
Abstract
Introduction:
Percutaneous tenotomy is an emerging, minimally-invasive procedure to treat muscle and tendon contractures, including those resulting from spasticity. Such contractures often cause pain, functional impairment, impact quality of life and may not respond to conservative or medical therapy. Further, spastic contractures typically affect frail, older patients unsuitable for management with open surgical procedures. We undertook the first PRISMA-compliant systematic review exploring use of percutaneous tenotomy to manage contractures occurring in the context of spasticity in adults.
Methods:
We searched 6 databases for primary research papers featuring an entirely adult sample undergoing percutaneous tenotomy, published in either English or French. Quality assessment was performed using the Oxford Centre for Evidence-Based Medicine Scale and the Methodological Index for Non-Randomized Studies. Synthesis of included study data was performed where possible.
Results:
Six studies were included, reporting 160 patients undergoing more than 430 tenotomies to 27 different tendons. All were low quality. Synthesis of evidence across studies indicated that percutaneous tenotomy has a low complication rate and may support patients to obtain a range of post-operative goals, including improved skin hygiene, ease of patient care and joint range. However, synthesis across studies was limited by heterogenous patient assessment and poor reporting.
Conclusion:
This review found some evidence supporting the safety and efficacy of percutaneous tenotomy in adults with contracture, but higher-quality studies are required. Further work should standardise the approach and reporting of these procedures to facilitate evidence synthesis and to develop best practice.
Keywords
Introduction
Percutaneous tenotomy (PCT) is an emerging minimally invasive procedure used to treat muscle and tendon contractures particularly in patients with spasticity; a velocity-dependent increased muscle tone resulting from insults to central motor systems.1,2 Regardless of aetiology, this chronic increased tone can result in shortening of the affected soft tissues, and leading to contracture. Spastic contractures can cause pain, lead to skin lesions or maceration, prompt difficulties in limb positioning and impair hygiene, dressing, grip or gait. 3 This can significantly impact patients’ quality of life.
Such contractures often result from failure of conservative treatments, including physical therapy, orthoses or pharmacological therapy, including chemodenervation. However, several studies have demonstrated the effectiveness of PCT in improving range of motion in spastic joints and reducing patient pain, indicating its potential as an additional intervention to manage contracture.3 -8
Tenotomy techniques range from total tenotomy, in which complete sectioning of the tendon results in permanent loss of function of the targeted muscle, to hemitenotomy, in which 2 hemisections of the tendon are made at different locations. 9
Compared to conventional surgical approaches, percutaneous tenotomy appears to offer potential advantages such as enabling procedures to be performed under local anaesthesia, reduced surgical trauma, reduced complications, shorter recovery times and hospital stays, and improved patient satisfaction. As such, it could offer a viable alternative to conventional surgery in frail patients with neurological conditions. Additionally, PCT has been applied to various tendons with positive outcomes.7,8
Despite its clinical utility, the application of PCT in spasticity management is still evolving, with varying protocols and outcomes reported across studies. 3 Reported procedures are heterogeneous and practitioner dependent. One previous systematic review has explored the efficacy of tenotomy but had very broad inclusion criteria. It included both cadaveric studies, and studies reporting both open and percutaneous tenotomy, which prevented the authors from undertaking any synthesis of obtained data.
Here, therefore, we undertake the first systematic review specifically exploring the use of PCT in adult patients with spasticity in an outpatient clinic setting, considering its potential indications, procedural techniques, clinical outcomes, and associated complications. Additionally, the study seeks to provide a comprehensive review of existing evidence to support the integration of this technique into multidisciplinary spasticity management programmes.
Methods
Search Strategy
Our systematic review was undertaken in line with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendations. 10 It was pre-registered with the PROSPERO database (ID: CRD42024560139). A search of 6 databases was undertaken (Medline, Embase, The Cochrane Library, Web of Science, CIHNAL and PEDro) to 9th September 2025. Tailored search strings including relevant key words connected (eg, ‘percutaneous tenotomy’, ‘spasticity’, ‘thumb-in-hand’) with Boolean operators were used to search each database.
Our search was not restricted to any specific timeframe. To increase search yield, the references of any articles undergoing full-text review also had their references screened to identify any further potentially eligible studies. The search strategy is summarised in Figure 1.

PRISMA flow chart showing selection of included studies.
Inclusion and Exclusion Criteria
Titles and abstracts were independently screened by 2 authors (IJB and AS for English language abstracts, JD and EB for French language abstracts) to identify eligible studies. The same authors then independently reviewed article full-texts to determine suitability for inclusion.
