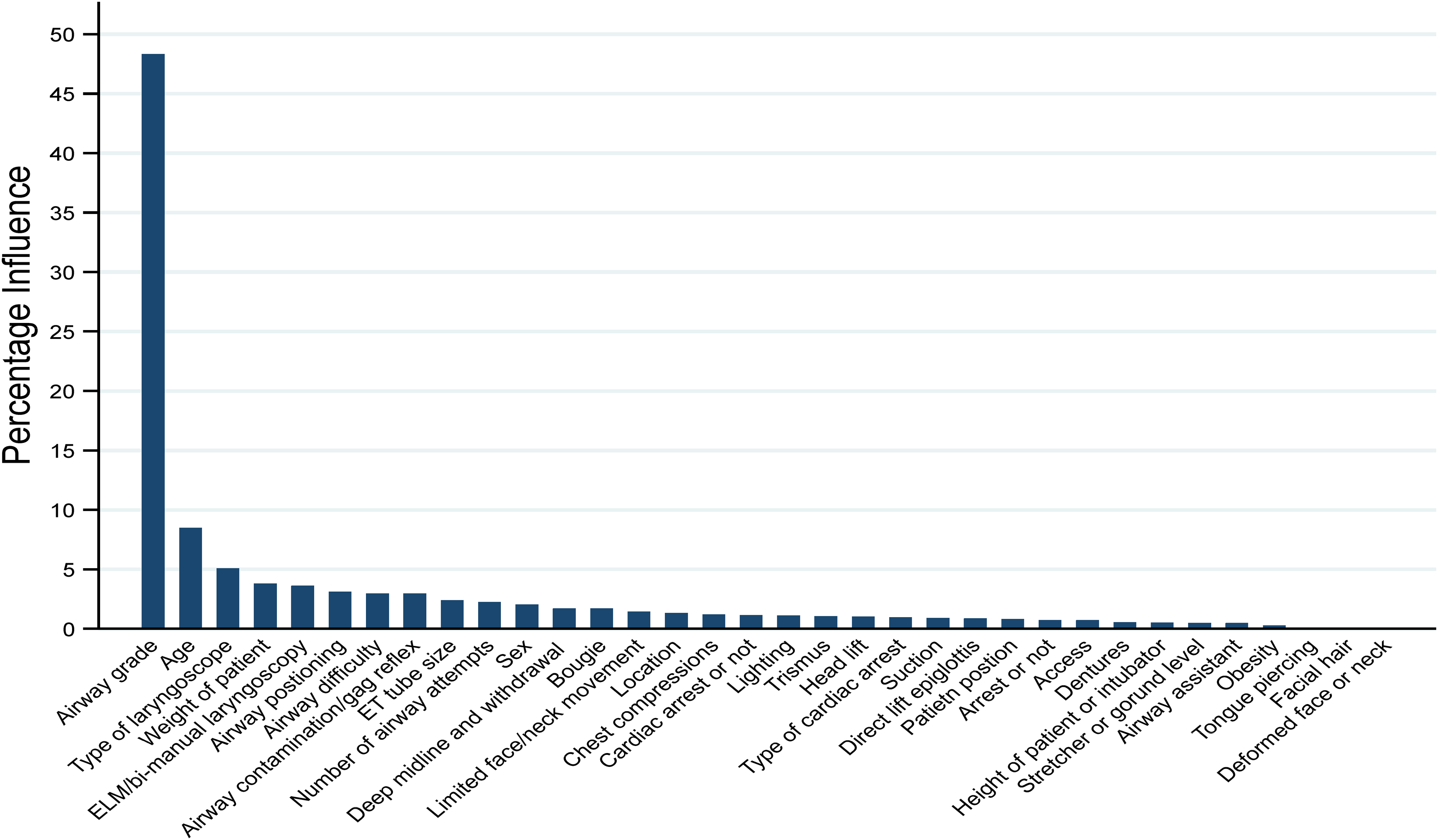
Factors that influence the probability of endotracheal intubation success, machine learning analysis.
