
Abstract
Background:
Effective management of heart failure (HF) critically relies on adherence to evidence-based pharmacotherapy. However, adherence remains suboptimal, contributing to preventable hospital readmissions, disease progression, and increased healthcare costs. This study assessed medication adherence and associated factors among adult HF patients in selected hospitals of North Shewa Zone, Oromia, Ethiopia.
Methods:
An institutional-based cross-sectional study was conducted among 327 adult HF patients selected via simple random sampling. The sample size was calculated using a single population proportion formula (P = .738, 95% confidence interval [CI], 5% margin of error) and adjusted for a 10% non-response rate. Medication adherence was measured using the Amharic version of the Morisky Medication Adherence Scale (MMAS-8). Data were entered and analyzed using SPSS version 26. Logistic regression identified factors associated with adherence, with statistical significance set at P < .05.
Results:
Out of 327 participants, 165 (50.5%) were female, with a mean age of 43 ± 17.6 years. Good medication adherence was observed in 146 participants (44.65%). Independent predictors of adherence included higher HF knowledge (AOR = 2.03; 95% CI = 1.13-3.66; P = .018), access to free medications (AOR = 1.78; 95% CI = 1.04-3.03; P = .034), and receiving education on medication adherence (AOR = 2.20; 95% CI = 1.22-3.97; P = .009).
Conclusion and Recommendations:
Less than half of HF patients demonstrated good medication adherence. Structured patient education, reliable access to medications, and improved HF knowledge were key determinants of adherence. Interventions targeting these factors are strongly recommended to enhance medication adherence and improve clinical outcomes among HF patients in North Shewa Zone.
Keywords
Introduction
Adherence to evidence-based medication remains the cornerstone of effective heart failure (HF) management, yet suboptimal adherence continues to undermine disease control and outcomes worldwide. Studies consistently demonstrate that high adherence is associated with reduced hospitalizations, slower disease progression, and improved survival, whereas poor adherence contributes to frequent readmissions and worsening morbidity1 -3 Identifying determinants of non-adherence is therefore crucial for developing targeted interventions that improve quality of care and reduce avoidable rehospitalizations.
The World Health Organization (WHO) defines adherence as the extent to which a patient’s behavior aligns with agreed recommendations from healthcare providers, encompassing treatment initiation, correct implementation, and discontinuation when appropriate. 4 Medication non-adherence—often described as taking less than 80% of prescribed doses—remains a major, yet preventable, barrier to optimal clinical outcomes. It is linked not only to increased morbidity and mortality but also to escalating healthcare costs.5,6
Globally, cardiovascular diseases (CVD) remain the leading cause of death, accounting for nearly 18 million deaths annually, with more than 3-quarters occurring in low- and middle-income countries (LMICs). 7 In sub-Saharan Africa, CVD contributes substantially to adult hospital admissions, with HF representing 3% to 7% of inpatient cases.8,10 Unlike in high-income countries where ischemic heart disease (IHD) predominates, the burden of HF in Africa is often attributed to hypertension, rheumatic heart disease (RHD), and, increasingly, IHD.8,10 Patients tend to present at a younger age and with more advanced disease.8,9
Ethiopia mirrors these regional trends. Hospital-based studies reveal a growing burden of HF, largely attributable to hypertensive heart disease, RHD, and IHD.10,11 Despite the availability of effective HF medications, adherence rates remain low, posing a critical challenge to disease management. Several Ethiopian studies report poor adherence and highlight factors such as limited health literacy, complex treatment regimens, and socioeconomic barriers.6,7,11,12 Given the fragmented evidence and limited data from semi-urban and rural Ethiopian settings such as the North Shewa Zone, this study was undertaken to address an important knowledge gap. Specifically, it sought to answer the following research questions:
What is the level of medication adherence among adults with heart failure in selected hospitals of the North Shewa Zone, Oromia, Ethiopia?
What are the key patient-, disease-, medication-, and healthcare system–related factors influencing medication adherence in this population?
