
Abstract
Background:
In patients with amyotrophic lateral sclerosis, the atrophy of hand muscles often causes impairment of thumb/finger motion and disabilities in their activities of daily living. Hand orthoses are effective for such impairment and disabilities; however, there are some difficulties in their application.
Case description and methods:
In this case report, we present the timely application of hand orthoses and introduce our clinical algorithm for the application of hand orthoses to patients with amyotrophic lateral sclerosis.
Findings and outcomes:
Our clinical algorithm was applied to 11 patients. The numbers of applications and the durations of the use of orthoses were as follows: 4, web spacer; 4, short thumb spica; 8, long thumb spica; and 2, cock-up splint; and 2.75, 2.0, 0.63, and 2.0 months, respectively.
Conclusions:
The clinical algorithm for the application of hand orthoses is helpful in choosing the optimal orthoses and contributes to maximizing patients’ function, independence, and quality of life.
Clinical relevance
Hand orthoses are useful for improving the activities of daily living of patients with amyotrophic lateral sclerosis. The clinical algorithm might be helpful for many physicians in choosing the optimal orthoses in a timely manner.
Background
In patients with amyotrophic lateral sclerosis (ALS), the atrophy of hand muscles often causes impairment of thumb/finger motion and disabilities in their activities of daily living (ADL). In particular, thumb opposition is very important for ADL, and it is very important to maintain this ability by every means possible.
Hand orthoses are generally effective for these disabilities; however, there are some difficulties in their application. First, it is quite difficult to predict the functional prognosis of ALS because of the wide variation and rapid progression of symptoms. If it takes a long time from “planning” to “application,” they become worthless, or even when the patient can use them, the duration of their use becomes very short because when the disorder has progressed, their use cannot improve ADL. Therefore, if their use is considered, they should be prepared as soon as possible. Second, in considering the use of orthoses, it is important to be flexible, such that they may be changed in a timely manner and in accordance with the stage and condition of the disease. However, it is difficult for many physicians to choose the optimal orthoses. We herein report the case of a male patient, in whom significant improvements in his ADL were observed by the timely application of orthoses, and we propose a clinical algorithm for the application of hand orthoses for ALS.
This study was approved by Okuma Central Hospital Ethical Committee, and written informed consents about the purpose of this study and publishing the data with their anonymousness were obtained from all participants.
Case description and methods
A 68-year-old man was admitted to our hospital 6 months after being diagnosed as having ALS with the complaint of difficulty in performing precision hand motions. An examination of the upper extremities showed weakness of the wrist extensors (manual muscle test (MMT), 4), intrinsic hand muscles (MMT, 3), and thenar muscles (MMT, 2). Spasticity was mild (Modified Ashworth Scale, 1). His stage of ALS identified by Sinaki and Mulder 1 was stage 2 and 32/48 in the ALS Functional Rating Scale–Revised (ALSFRS-R). 2 During motions requiring opposition, especially in writing and fastening buttons, he used his thumb in the extension position (palmar adduction) because of hand deformation due to the atrophy of the hand muscles.
By wearing a customized simple web spacer (SWS), 3 his grip strength and tip-to-tip form pinch strength of his dominant right hand were improved from 7.0 kg (left, 10 kg) and 0.15 kg (left, 6 kg) to 8.0 and 0.35 kg, respectively. Moreover, he was able to easily write and fasten buttons (Figure 1(a) and (b)).
