
Abstract
Objective:
The purpose of this study was to qualitatively assess the first-hand lived experiences of patients with amputation who had transitioned from a traditional socket (TS) to Osseointegration (OI) to impact their overall quality of life (QOL) and function.
Methods:
This was a qualitative phenomenological study. Participants who had a unilateral transfemoral amputation and fit the study’s inclusion criteria were interviewed in a semi-structured format regarding their quality of life and function before and after transitioning from a traditional socket (TS) to Osseointegration (OI). Responses were then analyzed through line-by-line coding to determine themes that were relevant to QOL outcomes for this study.
Results:
Eleven participants were interviewed in this study. The qualitative analysis demonstrated an emergence of 6 main themes consisting of “Improved Quality of Life,” “Supportive Community,” “Previous Ill-fitting Socket,” “Greater Function,” “Improved Osseo-perception,” and “Promotion of Community Accessibility”. Strengths included the use of an OI-specific quality of life assessment with adapted questions from validated outcome measures, international participants, and use of thematic analysis for data analysis. Weaknesses included sample size, niche participant population, and OI as a revision procedure only. More research is still necessary to explore/determine the benefits and detriments of Osseointegration as an alternative to traditional sockets for prosthetic devices.
Conclusion:
Individuals who have undergone Osseointegration procedure discuss being more satisfied with their prosthesis and quality of life when compared to their previous experience of a traditional socket.
Impact Statement:
This is a first of its kind study reporting on the lived experiences of those who have undergone OI. The field of amputation rehabilitation is expanding rapidly and knowing how this procedure impacts quality of life is important for healthcare professionals to understand as new frontiers are explored in this field.
Introduction
There are approximately 1.6 million individuals living with limb loss in the United States alone. 1 There are many reasons a person may experience limb loss including but not limited to a traumatic event/accident, vascular insufficiencies, and congenital anomalies. However, a vital aspect of the history of limb loss, particularly in the United States, is attributed to injuries suffered from those who participated in historic battles and wars. 2 Because of this, money, time, and resources have been dedicated to the reintegration of those with limb loss back into everyday society. 2 This effort has directly influenced the innovation of prosthetic devices throughout history with the hopes of creating a smoother transition back into daily activities for those returning from positions of war. 2 Prosthetic innovation has since been implemented into civilian populations as well due to learned experiences from the military, though research is still taking place regarding the impact of limb loss on the veteran population. 3 With advancements in prosthetic componentry and a diverse population using prosthetic devices, prosthetists are challenged with adapting devices to accommodate the many functional needs of individuals who sustain limb loss. Prosthetic sockets as known today were developed in the late 19th and early 20th century; Parmelee developed the first suction socket in 1868, and Riedel developed the first tuber enclosing socket in 1911. 4 Since then, prosthetic componentry has advanced through design and implementation to accommodate functional tasks of the population including swimming, running, climbing stairs, grasping, and many others, including the sub ischial socket since 2000. 5 Despite the advances however, traditional sockets (TS) have been the primary choice of application to the residual limb for suspension of the prosthetic device.
After decades of research, the TS is currently considered the standard of care for those who have suffered limb loss, and many patients with amputations have opted for this option. 6 However, research shows that as much as one-third of traditional socket users are dissatisfied with the function and comfort of their prosthetic limb. 7 Common problems of those who use a traditional socket can include chronic skin issues, pain in the residual or opposite limb, low back pain, and anatomical asymmetry leading to poor or inefficient gait mechanics. 8 There is also research to support that satisfaction of a patient with their prosthesis plays a main role in gaining mobility and participating in desired activities, as well as overall compliance with the prosthetic device. 9 Because of the connection between a patient’s mobility and satisfaction with their prosthetic device, it is important to find solutions to various problems that can arise from the use of a traditional socket. Many researchers have looked for the answer to these common problems seen with traditional socket users, one solution being the use of Osseointegration (OI), particularly in lower limb amputations. 10
OI is defined as the direct structural and functional connection between living bone and the surface of an artificial metal implant. 10 This concept was initially used with dental implants, 11 but has been modified as an alternative solution for those with limb loss. 12 The implant itself consists of the bone anchored implant as well as a transdermal component, often called an attachment site or abutment, that protrudes outside the skin to allow for the attachment of the prosthetic limb itself. 12 This implant requires a surgical procedure that often involves both orthopedic and plastic specialties to complete. There is currently only one Osseointegration Procedure that is FDA approved within the United States: The Osseointegrated Prostheses for the Rehabilitation of Amputees (OPRA) system, which consists of 2 stages. 12 This procedure was officially approved in December of 2020 for above the knee (AKA), or transfemoral amputations. The OPRA system utilizes a screw fit mechanism in which the implant is screwed directly into the bone. Currently, the OPRA system is only approved for those who did not have success with a traditional socket. 13 The process of receiving OI includes both a surgical phase and rehabilitation phase. The rehabilitation phase consists of both a preoperative and postoperative phase to ensure the highest success. 12 The alternative to the OPRA system is the Osseointegration Group of Australia Accelerated Protocol (OGAAP) procedure. 14 This procedure is a single step procedure as opposed to a 2-step procedure, which may reduce overall recovery time. This procedure is also a press fit mechanism as opposed to the traditional screw fit mechanism. 14 The press fit mechanism is inserted deeper into the bone which may allow for a larger load bearing capacity, though there is still room for research on the best method.
