
Abstract
Case Description:
Osseointegration is a relatively new technique for prosthetic limb attachment that offers various improvements for patients with amputation and facilitates joint preservation. We present a case of implant loosening during rehabilitation in a patient with transtibial amputation that was successfully managed through a combination of measures, aiming to promote re-osseointegration of the implant.
Objectives:
Not much is known about structured management of adverse events after osseointegration. Septic or aseptic loosening is currently regarded as implant failure, prompting removal and possible re-implantation at a later stage. The objective of this case report was to evaluate the feasibility of salvaging a loosened implant.
Study Design:
Case report.
Treatment:
A novel treatment approach was employed to enable renewed osseointegration of the implant. First, the bone-implant interface was disrupted and renewed through axial rotation and distal repositioning of the implant. Afterwards, extracorporal shockwave therapy and antibiotic treatment were administered. Prosthetic rehabilitation was then started anew. Regular follow-up x-rays and clinical evaluations were conducted, including standardized outcome tests.
Outcomes:
These combined measures led to a successful re-osseointegration of the implant. In a 21-month follow-up, the patient regained a stable and secure gait pattern, using his prosthesis every day for 15 hours and scoring above average on standardized outcome measures.
Conclusion:
This represents the first report of implant salvage after failed primary osseointegration. As the associated risks of this novel treatment are very low, investigations are warranted to evaluate this approach on a larger scale.
Background
There is a growing body of evidence for the safety and efficacy of osseointegrated prostheses to treat extremity amputations of different levels.1–3 Reported advantages compared with regular socket prostheses include increased comfort, higher range of motion, faster donning and doffing, a more stable mechanical connection, and improved vibrotactile feedback via bone conduction.4–6 These factors generally result in prolonged daily prosthetic use as well as an overall gain in quality of life for the patient. 7 However, orthopedic implants, in particular those with a transcutaneous port, entail a constant risk of infection and failure. While superficial infections after osseointegration can be effectively treated with oral antibiotics in most cases, deep infections frequently result in implant failure and loosening. 8 Rates of long-term implant survival are well reported for the transfemoral level, roughly ranging between 90% and 100%, depending on the system employed, cohort size and follow-up time. 9 Regardless of implantation level, septic or aseptic loosening is generally considered a failure of the implant and prompts surgical removal. 10 To our knowledge, no clinically successful strategies have been described to salvage an implant in such a situation.
Case description and methods
The patient reviewed the manuscript, including all images, and approved publication. We report of a 30-year-old male patient, who approached our center with regard to prosthetic reconstruction after a short transtibial amputation of his left leg. He was a non-smoker without secondary diseases, at the beginning of his working career, and leading an active life as father of a young child. Five months earlier, the patient had sustained a work-related accident involving a forklift, which injured his left lower leg, including multiple fractures and extensive soft tissue destruction. Despite multiple reconstructive efforts, the leg could not be saved, and a transtibial amputation was performed with a remaining tibia length of 15 cm. Because of the extensive soft tissue loss, the residual limb had to be covered entirely with split thickness skin grafts (Figure 1(a)). Unstable skin and shortness of the residual limb rendered the fitting of a conventional socket prosthesis impossible. Even compressive garments applied to the residual limb resulted in ulcerations and pain. Therefore, shortening to a transfemoral level was considered.
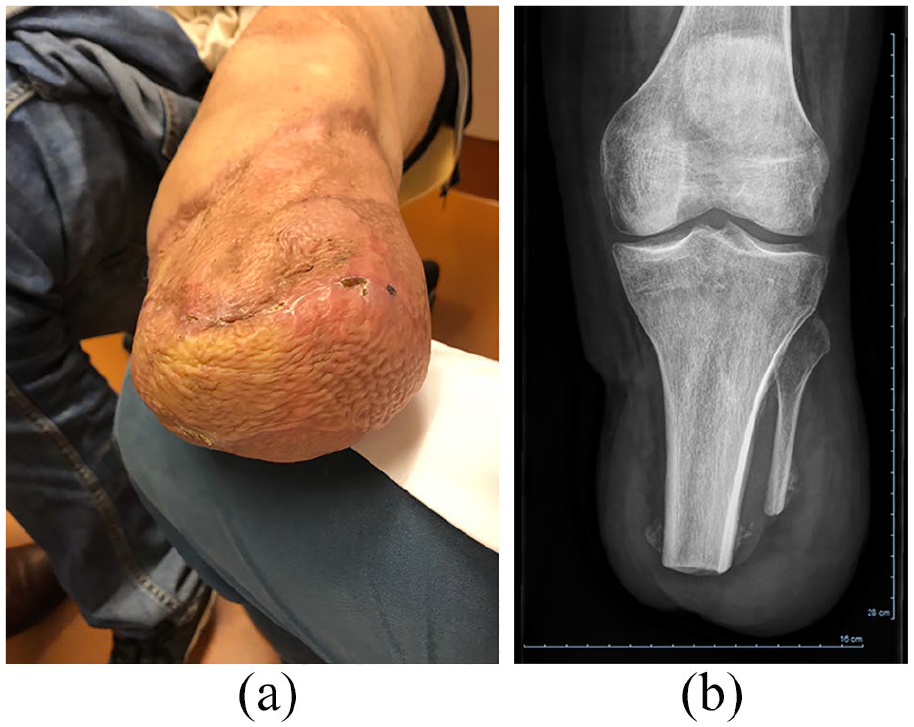
(a) Residual limb during initial presentation of the patient, showing the split-skin grafted areas. (b) The corresponding x-ray reveals a residual tibia length of 15 cm.