By identifying these context-specific determinants, the study aims to inform targeted interventions that improve adherence and, ultimately, enhance clinical outcomes for heart failure patients in this and similar underserved regions. While previous studies in Ethiopia—such as those conducted in Addis Ababa.12,24 have provided valuable insights, they mainly reflect conditions in specialized, tertiary-care urban centers. In contrast, this study focuses on a predominantly rural and semi-urban population in the North Shewa Zone, where healthcare access, socioeconomic circumstances, and health literacy levels may differ markedly. Thus, our findings offer novel, context-specific evidence that is essential for informing equitable health strategies across Ethiopia’s diverse settings.
Review of Literature
Medication adherence in heart failure (HF) patients is a multifactorial challenge, influenced by patient-related, disease-related, and healthcare system-related factors. Comorbidities in HF patients often lead to polypharmacy, with individuals commonly taking 6 to 8 medications daily. 13 Polypharmacy increases the risk of non-adherence due to regimen complexity, higher side effect burden, and patient confusion. Recent evidence from sub-Saharan Africa indicates that patients on 5 or more medications are significantly more likely to exhibit non-adherence compared to those on fewer drugs. 14
Psychological comorbidities, particularly depression and anxiety, further complicate adherence. Studies from 2021 to 2023 show that 20% to 50% of HF patients experience depressive symptoms, which are independently associated with lower adherence and worse clinical outcomes.15,16 Cognitive impairment, common in older adults with HF, also reduces adherence and increases hospitalizations. 17 A systematic review in 2022 highlighted that HF patients with mild cognitive decline were 1.5 to 2 times more likely to miss doses or take medications incorrectly. 18
Medication-related factors such as adverse effects, dosing frequency, and prolonged treatment duration continue to challenge adherence. 19 Complex regimens are associated with reduced quality of life, increased healthcare utilization, and higher risk of medication errors. 20 Recent studies in Ethiopia and other LMICs (2021-2023) report that irregular drug supply, medication cost, and lack of patient counseling are significant barriers to adherence.21-23
Healthcare system factors, including patient education and follow-up care, are critical determinants. Patients who receive structured education on HF self-care and medication management have over twofold higher adherence compared to those without such support. 24 Peer support programs and family involvement have also shown promise in improving adherence by addressing behavioral and social barriers. 25
Despite these insights, data on adherence determinants in semi-urban and rural settings, such as North Shewa Zone in Ethiopia, remain limited. Existing studies highlight the importance of tailored interventions that address polypharmacy, psychological comorbidities, medication accessibility, and patient knowledge to optimize adherence and improve clinical outcomes.26,27
Research Questions
What is the level of medication adherence among adults with heart failure in selected hospitals of North Shewa Zone, Oromia, Ethiopia?
What are the key determinants influencing medication adherence among adults with heart failure in the study area?
Methods, Study Design, and Period
A cross-sectional study was carried out at selected Hospitals in North Shewa Zone The study was carried out at selected hospitals in North Shewa Zone, Oromia Region, Ethiopia. Fitche town, capital town of zone and is found 114 km from the capital city of Ethiopia. In this zone, there are 5 total public hospitals are found. From those 5 hospitals: Fitche Teaching Hospital, Kuyu General Hospital, and Muketuri Primary Hospital are the selected study areas. According to the information provided from perspective health offices, these hospitals provide health care service for total catchment area population of 2 232 938, of which 1 132 827 are females and 1 100 111 are males. There are an average of 856 heart failure patients per month served in these 3 selected hospitals. These hospitals’ climate is almost similar, which is categorized into temperate (weyna dega) and Qola zone and topography is plain at which many health workers give health care services. A majority of the residents are sedentary farmers, whose basic livelihood is farming. Study was conducted at Fitche, Kuyu, and Muketuri hospitals. Study was conducted from April 1 to June 30/2024.
