
Abstract
Background:
Cardiac rehabilitation (CR) improves exercise capacity and is strongly recommended in clinical guidelines. However, no established scoring system exists to predict improvements in exercise capacity following CR.
Objective:
This study aimed to assess whether the CHA2DS2-VASc score could serve as a predictive scoring system for improvements in exercise capacity after CR.
Methods:
Of the 99 patients with cardiovascular disease who participated in the hospital-based CR, those who were ineligible were excluded. The remaining patients were stratified into 2 groups based on the median CHA2DS2-VASc score. Changes in peak oxygen uptake (peak VO2) and clinical parameters from baseline to follow-up were compared between the groups.
Results:
A total of 46 patients (median age, 74 years; 72% male) were stratified according to the median CHA2DS2-VASc score of 4. Patients in the high-score group (CHA2DS2-VASc score ⩾ 4) were older, more likely to be female, and had elevated B-type natriuretic peptide levels compared with those in the low-score group (CHA2DS2-VASc score <4). The prevalence of comorbidities was similar between the groups. The low-score group showed a significantly greater improvement in peak VO2 from baseline to follow-up compared with that of the high-score group (2.8 [1.3-4.7] vs 0.4 [−1.0 to 2.4] mL/kg/min, P < 0.01). Spearman’s rank correlation analysis showed a significant negative correlation between CHA2DS2-VASc scores and the change in peak VO2 between baseline and follow-up (r = −0.37, P = .01). A CHA2DS2-VASc score <4 was independently associated with an increase in peak VO2 (β = 0.50, 95% confidence interval 0.23-2.14, P = .01) in the multivariate analysis using multiple linear regression.
Conclusions:
The CHA2DS2-VASc score may be a useful tool for predicting potential improvements in exercise capacity after CR.
Introduction
Cardiac rehabilitation (CR) is an evidence-based, comprehensive intervention that contributes to improved exercise capacity, enhanced quality of life, and better long-term prognosis in patients with cardiovascular disease (CVD). 1 Its efficacy has been demonstrated in numerous randomised controlled trials and meta-analyses, and current guidelines recommend CR as a Class I indication for major CVDs, including acute coronary syndrome and heart failure. 2 However, recent studies have revealed considerable inter-individual variability in the response to CR.3,4 A certain proportion of patients, so-called non-responders, do not exhibit significant improvement in exercise capacity or clinical outcomes, even after completing CR. 5 Factors underlying this limited response may include patient characteristics such as advanced age and comorbidities (e.g. sarcopenia, frailty, chronic kidney disease, and cognitive impairment), as well as the standardised nature of CR programs that may fail to address individual needs. 6 In light of these limitations, recent attention has shifted toward the importance of targeted strategies based on individual prognostic profiles and risk stratification, as well as the concept of precision rehabilitation tailored to the specific needs of each patient. 2 Stratifying patients who are more likely to benefit from CR is crucial for optimising the implementation and planning of CR programs, as well as for the efficient use of healthcare resources. However, a standardised scoring system for predicting improvements in exercise capacity resulting from CR has not yet been established. 7
The CHA2DS2-VASc score was originally developed to estimate the risk of stroke in patients with atrial fibrillation. 8 More recently, studies have explored its efficacy as a predictor of long-term prognosis in patients with acute coronary syndrome and heart failure.9,10 The CHA2DS2-VASc score may be a useful prognostic factor because it reflects not only stroke risk but also a broad range of systemic cardiovascular risk factors, including atherosclerosis, chronic inflammation, and comorbidities. Thus, the CHA2DS2-VASc score can be considered an indicator of overall clinical vulnerability. This study aimed to assess the association between the CHA2DS2-VASc score and improvements in exercise capacity following CR.
