
Abstract
Background:
The goals of rehabilitation in knee osteoarthritis are adequate pain relief, functional improvement, and prevention of psychological deconditioning. Gait abnormalities in osteoarthritis patients have been studied using gait analyses. Genicular nerve block (GNB) is used for knee osteoarthritis (OA) related pain, but its impact on objective gait biomechanics remains underreported.
Aim:
To evaluate and compare spatiotemporal gait improvements at baseline and after 6 months of ultrasound-guided GNB in patients with knee OA using wearable sensor-based assessment.
Methods:
Fifty-one patients with knee OA (Kellgren–Lawrence Grade II-IV) who underwent ultrasound-guided GNB in the Department of Physical Medicine & Rehabilitation, AIIMS Jodhpur were assessed for cadence, affected knee propulsion, stance phase duration, and Timed Up and Go (TUG) using the G-Walk sensor pre and 6 months post-procedure. Statistical tests included paired t-tests, Wilcoxon signed-rank, and Mann–Whitney U Test.
Results:
Significant improvements in spatiotemporal gait parameters were observed at 6 months post-procedure compared to baseline. Cadence improved from 94.13 ± 9 to 109.02 ± 9.38 steps/min (P < .0001), propulsion from 4.47 ± 1.2 to 6.11 ± 1 W/kg (P < .0001), and stance duration from 57.8% to 59.9% (P < .0001). TUG time decreased from 19.12 to 12.67 seconds (P < .0001). Propulsion gain was lower in patients with comorbidities (P = .047).
Conclusion:
Sensor-based gait assessment offers an objective, quantifiable means to measure the impact of pain interventions in musculoskeletal rehabilitation. Pain alleviating interventions like GNB yield measurable gait improvements in knee OA. Adequate pain relief promotes active rehabilitation, enhancing biomechanics and mobility.
Self Declaration:
This is a secondary analysis of data previously collected as part of a published study on pain and quality of life outcomes post-genicular nerve block. The present study explores gait parameters using a novel approach not addressed earlier.
Keywords
Introduction
Osteoarthritis is the most prevalent degenerative musculoskeletal disorder in India, leading to significant functional decline. 1 Osteoarthritis is the second most common rheumatological disorder in the Indian population, affecting females more often than males. 2 An osteoarthritic joint is characterised by cartilage degradation, osteophyte formation, bone remodelling, and synovial inflammation which leads to joint pain, stiffness, restriction of range of motion, and loss of function. 3 Osteoarthritis commonly affects the hand, knee, and hip. Knee osteoarthritis is a major cause of impairment in mobility thus affecting vocational and avocational aspects of the patient subsequently.
According to the American College of Rheumatology (ACR), knee osteoarthritis can be managed non-pharmacologically and pharmacologically. While Total Knee Arthroplasty (TKA) remains the treatment of choice for advanced osteoarthritis (Grade IV according to Kellgren-Lawrence Grading), a multitude of therapeutic interventions can be offered to patients suffering from lower grades of the condition.4,5 ACR recommends the use of corticosteroid injections in knee osteoarthritis. However, conditionally recommends against the use of injectables like Hyaluronic Acid. 3 In recent years, targeting sensory innervation of the knee joint has gained popularity due to the ease of administration, non-invasive nature, and lasting effects on pain relief. Multiple randomised clinical trials have shown significant pain relief in knee osteoarthritis patients after Genicular Nerve Blocks (GNB).6 -10 Genicular Nerve Radiofrequency Ablations (GNRFA) have also been proven to provide long-term pain relief in such patients without any major side effects.7,11,12
The goals of rehabilitation in knee osteoarthritis are adequate pain relief, functional improvement, and prevention of psychological deconditioning. Gait abnormalities in osteoarthritis patients have been widely studied using observational and instrumental gait analyses. An increased gait asymmetry is linked to the severity of knee osteoarthritis particularly in stance phase duration and stride length. 13 Furthermore, reduced walking speed, due to pain and joint stiffness, may also lead to pathologies like lower cadence, reduced power generation by quadriceps and calf muscles. 14 Reduced range of motion on sagittal plane and reduced stance phase duration of the affected knee joint are strategies to mitigate dynamic instability of the osteoarthritic joint. 15
While several studies have evaluated GNB and GNRFA for subjective pain relief, few have investigated their impact on objective, sensor-based measures of gait and functional performance. This gap in the literature highlights the need to examine quantifiable changes in gait parameters following interventional pain procedures. The present study aimed to evaluate longitudinal changes in spatiotemporal gait parameters over 6 months following genicular nerve block in patients with knee osteoarthritis.