Some research has reported the effectiveness of OI as a solution for those with limb loss, including pros and cons, different types of procedures to accomplish it, and which extremities OI could be used for.6,15,16 The main advantage to OI is the implementation of Wolff’s Law in that the increased forces applied to the femur will create a remodeling to make bone stronger and over time decrease bone thinning; this is due to the direct connection between the implant and the bone, allowing ground reaction forces to be directly transferred into the bone, leading to improved prosthetic suspension. 15 This does require patients to have adequate bone mineral density to be considered for the OI procedure. Due to this, there is no socket fit issue and following rehabilitation, donning and doffing the prosthetic is much easier. 15 The main disadvantage of OI can be infection, as the implant requires a stoma. 15 Additionally, there could be unexpected events such as mal-union, fracture, or increased pain in the bone. These risks could also include cost or availability of replacement components or the need for follow up surgeries. 15 Though there has been much research into OI as an alternative solution for those with limb loss, there is very little research that has pertained to the patients’ lived experience and conclusions of their overall function and quality of life with OI, particularly in comparison to the use of a traditional socket. In response to declining levels of satisfaction with TS use and the emergence of OI procedures, the purpose of this qualitative phenomenology was to explore and understand the first-hand lived experiences of patients with limb loss who have transitioned from a traditional socket to OI regarding their overall quality of life and function.
Methods
Study selection
A qualitative phenomenological study was designed and conducted following Institutional Review Board Approval. To understand the lived experience from the vantage point of the participant, the researchers considered their own beliefs and feelings about OI. Through a process of bracketing, the researchers initially identified what they expected to discover and then deliberately put those ideas aside in the creation and development of an interview guide. Prior to the development of data collection and instrumentation methods, authors met on 2 occasions to review research and experience evidence pertaining to the lived experience of those with OI. The authors used the process of bracketing to identify an expected phenomenon based on available information to date. To prepare for interviewing participants, the expectations were revealed, identified, and discarded. It was identified that there were strong positive and negative perceptions of OI. Positively, OI was perceived as a solution to the consistent issue of poor fitting sockets, an opportunity to restore a more natural junction between anatomy and prosthesis, and a utilization of novel technology/surgical techniques. Negatively, OI was perceived as a heedless or unnecessary intervention, increasing vulnerability to infection, poor outcomes, and other adverse events.
Data sources and searches
In order to develop an interview guide for analysis of the lived experience of participants, a review of literature was conducted. No specific outcome measure dedicated to assessment of quality of life (QOL) for patients who have undergone orthopedic OI procedure were identified. A structured interview guide and script were developed for collecting patient data. To increase the psychometric properties of the interview guide, components of existing QOL outcome measures intended for individuals with amputation were used. The interview guide included several adapted questions from The Short Form Survey (SF-36), The Questionnaire for Persons with Transfemoral Amputation (Q-TFA), 17 the Prosthesis Evaluation Questionnaire (PEQ), 18 and the Orthotics Prosthetics Users Survey (OPUS). 19 Finally, open-ended questions geared toward understanding the lived experiences of those who underwent OI were included in the final interview guide, Supplemental Appendix 1.