Methods
Study Design
This single-centre, retrospective observational study was conducted at Kindai University Nara Hospital and included consecutive patients who received outpatient CR between December 2021 and December 2024 and underwent cardiopulmonary exercise (CPX) testing at the start of the CR program and 4 to 6 months later. The CHA2DS2-VASc score (congestive heart failure/left ventricular dysfunction, hypertension, age ⩾75 years, diabetes mellitus, stroke/transient ischemic attack/thromboembolism, vascular disease, age 65 to 74 years, and female sex) was calculated at baseline based on clinical characteristics, and patients were stratified into 2 groups according to the median score. 8 The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Kindai University Nara Hospital (approval no. 786). Informed consent was obtained by an opt-out procedure from all patients.
Study Population
The study included patients aged 40 to 90 years with a confirmed diagnosis of CVD, including angina pectoris, myocardial infarction, atrial fibrillation, or hypertrophic cardiomyopathy. A total of 99 patients met these criteria and were enrolled in the study. The exclusion criteria consisted of the following: lack of baseline CPX (n = 22); lack of follow-up CPX (n = 26); failure to reach symptom-limited exercise levels during CPX (n = 3); post device implantation (implantation of a pacemaker, implantable cardioverter-defibrillator, or cardiac resynchronisation therapy device) (n = 1); or ongoing haemodialysis (n = 1) (Supplemental Figure 1).
CR Protocol
Outpatient CR following hospital discharge was conducted in accordance with the guidelines of the European Society of Cardiology and the European Association of Preventive Cardiology. 11 CR was delivered as a comprehensive program consisting of 4 key components: exercise therapy, cardiovascular risk factor management, nutritional counselling, and patient education. All the patients underwent baseline CPX to determine their anaerobic threshold (AT). Exercise prescriptions were individually tailored based on the CPX results. Aerobic exercise using a bicycle ergometer was performed once or twice a week for 20 to 30 minutes per session. Exercise intensity was adjusted according to the target heart rate derived from AT or a perceived exertion level of 11 to 13 on the Borg scale. Physical therapists supervised all sessions, and the training intensity progressively increased over time. In addition, resistance training aimed at maintaining or improving muscle strength (30%-60% of 1-repetition maximum [1RM]) as well as flexibility and balance exercises were incorporated. Cardiovascular risk factor management includes setting target values and monitoring blood pressure, blood glucose levels, lipid profiles, body weight, and smoking status. Appropriate interventions were implemented in collaboration with physicians and registered dieticians as needed. Nutritional counselling was provided either individually or in group sessions by registered dieticians, promoting dietary modifications focused on reduced salt and fat intake and increased dietary fibre. Patient education aims to enhance self-management skills by promoting disease understanding, emphasising the importance of preventing recurrence, ensuring medication adherence, and providing teaching methods for continuing exercise at home.
Outcome Measures
The primary outcome was the change in peak oxygen uptake (peak VO2) from baseline to follow-up, which was compared between the 2 groups stratified by the median CHA2DS2-VASc score. Secondary outcomes included within- and between-group comparisons of changes in the 6-minute walk distance (6MWD), grip strength, calf circumference, Short Physical Performance Battery score, body composition, and other exercise tolerance parameters.
Data Collection
Baseline data included age, sex, body mass index (BMI), medical history, laboratory parameters, medications, and LVEF measured by echocardiography. The 6MWD, grip strength, calf circumference, Short Physical Performance Battery score, body composition, and CPX were assessed at both baseline and follow-up. Grip strength was measured using GRIP-D (Takei Scientific Instruments Co., Tokyo, Japan), and body composition was determined using bioelectrical impedance analysis (InBody S10; InBody Co., Tokyo, Japan).
CPX Testing
CPX testing was performed using a ramp protocol on a cycle ergometer (Strength Ergo 8; Fukuda Denshi, Tokyo, Japan). Heart rate, blood pressure, 12-lead electrocardiography (FCP-8800; Fukuda Denshi), and respiratory gas exchange (Cpex-1; Fukuda Denshi) were continuously monitored. The test was considered maximal if the respiratory exchange ratio was ⩾1.1 or if the heart rate was ⩾85% of the predicted maximum. Peak VO2 was defined as the average oxygen consumption during the final 30 seconds of the test.