Inclusion criteria were: (1) a primary research paper (including case reports) detailing the percutaneous use of a needle to perform a soft tissue release to manage contracture following spasticity, (2) an available full-text, (3) publication in English or French and (4) an all-adult sample (all patients age >16 years). Cadaveric studies, conference abstracts and papers performing tenotomy to manage non-spastic pathologies were excluded.
Any disagreement between authors as to an article’s suitability for inclusion was resolved through arbitration by a third author (AP).
Quality Assessment
Two authors (IJB and AS for English language abstracts and JD and EB for French language abstracts) independently assessed the evidence quality by each eligible study using the Oxford Centre for Evidence-Based Medicine Scale 11 and the Methodological Index for Non-Randomized Studies (MINORS) tool. 12 The latter was chosen for its suitability in evaluation of non-comparative studies, good test-retest reliability and wide use across orthopaedic systematic reviews. 14
The MINORS features 12 items, 4 of which are only relevant to comparative studies. Each item is scored 0 (not reported), 1 (reported but inadequate) or 2 (reported and adequate), combining to a maximum score of 24 for comparative and 16 for non-comparative studies. Higher scores indicate higher study quality. Details can be found in Table 1. Any discrepancy between reviewer scoring was resolved through a third author’s arbitration (AP).
The MINORS Score.

Data Extraction
All eligible English language manuscripts were reviewed independently by IJB and AS, whilst eligible French language manuscripts were reviewed JD and EB. The following data were extracted: (1) study design, (2) study aim, (3) patient demographics (inc. sample size, sex, age, underlying UMN pathology, cognitive capacity, time since spasticity onset), (4) presenting spasticity-related deformity, (5) indication for tenotomy, (6) details of tenotomy technique and tendons targeted, (7) post-operative management plans, (8) primary aim of tenotomy, (9) post-operative outcomes, (10) details of patient follow up and (11) reoperation/complication rates.
Each reviewers’ extracted data was then compared, and discrepancies resolved with reference to the original manuscript.
Results
Searches of Medline, Embase, The Cochrane Library, CIHNAL and PEDro yielded 1517, 934, 113, 162 and 13 results respectively. After removal of duplicates 2016 references remained, of which 73 were identified as suitable for full-text review. Manual review of eligible studies’ references yielded no further eligible papers. A total of 6 studies were finally included (see Table 2).
Included Studies.

Abbreviations: NR, not reported; CVA, cerebrovascular accident; CP, cerebral palsy; MS, multiple sclerosis; TBI, traumatic brain injury; ABI, anoxic brain injury; SCI, spinal cord injury; ALS, amyotrophic lateral sclerosis.
Most of the included studies were case series (n = 4) and graded as OXFORD Level IV evidence. 11 Three of these were retrospective and 1 prospective. 7 Two case reports were also included (OXFORD Level V evidence). The average MINORS score for included studies was 6.8 (range 2-11).
Study Participants
A total of 169 patients were included in the studies eligible for inclusion. Of these, 9 patients reported peripheral rather than central nervous system lesions underlying their contracture (8 belonging to a retrospective trial 3 and 1 to a prospective study 4 and where therefore excluded, leaving a final total sample of 160 patients.
The mean study sample size was 27 patients (range 1-77 patients). 46% of patients were male. Mean patient age was 48.0 years (range 20-97). The neurological condition resulting in spasticity was reported in all but one study 6 (n = 18). Most commonly, spasticity resulted from CVA (n = 65, 40.6%), Cerebral Palsy (n = 17, 10.6%), and TBI (n = 15, 8.8%). Patients’ cognitive capacity was reported in 5 studies. 4 studies (n = 46) explicitly reported capacity to consent to treatment, with 10 of 46 patients having capacity (22%).
Indication for tenotomy was reported in all studies. Most commonly, intervention was indicated to address contractures resulting in a non-functional limb (n = 3 studies). In 3 studies (n = 140), patients’ unsuitability for general anaesthetic or open surgery was explicitly cited as an indication for PCT. Intervention aims for individual patients were reported in all studies, often with more than 1 goal being attributed to each patient’s procedure. Most commonly, procedures were performed to improve patient gait (n = 79, 49%), reduce pain either at rest or when walking (n = 57, 36%), or reduce risk of skin damage (n = 32, 20%).
Time between UMN injury and operative management was poorly reported and only detailed in 2 studies, both of which were case reports.
