
Abstract
Purpose:
The purpose of this study was to understand how spousal caregivers of people with amyotrophic lateral sclerosis and cognitive and/or behavioural impairments felt about the EMBRACE intervention.
Materials and methods:
A qualitative interpretive study, using individual semi-structured interviews pre- and post-participation in a palliative rehabilitation blended learning programme, was applied. In total, 13 spousal caregivers were interviewed pre-intervention and 10 of them post-intervention.
Results:
Three overarching themes were identified: Striving to Obtain Control in Everyday Life, Peer support Across the Illness Trajectory and The Complexity of Relations. Information provided in targeted videos and sharing experiences with peers in virtual group meetings were beneficial to comprehend, manage and find meaning in everyday challenges related to being a caregiver.
Conclusion:
The EMBRACE intervention helped spousal caregivers cope with everyday needs and challenges related to being a caregiver. EMBRACE was found to support and strengthen the participants in gaining more control in everyday life, creating a sense of coherence. Through targeted videos and discussions with peers, the participants felt prepared for the illness trajectory of their relative. Peer support promoted resilient functioning and reduced their feelings of loneliness.
Clinical trial registration:
This study was registered on clinicaltrials.gov under the name: A Complex Intervention Study on a Palliative Rehabilitation Blended Learning Programme to Support Relatives and Health Care Providers of People with ALS and Cognitive Impairments in Coping with Challenges. ID no. NCT04638608. URL: https://clinicaltrials.gov/ct2/results?cond=&term=NCT04638608&cntry=&state=&city=&dist=.
Keywords
Introduction
Amyotrophic lateral sclerosis (ALS) is a progressive, heterogeneous neurodegenerative disease with no cure 1 with death occurring after a median of 3.2 years. 2 Research shows that there is some degree of overlap between ALS and frontotemporal spectrum disorder, but this does not imply that the spectrum is a continuum, nor does it imply that frontotemporal dementia (FTD) is the endpoint of ALS. 3 Cognitive and behavioural impairments are prominent non-motor manifestations of ALS. 4 Behavioural impairments in ALS are associated with poorer prognosis and risk of death that is 2 to 2.53 times higher than in unimpaired controls. 5 The presence of cognitive and behavioural impairments in these people are a major source of high family caregiver burden, and family caregivers of people with ALS and FTD are 3 times more likely to report higher burden than are those caring for people with ALS without FTD. 4 Family or informal care is defined as unpaid care (without a contractual agreement) carried out by untrained individuals, often relatives and friends. 6 Family caregivers express a need for psychosocial support 7 such as a need to share feelings and viewpoints with people who are in related situations. 8 However, they struggle with limited time, restricted social life and extra responsibilities related to caring for a person with ALS.9,10
Online programmes may enhance accessibility and provide a flexible platform that enables family caregivers of people with ALS to work on programme components where and whenever they have a moment. 11 However, supportive interventions for family caregivers can be complex to evaluate because their effect depends on the synergistic effect between the intervention components, and therefore conclusions tend to be ambiguous. 12 Furthermore, the success of interventions intended to change behaviour is largely dependent upon the participants finding the intervention helpful. 13 It is therefore important to assess the participants’ perspectives on the intervention and to make the necessary modifications to strengthen it, if needed.13,14 Focussing on identifying and refining the active components in an intervention is therefore important to fully understand how an intervention works. 12
Gathering knowledge on the spousal caregivers’ experiences of a specific intervention is necessary to fully tailor a palliative rehabilitation programme supporting spousal caregivers (hereafter caregivers) of people with ALS and cognitive and/or behavioural impairments (hereafter PALS/CIs). We therefore developed a 4-month palliative rehabilitation blended learning programme, named EMBRACE to support caregivers of PALS/CIs in comprehending, managing and finding meaning in everyday challenges related to the affected relative.