Data extraction and quality assessment
Selection of interview components relied on a researcher scoring system, where each researcher graded every question from 0 to 4 on relevance to individuals with OI, in which a score of 4 was the highest relevance. Each researcher was given the opportunity to justify a low graded component of these outcome measures for adaptation to the interview script, and only 7 questions were added after initial average relevance grades of 2 or less. There were also only 2 script components included that initially had a relevance grade of 1. The foundation of each question was not changed when added to the interview script. However, certain words or question endings were adapted to allow for each participant’s elaboration on their experience pertinent to the difference between OI and traditional socket use. For example, one script bullet point from the PEQ was adapted from “rate how much you sweat inside your prosthesis” to “rate how much you sweat around the attachment site [OI stoma].” Following unanimous agreement and completion of the interview guide, pilot interviews were conducted on a licensed physical therapist who specialized in prosthetic care and a participant who had undergone OI. Following the pilot interview, the interview guide was modified for grammar and ease of interpretation, but content and questions were finalized for data collection in the research study.
Inclusion criteria were determined with consideration for different types of amputation, availability, and access to OI and each participant’s time of socket and OI use. The inclusion criteria were: (1) Participants had to be over 18 years of age. (2) Participants had to speak primarily English. (3) Participants had to have had amputation and have been a traditional socket user for at least 1 year prior to OI
Data synthesis and analysis
Following IRB approval, the study was advertised and posted via social media support groups for individuals/families who have undergone OI and at a local prosthetist’s office. The flyers contained study and contact information for potential participants to be contacted for screening for study eligibility. Participant screening was performed with a short phone call, in which each potential participant was asked to confirm each component of inclusion criteria.
Once participants were screened for eligibility and scheduled for a virtual interview, the participant was provided with a direct link for a video conference. Participants were given approximately 1 hour to complete the interview. Participants were given the opportunity to consent for participation at initiation of the interview. The interview was conducted by 2 research authors in a semi-structured format using the accepted interview guide. This gave researchers the opportunity to probe or follow up on components of the interview guide that would provide more information data to fully understand the participant’s answer and experience. Interviews were carried out with a minimum of 2 researchers taking field notes and the sessions were recorded and transcribed for review. Field notes typically consisted of a researcher dictating participant responses with a paragraph or less per question. Direct quotations that were deemed impactful, important, or unique from participant to participant were also noted separately. Upon termination of the interview, participants were offered a gift card as compensation for their time and responses.
Field notes taken during interviews were recorded in a data collection form for each participant to allow for analysis of participant’s answers. The goal of data collection was to achieve saturation of participant responses, in which trends and similarity of each experience began to become consistent. Interviews were recorded and transcribed. The researchers then reviewed transcripts and field notes and utilized thematic analysis methods as described by Braun and Clarke 20 to analyze the data. Field notes were used as a comparison and guide to the transcripts to triangulate the data. Following the methods the authors described, the interview guide was first divided into components and all responses were coded and themed within the construct measured, which included: open-ended satisfaction, function, pain, prosthetic training, quality of life, and clothing. Then, 2 independent researchers then performed a first round of line-by-line coding, using field notes and interview transcripts to produce codes for each section of the interview. These researchers then performed a second round of line-by-line coding and then met to discuss the similarities and if there were disagreements on the specific codes generated. All disagreements were discussed so that the second round of line-by-line coding produced agreed upon codes. Finally, an expert researcher reviewed the mapping process from transcripts and each round of coding. Any questions were reviewed as a group and final codes were unanimously decided on. This data was then used to synthesize themes relevant to the lived experiences of this study. Saturation was achieved after interviews with 10 participants.
Results
Eleven participants were screened and were eligible to participate in the study by meeting the inclusion criteria. Please see Table 1 for participant demographics. Participants consisted of 6 females and 5 males residing within the United States (8) and Australia (3), with an average age of 56.8 years. Individuals within our study had histories of 2 to 36 years of experience with traditional sockets and ranged from 3 to 7 years post-OI procedure. Ten participants sustained transfemoral amputations and had a one-step OI procedure. One participant received the 2-step procedure. One participant (Participant 4) was initially enrolled in the study via population screening but was removed from the analyzed data as it was found they had a transtibial amputation and were considered a population outlier. The final analysis includes data from 10 participants. It is important to note the current health status of the participants since health status could affect the participant responses to subjective and objective questioning. Figure 1 demonstrates participant health status in the previous year prior to participation in this study.