Interventions
The tendons targeted during tenotomy were reported in 5 studies. The remaining study instead reported the number of limbs targeted. 4 However, in 2 of the 5 studies reporting which tendons were targeted, the exact number of tenotomies performed could not be determined due to lack of reporting detail (eg, procedures were reported as tenotomy of ‘finger flexors’, without specifying the number of flexors sectioned). One study grouped less commonly performed tenotomies together as ‘other’ tenotomies, which also limited synthesis. 3 Total tenotomies across the included studies can be found in Table 3. Overall, the most performed tenotomies targeted finger flexors (34 hands), toe flexors (95 feet), and knee flexor tendons (n = 44).
Summed Tenotomies Across Studies for Each Tendon.

The exact number of tendons was not specified in papers reporting percutaneous tenotomy to finger and toe flexors.
There was significant variation reported in tenotomy technique across included studies. The background and training of the operating clinician was only reported in a single study. 4 Three studies reported the location where procedures were conducted, most commonly in the patients’ own nursing home (n = 2).
Local lidocaine injection was the most commonly used form of analgesia (n = 3). Only 2 studies reported use of sedation during the procedure.3,13 Three studies reported use of a topical antimicrobial prior to tenotomy, most commonly povidone-iodine (n = 2). Tenotomy needle gauge was reported in 5 cases and varied across studies.
Tendon identification was reported by 5 studies, in 4 of which identification was achieved through palpation of the tendon alone. Both palpation and ultrasound guidance were used in the remaining reporting study. 14 Tenotomy technique was reported in 5 studies. Four reported insertion of the tenotomy needle perpendicularly to the tendon of interest. Two techniques were described across studies; tendons were either severed via repeated advancement and retraction of the needle (3 studies) or repeated movement of the needle in a lateral shearing motion (2 studies). Reported procedure duration ranged from less than 10 to 40 minutes. Further details can be found in Table 4.
Details of PCT Procedure Technique Across Studies.
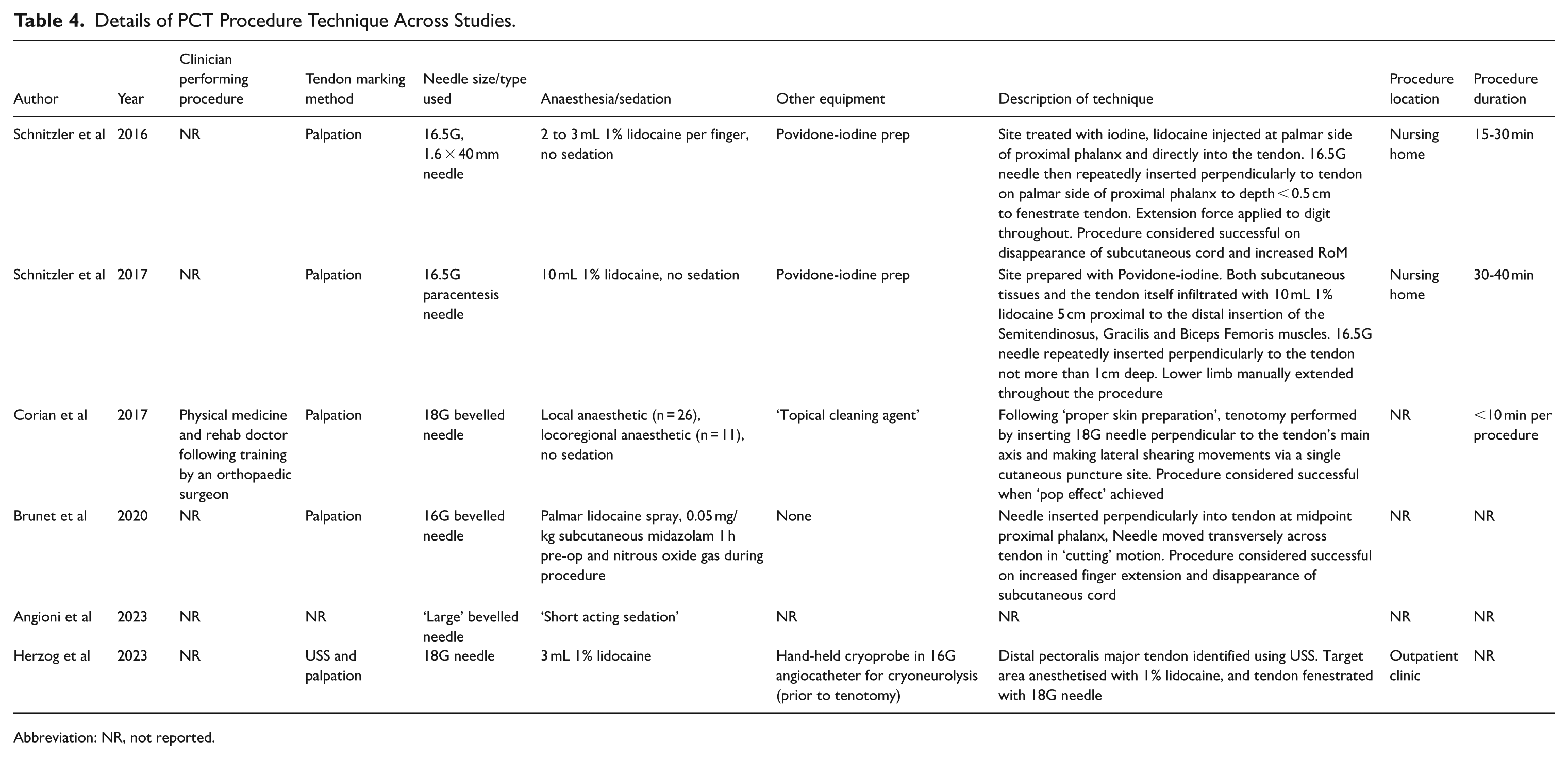
Abbreviation: NR, not reported.
Importantly, in one study tenotomy was used in combination in cryoneurolysis to manage contracture, 14 confounding assessment of the efficacy of each technique used.
Outcome Measures