Materials and Methods
Study Design
The study employed a single-group pre–post quasi-experimental design without a parallel control group. It was conducted from June 2023 to December 2024 in the Department of Physical Medicine and Rehabilitation [PMR] at a tertiary care center in Western Rajasthan, India. The study protocol was approved by the Institute Ethics Committee and was registered in the Clinical Trials Registry-India [CTRI]. This study represents a secondary post hoc analysis of prospectively collected data from a previously published randomized controlled trial evaluating genicular nerve block in knee osteoarthritis. 10 Gait parameters were analysed as exploratory outcomes and were not pre-specified as primary endpoints in the parent study. Of the 180 participants enrolled in the parent trial, 51 had complete wearable sensor-based gait assessments at baseline and 6 months and were included in the present analysis. Reasons for exclusion included incomplete gait recordings, loss to follow-up, or technical errors during data acquisition. Inclusion criteria for the study were: individuals over 18 years of age with knee pain persisting for more than 3 months, a history of receiving conservative treatment for at least the same duration, and a diagnosis of knee osteoarthritis (KOA) based on the American College of Rheumatology (ACR) guidelines. Radiographic severity had to correspond to Grade 2 to 4 according to the Kellgren-Lawrence scale. The majority of participants had medial compartment involvement. A subset of Grade 4 KOA cases also showed patellofemoral joint changes; however, they were included only if they were not suitable candidates for total knee arthroplasty (TKA) or had declined surgical intervention. Exclusion criteria encompassed patients planning to undergo TKA, those with prior surgical procedures on the affected knee, individuals with coexisting diagnoses such as rheumatoid arthritis or other alternative explanations for knee symptoms, evidence of peripheral neuropathy, poorly controlled hypertension or diabetes, severe psychiatric or neurological disorders, and any history of bleeding disorders. An informed written consent for recruitment and publication of data was obtained from the patients. All patients underwent a pre-procedure evaluation during which an exhaustive clinical and demographic history was taken. The study adheres to the STROBE guidelines.
Procedure
The patients underwent a baseline gait evaluation (Walk and Timed Up-and-Go Test (TUG)) with the G-Walk wearable sensor based system. The findings were entered in the data collection form. Each subject was then administered a 3-point Ultrasound-guided Genicular Nerve Block targeting Superomedial (SMGN), Superolateral (SLGN) and Inferomedial Genicular Nerves (IMGN) was administered to the patients. The drug admixture consisted of 2 mL of lidocaine 1% (1.5 mL) plus 33 mg of triamcinolone (0.8 mL of triamcinolone 40 mg/mL) at each target site.6,10 The patients were called for follow-up 6 months later and gait evaluation was done. During the 6-month follow-up, participants continued to receive standard care for knee osteoarthritis as determined by their treating physicians, which may have included physiotherapy, exercise advice, analgesic medications, and lifestyle modifications. No protocolised rehabilitation programme was mandated as part of this secondary analysis.
Evaluation and Statistical Analysis
This study represents a secondary analysis of a subset of participants drawn from a larger observational study which has already been published. The current analysis focused on patients for whom complete pre- and post-intervention gait data were available. The study parameters were- Cadence (steps/minutes), affected knee propulsion (Watts/kg), affected knee stance phase duration (seconds), and TUG test duration (seconds). The study outcomes were measured at baseline and at 6 months after the procedure. IBM SPSS v25 was used for statistical analysis.
The following statistical tests were applied-
The association of the variables which were quantitative and not normally distributed in nature were analysed using Mann-Whitney Test (for 2 groups) and Kruskal Wallis test (for more than 2 groups) and variables which were quantitative and normally distributed in nature were analysed using Independent t test(for 2 groups) and ANOVA (for more than 2 groups).
Paired t-test for normally distributed data and Wilcoxon signed rank test for not normally distributed data were used to compare quantitative variables across follow up.
Normality of distribution was assessed using the Shapiro–Wilk test. Effect sizes (Cohen’s d for parametric comparisons and rank-biserial correlation for non-parametric comparisons) were calculated to quantify the magnitude of change. No correction for multiple comparisons was applied; therefore, findings should be interpreted with consideration of potential type I error.
For statistical significance, P value of less than .05 was considered statistically significant.
