
Abstract
Background
Physicians often use their intuition during the diagnostic process. Intuition can also be used by professional medical intuitives trained to obtain information about the potential underlying causes of health concerns.
Objective
To evaluate physician and patient perceptions of the usefulness, accuracy of, and satisfaction with medical intuition sessions and their influence on the clinical process, comparing them to virtual usual care medical visits.
Methods
This prospective within-participant design study was conducted between April and August 2024. Forty patients received an online usual care medical visit followed by a medical intuition session attended by their physician. Quantitative and qualitative surveys assessed physician and patient perspectives of the visits.
Results
Physicians’ average usefulness rating for medical intuition sessions was high overall (80.8 out of 100) and greater than usual care (P = .001). Physicians’ accuracy ratings of the medical intuition assessments appeared very high (83.3 out of 100), and 79.5% reported that the information on the connection between a patient’s life events and their health was useful. All 6 physicians reported they would recommend using medical intuitives to colleagues and that they would likely continue to use them (60.2 out of 100). They rated the medical intuition sessions as influential to their clinical process (3.6 out of 4).
Conclusions
Medical intuition integration into healthcare has promising potential, especially in validating patients’ symptoms and enhancing comprehension of the emotional and spiritual contributions of disease. Future research should use more robust research designs, including randomized control, larger sample sizes, and a long-term follow-up.
Introduction
Physicians often consciously or subconsciously use their intuition during the diagnostic process, in addition to their knowledge and experience.1,2 While still unorthodox, a growing number of literature documents that physicians rely on intuition or ‘gut hunches’ in clinical decision-making.3-6 A comprehensive review of medical intuition literature is beyond the scope of this paper, but prior work spanning decades provides a relevant context, and representative sources are cited here. Intuition also can be brought into the clinical setting by professional medical intuitives. In a 2005 report funded by the U.S. National Institutes of Health, the Institute of Medicine Committee on the Use of Complementary and Alternative Medicine by the American Public defined medical intuitive as “the utilization of a focused, intuitive instinct to ... ‘Read’ energetic and frequency information in and around the human body.” 7 “Medical intuition” refers to the skill of intuitively observing, evaluating, and assessing information obtained from both the physical body, including its anatomy and physiology, as well as the biofield or energetic systems. This approach involves conducting in-depth, intuitive scans to identify underlying factors or root causes contributing to physical, emotional, mental, and spiritual imbalances, to promote holistic well-being.7,8 Although medical intuition uses the word ‘‘medical,’’ the use of medical intuition is not to be construed as the practice of medicine, psychotherapy, or any other licensed health care practice, and is not a substitute or replacement for the services of licensed healthcare providers.
Few studies have evaluated the usefulness and accuracy of medical intuition and physician and patient satisfaction with the inclusion of medical intuitives in the clinical setting. One study found that the information provided by medical intuitives did not correspond highly with that found in the medical records of 5 patients. 9 However, several studies have found medical intuitives to be accurate. In a double-blind study, 7 medical intuitives accurately distinguished between nineteen patients with congestive heart failure and their healthy spouses. 10 Other studies found medical intuitives accurately identified disc pathology and pain patterns in sixteen patients with low back pain 11 ; identified physical issues and connected those issues with life events, resulting in patient satisfaction 8 ; and detected health issues that patients noted in self-reports. 12 While these preliminary studies advanced the research in this area, they have several limitations, including using medical intuitives who may have lacked training and small sample sizes. 13
This study attempted to address that gap by examining 6 physicians’ and forty patients’ perceptions of the usefulness and accuracy of and satisfaction with medical intuition sessions. Physicians’ perceptions of influence on the clinical process were also evaluated. Five medical intuitives were used to foster the generalizability of the results. Study results can be used to support the inclusion of medical intuitives in clinical visits.