Source Population and Study Population
The source population for this study is all heart failure patients undergoing treatment at selected Hospitals in North Shewa Zone. The study population comprised all adult patients with heart failure who were either admitted as inpatients or attending follow-up clinics as outpatients during the study period and who met the inclusion criteria. Including both groups provided a more comprehensive understanding of medication adherence across the continuum of care, as adherence behaviors can be meaningfully evaluated in both settings. Combining them also allowed for a larger and more representative sample of heart failure patients receiving care at these hospitals.
Sample Size Determination
The sample size for the first objective is calculated using a single population proportion formula, based on the following assumption: a proportion level of P = 73.8%, taken from a study conducted at Addis Ababa black lion Specialized Referral Hospital. 24
❖ 95% confidence level and 5% degree of precision
❖ margin of error (0.05)
❖ Z ± α/2 is the standard normal value at a 95% confidence level (1.96)
❖ Fitting into the formula, the final sample size was


n = 297.12 By adding 10% for non-responders: The final sample size = 327
Inclusion and Exclusion Criteria
Patients aged 18 years or older, diagnosed with heart failure, who were admitted or had follow-up visits during the study period, and who were taking at least 1 medication after admission or continuing at least 1 previous medication were included. Patients who were critically ill, unable to communicate, had mental health problems, or hearing impairments, or were unwilling to participate at the time of data collection were excluded.
Dependent Variables
Medication Adherence
Independent Variables
Patient-related factors: age, sex, educational status, residence, marital status, occupation, smoking, alcohol use, and knowledge of HF.
Disease-Related Factors
Hx of hospitalization, comorbidity symptom, severity, and duration of heart failure.
Medication-Related Factors
Drug adverse effect, number of drugs, patient, education on medication adherence, duration of regimen, and availability of drug.
Sampling Procedure
Among the hospitals in North Shewa Zone, 3 hospitals (Fitche, Kuyu, and Muketuri) were selected using the lottery method. The total sample size was proportionally allocated to each hospital based on their respective heart failure patient populations using the formula for proportional allocation:

where n is the total sample size, N is the total population of adults with heart failure, Nj is the population size of the jth hospital, and nj is the allocated sample size for each hospital. With a total of 856 heart failure patients across the 3 hospitals, and a calculated sample size of 327, the proportional allocation resulted in 123 participants from Fitche Hospital (327/856 × 320), 106 from Kuyu Hospital (327/856 × 280), and 98 from Muketuri Hospital (327/856 × 256). Within each hospital, study participants were selected using simple random sampling Within each hospital, a sampling frame—a complete list of all eligible heart failure patients, both inpatients and outpatients, during the study period—was prepared. Study participants were then selected from this list using a computer-generated simple random sampling method. This 2-stage approach, involving the lottery method for hospital selection and simple random sampling for patients, enhances the study’s rigor and ensures that the design can be easily replicated in similar settings.
Data Collection Instruments and Procedures
Data were collected using a structured and pre-tested questionnaire, adapted from previously validated studies. The questionnaire gathered information on socio-demographic characteristics, medication adherence, challenges to adherence, and patient knowledge. Face-to-face interviews were conducted with eligible patients after their physician consultations, following informed consent. In addition, relevant clinical data were extracted from the patient’s medical records to supplement the interview data.
Medication adherence was assessed using the 8-Item Morisky Medication Adherence Scale (MMAS-8), which was translated into Amharic and validated for the local context. The translation process involved forward translation by 2 independent translators, back-translation by a third translator, and review by a panel of experts to ensure conceptual equivalence. The Amharic MMAS-8 demonstrated good internal consistency in this study (Cronbach’s α = .89). The MMAS-8 consists of 8 items, with total scores ranging from 0 to 8. A score of 8 indicates high adherence, scores of 6 to 7 indicate moderate adherence, and scores below 6 reflect low adherence. For this analysis, scores of 8 were classified as “good adherence,” and scores <8 were classified as “poor adherence.”