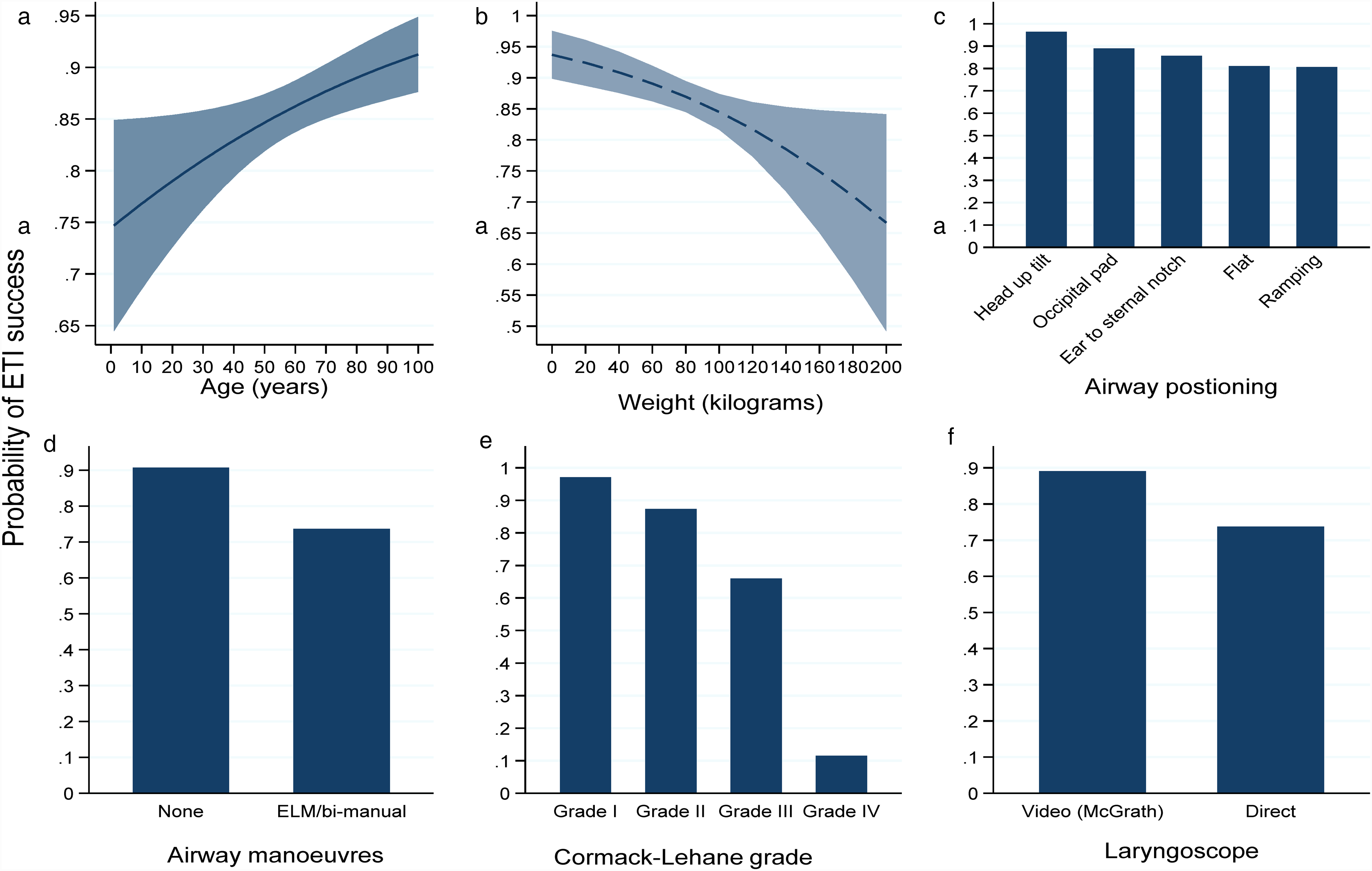
Top six factors that influence the probability of endotracheal intubation success, (a) age, (b) weight, (c) airway positioning, (d) airway manoeuvres, (e) airway grade and (f) laryngoscope type.