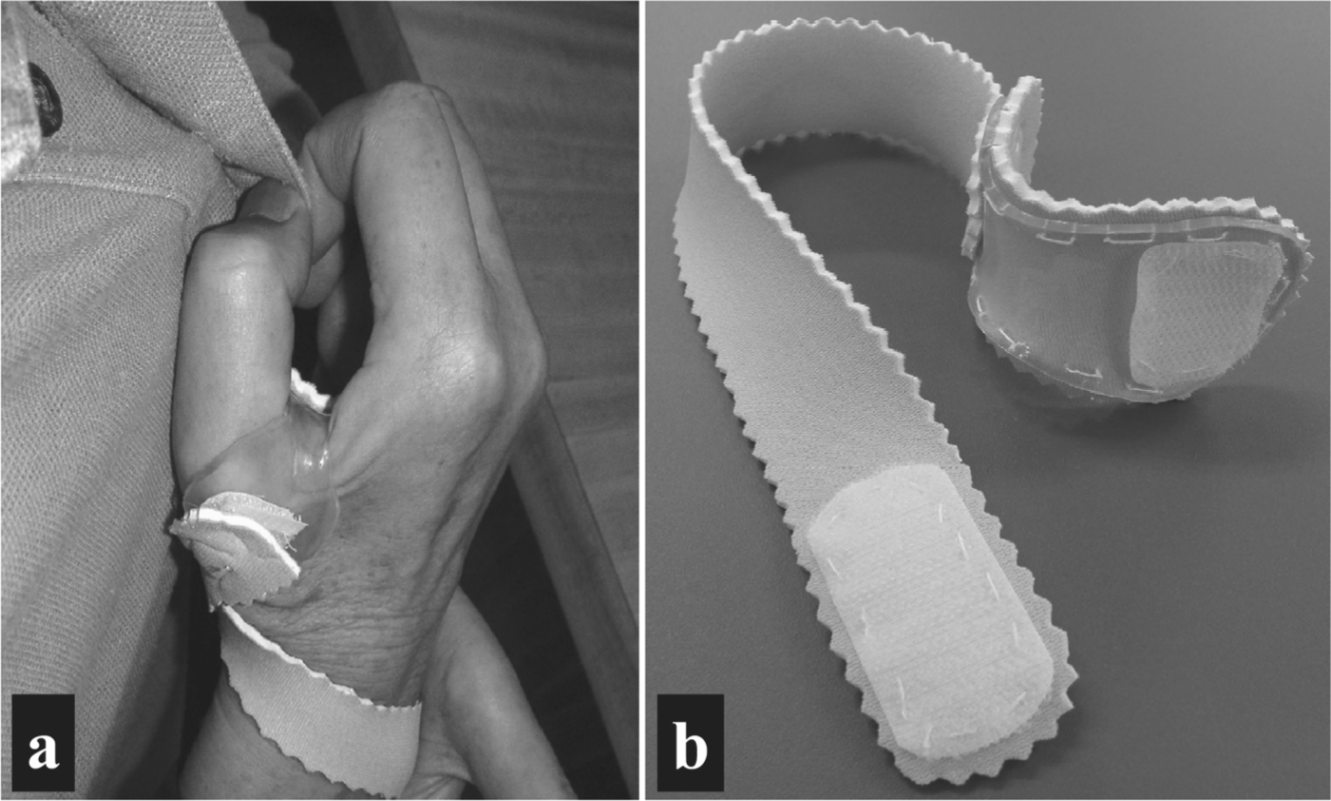
A simple web spacer.
However, when he consulted with our clinic 2 months later, the findings of clinical examination showed deterioration of the atrophy of the intrinsic muscles (MMT, 1–2), and he was unable to flex his metacarpophalangeal (MP) joints of the fingers; as a result, he could not do thumb opposition, even when using SWS. Therefore, a short thumb spica (STS) attached to the MP joint was applied in place of the web spacer, and he was able to easily write and pick up small things again (Figure 2(a) to (c)). However, after 3 months, he had to change his orthosis again to a long thumb spica (LTS) attached to the MP joint (Figure 2(d)) because of the further weakening of the wrist extensors (MMT, 2) as his muscle atrophy progressed.
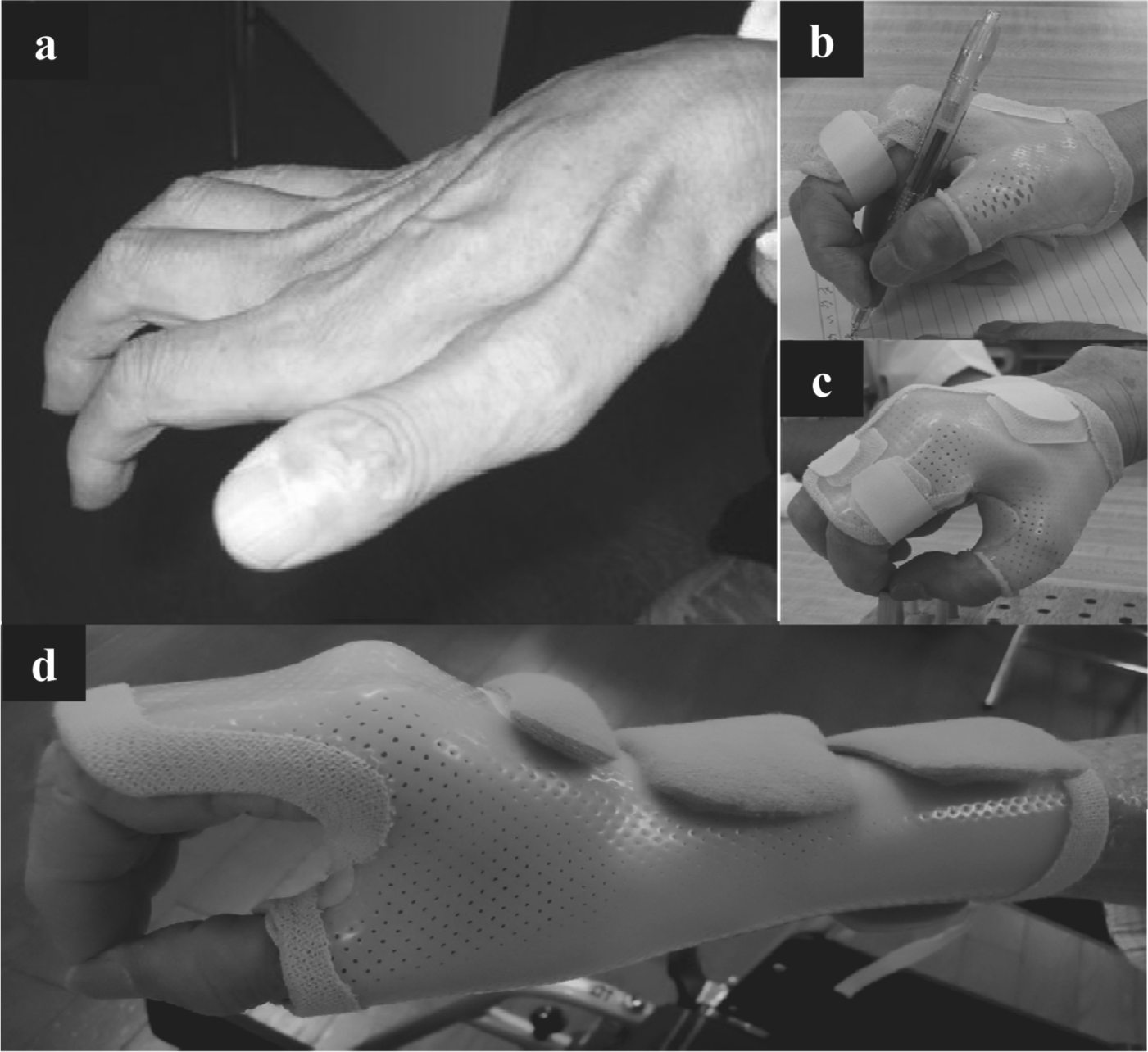
Application of a short/ long thumb spica.
Findings and outcomes
A clinical algorithm for the application of hand orthoses for ALS is proposed in Figure 3. In our small observational study, our algorithm was applied to 11 patients (7 males and 4 females; average age = 64.5 ± 6.83 years; ALSFRS = 27.7 ± 4.34/48). The numbers of applications and the durations of the use of orthoses were as follows: 4, SWS; 4, STS; 8, LTS; and 2, conventional cock-up splint (CS) and 2.75 ± 0.5, 2.0 ± 0.82, 0.63 ± 0.23, and 2.0 ± 0.5 months, respectively.
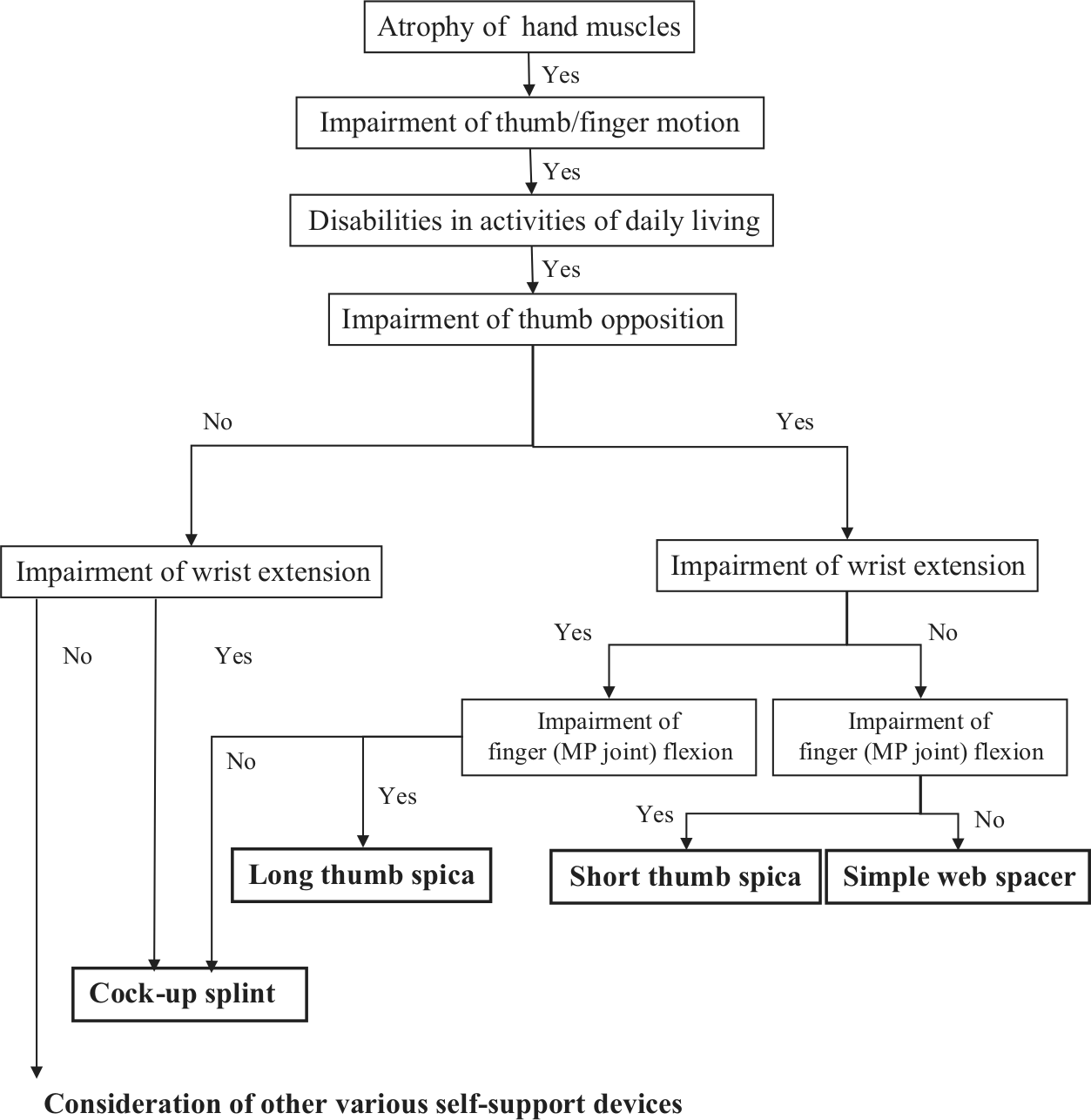
Clinical algorithm for application of hand orthoses in patients with amyotrophic lateral sclerosis.
Especially, SWS significantly improved “tip-to-tip form pinch strength” from 0.19 ± 0.08 kg to 0.39 ± 0.17 kg (p < 0.1). Functional independent measurement (FIM) score was also improved from 105.8 ± 1.5 to 119.3 ± 1.26.