Assessment of 6MWD
The participants were instructed to walk back and forth along a flat, straight 30-meter corridor for 6 minutes, covering as much distance as possible. Standardised verbal encouragement (e.g. ‘You’re doing well’, ‘Keep it up’) was provided every minute. The heart rate, peripheral oxygen saturation, and subjective exertion levels were measured using the Borg scale before and after the test. The total distance walked in the 6 MWD was recorded in metres. Participants were allowed to slow down or rest as needed during the test, but were instructed to resume walking as soon as possible. The test was conducted indoors under the supervision of trained staff.
Statistical Analyses
Continuous variables are presented as medians with interquartile ranges and categorical variables as number and percentage. The Wilcoxon signed-rank test was used to analyse differences in baseline and follow-up data within groups, whereas the Wilcoxon test was used to compare parameters between the 2 groups. Correlations between CHA2DS2-VASc scores and the change in peak VO2 between baseline and follow-up were assessed using Spearman’s rank correlation coefficient. A multivariable analysis using multiple linear regression, with age, sex, and baseline peak VO2 included as covariates, was performed to examine the impact of the CHA2DS2-VASc score on improvement in peak VO2. Statistical significance was set at P < .05, and JMP Pro 18.1.0 software (SAS Institute Inc., Cary, NC, USA) was used for all statistical analyses.
Results
Patients
The median follow-up duration was 182 days. Among the 46 patients included in the analysis (median age, 74 years; 72% male), participation in the hospital-based CR program led to an average 8.0% increase in peak VO2 from baseline to follow-up. Peak VO2 improved between baseline and follow-up in 34/46 (74%) patients. The distribution of the CHA2DS2-VASc scores is shown in Figure 1. The median CHA2DS2-VASc score was 4, and patients were stratified into 2 groups based on whether their score was <4 (low-score group; n = 22) or ⩾4 (high-score group; n = 24). The baseline characteristics of patients stratified by