Participant demographics.

Participant 4 has been removed from the analyzed data as it was found they have a transtibial amputation and are considered a population outlier.

Current health status impacting quality of life.
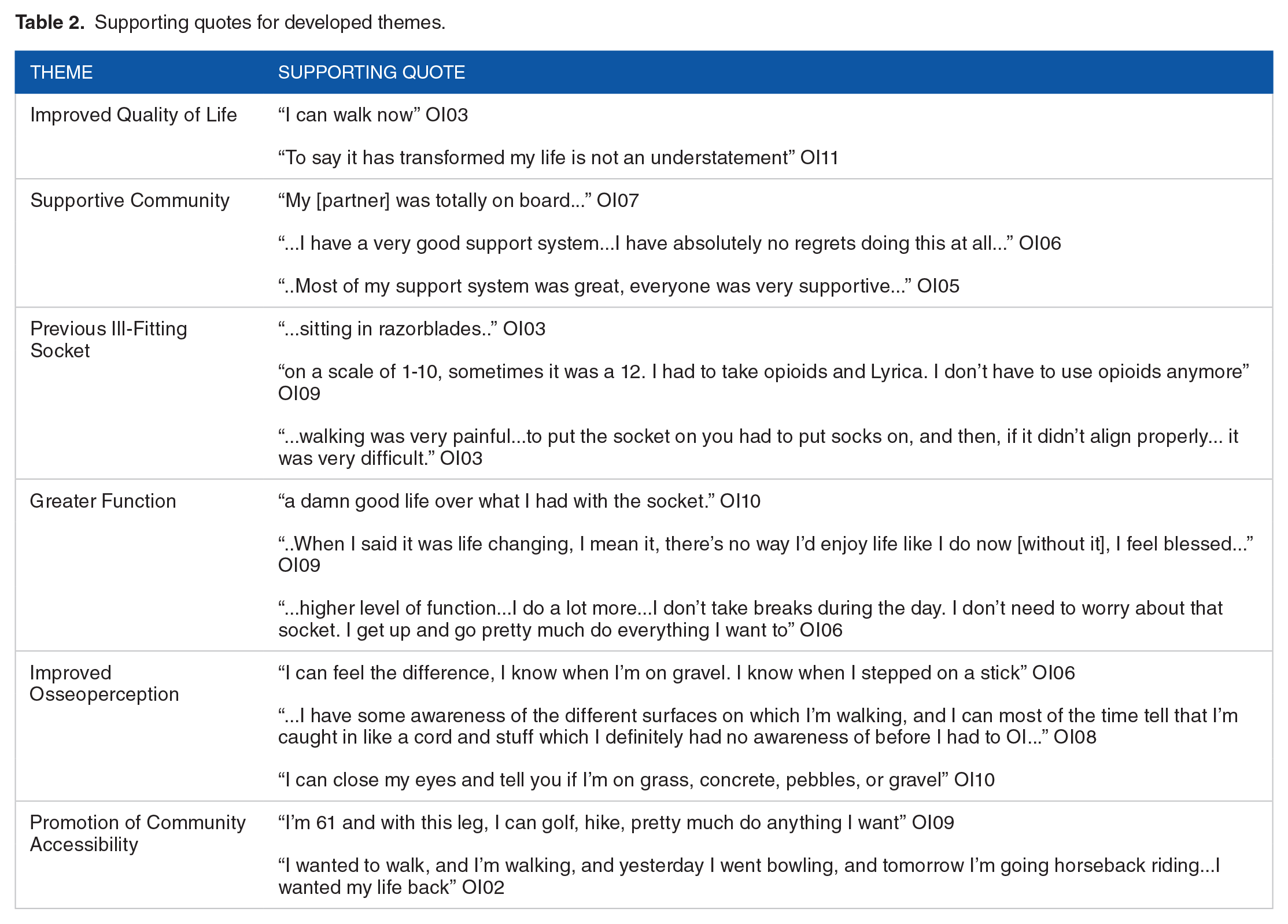
The thematic analysis portion of this study demonstrated an emergence of 6 main themes including "Improved Quality of Life”, “Supportive Community,” “Previous Ill-fitting Socket,” “Greater Function,” “Improved Osseoperception,” and “Promotion of Community Accessibility.” These themes were derived from codes that were developed from 485 participant responses. The codes achieved saturation throughout the 10 analyzed interviews. Supporting quotes for the following themes are presented in Table 2.