The aim of this study was to understand how caregivers of PALS/CIs experienced a palliative rehabilitation blended learning programme named EMBRACE.
Materials and Methods
Design and setting
A qualitative interpretive study design was applied. The study was conducted at the Danish National Rehabilitation Center for Neuromuscular Diseases (RCFM). This study is embedded in a larger research project, the EMBRACE intervention, which is guided by the British Medical Research Council (MRC) framework for developing and evaluating complex interventions in health.15,16
The EMBRACE intervention
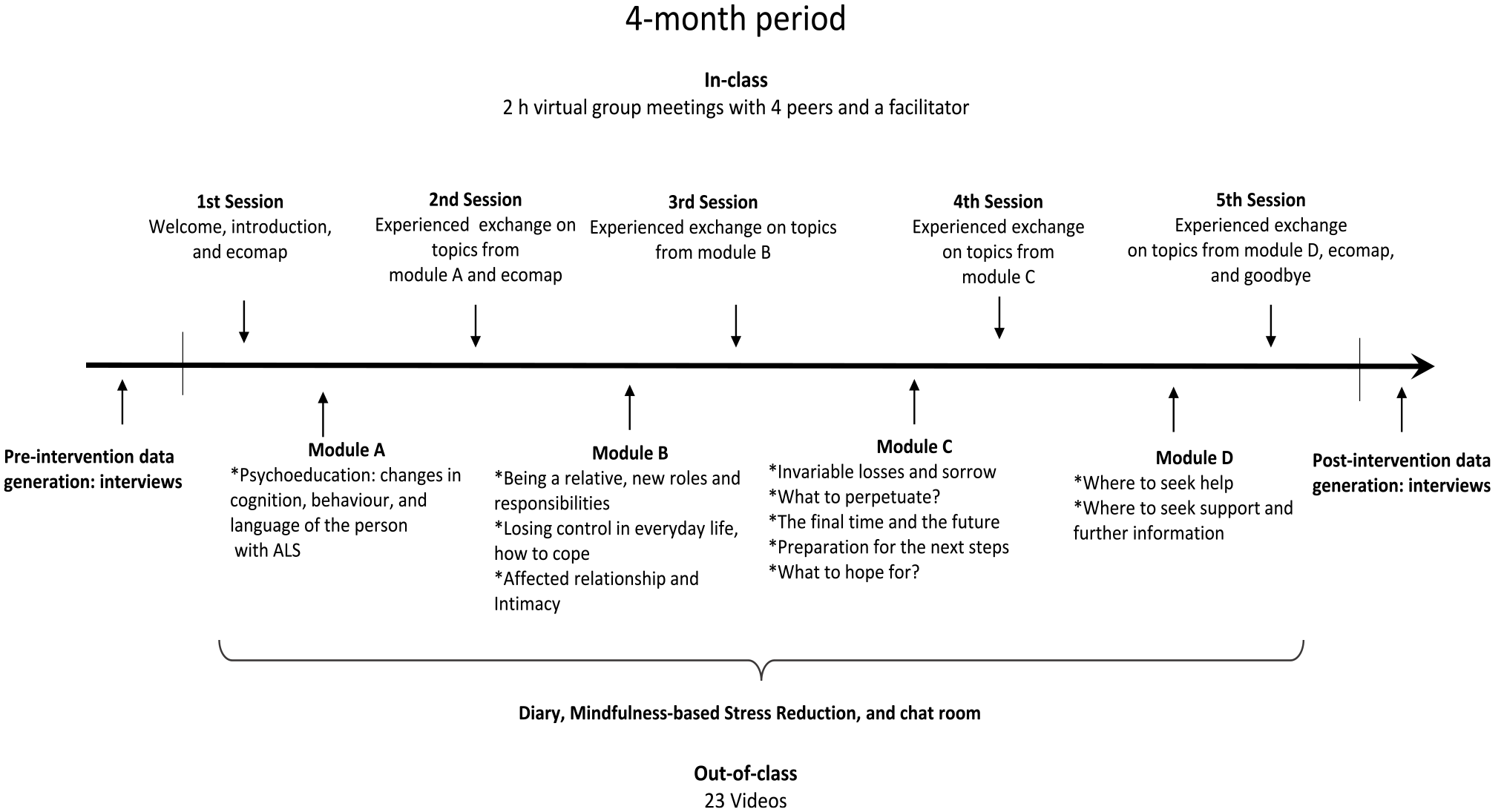
The EMBRACE intervention was conducted in 2020 and designed as a blended online learning format consisting of in- and out-of-class-activities (Figure 1, inspired by Olesen et al17,18). The in-class-activities were 5 virtual group facilitated meetings every fourth week and 3 exercises using an ecomap, which is a visual booklet of personal and family relationships. 19 Out-of-class-activities were 17 targeted videos, a chat room, a diary and 7 customized videos on mindfulness-based stress reduction. The targeted videos were based on topics identified in research evidence and findings in a previous study on the challenges and needs among caregivers of deceased PALS/CIs. 20 In-class-activities were executed on Microsoft Teams and out-of-class-activities were provided on the online hosting platform Simplero. The participants received a blank notebook to use as their private diary and were free to write whatever they felt was meaningful. Virtual group meetings were facilitated by the fourth author who had extensive knowledge of the target group from working as a healthcare professional at RCFM.
Participants
Thirteen participants were included (Table 1). The inclusion criteria were: (a) partners or spouses (hereafter caregivers) of individuals diagnosed with ALS, referred to RCFM and who had received an initial visit from a professional at RCFM; (b) caregivers who understood and spoke Danish; and (c) caregivers of people with ALS with a cut-off score ⩾22 on the Amyotrophic Lateral Sclerosis-Frontotemporal Dementia-Questionnaire (ALS-FTD-Q), a validated caregiver-reported questionnaire containing 25 items, with a total score ranging from 0 to 100, higher scores indicating more behavioural impairments. 21

Scores are separated into participants dropping out and the intervention group. Post-intervention scores were collected right after finishing the 4-month intervention. The Zarit Burden Interview (ZBI) ranges from 0-88 points with higher scores indicating greater burden. 23 Scores ⩾24 indicate clinical high burden. 24 The Hospital, Anxiety and Depression Scale (HADS) cut-off score ⩾8 indicate possible cases of anxiety and/or depression. 22
Total number of included participants. One participant lost her spouse with ALS and cognitive and/or behavioural impairments between the pre-intervention data generation and start of the EMBRACE intervention.
Abbreviation for person with amyotrophic lateral sclerosis and cognitive and/or behavioural impairments.
One participant did not return the questionnaires.
One participant did not return the questionnaire.
Participants were encouraged to invite a person from their network or family to participate alongside them in the virtual group meetings to support them throughout the illness trajectory of their relative. The co-participants were not considered participants and therefore not interviewed.
Recruitment
Recruitment took place at RCFM. Healthcare professionals from RCFM sampled the participants by identifying 208 people diagnosed with ALS, referred to RCFM up to September 8th, 2020 who met inclusion criteria a and b (Figure 2). An information letter about the EMBRACE intervention was then sent to each of the 208 caregivers of the people with ALS identified by the healthcare professionals. Cognitive and behavioural impairments were described in the invitation as changes in personality, behaviour and/or language. The intention was to get the caregivers, who perceived their partner or spouse as cognitively and/or behaviourally impaired, to contact the first or fourth author for screening using the ALS-FTD-Q (inclusion criteria c). In total, 31 interested caregivers contacted the first or fourth author by phone who guided them through the questionnaire, asking 1 question at a time with score possibilities and with additional information if needed to score their affected relative. 21 Participants who were not eligible for EMBRACE were offered extra support from relevant healthcare professionals at RCFM.

Flow chart of the recruitment and enrolment process.