CHA2DS2-VASc score are summarised in Table 1. The patients in the high-scoring group were older, more likely to be female, and had higher levels of B-type natriuretic peptide than those in the low-scoring group. The use of beta blockers was more prevalent in the high-score group. No significant differences were observed in LVEF and the presence of comorbidities between the 2 groups. Peak VO2 was significantly higher in the low-score group than in the high-score group (22.8 [20.5-27.1] vs 17.3 [14.4-19.9] mL/kg/min, P < .0001) at the baseline.

Distribution of CHA2DS2-VASc scores.
Baseline Characteristics.
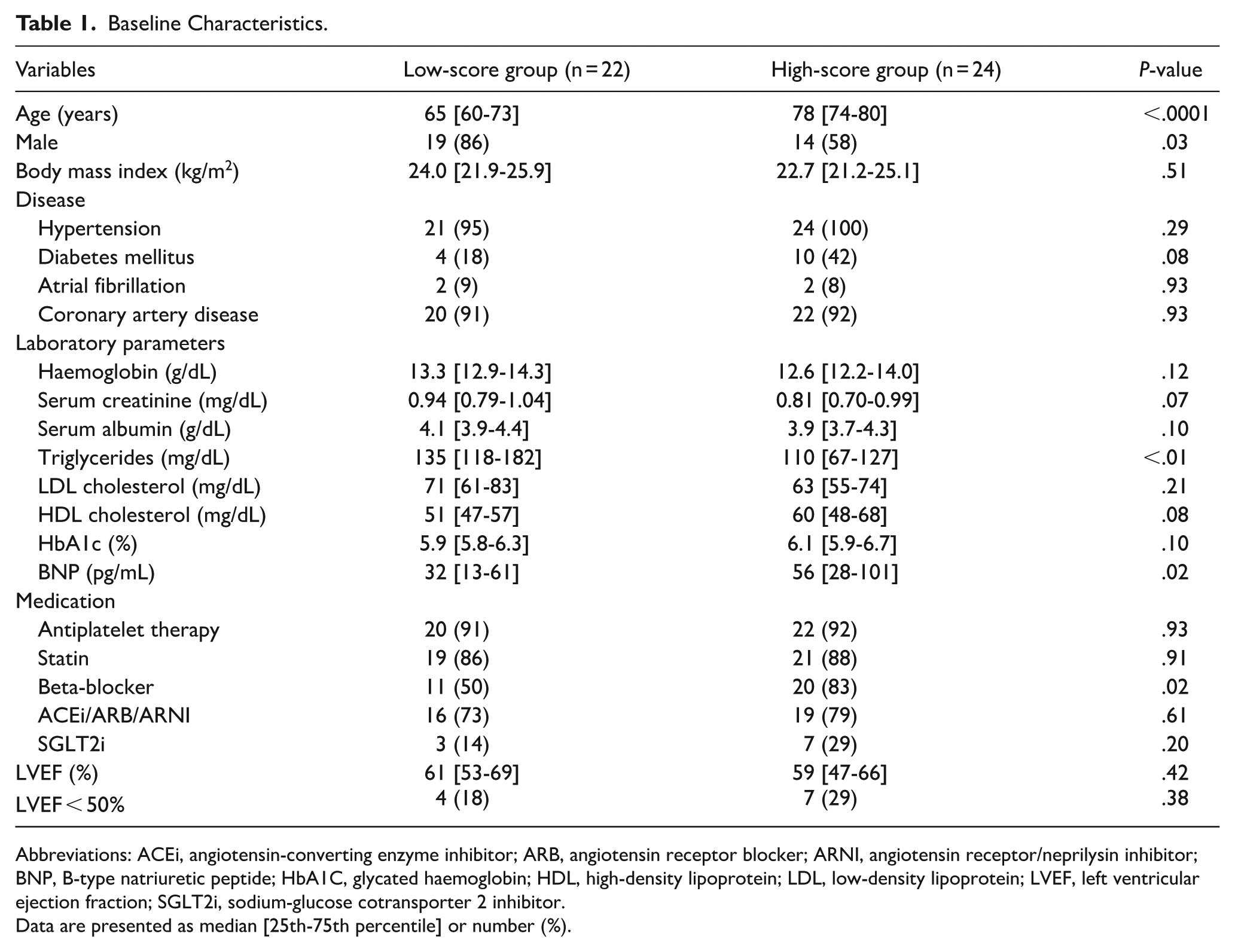
Abbreviations: ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; ARNI, angiotensin receptor/neprilysin inhibitor; BNP, B-type natriuretic peptide; HbA1C, glycated haemoglobin; HDL, high-density lipoprotein; LDL, low-density lipoprotein; LVEF, left ventricular ejection fraction; SGLT2i, sodium-glucose cotransporter 2 inhibitor.
Data are presented as median [25th-75th percentile] or number (%).
Comparison Between Baseline and Follow-Up Within Groups
Peak VO2 increased significantly from baseline to follow-up in low-score group (22.8 [20.5-27.1] vs 25.3 [22.2-30.5] mL/kg/min, P < .0001; Figure 2). In contrast, the change in peak VO2 was not significant in high-score group (17.3 [14.4-19.9] vs 17.6 [15.8-21.3] mL/kg/min, P = 0.24). Table 2 outlines the differences between baseline and follow-up in the 2 groups. In the low-score group, the 6 MWD, body fat mass, peak metabolic equivalents, and AT showed significant improvements from baseline, while in the high-score group, significant improvements were observed in the 6 MWD, handgrip strength, and peak respiratory exchange ratio.

Comparison of within-group changes in peak VO2 between baseline and follow-up: (a) low-score group and (b) high-score group.
Physical Parameters at Baseline and Follow-Up.

Abbreviations: 6MWD, 6-minute walk distance; AT, anaerobic threshold; HR, heart rate; METs, metabolic equivalents; RER, respiratory exchange ratio; SPPB, Short Physical Performance Battery; VE/VCO2, ventilatory equivalent for carbon dioxide.