Results
Baseline Characteristics
The total sample size was 51 patients of which 33 (64.71%) patients were females and 18 (35.29%) were males. Distribution of body mass index (BMI) among the cases was as follows: 25 (49.02%) had BMI 25 to 29.99 kg/m2 (Obese I), 21 (41.18%) had BMI > 30 kg/m2 (Obese II), 3 (5.88%) had BMI 23 to 24.99 kg/m2 (Overweight) and 2 (3.92%) had BMI 18.5 to 22.99 kg/m2 (Normal BMI). Mean BMI was 29.41 ± 3.36 kg/m2, with median (25th-75th percentile) of 29.05 (27.48-31.658) kg/m2. Among comorbidities, 23 (45.10%) cases had low back pain (LBP), 15 (29.41%) had hypertension, 7 (13.73%) had knee effusion, 5 (9.80%) each had type II diabetes mellitus and hypothyroidism, and 1 (1.96%) had coronary artery disease. According to Kellgren–Lawrence (K-L) grading for knee osteoarthritis (OA), 29 (56.86%) cases were grade 3, 16 (31.37%) were grade 2 and 6 (11.76%) were grade 4. Mean ± SD (median [25th-75th percentile]) values were: age 58.86 ± 8.5 years (median: 59 [52.5-63.5] years), height 1.61 ± 0.1 m (median: 1.58 [1.52-1.685] m) and weight 75.56 ± 9.1 kg (median: 76 [68-82.2] kg; Table 1).
Demographic Characteristics Distribution.

Significant improvements were seen in gait parameters at 6 months compared to baseline (P value < .0001). Mean ± SD cadence (109.02 ± 9.38 steps/minute vs 94.13 ± 9 steps/minute), affected knee propulsion (6.11 ± 1 vs 4.47 ± 1.2) and median affected knee stance (59.9 [59-61.15]% vs 57.8 [56.25-58.75]%) at 6 months were significantly higher, while median tug test duration was significantly lower compared to baseline (12.67 [11.435-13.685] seconds vs 19.12 [14.83-24.92] seconds; Table 2).
Comparison of Gait Parameters Between Baseline and 6 Months.
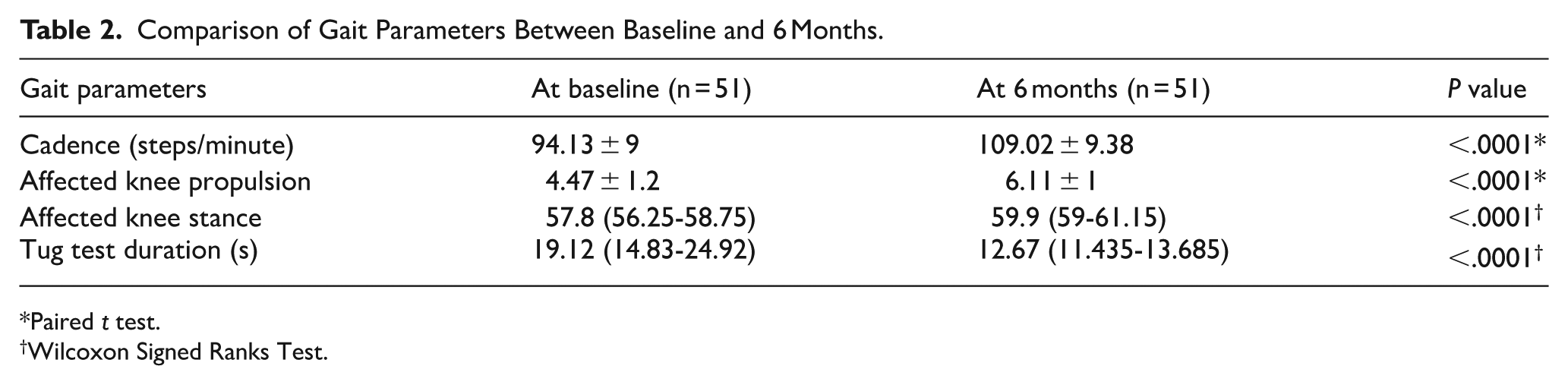
Paired t test.
Wilcoxon Signed Ranks Test.