Heart failure knowledge was measured using the Dutch Heart Failure Knowledge Scale (DHFKS), which underwent a similar translation and validation process. The DHFKS demonstrated acceptable internal consistency (Cronbach’s α = .86). A score of ⩾75% correct responses was considered indicative of good knowledge (Jaarsma et al., 2003). 28
Data Quality and Management
A standardized questionnaire was developed based on a literature review and evaluated by experts for content validity. A pretest on 5% (17 participants) of the sample led to necessary adjustments. Data collectors received training, with continuous supervision and daily review to ensure data quality. Data were cleaned and checked for completeness using Epi Data before being exported to SPSS for analysis; incomplete or unclear data forms were excluded from the analysis.
Data Entry, Analysis, and Interpretation
Data were entered into Epi Data 4.4.1 and analyzed using SPSS version 26. Frequencies were calculated for patient, disease, and medication-related factors. Categorical variables were presented as counts and percentages, while continuous variables were expressed as mean ± SD. Multi-collinearity was checked using the Variance Inflation Factor (VIF), and all values were below 5, indicating no significant multi-collinearity. Chi-square tests were used to assess associations between categorical variables. Variables with P < .25 in the bivariate analysis were included in the multivariate logistic regression to identify independent predictors of medication adherence. The model fit was evaluated using the Hosmer-Lemeshow goodness-of-fit test (P = .72), indicating an acceptable fit. Statistical significance was set at P < .05, and Adjusted Odds Ratios (AORs) with 95% confidence intervals (CIs) were used to measure the strength of associations. Results were presented in narrative form and in tables for clarity.
Operational Definition
Medication Adherence: The extent to which a patient’s medication-taking behavior follows the prescribed recommendations, assessed using the 8-Item Morisky Medication Adherence Scale (MMAS-8; Morisky et al., 2008). 29
Good Medication Adherence: Patients scoring 8 on the MMAS-8 are considered to have good adherence (Morisky et al., 2008).
Poor Medication Adherence: Patients scoring below 8 on the MMAS-8 are classified as having poor adherence (Morisky et al., 2008).
Knowledge About Disease: Patients’ knowledge regarding heart failure, was measured using the Dutch Heart Failure Knowledge Scale (DHFKS). A score of ⩾75% correct responses indicates good knowledge (Jaarsma et al., 2003). 28
Education on Medication Adherence: A “Yes” response indicated that the patient recalled receiving structured verbal counseling or written information from a healthcare provider—such as a doctor, nurse, or pharmacist—about the importance of taking heart failure medications exactly as prescribed, including proper dosage, timing, and continuity of treatment.
Free Medication: A “Yes” response indicated that the patient obtained their prescribed heart failure medications at no personal cost, typically through hospital-based waivers, government safety-net programs, or other subsidy schemes, as documented in their medical record or self-reported during the interview.
Results
Study Population Characteristics
During the study period, a total of 453 patients were assessed for eligibility at the 3 hospitals. Of these, 327 patients were included in the analysis (Figure 1). A total of 126 patients were excluded: 35 refused to participate, 68 were aged less than 18 years, and 23 had incomplete medical documentation.

Flow chart showing the number of study participants, April 1 to June 30, 2024.