Data are presented as median [25th-75th percentile].
Primary Outcome
The change in peak VO2 from baseline to follow-up was compared between the 2 groups (Figure 3). The low-score group exhibited a significantly greater increase in peak VO2 than the high-score group (2.8 [1.3-4.7] vs 0.4 [−1.0 to 2.4] mL/kg/min, P < .01).

Comparison of changes in peak VO2 from baseline to follow-up between the low- and high-score groups.
Comparison of the Changes from Baseline to Follow-Up Between Groups
Changes in exercise capacity and physical parameters from baseline to follow-up were compared between the 2 groups (Table 3). Compared to the high-scoring group, the low-scoring group showed significantly greater increases in peak metabolic equivalents and AT.
Change in Exercise Capacity and Physical Parameters Between Baseline and Follow-Up.

Abbreviations: 6MWD, 6-minute walk distance; AT, anaerobic threshold; HR, heart rate; METs, metabolic equivalents; RER, respiratory exchange ratio; SPPB, Short Physical Performance Battery; VE/VCO2, ventilatory equivalent for carbon dioxide.
Data are presented as median [25th-75th percentile].
Association Between CHA2DS2-VASc Scores and Change in Peak VO2
The correlation between CHA2DS2-VASc scores and the change in peak VO2 from baseline to follow-up was examined (Figure 4). Spearman’s rank correlation coefficient showed a significant negative correlation between these variables (r = −0.37, P = .01). Multivariate analysis using multiple linear regression was conducted with age, sex, and baseline peak VO2 as covariates. As a result, a CHA2DS2-VASc score <4 was independently associated with change in peak VO2 (β = 0.50, 95% confidence interval: 0.23-2.14, P = .01; Supplemental Table 1).

Relationship between CHA2DS2-VASc scores and change in peak VO2 from baseline to follow-up. Pearson correlation analysis shows a negative correlation between CHA2DS2-VASc scores and change in peak VO2.
Discussion
In this study of 46 patients with CVD who underwent outpatient hospital-based CR, changes in peak VO2 from baseline to follow-up were compared between 2 groups stratified based on the median CHA2DS2-VASc score. We found that patients with CHA2DS2-VASc scores <4 (low-score group) had significantly greater improvements in peak VO2 than those with scores ⩾4 (high-score group). Furthermore, patients with CHA2DS2-VASc scores <4 exhibited significant increases in the 6MWD, peak metabolic equivalents, and AT, as well as significant decreases in body fat mass. In patients with CHA2DS2-VASc scores ⩾4, the 6MWD, grip strength, and respiratory exchange ratio significantly improved. There was a significant negative correlation between CHA2DS2-VASc scores and the change in peak VO2 between baseline and follow-up. Additionally, CHA2DS2-VASc <4 was an independent predictor for a change in the peak VO2 from the baseline to follow-up. Therefore, the CHA2DS2-VASc score, a simple and widely used clinical tool, may be useful for predicting CR-derived improvements in exercise capacity.
Exercise capacity is intricately associated with vascular function. Peak VO2 reflects the ability to deliver, extract, and utilise oxygen in working muscles, a process heavily reliant on adequate vascular perfusion. Vascular dysfunction is associated with reduced peak VO2 and impaired physical endurance. 12 In our study, patients with CHA2DS2-VASc scores ⩾4 had significantly lower baseline peak VO2 than those with a score <4, supporting the association between vascular dysfunction and reduced exercise capacity. Impaired oxygen delivery, especially to the lower limb muscles, leads to lactate accumulation, contributing to fatigue and reduced exercise capacity. 13 Furthermore, in older patients with heart failure, increased arterial stiffness correlates with reduced exercise capacity. 14 These underlying mechanisms suggest that the CHA2DS2-VASc score may serve as a valuable clinical indicator for predicting improvements in exercise capacity during CR.