After the initial consultation, x-ray and computer tomography (CT) scans were performed, revealing good bone quality of the tibia (Figure 1(b)). We thus proposed an osseointegration procedure with the OPRA system (Integrum, Sweden), with the aim to facilitate a stable prosthetic attachment while preserving the knee joint. The two-stage surgery was performed over a 3-month interval. Three weeks after the second surgery, the last sutures were removed and the patient was instructed to slowly initiate axial loading on a regular weight scale using a training prosthesis. Starting with 10 kg in daily sessions, this was increased in weekly intervals until he reached bodyweight, taking care not to cause any pain during the process of 5 or more on a visual analog scale (VAS). The residual limb was inconspicuous in presentation throughout rehabilitation, with a dry and stable port (Figure 2(a)). The patient then received the first prosthesis for gait training, which was regularly supervised by our physiotherapist. The prosthesis initially included a size 26 prosthetic foot (1D35, Otto Bock Healthcare, Germany), which is two sizes smaller than the patient’s shoe size, in order to reduce shearing forces on the implant during early rehabilitation. About 5 months after stage two surgery, the patient was able to walk without crutches for short distances. He subsequently entered an inpatient training program at a rehabilitation center to further improve gait stability and duration. Prior to admission, a control x-ray of the residual limb was performed, showing unchanged position and no signs of lucency around the implant (Figure 2(b)).
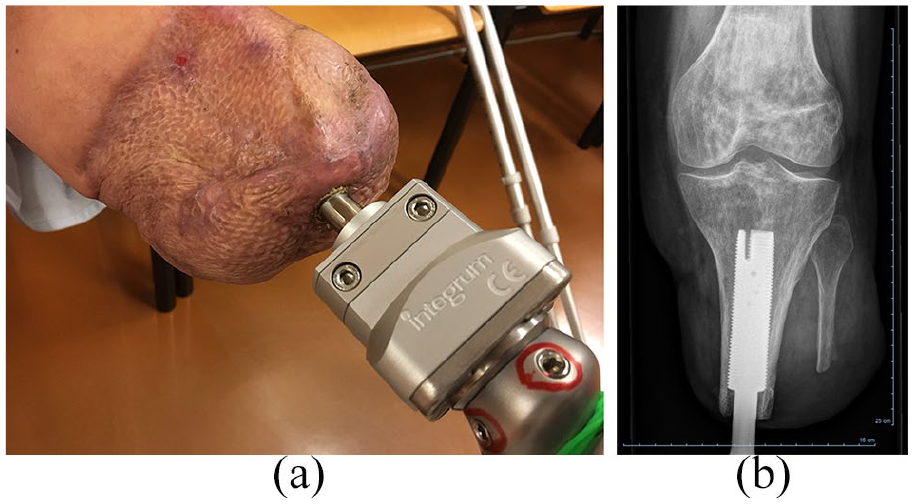
(a) Residual limb of the patient after osseointegration, showing a dry, inconspicuous port. (b) X-ray of the implant performed 5 months after stage two surgery, before starting inpatient rehabilitation.