Supporting quotes for developed themes.
Theme 1: Improved quality of life
With the interview question “What is the most positive aspect about OI?,” all analyzed participants responded with feeling as if they have improved quality of life compared to living with a traditional socket. When referring to quality of life with a traditional socket, 8 participants stated they had decreased satisfaction with their life, and 2 participants stated they experienced suicidal thoughts due to pain and a low quality of life. An important quote includes: “I always had to plan my day and life around the socket and how my leg was feeling that day and now I do not have limits to anything I do because of my socket.”
It is important to note that infection risk of the abutment site is a negative aspect of the OI procedure that plays a role in perceived quality of life. An important quote includes: “I know that infection is common so I just have to make sure to keep cleaning it regularly, that is one thing I think about more now, but it doesn’t hinder me as the infections are usually minor.”
Theme 2: Supportive community
Multiple questions addressed participants perception of support from their community during their process of obtaining the OI procedure. A majority of individuals experienced supportive responses by partners and family members, close friends, and their health-care team. An important quote includes: “Any fear I had was gone with the love and support of my family. They know how much I suffered so anything that promised help was something they were going to join me in.” There was also an overwhelming difference in the satisfaction with the quality and intensity of rehabilitation after the OI procedure as compared to the instruction and training that was received after the initial amputation. An important quote includes: “I felt like the rehabilitation was of higher quality maybe because those therapists and team members were specifically trained in how to help someone like me.”
Theme 3: Previous ill-fitting socket
With interview questions regarding seasonal changes and sweating inside the traditional socket, all 10 analyzed participants reported excessive sweating. After the OI procedure, all 10 analyzed participants reported no sweating issues, and 9 participants reported decreased skin irritation. All of the participants decided to undergo the OI procedure due to ill-fitting sockets due to short or difficult-to-fit residual limbs. An important quote includes: “There is no doubt that the socket cannot be fit perfectly to your leg. . .and those issues are now gone and it is freeing.”
Theme 4: Greater function and theme 6: Promotion of community accessibility
With the interview question “Did pain interfere with your activities (including both work outside the home and household duties)?,” all participants responded that pain limited their level of function before the OI. After the OI procedure, most participants reported no pain, or a decrease in pain to a level that allowed them to be more functional. An important quote includes: “Much of the pain was due to the socket and some phantom limb pain. Now the socket is gone and the phantom limb pain even feels less, but not gone.” This is also demonstrated in the functional task results which were aggregated in Figure 4. Figure 4 includes tasks such as standing, sitting, and ambulation with a bilateral upper extremity task (such as carrying). Participants also reported a decrease in phantom pain, decrease in back pain, and a decrease in sound limb pain due to a decrease in compensatory gait and functional movement patterns.
Theme 5: Improved osseoperception
Interview questions addressing ability to negotiate various terrains and individuals’ perception of different surfaces demonstrated an improvement in ability to detect changes while ambulating. No participants described their ability after the OI as decreased from their previous socket wear. Perception of ground was recorded as no change or improved compared to traditional socket use. In addition to improved osseoperception, certain individuals noted a decrease in falls during ambulation. Prior to the OI procedure, participants stated a history of falls secondary to a lack of recognition of ground surfaces. When asked about improved ability to detect changes in surfaces during walking, participants verbalized that they believed their improved ability with osseoperception contributed to diminished falls. An important quote includes: “I can actually feel different surfaces now. . . it is amazing!”
Analysis of function
The interview guide created included closed-ended questions from validated outcome measures. Analysis of function through wear time and functional tasks was performed by asking each participant to provide this information. The authors aggregated the sample to provide the cumulative responses of the sample to demonstrate the overall importance of wear time and function in our sample’s lived experience. On average, the participants reported they were wearing the traditional socket 5.9 days out of the week. After the OI procedure, they are wearing their prosthetic 7 days a week, an 18.64% increase in daily wear. Figures 2 and 3 depict wearing schedule before and after. Total daily wearing time demonstrated a 133.4% increase, with the average total wearing time with the traditional socket being 6.68 hours/day, and total wearing time with their OI procedure being 15.59 hours/day.