A mean of 2 different outcome assessments were performed per study (range 1-3). Outcome measure use is summarised in Table 5. Across studies, the most used outcome measure was passive range of movement (pRoM; n = 5), followed by Goal Attainment Scaling (GAS; n = 3). Mean changes in pRoM pre/post-operatively, synthesised where possible, are presented in Table 6.
Aims, Outcomes and Complications of PCT Across Studies.
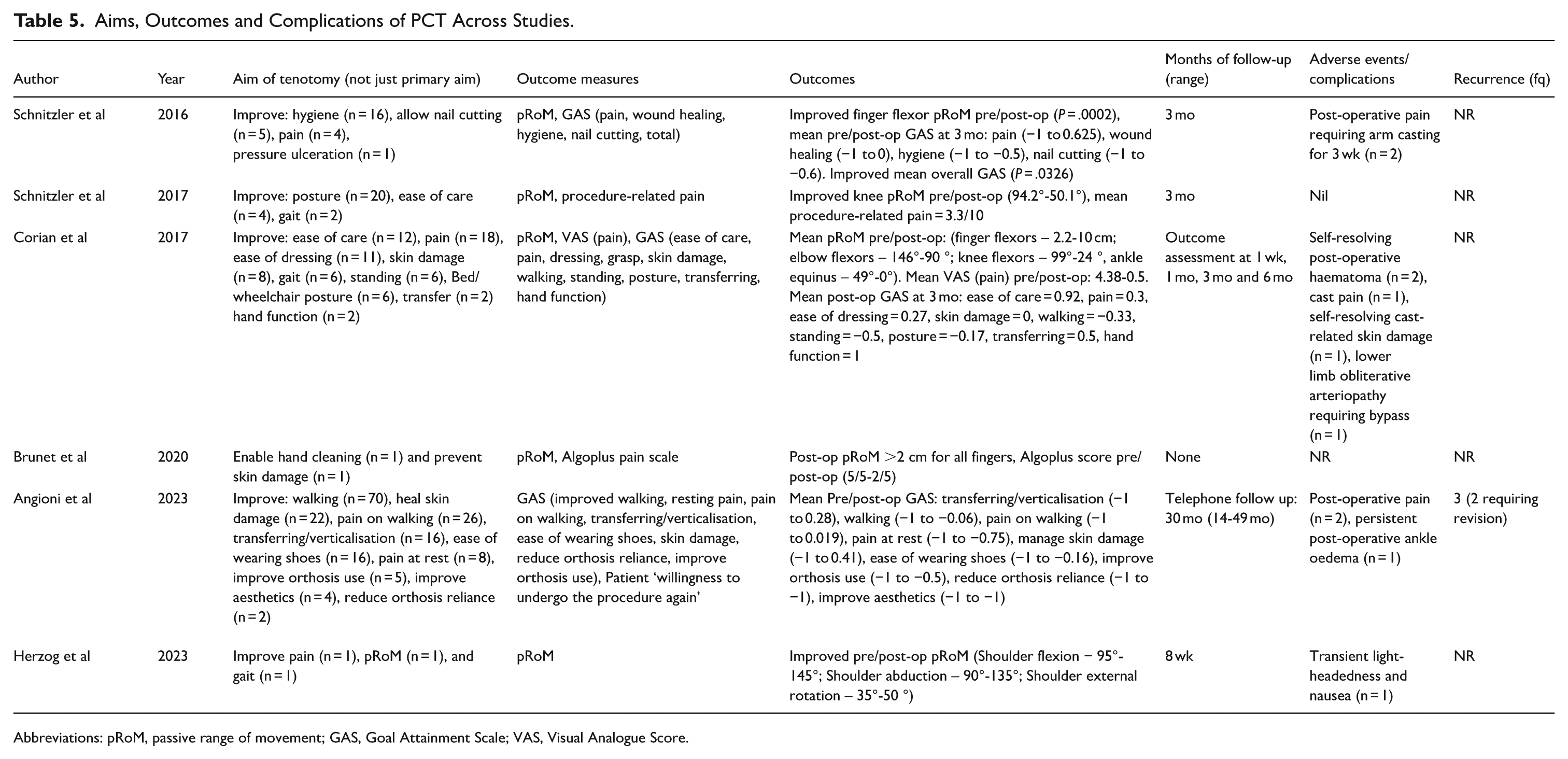
Abbreviations: pRoM, passive range of movement; GAS, Goal Attainment Scale; VAS, Visual Analogue Score.
Synthesised Passive Range of Motion (pRoM) Change Pre Versus Post-Operatively Across Studies.

The most common goals measured using GAS were reduction in pain, improved hygiene and reduced skin damage (n = 3). Mean post-operative GAS scores, where studies could be synthesised, are shown in Table 7. Notably, across studies, there was a greater success in achieving passive function outcomes than active function. Only one study collected pre-tenotomy baseline data to enable significance testing comparing pre- and post-operative assessment scores. 5 They reported a statistically significant increase in finger flexor pRoM (P = .0002) and improvement in GAS scoring (P = .0326) following tenotomy.
Synthesised GAS Scores Across Studies. GAS = Global Attainment Scale.
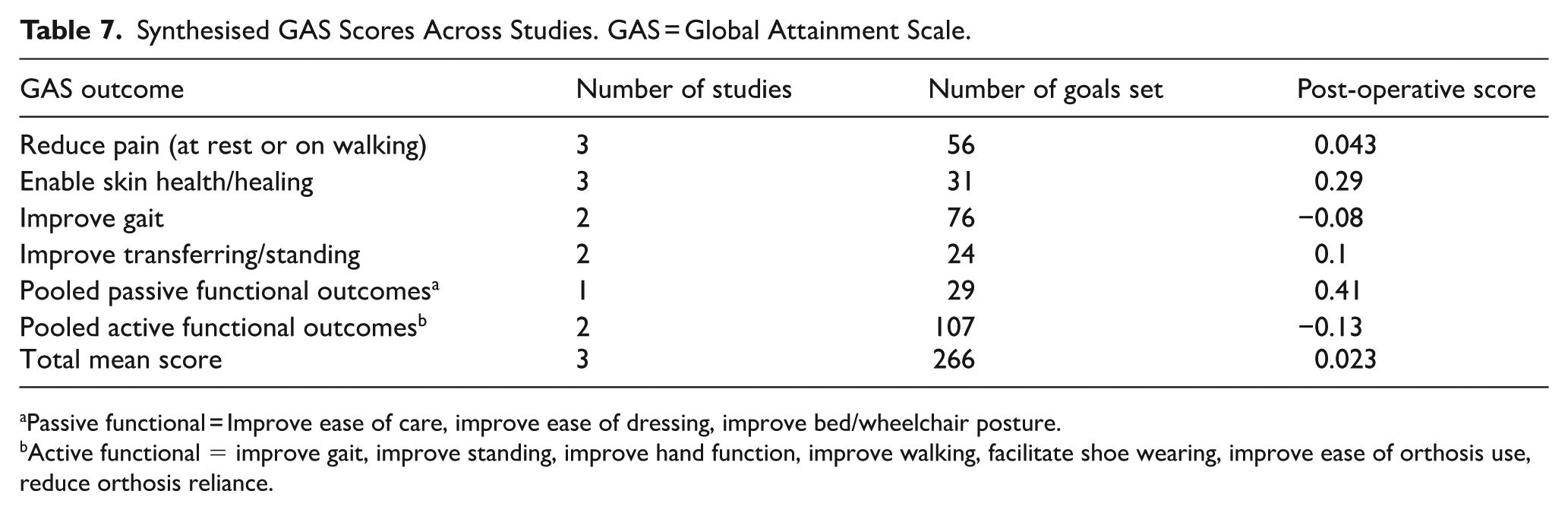
Passive functional = Improve ease of care, improve ease of dressing, improve bed/wheelchair posture.