Data Generation
Data was generated using individual semi-structured interviews with the participants enrolled pre- and post-intervention and with non-completers post-intervention. Interviews with non-completers were analysed to explore the participants’ potential barriers for participation. Interviews were conducted in Danish by the first author and quotes were later translated by 2 interpreters, 1 Danish speaker and 1 English speaker, who were not on the research team. Semi-structured interview guides with open-ended questions were used (Appendix 1). The questions focussed on the participants’ experiences in relation to EMBRACE with specific attention to the intervention components, for example, the diary, mindfulness, group meetings, peer support etc. The participants were introduced to the intervention components during the pre-intervention interviews to explore their expectations towards the components (Appendix 1). Seventeen of 23 (74%) interviews were completed online using Microsoft Teams. One interview was conducted via telephone and 3 as in-person interviews at the RCFM and 2 at the caregiver’s workplace according to their preferences. Interviews were digitally recorded and lasted between 27 minutes and 1 hour and 41 minutes. Background characteristics of the participants’ experience of burden, anxiety and depression were obtained using the Zarit Burden Interview (ZBI) and the Hospital, Anxiety and Depression Scale (HADS) pre- and post-intervention22,25,26,27 (Table 1).
Data Analysis
Methodology and theoretical framework
A qualitative inductive analytical methodology was used to gain insight into the participants’ experiences of EMBRACE. 28 We thus analysed empirical data that went beyond the self-evident content analysis. 28 Our interpretation involved inductive reasoning and pattern recognition to reveal the underlying complexity of practice as a means to improve palliative rehabilitation services in the future. 28 This was a fully theory informed inductive study design. 29
The theoretical framework of Sense of Coherence (SOC) was used inductively to explore the participant’s way of coping with life stressors such as the disease and the consequences of it in relation to their participation in EMBRACE. 30 SOC consists of the 3 concepts comprehensibility, manageability and meaningfulness that should be present to cope with and experience life as coherent and thereby reduce the experience of stress. 30 SOC helped derive knowledge that could be essential when designing health-promoting interventions for caregivers of PALS/CIs and to increase the intervention’s capability to strengthen caregivers’ sense of coherence. 30 SOC indirectly permeated the entire study from the development of EMBRACE to the design, data collection, analysis and writing of the findings.30,31
The analysis was guided by 4 steps according to the ID methodology and by the SOC concepts.28,30,32 First, interviews were transcribed and uploaded to NVivoTM12. Second, transcripts were read intensively for the pre- and post-intervention interviews respectively and coded for insights related to the participants experiences. Third, patterns and relationships within and between the data groupings were explored and finally across the whole data set. The whole research team critically discussed the relationships and patterns within data, and relevant tentative thematic insights leading to the primary categorization of themes were negotiated and defined. An iterative process of going back and forth between raw data and tentative themes lead to the overarching themes which were then indirectly associated with the SOC concepts. 30 Fourth, a visual depiction of main findings and the relationship among these was developed to represent a coherent interpretive thematic and conceptual description which is presented in the results section. 28
Ethics
The study was registered on clinicaltrials.gov [ID no. NCT04638608] and adheres to the COREQ check-list, 33 the ICMJE 34 and the Declaration of Helsinki. 35 Ethical approval for this study was deemed unnecessary according to national legislations by the Danish Data Protection Agency [File no. 2019-521-0144] and the Central Denmark Region Committees on Health Research Ethics [File no. 1-10-72-1-19]. Informed written and oral consent were obtained from all participants and data were anonymized and participants referred to by IDs.
Findings
Our findings represent the participants’ pre-intervention expectations to and post-intervention experiences of the EMBRACE intervention (Figure 3). An interrelated hierarchically informed structure consisting of 3 themes influenced on the participants’ experiences of EMBRACE. The themes entailed both individual and interpersonal factors. The first theme, ‘Striving to Obtain Control in Everyday Life’ characterized the participants’ primary and individual impetus to participate in the intervention which was to gain new knowledge and be able to transform this into ways of understanding and dealing with everyday life as a caregiver of a PALS/CIs. The second theme, ‘Peer support Across the Illness Trajectory’ deals with interpersonal relations and is centred around the unique connection between people who share the same destiny and who understand, relate to and support each other through knowledge-sharing about everyday life as a caregiver. Lastly, the third theme, ‘The Complexity of Relations’ comprises the meaning of interpersonal relations with family members and friends and is centred around the participants’ considerations of pros and cons of involving their surrounding network in everyday life through participation in EMBRACE. The themes affected one another as the participants’ striving to obtain control in everyday life entailed gaining knowledge and skills, sharing experiences with peers as well as becoming aware of strengths and limitations in their personal and professional network.

A visual depiction of experiences of the EMBRACE intervention perceived by spousal caregivers of people with ALS and cognitive and/or behavioural impairments.
Striving to Obtain Control in Everyday Life
Pre-intervention: Anticipating everyday life coping skills
This theme demonstrated how individual factors such as readiness for change, expectations, self-confidence and self-efficacy influenced the pursuit of building coping skills. The participants talked about their anticipation of the intervention’s focus and looked forward to the time allocated to talk about their needs instead of those of the PALS/CIs. They expressed a motivation and wish to gain knowledge about ALS and its cognitive and behavioural impairments as well as insights on how to manage disease challenges.
‘To get as much knowledge as possible will help me later, yes, make things easier. Well, I become more autonomous and not so dependent on other people. . .and that’s what I think the intervention could help me with’. (ID 1H)
It appeared that knowledge gained from EMBRACE was regarded as helpful in preparing them for future challenges and thereby enhancing their possibilities of regaining control of and autonomy in everyday life. The participants anticipated that EMBRACE could help them find meaning in life but also how to deal with different dilemmas. For instance, they talked about the dilemma of being indirectly burdened by the severity of ALS, meanwhile grappling with the realization that they were not the one who was going to die. They said that they envisioned and hoped that the intervention would help them relax, process grief and relieve a heavy conscience.