Wearing schedule for participants before osseointegration.

Wearing schedule for participants after osseointegration.
The Functional Task portion of the interview resulted in a clear difference in functional ability prior to OI versus after the procedure. Figure 4 artwork depicts the number of participants who could complete 6 specific tasks before and after the OI. These 6 tasks were presented as a yes/no question to the participants on whether they could complete the task successfully. Overall, 38% of the participants reported they could complete the tasks while wearing their traditional socket. Eighty-eight percent of the participants reported they can currently complete the tasks after the OI procedure, a 131.6% increase in overall function.

Frequency distribution of functional task completion.
Participants also rated 13 additional tasks on their perceived ability to complete the task. Participants rated each task on a scale of 1 = Very Limited, 2 = Moderately Limited, and 3 = No Limitations. With a total possible score of 39, the average total score with a traditional socket is 25.36. The average total score with OI is 36.18. The difference is an average increase of 42.7% in perceived ability to complete the tasks successfully. Figure 5 artwork depicts the average scores per task comparing the participants answers based on their experience with the traditional socket and their experience with OI. Since the functional task questions were generated from validated instruments, the improvements noted were: standing without discomfort, walking and carrying objects, sitting in all surfaces, cycling, sit to stand from floor, stair management, walking one block, bending, kneeling, or stooping.
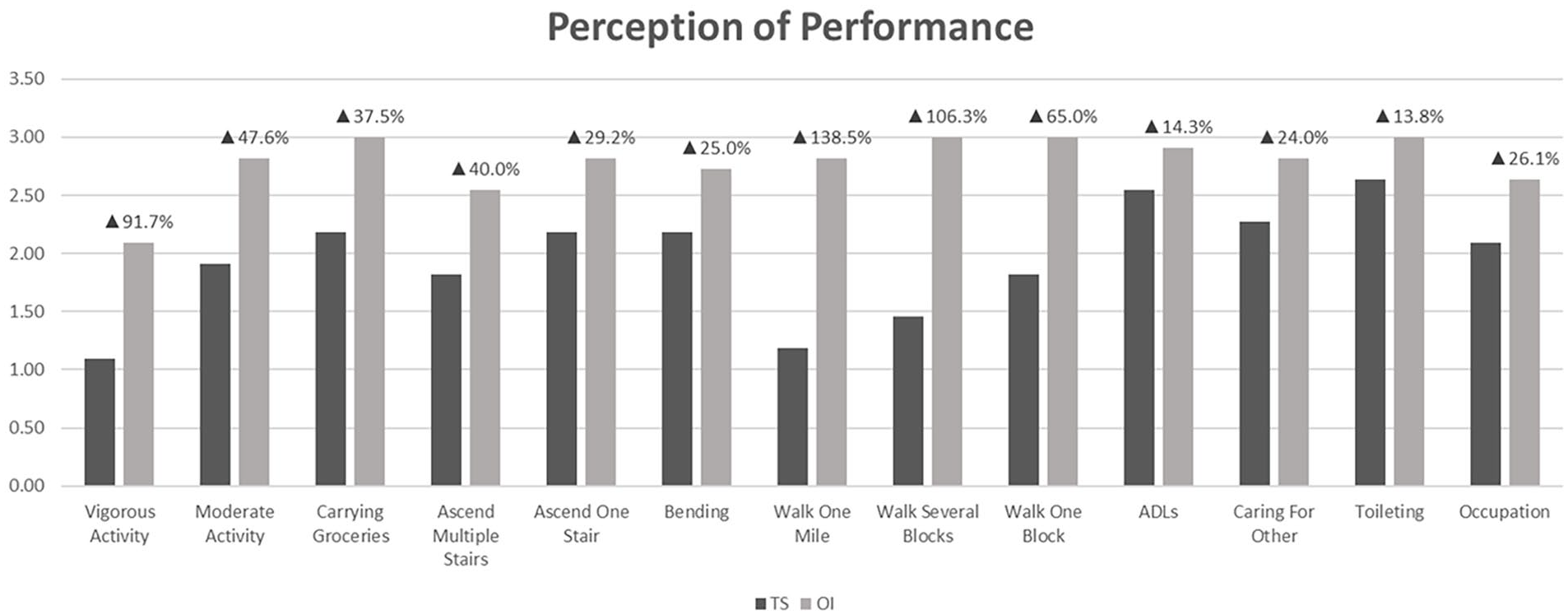
Perception of performance limitation on functional tasks before and after osseointegration.