Time series analysis
A time series analysis shows that ETI first-pass and overall success improved during the study period. Overall ETI success increased by 0.15% per month (95% CI −0.07 to 0.36, P = 0.18) and first-pass by 0.6% (95% CI 0.09–1.1, P = 0.03) (Figure 4). During this time, a large increase in the percentage of all ETI that use VL was noted with a 0.6% per month rise (95% CI 0.2–1.1, P = 0.07). This increase in VL use strongly predicted increased ETI first-pass success by 0.35% per month (95% CI 0.11–0.60, P = 0.006). Similarly, the overall success for iGel® use increased by 0.87% per month (95% CI 0.65–1.1, P < 0.001) and iGel® first-pass by 0.88% (95% CI 0.63–1.1, P < 0.001). End-tidal CO2 usage during the study period did not increase significantly for ETI; 0.3% per month (95% CI −0.17 to 0.23, P = 0.78). Similarly, no significant improvements in end-tidal CO2 usage were noted for iGel® use; 0.45 per month increase (95% CI −0.26 to 1.1, P = 0.22).
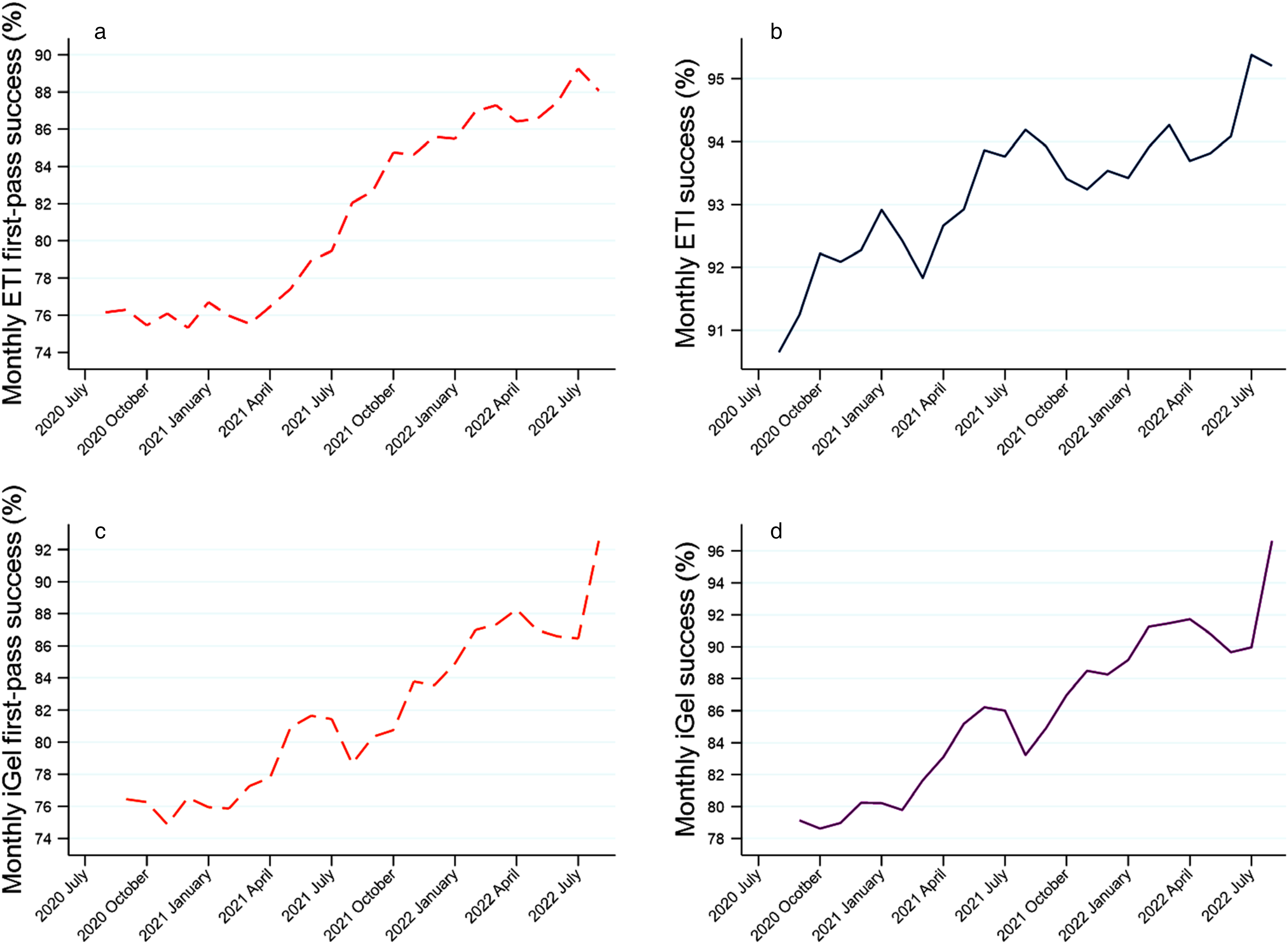
Time-series trends in (a) ETI overall, (b) ETI first-pass, (c) iGel overall and (d) IGel first-pass success during two-year study period.