During the rehabilitation program, the patient suddenly noticed rotational instability of the abutment, as well as increased secretion from the port. This occurred after a long training session on a treadmill, approximately 6 months after the stage two surgery. The patient was immediately told to stop loading. Clinical examination unfortunately confirmed slight rotational instability, which allowed a 1 mm rotation of the abutment to either side upon manual manipulation, thus indicating a loosening of the implant. However, neither x-ray nor CT scans revealed any signs in that regard. Since clinically the failed osseointegration of the implant was apparent and it did not improve during 6 weeks of unloading, removal of the implant was considered. However, because of the lack of definitive loosening indicators radiologically and also because of inadequate soft tissue availability to close the wound after removal, it was decided to facilitate the creation of a new interface between the bone and implant. Under full anesthesia, the implant was carefully rotated counterclockwise, to disrupt the interface and to create a hematoma. It was thereby moved distally, until a new and stable contact to the cortex was felt. No skin incision was necessary for that procedure. Afterwards, still under anesthesia, the patient received extracorporal shockwave therapy of his residual limb, with 3000 shockwaves at a frequency of 4 Hz (Orthogold 280, MTS Medical, Germany). A follow-up x-ray showed a distalization of the implant of 5 mm, with good contact to the cortex (Figure 3(a)). Oral antibiotic therapy was subsequently prescribed for 8 weeks, using a combination of trimethoprim and clindamycin. The rehabilitation process was restarted 6 weeks after the procedure.
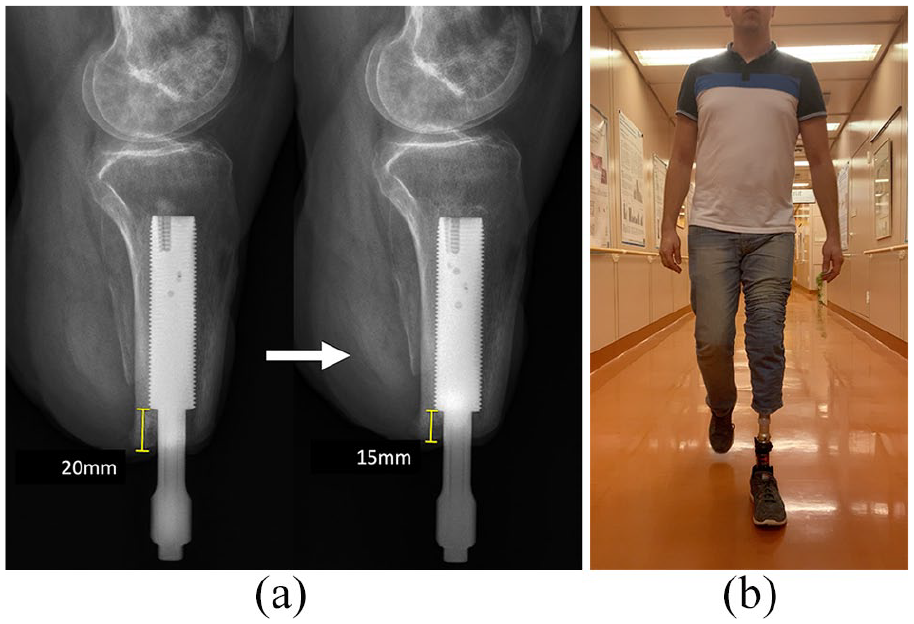
(a) The left image shows a lateral x-ray which was performed 2 months after stage two surgery. The right side shows a follow-up x-ray which was performed 4 weeks after the repositioning of the implant and subsequent shockwave therapy, displaying its more distal position with decreased distance to the bone ending (20–15 mm). (b) The patient during gait at a follow-up visit, 15 months post stage two surgery.
Findings and outcome
The second prosthetic rehabilitation went without further complications or delays. The patient finished the axial loading phase after 2 months and then started again with a gait prosthesis, initially with a shorter prosthetic foot. His gait pattern and stability progressed with physiotherapy until he was able to stop using crutches about 5 months after the intervention. The skin of the residual limb was inconspicuous in presentation throughout rehabilitation. At a follow-up 15 months post stage two surgery, he reported using the prosthesis every day for an average of 15 hours, having gained increased trust in the stability of his left leg, and was climbing stairs without restraint. He reported some remaining insecurity when descending stairs without handrails or going downhill over uneven terrain. His gait pattern was stable without compensatory movements and he reported no pain during everyday use of the prosthesis (Figure 3(b)). At the final follow-up at 21 months post stage two surgery, stability and trust of the implant and prosthesis during everyday use had increased further, with the patient reporting descending stairs and walking over uneven terrain without problems or fear of falling. Standardized outcome measurements for lower limb prosthesis users were conducted: the patient scored 6.06s on the Timed Up and Go Test, 4.94s on the Ten-Meter-Walking-Test (which is equivalent to a walking speed of 2.02 m/s) and 640 m on the Six-Minute-Walking-Test (which is equivalent to a walking speed of 1.78 m/s). All scores were comparable or better than average results reported in the literature for patients with unilateral transtibial amputation.11–14 Results of the Trinity Amputation and Prosthesis Experience Scales—Revised (TAPES-R) 15 questionnaire revealed good outcomes for psychosocial adjustment, activity restriction and satisfaction with the prosthetic system. In detail, the following Adjustment Scores were achieved: 4 for the General Adjustment subscale (best possible score), 4 for the Social Adjustment subscale (best possible score) and 2.4 for the Adjustment to Limitation subscale (scale from 0 to 4 with 4 being the best outcomes). The Activity Restriction Scale had a score of 0.6 (scale from 0 to 2 with 0 meaning no limitation in activity), and both Satisfaction with Prosthesis Subscales (aesthetic satisfaction and functional satisfaction) had the best possible score of 3, indicating a high level of device satisfaction. The final prosthetic fitting included a size 28 foot (1C61 Triton, Otto Bock Healthcare, Germany) as well as an eccentric adapter to the implant (AxorTC Excentric, Integrum, Sweden).