Active functional = improve gait, improve standing, improve hand function, improve walking, facilitate shoe wearing, improve ease of orthosis use, reduce orthosis reliance.
Follow-Up and Complications
Five studies reported follow-up duration, with a mean of 7 months (range 0-49). Five studies reported adverse events or complications, with 11 adverse events in total, resulting in an overall reported per-patient complication rate of 6.9%. Ten of these were minor, classified as Grade I according to the Clavien-Dindo Classification. 15 The most reported adverse event was post-operative pain (n = 5), followed by self-resolving post-operative haematoma (n = 2). A single major complication was reported: cutaneous necrosis in a patient with previously undiagnosed lower limb obliterative arteriopathy, requiring bypass. This was classified as Clavien-Dindo Grade IIIb. 4
Only one study provided data on recurrence, reporting 3 instances of recurrence (3.8%) within 3 months postoperatively. 3 Two of these required revision procedures, both following toe flexor tenotomy, resulting in a study reoperation rate of 2.6%. Details on follow up and complications are presented in Table 5. Importantly, no cases of novel post-operative deformities were reported, which contrasts with findings from other spasticity-management procedures. 16
Discussion
Contracture is a common cause of functional impairment, pain and reduced quality of life amongst patients with spasticity. Typical spasticity-managing treatments, including physiotherapy, orthoses and botulinum toxin, are often ineffective for management of contracture. As such, there is a need for novel, safe and effective treatments for spasticity-related contractures. Percutaneous tenotomy may represent such an approach to contracture management, particularly amongst patients unsuitable for the general anaesthetic often required for open surgical procedures.
This systematic review is the first to specifically evaluate the evidence base for percutaneous tenotomy under local anaesthetic as a management for contractures resulting from spasticity in adults. It is unique in the literature due to its focus solely on (1) a living adult population, (2) spasticity as an underlying pathology, (3) local anaesthetic procedures performed outside the operating theatre environment. This group differs from paediatric patients with spasticity-associated contracture due to its greater burden of comorbidities, different common spastic aetiologies and situation in different social and healthcare contexts. Further, this older patient group is both growing in size and associated with significant healthcare and economic burdens, leaving it of particular interest. Inclusion of both paediatric and adult patients was a common reason for study exclusion from this review.
This review included 6 studies. However, as is typical in reviews of novel interventions, evidence for percutaneous tenotomy is limited by its poor quality. Heterogenous and incomplete reporting across studies prevented substantive synthesis of findings, and only a single study reported significance testing. 5
Four studies were graded OXFORD Level IV, with the remaining 2 graded OXFORD Level V. Small sample sizes limited study quality and perhaps reflect a lack of awareness of these procedures, despite the significant numbers of patients to whom they may offer benefit. It may also indicate lack of integration of surgical expertise into multi-disciplinary neurorehabilitation teams, lack of consensus surrounding appropriate technique for these procedures and over-estimation of the procedures’ risks, as has been hypothesised for other spasticity-managing procedures. 16 Supporting rehabilitative clinicians to either complete surgical referrals, or themselves offer, percutaneous tenotomy should be a key clinical and research priority to increase availability and understanding of these procedures.
Patient Population
160 patients were included in this review’s 6 studies, of which the mean age was 48.0 (range 20-97) and 46% of patients were male. Spasticity resulted mainly from CVA (n = 65, 40.6%), Cerebral Palsy (n = 17, 10.6%), and TBI (n = 15, 8.8%). Time between central nervous system injury was on average between 5 and 16 years. Patients’ cognitive capacity to consent to treatment was explicitly reported in 4 studies, whilst the remaining 2 studies made no reference to cognitive capacity or procedure consenting. Of the 46 patients included in those studies reporting capacity, 10 were reported to have capacity to consent to the procedure (22%). These characteristics confirm that PCT may be particularly of value in managing contractures in frail patients unsuitable for general anaesthesia.