‘My expectations are perhaps that I’ll learn to understand myself better and just be with it, instead to trying to push it away. . .I am not sick, so perhaps. . . learn how to live with it, myself and my sorrow’. (ID 1E)
The participants seemed to have realized the severity of the disease and how it was necessary for them to balance their everyday life and feelings, during the disease, in order to get through it. The participants wished that the intervention could help them clarify whether they were on the right track in terms of how they managed everyday challenges.
‘It’s not up until now that I have realized how I have missed being informed, for a long time, about all these topics and being able to talk about them and have someone to share my views on them with’. (ID 1F)
It seemed as if the participants became aware of their knowledge gap when presented with topics in the videos and this realization evoked eagerness and motivation to participate in the intervention with the wish of gaining new perspectives. They hoped and envisaged that targeted information from the videos would lead to discussions with peers about topics, that they had not previously talked about and that this would help them understand their own situation better.
Post-intervention: A space to unload
After the intervention the participants shared thoughts about the individual outcome of their participation. They expressed how EMBRACE, with its focus on their needs and challenges, had provided them with a space to unload. They explained how topics from the videos were later brought up for discussion in the group meetings. This meant that they were given an opportunity to reflect on topics they had not considered or were suppressing because they were seen as challenging.
‘You get to touch upon various topics. Otherwise, you’ll just be sitting and talking about ‘this is my life, my life is like this, and what do you think about that?’. . .But when XXX [name of the group facilitator] is there and asks questions then you get to talk about topics that you haven’t brought up yourselves. . .Perhaps you start to think of some other things instead’. (ID 2C)
It appeared that the participants found the structure of the intervention, with the initial presentation of different topics in the videos followed by group discussions, meaningful and that this structure enriched their insights and empowered them to address sensitive issues with support from a healthcare professional. They also described how perspectives from group discussions on what to do or say helped them build resilience and which made them better at putting their foot down and setting boundaries.
‘I was reaffirmed that it was okay, well that you try to get your life working. I said at one of the meetings, that it feels like I’ve been withdrawing a bit from XXX and that I had a heavy conscience about that, right? And then I was told that it was important, right? I was told that it was okay to do that without having a heavy conscience. Well, it was a little like being set free’. (ID 2G)
Having a space to unload and feeling the empathy and support from peers and the group facilitator reassured the participants that their prioritization on everyday tasks were legitimate and not something that they should feel bad about. Generally, they experienced and highlighted peer support and the videos as being helpful in terms of feeling recognized, being able to breathe easier and feeling relief. One participant described the group meetings like this:
‘Well, I think there’s room to whine [at the group meetings]. That’s all there’s to it, if you could say it like that. . .Because I have said it before, you have a need to talk about yourself but also about the sick relative. And to hear yourself talk and the other members talk means that you are part of the process all the time’. (ID 2B)
It seemed like thoughts and concerns were demystified through a process of sharing experiences from everyday life in the group meetings and how this was a way of processing the harsh reality of everyday life. They described how the group discussions made them feel more capable of comprehending and managing the disease progression and its challenges. Information from the videos gave them new insights into general behavioural and psychological patterns of caregiver reactions. The participants expressed how this knowledge was useful to solve their ‘puzzle’.
‘Like the many arms of an octopus, all the thoughts that are present, but how do they find their way to where they belong? ‘These thoughts belong on THAT arm’. . . Well, it’s been nice like that. I don’t know how to describe it. Well, a relief. It’s nice because the thoughts are there anyway’. (ID 2E)
The participants strived to obtain control by structuring all the information that was provided to them during EMBRACE. They described how the information had helped them develop new strategies and given them the courage to talk to the PALS/CIs about difficult things at home and with the peers during group meetings. Being able to reflect and discuss topics with peers or perhaps write about them in the diary was regarded as a way of processing sorrow, stress and doubt. Stress made it difficult for them to remember things, and they reported how notes in the diary or on a computer or piece of paper had helped them structure and memorize information and thereby regain some control again. Others described how they were too tired to write things down, while other expressed that keeping a diary was not something they would do.
Peer support Across the Illness Trajectory
Pre-intervention: Expectations regarding meeting peers
In the pre-intervention interviews, interpersonal factors, like social support, influenced the participants’ expectations for meeting peers. They expressed how they believed that meeting peers would be the most important and meaningful component in EMBRACE. They said that they expected that their peers would more readily understand their experiences, frustrations and sorrow because they would be in similar situations.
‘I’m looking forward to it [meeting people in the same situation], I really am. Because I hope...we don’t have to sit and gaze at our navels, it’s just that you get to talk to someone who knows. Well, you don’t have to explain things, they know exactly what you mean, if you say ‘Yes, how are things going with X and X or how do you experience X and X, and what do you do?’ (ID 1O)
It appeared that the participants envisaged that they would have a common point of departure, namely being partners of a PALS/CIs and that this situation would entail a knowledge taken for granted. Sharing experiences with someone who understands did not seem to be the usual case for the participants. For instance, those who were new to caring for a PALS/CIs talked about being anxious about meeting caregivers with experiences of caregiving during the later stages of the disease because they anticipated that these caregivers would present them with information and challenges about what might occur. The participants with years of experience with ALS expressed an urgent, altruistic need to prepare caregivers new to ALS for what will come.
‘We are our own little knowledge bank, right? And why not share with others what you have figured out or what you know is a practical way to handle problems here and now’. (ID 1O)
It became apparent that the participants had knowledge and experience and that these insights were regarded as potential supportive ‘guidelines’ for others. A mutual sharing of experiences on dos and don’ts between the participants on how to deal with ALS/CIs was desirable. For instance, they believed and expressed that it was important and necessary to engage with peers with the aim of sharing experiences because they considered every peer to be in ‘the same boat’, as 1 participant said.