Socio-Demographic Characteristics of the Study Population
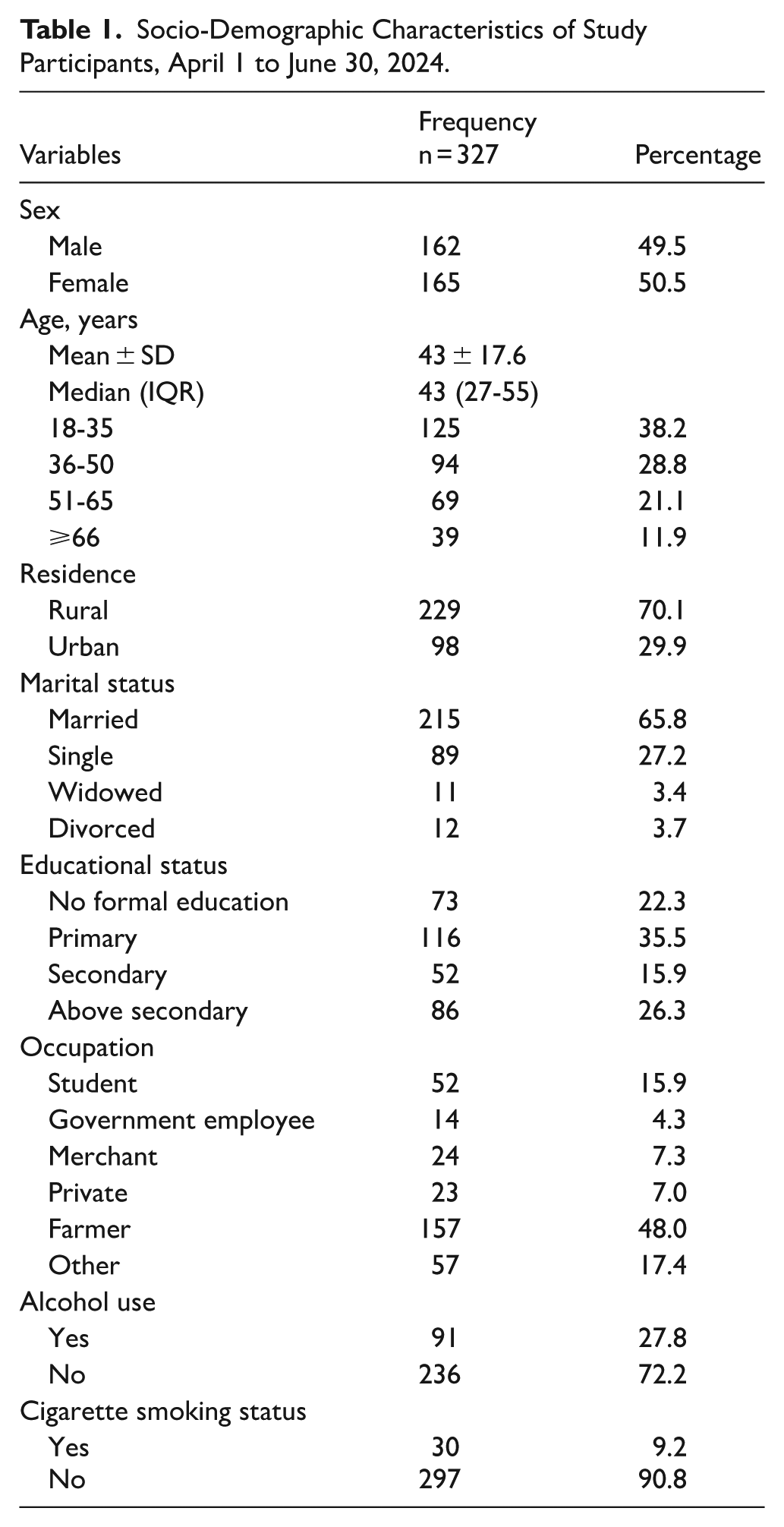
The socio-demographic and clinical characteristics of the 327 participants are summarized in Tables 1 and 2, respectively. The mean age of participants was 43 ± 17.6 years, 165 (50.5%) were females, and 229 (70.1%) resided in rural areas. The majority (269, 82.3%) demonstrated poor knowledge levels about heart failure. Most patients (253, 77.4%) paid for their medications out-of-pocket, while 260 (79.5%) reported receiving education on medication adherence.
Socio-Demographic Characteristics of Study Participants, April 1 to June 30, 2024.
Clinical Characteristics of Study Participants, April 1 to June 30, 2024.

Clinical Characteristics of the Study Population
Among the 327 heart failure patients, 80 (24.5%) had a history of hospitalization, while 278 (85%) presented with chronic comorbidities. The most common comorbid conditions were hypertension (113 patients, 34.6%), both diabetes and hypertension (62 patients, 19%), and diabetes alone (47 patients, 14.4%). Over half of the participants (52.3%) had been on treatment for more than 5 years. Most patients (253, 77.4%) covered their medication costs themselves, while 260 (79.5%) reported receiving education on medication adherence. The mean number of prescribed medications was 4.4 ± 2, with the majority (170 patients, 52%) taking between 4 to 6 medications. Regarding heart failure knowledge, 269 participants (82.3%) demonstrated poor knowledge levels (Table 2).