Intervention aims for individual patients were reported in all studies. Patients had 1 or more goals for their procedure, most commonly to: improve gait (n = 79, 49%), reduce pain either at rest or when walking (n = 57, 36%) or reduce risk of skin damage (n = 32, 20%). In patients with non-functional limbs (n = 3 studies), the most common goal was to reduce degree of contracture.
Intervention
There is a particular need for a defined intervention protocol to facilitate incorporation of PCT into clinical practice, given the procedure’s absence from the training of clinicians managing spasticity. 17 However, whilst this review provides some indications on how PCT should be performed, the poor quality and heterogeneity of studies included prevents clarification of a best practice protocol.
Only 1 study specified the training of the clinician performing PCT (a Physical Medicine and Rehabilitation physician trained by an orthopaedic surgeon), 4 preventing robust conclusions being drawn on the background or training required for safe PCT. Three studies reported procedures occurring in community or outpatient settings (nursing home, n = 2; outpatient clinic n = 1), suggesting that PCT may not require a surgical setting, but more evidence is required to confirm this. Only 3 studies reported procedure duration (range 10-40 minutes).
There was significant heterogeneity in the description of the technique. Variation was found in the type of needle used, the utilisation of anaesthetic or sedation, and skin preparation, but sufficient similarities were identified to enable preliminary conclusions to be drawn. These commonalities may serve as a framework for development of protocols for performance of PCT.
All papers but one reported the utilisation of bevelled 16 or 18 gauge needles and pre-procedural skin preparation, whilst all studies utilised one or both of topical anaesthetic and short acting sedation. Tendon identification via palpation was reported in 5 of 6 studies, with one study utilising both palpation and ultrasound for identification. 14
Four of the 5 papers reporting procedural technique described insertion of the tenotomy needle perpendicularly to the tendon of interest. However, there was variation in technique. Three studies reported repeated advancement and retraction of the needle through the tendon, whilst 2 studies reported tenotomy through a lateral shearing motion. This may reflect need for different techniques in different tendon types. This should be clarified in future publications. Procedural success was defined as achieving sudden increased joint extension (2 studies), disappearance of subcutaneous cord (2 studies), or when a ‘pop effect’ was achieved in (1 study). There was no discussion of different tenotomy types (total or hemitenotomy) in any of the included studies.
Complications
Importantly, PCT appeared to be safe with an overall rate of adverse events and complications of 6.9%, the majority of which were low grade according to the Clavien-Dindo Classification. 15 This is particularly notable given the frailty of the typical PCT patient but is consistent with previous findings. 18 However, poor reporting across studies resulted in limited detail regarding the detection and management of adverse events and may have impacted evaluation of their severity.
One study described an instance of cutaneous necrosis, resulting from previously undiagnosed lower limb obliterative arteriopathy, which required a bypass following PCT to allow proper wound healing. 4 Even if rare, such serious potential complications deserve particular attention. As the authors suggest, clinical vascular examination should be performed to avoid vascular complications, with at risk patients perhaps also warranting more sensitive diagnostic test (eg, ankle brachial index, arterial doppler ultrasound). Quantifying these risks, and including during consenting, is key to developing the clinical use of this procedure.
Avoiding inadvertent nerve injuries and vascular complications also requires detailed functional and neurovascular anatomical understanding during tendon identification, necessitating specialist training for PCT operators. Use of ultrasound alongside palpation during identification may also reduce incidence of neurovascular trauma, as suggested in the chemodenervation and nerve block literature.19,20
Outcome Measures
The current review identified relatively consistent use of the Goal Attainment Scale (GAS) and Passive Range of Motion (PRoM) across studies, and there was tentative evidence that PCT was effective in improving patient outcomes by both metrics. There is consensus among the authors of this review that both measures are appropriate for the intervention and patient population and their consistent use allowed for some degree of data synthesis. 21
Importantly, outcomes achieved by patients in this review included several complex, higher-level goals such as improved gait quality or improved ease of patient transfer. Coupled with the anticipated long-term effect of PCT, the opportunity to attain these functional outcomes following this procedure may further increase its value as a rehabilitative intervention.
However, generalisable data on overall function and quality of life is limited. Depending on the goals selected, GAS can provide some information on participation and functional outcomes. However, the studies included did not collect specific data on global function, such as FIM, or quality of life, such as SF36.21,22 In addition, none included spasticity-specific outcome measures, such as the ArmA, LegA or the SQoL-6D. 21 Including such measures in future studies will help to better understand the potential role of PCT within the broader treatment algorithm of patients with spasticity.