No significant association was seen in affected knee propulsion with presence of comorbidities. Mean ± SD propulsion was 4.42 ± 1.11 Watts/kg vs 4.49 ± 1.27 Watts/kg at baseline (P value = .85) and 5.78 ± 1.04 Watts/kg vs 6.28 ± 0.95 Watts/kg at 6 months (P value = .089) in patients with vs. without comorbidities. Significant association was seen in propulsion improvement at 6 months (P value = .047), with significantly lower improvement in patients with comorbidities (median 1.2 [1-1.875] Watts/kg) compared to those without comorbidities (1.64 [1.4-2.5] Watts/kg; Table 3).
Association of Affected Knee Propulsion with Presence of Comorbidities.

Independent t test.
Mann–Whitney test.
Discussion
The present study demonstrates that significant longitudinal changes in gait parameters were observed over 6 months following genicular nerve block, which were measured using wearable sensor-based technology. These findings support the functional impact of pain reduction following Genicular Nerve Block, beyond subjective relief; and also indicate measurable changes in functional gait characteristics during the post-intervention period.
Knee pain has been associated with reduced quadriceps strength, potentially due to reflex arthrogenic muscle inhibition triggered by pain during strength assessment. Although pain outcomes were not analysed in this secondary evaluation, knee pain has been associated with reduced quadriceps strength, potentially due to reflex arthrogenic muscle inhibition. 16 Reduction in nociceptive input may therefore contribute to improved limb loading and propulsion; however, in the absence of contemporaneous pain data, a direct mechanistic linkage cannot be established. The observed increases in cadence and propulsion may reflect improved confidence in limb loading, behavioural adaptation, or enhanced participation in daily activities following intervention.
Affected knee propulsion (Watts/kg) represents a wearable sensor–derived estimate of limb-level propulsive power during late stance, normalised to body mass. This parameter is algorithmically derived from inertial data and reflects an estimate of propulsion rather than direct joint-specific kinetic measurement obtained from force plate–based gait laboratories. Postural stability, balance, and mobility are a complex function maintained through coordinated neuromuscular responses regulated by the central nervous system. 17 A reduction in the absolute stance phase time is considered to reflect an antalgic gait. However, an increase in the relative stance phase represents an abnormal gait pattern that usually characterizes knee OA in patients. Reduced absolute stance time is typically associated with antalgic unloading of the affected limb, whereas increased relative stance duration has also been described in osteoarthritis due to slower walking velocity.14,18,19 An increase in stance phase duration following genicular nerve block suggests improved weight-bearing tolerance and limb stability during gait. This change likely may reflect reduced pain-related unloading of the affected limb, allowing more symmetrical and efficient gait patterns. Prolongation of stance phase duration is commonly interpreted as improved limb support and load acceptance, reflecting enhanced joint stability and neuromuscular control during single-limb support. In knee osteoarthritis, pain-related antalgic gait typically manifests as reduced stance time on the affected limb; normalization of stance duration therefore suggests attenuation of pain-avoidance strategies and restoration of more physiological gait mechanics. 20 While increased relative stance phase has been described in knee OA due to reduced gait velocity, the post-intervention increase observed in this study, alongside improved cadence and propulsion, likely may reflect improved limb loading rather than pathological gait adaptation. Nevertheless, causal attribution to the intervention cannot be made given the study design.
Timed-Up-and-Go (TUG) test is a reliable measure of functional mobility, balance, and walking ability in patients with knee osteoarthritis. Thus, improvements in TUG test duration after GNB demonstrate enhanced functional mobility, dynamic balance, and transitional movement efficiency. It also indicates increased confidence in ambulation and reduced mobility-related limitations in daily activities. Notably, improvement in propulsion was lower in patients with comorbidities, suggesting that systemic health status may modulate functional gains post-intervention.
Importantly, sustained gait changes at 6 months are unlikely to reflect a prolonged pharmacological effect of local anesthetic or corticosteroid injection alone. Rather, these changes may represent downstream effects such as improved engagement in rehabilitation, behavioural modification, reduced fear-avoidance strategies, or other concurrent management approaches during routine care. While prior studies have primarily focused on pain-related outcomes following Genicular Nerve Block, only 1 study to date has evaluated its biomechanical impact using sensor-based gait analysis. To our knowledge, the present study is the second to assess gait outcomes after Genicular Nerve Block and the first to report sustained functional changes at a 6-month follow-up.