Methods
This prospective, pragmatic study used mixed methods to compare 2 types of virtual visits: (1) usual care visits involving only the physician and patient, and (2) medical intuition sessions involving the physician, patient, and a medical intuitive. Quantitative self-reports were collected from primary care physicians and patients via online surveys. The study was conducted from April to August 2024. Participants were recruited between March 29 and August 5, 2024. All study activities were approved by the IONS Institutional Review Board [IORG#0003743] and pre-registered at the Open Science Forum (https://osf.io/m98aj).
Physicians were recruited from November 14 to December 7, 2023. An ad titled “Seeking Clinicians! Want to be Part of a Medical Intuition Study?” with study information was distributed through the Institute of Noetic Sciences networks (ie, newsletter and social media), shared with the Executive Director of the Academy of Integrative Health & Medicine and LW’s integrative medical doctor networks. The ad contained a link to a SurveyMonkey survey where they entered practice information, willingness to follow study protocol, and experience and beliefs around medical intuition. HW reviewed the survey applications and interviewed medical doctors for the position, attempting to engage heterogeneous practitioners (ie, from different geographical areas and diverse beliefs/experiences with medical intuition). WC and LW were not involved in physician recruitment and were blinded to physician identities throughout the study. Physician collaborators were 6 medical doctors (MD), 5 females and 1 male, with an average age of 55.8 years (SD 5.9 years).
Regarding racial identification, 4 were European, 1 was Asian, and 1 was Latinx. On average, they had 22.5 years of education (SD 2.7 years) and a socioeconomic status score of 77.3 (SD 12.9) on a scale from 0 to 100. Geographically, they were distributed across the United States (Southeast, n = 1; West, n = 1; Midwest, n = 2; Southwest, n = 2) and all operated office-based practices. They had an average of 21.7 years (SD 7.2 years) in practice. Physicians’ levels of belief in medical intuition varied widely, with an average of 73.0 (SD 21.1) on a scale of 0 to 100. Four physicians had never received a medical intuition session, while 2 had. None of the MDs had previously used a medical intuitive in their clinical practice.
Regarding participant distribution, 2 physicians saw 11 participants each, another 2 saw 7 participants each, and the remaining 2 saw 2 participants each. The 2 doctors with the fewest sessions had baseline belief-in-medical-intuition scores of 50 and 68 (0-100 scale, described above). Also, 1 physician with 2 visits was a specialist in women’s health, and the remainder were general practitioners.
Experienced medical intuitives, from a wide range of healthcare backgrounds and individual intuitive study pursuits were invited to apply via targeted outreach, including email and social media postings to practitioner networks. Each had completed 200-hours of study, mentorship, and/or certification in medical intuition, and each maintained a professional medical intuitive practice. Eleven applicants were screened through meetings with WC to review the study procedures, their comfort with study procedures, and their availability to participate during the study period. Five medical intuitives were referred to the IONS study staff. The IONS study staff then coordinated with them for session scheduling. These 5 medical intuitives constituted the practitioner group who participated in the study; no additional screening occurred beyond the procedures already described. They were not involved in any other study activities. The medical intuitives included 3 licensed nurse practitioners, 1 certified health coach, and 1 licensed aesthetician.
Participants
Of the 58 patients recruited by the 6 physicians, only 18 declined to participate or did not respond. The sample size of 40 was constrained by funding availability. Patients were screened using the following criteria: required to be English-speaking adults aged 35 to 65 with an internet connection, comfortable using the virtual platform, not pregnant (pregnancy considered a vulnerable research population), and have symptoms with an unknown etiology (ie, the physician has been unable to determine the cause of the symptoms) or a diagnosed medical condition that has been resistant to treatment. “Resistant to treatment” refers to a condition, illness, or disease that does not respond optimally or effectively to standard or commonly used medical or therapeutic interventions (ie, the condition persists or worsens despite undergoing appropriate treatment measures). The referring physicians determined and documented treatment resistance for each patient and had access to their medical records. To protect confidentiality across virtual clinical sites, the study did not collect or retain participants’ specific diagnoses, symptom histories, or other protected health information in the research dataset. Forty patients were referred, and study staff contacted them via telephone to answer any questions, consented them verbally, and provided them with an electronic consent form to sign. Patient participants were compensated for their time in the study at a usual and customary rate.