Discussion
This study aimed to explore and understand the first-hand lived experiences of patients with limb loss who have transitioned from a traditional socket to OI in regard to their overall quality of life and function. This study found that the lived experience of those undergoing the OI procedure appears to contrast with an initial amputation and subsequent traditional socket use. The positive life changes verbalized by participants as well as descriptions of what activities and abilities an individual with OI is now able to engage in support the statement that quality of life is improved after the OI.
When referring to life with a traditional socket, participants of the study stated moderate to severe limitations in their ability to engage in their environment, hindering their quality of life. Despite previous functional or health status limitations before their amputation and during traditional socket wear, each participant expressed a level of difficulty that impacted their quality of life negatively. This persistent theme among the participants is not unique to the OI patient population, but rather summarizes some socket users’ experience with a traditional socket regardless of their decision to transition to OI. 7 The impact of function, participation, and perceived ability is interconnected with quality of life. The themes most reported based on the participant codes reiterated this sentiment with resounding repetition. The study findings echo that quality of life, as described by the participants, is increased in comparison to use of a traditional socket as it presents with minimal limitation functionally.
In addition to limited quality of life or function, participants expressed discomfort secondary to their socket use. For the participants within the study, the traditional socket created a host of skin issues such a breakdown, chafing, sores, and blistering giving rise to pain and mobility limitations. Participants expressed a dissatisfaction with the previously mentioned diminished quality of life but also the constant discomfort experienced when attempting to interact with their environment while wearing a traditional socket. These findings suggest a theme of poor fitting sockets or that socket wear is not appropriate for long term satisfaction with a prosthetic device. Previous studies support the notion that traditional socket wear creates a host of skin issues and is common. 21 Our study sought to see if skin problems remained in individuals with OI. With the OI prosthesis, patients reported no chaffing or skin breakdown with minimal to no effects of temperature on device wearing. The main concern participants expressed throughout the study was the increased infection risk with OI due to the opened wound on the stoma. Participants acknowledge the risk but reported understanding signs of infection and how to contact their provider. They also understood that most infections are superficial and easily treated. Despite an unclosed wound, participants with OI report minimal to no current heightened concern for future skin issues or impairments. Participants prior to the OI procedure were educated on the severe signs of infection and made aware of the potential risks. Additionally, no participants within this study experienced a severe infection secondary to stoma infection. These conclusions allude to OI appropriateness for individuals severely affected by the skin irritation or discomfort caused by traditional socket use. These findings also suggest that despite possibility of infection, the benefits reported by participants with OI such as improved function, quality of life, and participation are worth the potential risk of infection. Participants noted an increased sense of osseoperception now with OI, and that feeling surfaces is important for mobility needs, but further exploration beyond this finding is warranted.
It is evident that adherence, comfort, and mobility improve with OI based on the lived experiences described by the participants in this study. For a prosthesis to be an effective option, minimal pain and maximal fit must be achieved to promote mobility and interaction with environment. Prior to OI, participants expressed decreased adherence to wear schedule because of discomfort and limitations in function, as previously stated. Based off the findings in this study, OI is presented as a relevant solution and contributor to patient function and mobility. With OI, increased adherence is achieved, per patient report, as participants consistently describe increased comfort and ease for donning/doffing their prosthesis. With promoted compliance and consistent wear schedule, the individuals within this study emphasized an ability to return to activities they once enjoyed, participate in meaningful experiences, and participants reported an overall increase in functional independence. These findings demonstrate that OI when compared to traditional socket wear may be more comfortable. Because of the improved comfort experienced in the study, prosthetic device compliance was increased allowing for function that is no longer restricted because of pain.