Our study highlights the ease of access, feasibility, and role of wearable sensor based gait analysis before and after interventions targeting pain relief in musculoskeletal conditions directly affecting gait parameters. Wearable sensor-based gait analysis offers a practical method for objective assessment in outpatient rehabilitation settings. Unlike laboratory-based motion analysis systems, inertial sensors allow evaluation in real-world clinical environments, enhancing ecological validity. Their integration into interventional rehabilitation assessment may improve quantification of functional trajectories over time. Wearable sensor-based gait analysis allows objective assessment across real-world clinical environments, making it particularly suited for rehabilitation settings.21,22 The growing accessibility of inertial sensors enables clinicians to better understand lower limb biomechanics and pathomechanics during daily activities, strengthening functional outcome assessment in interventional rehabilitation.
The ultimate goal of pain-alleviating procedures is to provide longer lasting outcomes and patient satisfaction. When linked with functional improvements, the credibility of these minimally invasive procedures increases manifold and provides a solid platform to work towards functional rehabilitation. Pain management and rehabilitation approaches have historically emphasized different therapeutic targets, with pain medicine focusing primarily on symptom reduction while rehabilitation programs prioritise restoration of function through graded activity and behavioural strategies. 23 Integrating pain medicine with objective functional gains reinforces the role of interventional pain management as a meaningful component of comprehensive rehabilitation. It is important to not look at Pain Medicine/Interventional Pain Management as a field overshadowing other subsets of rehabilitation, rather an important adjunct to the meaningful medicine we practice.
Limitations
The present study has certain limitations. First, the quasi-experimental single-arm design without a control group limits causal inference regarding the observed gait improvements. Second, gait assessment was restricted to selected spatiotemporal parameters rather than comprehensive kinematic or kinetic analysis. Third, the sample size was modest, which may limit the generalisability of the findings. Additionally, this was a secondary analysis of an existing dataset and was not originally powered with gait outcomes as the primary endpoint. Pain scores corresponding to gait assessment time points were not available for this secondary analysis, limiting mechanistic interpretation. Additionally, co-interventions during the 6-month follow-up period were not standardised, and may have influenced observed outcomes. The use of wearable inertial sensors, although validated and clinically feasible, does not provide the detailed joint-level information available from laboratory-based motion analysis systems. Finally, follow-up was limited to 6 months, and long-term sustainability of the observed gait changes could not be assessed.
Conclusion
Genicular nerve block is associated with significant improvements in objective spatiotemporal gait parameters in patients with knee osteoarthritis. Beyond pain relief in the knee joint, these findings suggest that pain-relieving interventions may facilitate improved weight-bearing, gait efficiency, and functional mobility, thereby enabling more effective participation in rehabilitation. Improved gait parameters also help increase confidence, and has a psychological component attached to overall well-being of the patients. Wearable sensor-based gait analysis offers a practical and objective approach to evaluating functional outcomes following interventional pain procedures.
In this secondary analysis of a single-arm cohort, wearable sensor-based gait assessment identified significant longitudinal changes in spatiotemporal parameters over 6 months following genicular nerve block in patients with knee osteoarthritis. While causal inference cannot be established, the findings highlight the potential utility of objective gait metrics in capturing functional trajectories during routine interventional pain management. Integration of wearable sensor technology may enhance functional outcome assessment within rehabilitation-oriented care. Future controlled studies with larger samples and standardized follow-up protocols are warranted. Studies should explore the molecular pathways involved in joint proprioceptive dysfunction and pain processing, and their modulation following pain-alleviating interventions. Future randomised controlled studies with larger samples and longer follow-up periods are warranted to further elucidate the role of genicular nerve block in optimizing functional recovery in knee osteoarthritis.
Footnotes
Acknowledgements
The authors would like to thank the patients who participated in this study. We also acknowledge the support of the doctors and staff of Department of Physical Medicine and Rehabilitation, AIIMS Jodhpur, for facilitating data collection and clinical assessments. We thank the technical staff and physiotherapists involved in patient coordination and gait assessment.
Ethical Considerations
The study was approved by the Institutional Ethics Committee of All India Institute of Medical Sciences, Jodhpur (AIIMS/EIC/2022/4201). Written informed consent was obtained from all participants prior to enrolment in the study. The original parent study was registered with the Clinical Trials Registry of India (CTRI/2023/06/054401) with registration date of 26/06/2023.
Consent to Participate
Written informed consent was obtained from all participants prior to participation in the study.
Consent for Publication
Written informed consent was obtained from all participants for the publication of anonymized data and result.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analysed during the current study are not publicly available due to institutional and ethical restrictions but are available from the corresponding author on reasonable request.