Adherence Status
According to the study, 146 participants (44.65%) demonstrated good adherence to their prescribed medications, as assessed by the MMAS-8 scale. In contrast, 181 participants (55.35%) exhibited poor medication adherence. Among them, 129 participants (39.45%) scored between 6 and 7 (moderate adherence), while 52 participants (15.9%) scored below 6 (low adherence).
Problems That Challenge Medication Adherence
The most commonly reported reason for non-adherence was forgetfulness, cited by 86 participants (47.5%). This was followed by the unavailability of medication (64 participants, 35.4%) and feeling worse after taking the medication (13 participants, 7.2%; Table 3).
Problems That Challenge Medication Adherence of Study Participants, April 1 to June 30, 2024.

Factors Associated With Medication Adherence
The results of the bivariate and multivariate logistic regression analyses are presented in Table 4. The multivariate analysis revealed several significant predictors of medication adherence:
Binary Logistic Analysis and Multivariate Analysis of Factors Associated With Medication Adherence of the Study Participants, April 1 to June30, 2024.

Abbreviations: AOR, adjusted odds ratio; COR, crude odds ratio; CI, confidence interval; I, Reference.
Bold text indicates a statistically significant association (P < .05).
Significant (P < .05).
Participants who received education on the importance of medication adherence were over 2 times more likely to adhere to their prescribed medications compared to those who did not (AOR = 2.203; 95% CI = 1.222-3.971; P = .009).
Participants who received their medications for free were 1.78 times more likely to adhere compared to those who paid out-of-pocket (AOR = 1.778; 95% CI = 1.044-3.029; P = .034).
Participants with good knowledge about heart failure were twice as likely to adhere compared to those with poor knowledge (AOR = 2.033; 95% CI = 1.129-3.663; P = .018)
In this study, 146 participants (44.65%; 95% CI = 39.2%-50.2%) were found to have good adherence to their prescribed medications.
Discussion
This study revealed that less than half (44.65%) of heart failure patients demonstrated good medication adherence. Three factors were independently associated with adherence: receiving education about adherence, having access to free medications, and possessing good knowledge about heart failure. Patients who received structured education were more than twice as likely to adhere, and free access to medications nearly doubled adherence rates. Likewise, patients with good knowledge of their disease had significantly higher odds of adherence, highlighting the role of health literacy in chronic disease management.
The medication adherence rate observed in this study (44.65%) is considerably lower than the 73.8% reported at Tikur Anbessa Specialized Hospital in Addis Ababa(24). This disparity underscores the pronounced urban–rural gap in healthcare resources and patient support systems across Ethiopia. It also illustrates that findings from the national capital may not be directly applicable to zonal hospitals serving rural communities, thereby reinforcing the significance and originality of this study in guiding decentralized and context-sensitive public health strategies. Consequently, our rate is higher than reports from Tanzania (25.3%) and India (28.3%),23,24 where systemic barriers such as medication shortages, high costs, and limited health literacy contribute. Recent African studies also confirm that adherence in heart failure patients remains consistently below 50% in many low-resource contexts.23,25
The strong link between patient education and adherence underscores the crucial role of healthcare providers, particularly nurses and pharmacists, in counseling patients. This is consistent with findings from the United States, where pharmacist-led interventions significantly improved adherence. 30 Our results also reinforce the financial barrier posed by medication costs. In LMICs, affordability remains one of the most frequently reported barriers.23,31 In our study, patients with free access to medicines were nearly twice as likely to adhere, echoing evidence from Sudan and East Africa.23,27
The association between knowledge and adherence emphasizes the need for continuous, simplified health education tailored to patients’ literacy levels. Peer support networks and group-based education have also been shown to enhance adherence, 26 an area that could be piloted in Ethiopian settings.