Another important unaddressed consideration is the cost-effectiveness of PCT. Although it is likely that PCT represents a cost-effective treatment option against open surgical techniques, formal health economic evaluation of the treatment and follow-up costs of this procedure against current standard of care is currently missing. To quantify this will require outcome data such as direct and indirect cost analysis, incremental cost effectiveness ratio and disability-adjusted life years (DALYs) to be collected in future studies.
Further Directions
Future studies of PCT in the management of spasticity related contractures should build on the findings of the observational research published to date. Randomised controlled trial evidence would be optimal, but the associated cost, design and recruitment challenges of these studies are likely prohibitive. As such, it is imperative that the design of future observational studies is carefully considered. Consensus must be reached on technique and appropriate training, equipment, outcome measure selection and results reporting.
A formal Delphi process, involving experts from across professional groups including surgical and rehabilitation specialists, would be ideal to reach such a consensus and standardise the clinical and research protocol. With clarity and agreement on the technique, measures and reporting, larger, multi-site, real world and comparable datasets could be built, improving the external validity and generalisability of the observational data. Longer term follow-up should also be sought to confirm the risks and benefits of PCT over a greater timeframe.
Study Limitations
Unlike a previous review, 18 which included heterogeneous patient populations – such as those with contractures unrelated to spasticity, mixed paediatric and adult cohorts, or procedures requiring surgical instruments and anaesthesia – this review specifically examines procedures feasible in an outpatient setting under local anaesthetic. By restricting inclusion to contractures secondary to spasticity, and to procedures that can be performed by a physical and rehabilitation medicine (PRM) physician (rather than requiring complex surgical expertise), this study offers a more clinically relevant synthesis for rehabilitation practitioners. This review’s focus on patients perhaps less suitable for general anaesthetic also enhances its clinical relevance given the significant and growing population of frail contracture patients within ageing populations.
A key strength of this review is its attempt to synthesise outcome data across included studies, particularly in relation to passive range of motion (PROM) and the Goal Attainment Scale (GAS). Previous systematic reviews have been unable to achieve meaningful synthesis due to excessive methodological and clinical heterogeneity in their included studies. By applying stringent inclusion criteria, this review reduces variability, thereby enhancing the reliability of its findings and providing more applicable evidence for clinical practice.
However, several limitations must be acknowledged. First, only studies published in English and French were included, potentially introducing language bias and excluding relevant data from other language sources. Second, while this review reduces heterogeneity relative to prior work, the synthesis of outcome data remains constrained by variations in intervention techniques and outcome measures across studies. Further, there was a marked lack of data across studies concerning any spasticity management options that included patients had previously trialled (including any previous surgery), complicating interpretation of the impact of tenotomy.
Citation and publication bias may also influence the findings, as studies with positive outcomes are more likely to be published and cited. Additionally, the follow-up duration in most included studies was limited, restricting insights into long-term recurrence rates and durability of treatment effects.
Many studies did not provide detailed descriptions of the tenotomy technique used, limiting the ability to carry out a comprehensive evaluation of optimal procedural approaches. Furthermore, while this review exclusively focuses on individuals with contractures arising after central nervous system insults, similar procedures may be relevant for patients with contractures arising from alternative aetiologies. The exclusion of such cases reduced the overall sample size available for analysis.
Despite these limitations, this systematic review provides an important contribution by consolidating evidence on a minimally invasive intervention with potential for wider application in PRM practice.
Conclusion
This is the first systematic review specifically exploring the use of PCT in adult patients with spasticity seen in an outpatient clinic setting. Due to heterogeneity and poor quality of published data, it was challenging to draw clear conclusions regarding indications, procedural techniques and clinical outcomes. Importantly, in experienced hands, the reported rate of serious complication for these procedures was low, which is especially compelling considering the frailty of the population that might be candidate for PCT. Large, multi-site prospective observational studies with longer term follow-up data are required to generate high-quality evidence on the safety and efficacy of this procedure. This will require consensus on the details of the technique, appropriate clinician training and outcome measure selection.
Footnotes
Author’s Note
Eve Boissonnault is now affiliated to Faculty of Medicine and Dentistry, University of Alberta, Edmonton, AB, Canada.
Author Contributions
All authors were involved in the conceptualisation and planning of this study, and in development of search strategy. IJB and AS undertook English text review, whilst EB and JD undertook review of French papers. Data synthesis and analysis was performed by IJB. IJB drafted the resulting manuscript. All authors contributed to manuscript review and revision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.