Discussion
This analysis shows that during the first two years of the airway registry, first-pass success improved markedly, although increases in monthly overall success were less pronounced. Improved ETI success is likely explained by increased VL usage during the study period. An earlier comparison of the performance of VL relative to DL examined the first year's data from this registry. 15 This study showed that VL has better success compared to DL and that the chance of intubation first-pass success increased over time as the usage of VL rose. Therefore, the difference between VL and DL success and the strong predictive ability of temporal changes in the use of VL of success bolsters the case that VL might have caused ETI success to rise rapidly. A recent Cochrane review found improved success with VL use and makes the case that VL use increases success.15,24 The authors of the Cochrane review concluded that VL may reduce the number of failed intubations, particularly among patients presenting with difficult airways by improving the glottic view. 24 Additionally, that review indicated that VL may reduce laryngeal/airway trauma. 24
Of note, it is not only ETI success that rose over the two-year study period but also iGel® success increased. The cause for this is less clear – a possible explanation is that the airway registry promoted the increased awareness of advanced airway management and enabled self-reflection, which increased success for both ETI and iGel® use. No comparable research to compare these findings of increased success for iGel® was found in a literature search. During the study period, ICPs engaged in advanced airway training, which could also have contributed to increased proficiency. However, this training was during the first 12 months of the study period.
While advanced airway success has improved markedly during the study period, it should be noted that the 92.9% ETI success might be considered sub-par. The success proportions for ETI are well below 98% threshold that International Liaison Committee of Resuscitation (ILCOR) considers a good ETI success in cardiac arrest. Even so, this ETI success is much higher than that which ILCOR considers ‘low success’, which they define as the success from the PART and AIRWAYS2 trial (51.6% and 69.8%, respectively).9,10,25 The ILCOR recommends the use of SGA in settings with a low ETI success rate, and either ETI or SGA in high success settings. 25 The ETI success rate of NSWA falls between these two success poles defined by ILCOR. It is encouraging that the VL success is almost 95% and NSWA is promoting VL use as first-line technique. For this reason, and keeping in mind the trend of increasing success over time, it is believed that NSWA will soon approach the ILCOR benchmark for ‘good success’ for ETI.
Most findings in this analysis are concordant with the literature on advanced airway management. In this review age, weight, airway positioning, airway grade and the type of laryngoscope predict success.15,26–28 Moreover, an 83% use of end-tidal CO2 technology was reported. ETCO2 use is mandatory in NSWA and 100% was hoped for. It could be that all end-tidal CO2 use was not recorded accurately, or the technology was not available always, or perhaps some other reasons that are not clear. In NSWA, a concerted effort to increase the use (and recording) of end-tidal CO2 is underway. This study also revealed chest compressions were interrupted in 41% of intubations during cardiac arrest, mostly between 10 and <30 s. This was intentionally recorded in the airway registry as NSWA recommended that ICPs cease chest compressions during advanced airway management for all patients during the height of COVID-19. This was due to advanced airway management being deemed to be an aerosol-generating procedure. Since early 2022 pausing chest compressions has only been required for confirmed or suspected COVID-19 patients. Needless pausing of compressions is a problem. A study by Wang et al. found a median interruption for intubation of 47 s, which is a concern as guidelines emphasise treatment of cardiopulmonary arrest with continuous uninterrupted chest compressions. 3
Another noteworthy finding is that 1.2% of all ETIs had a gag reflex that made intubation difficult. Rapid sequence intubation is used by pre-hospital clinicians for intubation of patients with a gag-reflex as this technique suppresses the gag reflex and increases ETI success.2,29–31 It is plausible that the use of RSI in this subset of patient with gag-reflex might improve ETI success in NSWA. Moreover, the authors believe that the actual number of patients eligible for ETI with an intact gag-reflex is much higher than the numbers reported here, and that these patients are not receiving ETI attempts because of an intact gag reflex. The belief that there are many more such patients comes from comparing these statistics to that of other Australian emergency medical services that report hundreds of RSI per annum. 29 Almost all of the advanced airways used were in cardiac arrest, and this likely reflects paramedics reluctance to attempt airways in those with a gag-reflex. As such, there might be a role for RSI for NSWA.