Post-intervention: The shared destinies
After the intervention, interpersonal factors were identified in relation to the participants’ experiences of shared destinies among peers. The participants described how meeting peers was the most important and meaningful element of EMBRACE because they experienced a special sense of community, honesty and support. They explained how heterogeneity in the groups was important.
‘Well, we are four totally different people, and at totally different places in our lives, more or less. Hmm, but I think the first time it was kind of hard to meet XXX [another participant] and hear her story. But then again, what I am left with now, then I think, well I wouldn’t have benefitted from it in the same way if she hadn’t been there. I wouldn’t!’ (ID 2H)
The disease was described as the steppingstone to the establishment of meaningful relations at the group meetings, and it was their experience with the disease that connected them in different ways, despite different background and their partners being at different disease stages. The shared destinies made it legitimate for them to ask sensitive questions during the group meetings, which they described as a safe place for feelings and forbidden thoughts.
‘No, but having someone to talk to sometimes who knows how it is and how it can be and how much effort the disease takes and how you’re just about to give up occasionally and think ‘I can’t bother anymore, can it just end’. That’s how it can be sometimes. And of course, people don’t understand that, if they are not in the middle of it, so you don’t say it out loud, but you can say it out loud to someone who is in the same situation because that’s how we all feel occasionally’. (ID 2C)
It seemed like the participants felt a need to speak candidly, and that this was something special that was possible in the group. They experienced and expressed how the mutual understanding made it easy to listen, relate and share personal experiences. For instance, expressing the frustrations involved in caring for a PALS/CIs or concerns about the long disease-trajectory. Contrary to that, they expressed that the chat room was not a place where they would share feelings and concerns because this would require a closer connection between the group members. One participant even described written communication in the chat room as a bit ‘dangerous’. Others said that they preferred to discuss issues at the regular face-to-face virtual meetings and that they perceived themselves as being too old for chatrooms.
The Complexity of Relations
Pre-intervention: Contemplations on including relations
Interpersonal factors, like social support, were also outlined by the participants in relation to including family members or friends in the intervention. The participants talked about the balance of trying to navigate the relations with family members and friends, who were in the surroundings of the participants’ everyday life. They described how they imagined that bringing a family member or a friend into the group meetings could provide support.
‘First, I thought it was a bit weird. But then after I had thought it through and talked to my friend about it, then it seemed like a good idea because you can continue to discuss the things afterwards without having to repeat everything. And it’s very nice that other people know about your problems so you can lean on them for support in everyday life’. (ID 1K)
It appeared that including a co-participant in the group meetings entailed both pros and cons. Regarding the disadvantages, they envisioned that involving a family member or friend in everyday life through participation in EMBRACE could potentially scare or worry them, and therefore their involvement prompted careful consideration.
‘Honestly, I must say I don’t think that anyone from our network could bear participating in the intervention. I don’t think they can, well they can’t’. (ID 1H)
The participants were very considerate of their network, wanting to shield them from the painful reality of living with a PALS/CIs. Furthermore, they didn’t want family members and friends to hear or be burdened about their concerns and frustrations.
‘I’ve decided that it was – that this was a road I wouldn’t want them to go down because it would be too difficult: I mean I’m not sure that I would want them inside my ‘headquarters’ in this’. (ID 1I)
For most participants, they hesitated to involve a family member or friend in the group meeting. They did not want to risk burdening their network even more and described how they did not expect that having a family member or friend present at the meetings would be an actual support for them during the disease trajectory. They seemed to want to protect the wellbeing of their family and friends and expressed concerns about having to engage in a balancing act of being open to talk about concerns and frustrations vs. protecting the network from the harsh details.
Post-intervention: The meaning of relations
After the intervention, the participants had gained new insights into the role played by people in their network (interpersonal factors) and their impact on the participants’ experiences of EMBRACE. They spoke of how relations with family members and friends contained a spectrum of both positive and negative feelings such as disappointment, sorrow, anger and love. They explained how the exercises with ecomaps in the intervention had been a positive eye-opener, but also confronted them with intense, complicated and strained relations. One participant said:
‘Because there’s always a dream scenario when someone’s missing. Then I think of my sisters. Well, for instance some of those who used to be close to me, well, they are not there. . .yes because then I realized that you are quite alone. It sorts of gets onto the paper. ’Wow’, right?’ (ID 2F)
The ecomap exercises seemed to induce different feelings among the participants, as the visual depiction displayed the reality and quality or the lack hereof, of their relations with family members and friends. They explained how they had come to realize, during the disease trajectory, how people reacted differently; some were staying and supporting them while others had vanished from their lives. Some participants were positively surprised when they wrote the names of people, they had not considered to be part of their network on the ecomap, but who they, during the exercise, had found relevant to include.
‘Luckily, I was also surprised by how many colleagues of mine were on the ecomap. Then I began ‘Well, hallo they are also there’. Not because they call all the time, but they are here when I need them. And the same goes for friends and so on. But there are also people of whom I think ‘Come on get going’, right?’ (ID 2K)
The ecomap exercises helped visualize and, for some participants, also expand the network of people they could reach out to in times of needing help or feeling lonely. On the other hand, they also talked about family members and friends who were reluctant to deal with the PALS/CIs because they found it difficult to communicate or be around the sorrow associated with PALS/CIs. One participant expressed her reluctance to talk about her situation with her network:
‘I have a good network and talk a lot with them, but the difference is that I don’t want to talk too much because then they say ‘Phew, I feel sorry for you, and can you cope with it, and are you going to sell the house’ and things like that. And I don’t feel the need to talk about that, and I don’t feel the need to share those very awful details’. (ID 2I)
It became apparent to some participants that there were people in their social networks who were not ready to be presented with disease information and whose pity and confronting questions they had no desire for. This was very contrary to what they experienced in the peer support group, where information, questions and sympathy were welcomed.
Discussion
This study explored the experiences of caregivers of PALS/CIs’ participation in the EMBRACE intervention and identified 3 themes: striving to obtain control in everyday life, meeting peers across the illness trajectory and the complexity of relations.