However, when a symptom of the upper arm worsened, SWS, STS, and LTS use was limited to training sessions and did not contribute to the improvement of ADL, even when the balanced forearm orthosis (BFO) was used in combination. In these conditions, self-support devices (SSDs) such as a universal cuff in combination with CS were applied. In 91% of our cases, the final orthoses for practical activities using their arms were BFO, CS, and SSD used in combination (average duration of their use = 2.30 ± 1.1 months).
Discussion
Impairments of hand function in ALS vary according to the remaining muscle strength. “Picking,” which requires thumb opposition, is the most important function in ADL. However, an assessment of the wrist function, particularly that of the extensors, is necessary, not only because wrist stability is required for performing hand function but also because a wrist extension position that leads to the tenodesis effect reinforces the remaining finger flexion power. When the wrist joint is unstable but finger function remains, CS is indicated. In contrast, when finger dysfunction accompanied by wrist instability exists, LTS should be considered.
Next, the indication for orthoses for thumb opposition should be considered. In our institute, we choose two orthoses, SWS and STS. SWS can be easily and rapidly prepared. Its principal advantage is that it can be promptly used by patients with progressive diseases such as ALS. Its secondary advantage is the use of flexible and soft materials. Because the sensory function of ALS patients often remains intact, hard or rough materials are not recommended. However, as muscle atrophy progresses, it will no longer be useful because (1) the correction of the opponens pollicis muscle gradually becomes insufficient and (2) when the strength of the finger flexor muscles weakens, tip-to-tip form pinching is impossible to do. In these situations, because a support for MP joint flexion is necessary, STS is a good candidate.
Furthermore, when muscle weakness of the upper arm worsens, the practicality of hand orthoses decreases, and the stratagem using SSDs such as a universal cuff in combination with BFO is necessary to improve ADL. However, orthoses for stabilizing the wrist including the CS are necessary even in this situation.
Conclusions
The aim of the treatment of ALS patients is to maximize their function, independence, and quality of life (QOL) for as long as possible. 4 In the clinical management of ALS patients, the assessment and prescription of assistive devices by a medical provider to improve their function and maintain independence are recommended.5–8 Hand orthoses are very useful for improving ADL as well. We believe that the application of hand orthoses as a therapeutic option for not only ALS but also other neuromuscular disorders should be promoted, and an algorithm that can help many physicians in choosing the optimal orthoses is required. We hope that our proposed clinical algorithm will become a preliminary milestone in this field in the future.
Finally, we emphasize that the most important thing is a careful observation to catch the chance for improving patient’s QOL. However, it is not always easy for the patients because it is difficult for them to go to hospital many times for evaluation. The algorithm might be also useful for their family and caregivers to solve these problems.
Footnotes
Declaration of conflict of interest
The authors declare no conflicts of interest. The authors alone are responsible for the content and writing of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.