Lastly, the participants represented by this data, based on their improvements in quality of life, participation, community navigation, and pain management, are clear in their improved greater function. Prior to OI, participants voiced concerns with ability to navigate environments, enjoy previous hobbies and participate in their daily life. These statements can be reflective of previous long-term effects in patients with TS. 8 When considering the improvements found in compliance to wear schedule, improved comfort and decreased pain, Figure 4 demonstrates the overall significant change in ability. Not only did participants perceive an improved ability to complete functional tasks, but their perception of the performance of tasks is improved as well (Figure 5). Every participant rated their perception of performance after OI higher than their previous experience with TS. An increased ability to perform functional tasks is important for individuals negotiating their environment but an improvement in perception as well is significant in promoting a mindset of capability. All participants reported a level of same or improvement for the following functional tasks: standing without discomfort, walking and carrying objects, sitting in all surfaces, cycling, sit to stand from floor, stair management, walking one block, bending, kneeling, or stooping.
Study strengths and limitations
Strengths of the study include that this is one of the earliest studies to describe the phenomenon of OI procedure in the words of participants who have undergone OI. This study utilized the lived experience of participants with OI and their perception on function, pain, and participation while comparing it to a previous traditional socket. There are limited outcome measures currently validated for the population with OI. This study’s questionnaire utilized modified outcome measures validated in patients with amputations. This study also included international participants which contributed to diversity of life experience and interview answers. Finally, this study utilized thematic analysis for identification of relevant themes within participant responses. This created a systematic model for gathering qualitative data and the result was an accurate representation of each participant’s experience.
Limitations became relevant throughout each stage of this study. Although the participant responses achieved saturation, the sample size of this study was small. A larger sample size could confirm major themes and offer a more detailed picture into the preconceived notion this study aimed to address. Another limitation is the specific patient population targeted. The candidates for OI at this time are primarily those with traumatic amputations, excluding individuals who have received an amputation due to vascular disease or pre-existing conditions. More research would be beneficial in determining the experience of individuals without traumatic cause to see if OI would be an appropriate option moving forward for a wider population. Additionally, OI is considered a revision surgery and is not available as a primary amputation technique. Individuals receiving this procedure had the opportunity to assess previous experience with a traditional socket. More research is necessary to determine if individual perception of OI would be different if it were a primary amputation technique rather than a revision surgery after incompatibility with a traditional socket. The selected participants within this study were advocates for the OI procedure because of this stance, our study did not address the perspective of an individual with a negative perception following OI. Future studies addressing individuals who recommend versus those who do not recommend the OI procedure and their respective reasoning is important to determine if the discovered themes remain consistent.
One participant received the OI procedure near the start of the COVID pandemic. Due to the timing of their rehabilitation, they were unable to attend outpatient Physical Therapy. Similarly, this study is limited in the fact that each patient’s experience with rehabilitation after initial amputation was variable. This limits the study in the ability to determine the effect of a patient’s initial rehabilitation intervention on their quality of life with a traditional socket compared to after OI. Therefore, this participant’s responses toward the type and quality of gait and prosthetic device training received were different than responses of other participants who were not affected as greatly by the timing of the COVID pandemic.
Conclusion
OI as a revision option demonstrates promise to the individuals who fit the patient criteria. Individuals who have undergone OI are more satisfied with their prosthesis and overall quality of life when compared to their personal experience with use of a traditional socket. The qualitative data and thematic analysis demonstrate a greater function with the use of OI and improved overall quality of life. Additionally, the objective data measuring wear time and ability continues to suggest the notion that OI promotes improved participation within an individual’s environment and community. More research exploring these themes and findings is needed to further solidify OI’s contribution to the current patient population it is appropriate for, and to consider additional patients that this procedure could benefit.
Supplemental Material
sj-docx-1-rpo-10.1177_27536351241271538 – Supplemental material for Qualitative Analysis of the Lived Experience of Individuals After Undergoing Osseointegration for Transfemoral Amputation
Supplemental material, sj-docx-1-rpo-10.1177_27536351241271538 for Qualitative Analysis of the Lived Experience of Individuals After Undergoing Osseointegration for Transfemoral Amputation by Michael Furtado, Joseph Carneglia, Rebecca Fletcher, Lindsay Spitaletto and Summer Swift in Advances in Rehabilitation Science and Practice
Footnotes
Acknowledgements
We would like to thank all the participants who agreed to be interviewed for this study. Crossing time zones in Australia can be a challenge, but everyone was so gracious and we are grateful for their meaningful contributions.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.