Our findings demonstrate that EMBRACE enabled the participants to reflect upon their own needs and challenges which had not been prioritized as focus typically was on the PALS/CIs’ needs. More specifically, the findings showed how the participants strived to gain knowledge and skills as a caregiver of a fatally ill PALS/CIs to become more autonomous in an everyday life characterized by uncertainty. A study on caregivers facing end-of-life-realities across 3 different disease trajectories; expected death (ie, ALS), unexpected death (ie, organ failure) and mixed (ie, lung cancer) showed that caregivers struggle with losing control over everyday life because of uncertainty related to the future and the disease. 36 In line with our findings, a scoping review on palliative care needs among caregivers of people with ALS found that the caregivers had needs related to disease information, course and skills. 37 In addition, our findings showed that the participants also had specific individual needs, such as how to set boundaries, prioritize time for themselves and continue having a life even though they were caring for a dying person. The findings suggest that the participants moved from limited experiences of comprehensibility, manageability and meaningfulness, before the intervention, to enhanced experiences of comprehensibility, manageability and meaningfulness after the intervention. This improvement of their sense of coherence 30 could be explained by the control spectrum presented by Strauss et al, 36 going from not having control (having less control, feeling out of control, losing control) at one end to having control (having/finding control, experiencing relief) at the other end. Through meaningful and relevant information provided in EMBRACE, the findings demonstrated how the participants were empowered to navigate and cope with everyday life in the present and future course of the disease. Gonella et al 38 found in a structured psychoeducational programme that caregivers of people with advanced dementia enhanced their understandings of their partner’s prognosis, the inevitable death and belief in their inner strengths and potentials, which is in line with our findings. Our study extends these findings indicating that EMBRACE helped the participants to unload during meetings and generally enhancing their resilience and positive thoughts. Overall, our findings suggest that EMBRACE provided the participants with beneficial knowledge and support that helped them clarify the uncertainties related to disease prognosis, inner strengths and insights on how to deal with different reactions and dilemmas, thereby enhancing their control and sense of coherence in everyday life.30,39
Findings on peer support illustrated that the participants valued being able to share and discuss issues without having to explain or argue. Meeting peers reduced their feeling of loneliness and created a feeling of community. Peer support is highlighted as important for building meaningful connections and empowerment in caregivers of people who survived a stroke. 40 Another finding was that the participants felt acknowledged and safe to share frustration, sorrow and ‘forbidden’ thoughts. Being part of a group allowed caregivers of people with ALS to feel that their negative emotions were common and legitimate among their peers who delt with similar difficult situations. 8 Being able to be authentic and being recognized by others in a similar situation are valuable aspects of peer support.11,18,41,42 Along with other positive findings on peer support in the EMBRACE intervention,18,43 our findings suggest that heterogeneity in the groups could be a way of targeting peer support as we found that the participants with years of experience with ALS/CIs were helpful in providing useful, meaningful and important knowledge to those new to ALS/CIs. Having characteristics in common such as caring for a person with stroke and being able to share difficult experiences is found to override demographic similarities, like gender and age. 44 Findings also indicated that those with years of experience with ALS/CIs wanted to support those new to ALS/CIs, which is in line with a study on patient ambassadors within acute leukaemia. 45 In that study, Nørskov et al 45 found that the patient ambassadors were motivated by the hope that their experiences might help others and have positive impacts on certain aspects of their everyday lives. Being of value to others have been found to boost people with depressions’ belief in their personal strength and foster an external focus, promoting interactional empowerment. 46 Furthermore, shared experiences are found to create a special connection and mutual recognition, leading to a sense of hope and a feeling of being able to cope,45,47 which is in line with our findings. However, we also found that seeking help from others was challenging for the participants with less experience of living with a PALS/CIs because of the potential of having to face difficulties related to the information about future stages of the disease. A study on caregivers of people with ALS also found there were both pros and cons of peer support, as some found it beneficial in terms of sharing experiences while others found it distressing. 41 The downside of meeting peers was the possible confrontation with future challenges, 41 which echoes our findings. That is, participants new to ALS/CIs expressed concerns pre-intervention (risks of facing information about future stages of the disease) which were replaced post-intervention by tremendous and meaningful inputs gained from the more experienced peers. Overall, our findings advance our understanding and add to the literature by showing potential nuances of peer support and the importance of group composition and offers novel ways to facilitate and target peer support that enhances caregivers of PALS/CIs’ ability comprehend and manage everyday life as a caregiver.30,39 The principle behind informal peer-support is to make people connect through shared experiences. 48 Professionally facilitated peer-support is found to reduce the perceived pressure, helplessness and depression of caregivers of people with dementia and to improve their self-efficacy compared to before an intervention. 49 By combining the benefits of professionally facilitated peer-support and informal peer-to-peer support, we were able to create ‘a safe place’, where the participants felt comfortable sharing thoughts and concerns while still being gently and respectfully guided through various topics and dilemmas that they may encounter along the disease trajectory. EMBRACE differed from informal peer-support in that it used targeted educational topics and evidence-based components to enhance a sense of coherence among the participants. On the other hand, it allowed for a more informal exchange of experience than formal peer support by providing a flexible meeting agenda that encouraged the participants to state their needs and thoughts, making every meeting participant centred. From the participants’ perspectives, the group facilitator broadened the discussions by introducing and addressing topics that they would never themselves have considered. Findings therefore underline the importance of combining formal and informal peer-support to target support initiatives on complex and sensitive issues.