It is noteworthy that this analysis found a relationship between the use of ELM/bi manual laryngoscopy and worse success, and that the poorest success using this technique was found among grade 3 views. This is not surprisingly given that these airway manoeuvres are only performed when sub-optimal laryngeal view is obtained.32–34 It is most likely that this technique is a marker for more complex airways and that these estimates are confounded. This model could not adjust for operator experience and other confounders. In NSWA, ELM/bi-manual laryngoscopy was taught and encouraged as a technique to improve suboptimal laryngeal view. Its presence as a risk factor needs to be considered in this context.
During the first two years of this registry, only ICPs entered data into the registry. NSWA has redesigned the registry and it has now been rolled out to all paramedics in NSWA who insert advanced airways. It is anticipated that this will result in many more advanced airways entered into the registry, especially iGel® which are used by the general paramedic workforce, increasing the utility of research stemming from this dataset. These results have public health implications. It shows that the use of high-quality registry data and the use of new technologies in addition to awareness and training can lead to improved advanced airway success.
Limitations
The airway use reported in this airway registry represents a segment of all the actual advanced airways used in NSWA. This analysis found that 63% of all ICP-led ETI s are captured in this registry during the study period. The lower number of entries in the registry can be explained by the newness of the registry and that only ICPs used the registry during this time. As such, the iGel® entries are low, because only ICPs entered data, and not the rest of the paramedics in NSWA. Entries were further limited by the ongoing on-boarding of ICPs in using the registry as they progressed through mandatory training for VL during the first year of registry use. Moreover, during most of the study period, ETI as an airway intervention was de-emphasised due to the COVID-19 pandemic. Finally, this study did not analyse iGel® in the machine learning analyses, for reasons described earlier.
Conclusions
This analysis of a new airway registry used by ICPs in New South Wales shows large increases in advanced airway first-pass success over the two-year period since its inception. Overall success improved, but not as markedly as the first-pass success. These increases can be explained in part by the awareness of airway management that results from the reflective practice of engagement in the airway registry, training and the increased use of VL.
Supplemental Material
sj-docx-1-pam-10.1177_27536386231175520 - Supplemental material for Lessons from the first two years of a new out-of-hospital airway registry in New South Wales
Supplemental material, sj-docx-1-pam-10.1177_27536386231175520 for Lessons from the first two years of a new out-of-hospital airway registry in New South Wales by Martin Nichols, Pieter Francsois Fouche, Thomas McPherson, Tom Evens and Jason Bendall in Paramedicine
Footnotes
Acknowledgements
The authors would like to thank Ms Sandra Ware, Dr Mathew Miller, Dr Clare Hayes-Bradley and Ms Clare Beech for their contributions to the formation of the NSW Ambulance Airway Register. The authors would also like to acknowledge the NSWA ICP Community of Practice.
Declaration of Conflicting Interests
Authors Pieter Francsois Fouche and Jason Bendall are members of the Editorial Board of Paramedicine. Fouche joined the Editorial Board October 2024 and Bendall joined the Editorial Board in November 2024, after the article had been published. Fouche and Bendall did not take part in the peer review or decision-making process for this submission and the authors have no further conflicts to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Correction (October 2025):
In this article, “Declaration of conflicting interests” section has been updated.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.