Discussion
From a bioengineering perspective, the concept of osseointegration relies on a stable interface between implant surface and osteocytes. In prosthetic limb reconstruction, this requires sufficient contact to the cortex of a diaphysis, which can be easily achieved in long residual limbs at the transfemoral or transhumeral level. However, the anatomy of the proximal tibia is not favorable in this regard. Since transtibial amputations are generally performed at a proximal level to ensure enough room for prosthetic fitting and sufficient soft tissue coverage, a cylindrically shaped implant can only achieve contact to the inner cortex of the bone at its distal aspect (see Figure 2(b)), limiting the stability of the interface. Furthermore, the drop-like cross section of the tibia further reduces the contact area of a cylindrical implant. 16 Rehabilitation in such patients should therefore be conducted carefully, with an emphasis on not increasing loading and bending forces too much too early. Also, if a conventional socket fitting is feasible in patients with transtibial amputation, good outcomes can generally be achieved.14,17 For these reasons, osseointegration is less frequently performed in this population, with so far only two reports published in the literature.16,18
In our patient, osseointegration was the only option to facilitate a prosthetic fitting without shortening by transfemoral amputation. The surgery and initial mobilization were performed without complications. Implant loosening occurred at a late stage of rehabilitation, 9 months after the first surgery. Since no deep cultures could be obtained, it is not clear whether an infection was present or whether aseptic loosening had occurred. However, osseointegration of the implant had clearly failed, as there was no stable connection to the bone. While this situation would normally result in a removal and possibly reimplantation later on, it was decided to instead try to enable a renewed osseointegration through a combination of measures. First of all, the implant was rotated to a new position more distally, in order to disrupt a thin fibrous tissue encapsulation as well as a potential biofilm, aiming to renew the healing process by creating an interfacial hematoma. This was only feasible because good stability between implant and bone could be attained after repositioning. If no stable bone contact had been achieved through rotation, an explantation of the system would have been necessary. Second, extracorporal shockwave therapy was applied to the residual limb directly afterwards. This approach was chosen for its known potential to induce osteogenic differentiation of mesenchymal cells, which is also reflected in clinical reports of its positive effects in situations such as delayed osseous union. 19 In a third step, oral antibiotics were administered according to a standard protocol for implant infections. Together, these measures aimed to disintegrate a potential biofilm, promote osteogenic capacities and treat a possible infection. This combined approach induced a renewed osseointegration process, leading to a positive outcome for the patient. Regarding the first step, rotation of the implant is only feasible in OPRA implants. In press-fit systems, such as the integral leg prosthesis (ILP) or osseointegrated prosthetic limb (OPL), 20 other strategies would be necessary to facilitate interface disruption while maintaining adequate bone engagement and mechanical stability.
Conclusions
To our knowledge, this represents the first report about successful implant salvage after failed primary osseointegration in a patient with amputation. We therefore propose further investigation of this approach in similar cases, as it has the potential to prevent implant removal while posing little risk for serious adverse events.
Footnotes
Author Contributions
CG - conceptualization, resources, writing - original draft, writing - reviewing and editing
SS - conceptualization, resources, writing - original draft, writing - reviewing and editing
RB - conceptualization, resources, writing - reviewing and editing
OCA - conceptualization, writing - reviewing and editing
VM - resources, writing - reviewing and editing
AS - resources, investigation, formal analysis, writing - original draft, writing - reviewing and editing
TH - resources, writing - reviewing and editing
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.