In regard to complex relations, the participants experienced that their relations were strained because some family members and friends were afraid of PALS/CIs and had withdrawn from the relationship, which was also found in a newly published study on caregivers of people with ALS. 50 This study of Poppe et al 50 showed that social support from family members and friends was very important for the caregivers and they valued if neighbours helped them out. Goldstein et al 51 found that the best predictors of caregivers’ distress were early reduction in social activities and dissatisfaction with social relationships. This is not surprising, since a study shows that social environment has a dramatic impact on life satisfaction and well-being, especially in times of distress, crisis or disaster. 52 Human resilience depends on the strength and richness of social connections and affiliations with groups, 52 which emphasizes the importance of EMBRACE in supporting caregivers of PALS/CIs, so that they can maintain and nurture relations to support them through the disease of their relative.
Limitations
EMBRACE was designed as a multi-component intervention, but findings revealed that not all components were relevant to the participants, for example, only some participants were keen on using mindfulness or the diary, and no one used the chatroom. This may indicate that the intervention was too ambitious in its design, providing the participants with too many components.53,54 Changes in the design should therefore be taken into account in the future; keeping the intervention more simple by reducing the numbers of components to strengthen the intervention. 53 Due to a high caregiver burden, we decided that the components should be optional. However, this decision may have influenced our possibility of fully grasping if and how all components might impact on the participants or not, as findings primarily centred around the group meetings and videos, components that the participants prioritized in their busy everyday life.
As to representative credibility, the findings from the 23 interviews reflect 13 participants’ firsthand perspectives, and these helped to understand the experiences of EMBRACE. The majority (69%) of the participants were females, and findings may therefore primarily represent female perspectives.
In the invitation letter, we encouraged interested caregivers to contact the research team if they perceived their relative with ALS to be cognitively and/or behaviourally impaired. We knew that this group of caregivers were often highly burdened, lacking time and energy to engage in other activities than caregiving.9,10 By giving this group of caregivers the responsibility of reaching out to us to be included in the study, we might have failed to include caregivers with profound needs as they may not have had the capacity and resources to engage and findings may, thus, only represent experiences from socioeconomical advantaged spousal caregivers. Furthermore, the caregivers’ answers in the ALS-FTD-Q screening (inclusion criteria c) might also have been influenced by and reflected the caregivers’ own burden and not only the level of behavioural impairments of their relative with ALS.
In this study we invited spousal caregivers on the assumption that couples have special relationships and roles, and most often live together, which means that they are connected and depend on each other in a different way than non-spousal caregivers. 55 Furthermore, spousal caregivers of PALS/CIs have in common that the disease is present in their lives around the clock whereas non-spousal caregivers can get respite. Nevertheless, research shows that ALS and dementia impacts the whole family and network,56,57 and so, non-spousal caregivers might benefit from participating in EMBRACE. In fact, a study on cancer caregiving and consequences showed that more distant caregivers were affected to the same degree as primary (partner/spousal) caregivers, which emphasizes the need for initiatives targeting other than spousal caregivers. 58 Including non-spousal caregivers in EMBRACE calls for careful consideration of how to target other groups of caregivers without compromising the opportunity for spousal caregivers to speak candidly with those who share similar lived experience.18,43,59 Our participants emphasized the uniqueness of ‘being in the same boat’ during meetings which enabled them to unload and share what they called forbidden thoughts which they could not do in the presence of friends and family members.
We were unable to systematically explore whether the experiences of EMBRACE differentiated among those with no or little experience of ALS/CIs and those with years of experience with ALS/CIs. Such investigation may have provided further insights into the timing of the intervention and relevance of information, especially for those with years of experience with ALS/CIs. 11
Prior to the pre-intervention interviews, none of the participants knew the first author who conducted the interviews. However, in the post-intervention interviews she had met with all the participants during the pre-intervention interviews and briefly during the first and fifth group meeting, welcoming and thanking them for their participation, which might have influenced the participants’ statements, for example, by being more positive. In addition, this made the interviewer an ‘insider’ with an increased risk of having blind spots, for example, missing aspects or interpretations in relation to what an ‘outsider’ would find. 26 The credibility and trustworthiness of the findings were enhanced through pre-defined analytical steps based on the ID methodology with clear descriptions elaborated within each of them. For example, two of the researchers performed the initial analysis respectively and later compared, discussed and verified codes with the whole research team with the interpretations continuously being linked to raw data, which added to the trustworthiness of the findings. Furthermore, to enhance transparency of the analysis process, a table of the analytical steps showing how codes were developed and extracted was provided to the readers to verify findings and conclusion of this study. The research team consisted of a combination of researchers who conducted the intervention and researchers who had not been part of the intervention, which provided different angles and critical methodological discussions and considerations, potentially preventing blind spots and biases of a single researcher or insider on the study findings. 28 Findings from this study may be transferable to other caregivers of fatally ill relatives who struggle with lack of control and various support needs in their everyday lives.
Conclusion
Our study shows that EMBRACE was beneficial to caregivers of PALS/CIs struggling with everyday needs and challenges related to being a caregiver of a PALS/CIs. Through relevant information and peer support, the participants felt prepared for the illness trajectory of their relative. EMBRACE was found to support and strengthen the participants in gaining more control in everyday life. Generally, the videos and discussions with peers were highlighted as the most beneficial and important components of EMBRACE because they helped the participants to navigate, comprehend and manage the inherent and potential future challenges and offered them a sense of coherence by enhancing their ability to deal with the PALS/CIs and their caregiver life. Peer support promoted resilient functioning and reduced their feelings of loneliness. Ecomaps helped them understand their complex relations with family members and friends. Overall, these findings contributed to an understanding of the experiences of EMBRACE and how some of the intervention components, in different ways, facilitated the participants to obtain control and manage everyday life as caregivers of a PALS/CIs. This study shows that it can be difficult to develop and target a generic palliative rehabilitation intervention to a heterogeneous group of caregivers, as some intervention components and information may be more important and relevant to some rather than others, depending on their situation, needs and stage of disease. Palliative rehabilitation initiatives should offer an opportunity to engage and share experiences with peers across the illness trajectory. Finally, supportive components in the intervention, such as mindfulness, diary and ecomaps, should be optional since the caregivers are already burdened.