A nationwide database analysis reported that patients with a high burden of comorbidities are significantly less likely to undergo CR. 15 This suggests a clinical paradox in which high-risk patients who may potentially derive the greatest benefit from CR are excluded from participation. However, the mere presence of comorbidities should not justify withholding CR; rather, these patients should be considered prime candidates for intervention. Applying the CHADS2 or CHA2DS2-VASc score in clinical practice may aid in the early identification of patients at high risk for poor responsiveness to CR, thereby facilitating the development of individualised programs and the implementation of enhanced multidisciplinary interventions. In particular, a standard CR program may be insufficient for older adults with multiple comorbidities. Therefore, a comprehensive approach that considers physical, cognitive, and social factors is essential. In this context, the simple and practical use of the CHADS2 or CHA2DS2-VASc score may be valuable for determining the appropriateness and prioritisation of CR. Further prospective studies with larger patient populations are warranted to validate the clinical utility of the CR score.
Strength and Limitation
In many previous clinical trials, attempts have been made to stratify patients who are less likely to experience improvements in exercise capacity through CR.3 -6 As a result, various factors such as age, comorbidities, impaired physical function, and poor nutritional status have been reported to be associated with poor responsiveness to CR. Furthermore, it has been shown that patients with a poor response to CR, namely those with limited improvement in exercise capacity, tend to have worse long-term outcomes. Therefore, it is crucial to predict in advance which patients are likely to respond poorly to CR interventions in clinical practice to develop appropriate and individualised treatment strategies. However, no scoring systems have been proposed to predict improvements in the exercise capacity of patients undergoing CR. The CHA2DS2-VASc score was originally developed as a risk stratification tool for thromboembolic events in patients with atrial fibrillation. Owing to its simplicity, it has become widely recognised and is frequently used in clinical practice. The findings of this study suggest that the CHA2DS2-VASc score may have clinical implications in predicting CR-derived improvements in exercise capacity, thereby enabling a personalised approach for CR program development. For patients predicted to have limited improvements in exercise capacity, it may be appropriate to consider multidisciplinary interventions or implementing more comprehensive CR programs. 16 Additionally, reviewing the exercise intensity, increasing the frequency of CR sessions, or extending the duration of intervention may be beneficial. 17 Furthermore, the CHA2DS2-VASc score may serve as a useful tool for explaining the benefits of CR to patients, thereby enhancing their motivation. 18 The adoption of mobile health technologies could also be considered in these patient populations.19,20
This study had some limitations. First, this was a single-centre retrospective analysis with a small sample size, and the findings may not be generalisable. Second, the study included only patients who participated in outpatient CR, which may have introduced a selection bias. Therefore, further investigations involving larger and more diverse patient populations are warranted. Lastly, exercise intensity during CR was not recorded in the electronic medical records, making it impossible to assess the impact of exercise intensity on peak VO2 fully.
Conclusions
Stratification using the CHA2DS2-VASc score may be useful for predicting improvements in exercise capacity in patients with CVD who require outpatient hospital-based CR. Consequently, personalised optimisation of CR programs may be considered for patients expected to gain limited improvements in exercise capacity.
Supplemental Material
sj-docx-1-rpo-10.1177_27536351251381134 – Supplemental material for Predictive Value of the CHA2DS2-VASc Score on Exercise Capacity in Patients with Cardiovascular Disease
Supplemental material, sj-docx-1-rpo-10.1177_27536351251381134 for Predictive Value of the CHA2DS2-VASc Score on Exercise Capacity in Patients with Cardiovascular Disease by Eijiro Yagi, Koichiro Matsumura, Shohei Hakozaki, Yuki Uchigashima, Jun Shiroyama, Mitsuki Hase, Tomoya Nanba, Masafumi Ueno and Gaku Nakazawa in Advances in Rehabilitation Science and Practice
Footnotes
Ethical Considerations
This study complied with the Declaration of Helsinki. The study protocol was approved by the ethics committee of Kindai University Nara Hospital (approval number: 690).
Consent to Participate
Informed consent was obtained by an opt-out procedure from all patients.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author, KM, upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.