Our findings further highlight the financial barrier posed by medication costs. In this study, patients with free access to medicines were nearly twice as likely to adhere to their prescribed regimen. It is important to note that “free access” in this context depends on hospital-specific waiver systems as well as broader national supply chain dynamics. Disruptions—such as those experienced during the COVID-19 pandemic—can compromise the reliability of this access. The recent expansion of Ethiopia’s Community-Based Health Insurance (CBHI) program could help alleviate this barrier, provided it ensures consistent coverage and availability of essential heart failure medications.
Limitations
This study has several limitations. First, its cross-sectional design precludes causal inference; therefore, the observed associations should not be interpreted as direct causal relationships. Second, although random sampling was employed, selection bias remains possible since only patients who presented to hospitals were included, potentially excluding the most non-adherent or severely ill individuals in the community. Third, medication adherence was assessed using a self-reported tool, which is subject to recall and social desirability biases and may have led to an overestimation of true adherence levels. Fourth, although adjustments were made for several confounding variables, residual confounding—such as unmeasured factors related to health beliefs, social support, or subtle differences in disease severity—may still exist. Finally, the generalizability of these findings is limited to comparable low-income, semi-urban settings within sub-Saharan Africa. Furthermore, although we identified key predictors, we did not perform stratified analyses (eg, by rural or urban residence or by sex) to explore potential effect modification. Future studies with larger sample sizes could examine whether the effects of factors such as free medication or patient education vary across these important subgroups.
Conclusion and Recommendations
Medication adherence among heart failure patients in this study was suboptimal. Education, access to free medications, and good disease knowledge were significantly associated with higher adherence.
For policymakers: Expand health insurance coverage and subsidize essential medications to reduce out-of-pocket costs.
For healthcare professionals: Integrate structured, ongoing adherence counseling into routine care, using both individual sessions and peer support groups.
For hospitals: Ensure a reliable supply of essential medicines and involve pharmacists and nurses in adherence-focused patient education.
Improving adherence requires a multifaceted approach addressing patient-level and systemic barriers.
Footnotes
Acknowledgements
The authors extend their sincere gratitude to the hospital managers and unit team leaders for their valuable cooperation and support during the data collection process. We also express our heartfelt appreciation to the data collectors and friends whose dedication, assistance, and encouragement were instrumental in the successful completion of this research.
Ethical Considerations
Ethical clearance was obtained from the Institutional Review Committee of Addis Ababa Health Bureau with the ethical reference number AAMBC/stu/10797/2024. A formal letter was submitted to the Addis Ababa Health Bureau and each selected study hospital to ensure permission and maintain confidentiality.
Consent to Participate
Verbal and written informed consent was acquired from each study participant under the principles of the Helsinki Declaration. The Declaration of Helsinki was considered, and its principles and recommendations have been applied.
Consent for Publication
All authors read and approved the revised manuscript for publication.
Author Contributions
Abdurehman Seid Mohammed has contributed to the Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Supervision, Validation, Visualization, Writing—original draft, and Writing—review & editing. Wubanchi Seid has contributed to the Conceptualization, Data curation, Formal analysis, Investigation, and Methodology. Mustofa Hassen Yesuf has contributed to the Conceptualization, Data curation, Formal analysis, Investigation, and Methodology. Selam Seyoum Abebe has contributed to the Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Supervision, and Validation. Ali Seid Kolbay has contributed to the Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Supervision, and Validation. Bisrat Solomon has contributed to the Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Supervision, and Validation. Getachew Mekete Deress has contributed to the Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Supervision, Validation, Visualization, and writing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during this study are not publicly available to protect patient confidentiality and comply with institutional policies. However, a fully de-identified dataset can be made available from the corresponding author upon reasonable request, following approval of a methodologically sound research proposal.
Provenance and Peer Review
Not commissioned, externally peer-reviewed.
Clinical Trial Number
Not applicable.