Implications for Research
In future research it is necessary to explore if participants can translate competences and skills learned in online interventions into meaningful, supportive initiatives in their everyday lives. Additionally, it would be relevant to explore how their work attachment is influenced from having a fatally ill partner. Lastly, it would be interesting to explore how the socioeconomic status of the caregivers’ is related to caregiver coping and resilience, and if certain coping strategies are related to the gender of the caregivers.
Implications for Palliative Rehabilitation
Future palliative rehabilitation programmes targeted at caregivers of PALS/CIs should include information on how to maintain/obtain control in everyday life and on ways to manage everyday challenges to reduce stress and find meaning in the caregiver role.
Interventions should be developed to support partners and spouses at different stages of the disease to provide them with the opportunity to share experiences with peers through professionally facilitated group meetings.
Interventions should help caregivers of PALS/CIs to maintain and nurture relations to support them through the disease of their relative and post-mortem.
Healthcare professionals should be aware of how some participants may be more talkative and having wider boundaries when it comes sharing information about challenges that everyone might not be ready to hear about yet.
Intervention components should be easily accessible, for example, on an online platform or a physical notebook while being introduced as optional, leaving the caregivers with a choice between using or rejecting any of them to make sure they do not constitute an additional burden.
Supplemental Material
sj-pptx-1-rpo-10.1177_27536351241227860 – Supplemental material for Experiences of an Online Palliative Rehabilitation Programme for Spousal Caregivers of People With Amyotrophic Lateral Sclerosis and Cognitive and/or Behavioural Impairments: A Qualitative Interpretive Study
Supplemental material, sj-pptx-1-rpo-10.1177_27536351241227860 for Experiences of an Online Palliative Rehabilitation Programme for Spousal Caregivers of People With Amyotrophic Lateral Sclerosis and Cognitive and/or Behavioural Impairments: A Qualitative Interpretive Study by Lene Klem Olesen, Karen la Cour, Laura Nimmon, Heidi With and Charlotte Handberg in Advances in Rehabilitation Science and Practice
Footnotes
Appendices
Interview guide post-intervention for caregivers of people with amyotrophic lateral sclerosis and cognitive and/or behavioural impairments.

| Key questions | Elaborative questions |
|---|---|
|
|
What did you gain from participating? Was there anything you experienced that was beneficial to you? If yes, what? What prompted you to participate? Do you feel that something was lacking in the intervention? |
|
|
How was EMBRACE beneficial to you in your everyday life? How did you use the things your learned in EMBRACE in coping with everyday challenges? Which challenges did you experience when trying to incorporate the learned skills into your everyday life? In general, what did you think of EMBRACE? |
Which components were the most meaningful for you? |
Please elaborate why? |
|
|
How many videos did you watch? What was your impression of the content of the videos? How did you use the videos during the intervention? How did you use the videos as preparation before the meetings? How did the topics fit your needs? What did you think of the number of videos? What did you think of the lengths of the videos? What did you think of the way the videos were distributed to you after each meeting as preparation for the next meeting? |
|
|
What you think of the group meetings? How did you use the other participants? What influence did the group composition have on your openness? What was beneficial about the meetings? What did you think about the content of the meetings? What did you learn? What was challenging about the meetings? How did the virtual meetings work out? What did you think about the size of the group? What would you have liked to see being done differently in the meetings? What did you think about the facilitator? How did the length of the meetings fit you? How did the time of day fit you? How did the frequency fit you? How did the number of meetings fit you? |
|
|
What did you think of the online format? What did it mean to you that EMBRACE was online? Which challenges did you experience with the online format? How did you experience the coherence between the videos and the meetings? How did you prioritize your time between watching the videos and participating in the meetings? |
|
|
What prompted you to use/not use the diary? How did your dairy reflections support you during the intervention? How will you use the diary in the future? Would you like to share the content of your diary with family and friends? |
|
|
What made you use/not use the exercises? What impact did the exercises have on you? In which situations did you use mindfulness? |
|
|
What prompted you to draw/not draw the ecomaps? How did the ecomaps effect you? What were the benefits of making ecomaps? What was challenging about making ecomaps? What did you think about making 3 ecomaps? |
|
|
Why did you use/not use the chatroom? What was beneficial about the chatroom? What was challenging about the chatroom? |
|
|
What did you like most? What did you not like? What was most beneficial to you? What was most challenging for you? All things considered, how has it been for you to participate? |
Acknowledgements
We thank all the family caregivers who offered their time and were so willing to share their experiences on everyday challenges and their evaluation of the EMBRACE intervention. Finally, thanks to student assistant Mathilde Grøn Laursen for transcription of interviews and to RN, PhD Astrid Lindman for supervision with the analysis of questionnaires characteristics.
Author Contributions
All authors have made a substantial contribution to all the following: (a) conceptions and design of the study, or acquisition of data, or analysis and interpretation of data; (b) drafting the article or critical revision for important intellectual content and (c) final approval of the submitted article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The patient organization the Danish Foundation for Neuromuscular Diseases, the Institute of Public Health, University of Aarhus, Denmark and the National Rehabilitation Center for Neuromuscular Diseases, Denmark.
Consent to Publication
Not applicable.
Clinical Trial Registration Number
Trial register: Danish Rehabilitation Centre for Neuromuscular Diseases Protocol Record DanishRebCND Lene Klem Olesen [ID no. NCT04638608]. A Complex Intervention Study on a Palliative Rehabilitation Blended Learning Programme to Support Relatives and Health Care Providers of People with ALS and Cognitive Impairments in Coping with Challenges – Full Text View – ClinicalTrials.gov. Registration was done after the interviews had been conducted because the need to register was not known beforehand by the research team.
Data Availability Statement
The datasets generated and analysed during the current study are not publicly available because they contain information that could compromise research participant privacy/consent, but they are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.