Patient Involvement
Patients’ priorities, experiences, and preferences played an important role in shaping the research questions and outcome measures for this study. The research team made a concerted effort to incorporate patient-centered assessments and ensure minimal participant burden. This consideration was reflected in the development of outcome measures that were accessible and meaningful from the patients’ perspective. Patients were not involved in study design development, recruitment, or conducting the study. Once the study has been published, participants will receive a layperson summary via email, alongside a digital link to access the full paper.
Study Procedures
Overall
Figure 1 summarizes the following study procedures. The physicians and their patients each completed five-minute baseline surveys followed by their “usual care” half-hour virtual medical appointment. Patients then completed a five-minute survey immediately after the usual care visit while still on the Zoom meeting, assessing their perspectives of the visit. Within 2 weeks following the usual care visit, physicians and patients were joined by a medical intuitive for a virtual 45-minute session, followed by a 15-minute session with only the physician and medical intuitive present to allow the physician to ask the medical intuitive additional questions. Subsequently, physicians and patients each completed a closed-ended 6- to 7-minute survey immediately after the medical intuition session, while still on the Zoom meeting. After their final medical intuition session, physicians completed a second, closed-ended five-minute survey regarding their perspectives on the medical intuition sessions overall. Just prior to the study’s conclusion in August 2024, physicians completed a final but optional survey with open-ended questions. Study Design.
Usual Care Visit
Patients completed baseline surveys, taking approximately 5 minutes to answer questions on their 1) demographic characteristics, 2) history with medical intuitives, 3) how credible they felt the usual care visit and medical intuition sessions would be, and 4) their expectations of effectiveness for the 2 sessions. As part of routine care during the usual care visit, the physician inquired about the patient’s symptoms, life history, and potential causes of their health issues according to their usual care process (no scripted questions), and the patient could ask clarifying questions. Patients then completed a post-usual care visit survey asking about the usefulness and accuracy of, and their satisfaction with, the medical intuition session. Physicians also completed a baseline survey reporting how credible they felt the medical intuition sessions would be and their expectations of effectiveness for the sessions before the study began.
Medical Intuition Session
One to 2 weeks following the usual care visit, an online session was conducted with the physician, patient, and medical intuitive. The patient’s camera was turned off, allowing the medical intuitive to be blinded to the patient’s identity and not use visual cues. The medical intuitives had no access to the patients’ medical information or life history information prior to or during the session. The session began with the medical intuitive providing a brief overview of what would occur and instructions to the patient and physician. This included a disclaimer that the session was an intuitive assessment of the physical body and biofield and not intended to replace licensed medical care, diagnosis, prescription, therapy, counseling, or treatment of any kind. The physician and patient were told they could stop the session to ask clarifying questions. Additionally, they were told that the medical intuitive may perceive energy and information that they might be unaware of or might not be present in the patient’s experience. The medical intuitive performed a non-invasive intuitive assessment of the physical body, biofield, and information about the patient’s health issues and described what they assessed. They also intuitively assessed the patient’s life history, including possible limiting beliefs and life experiences related to their health. After 45 minutes, the patient left the online session, and the physician privately asked the medical intuitive questions about the patient for 15 minutes to glean anything else of medical importance. Then, the patient and physician completed a post-medical intuition session survey evaluating the session.
From Final Patient to Study Conclusion
After their final medical intuition session, physicians completed a final closed-ended survey on the medical intuition sessions overall and, in mid-August 2024, completed additional open-ended questions in an optional survey.
Quantitative Survey Measures
Measure Descriptions

Notes. Recipient legend. MD = Physician, Pt = Patient. Timeline legend. 1. Prior to study onset. 2. Baseline Survey – Measures completed immediately before the Usual Care (UC) visit during Zoom Visit #1. 3. Post-UC Session – Surveys completed immediately after the Usual Care visit during Zoom Visit #1. 4. Post-MedInt Session – Surveys completed immediately after the Medical Intuition session during Zoom Visit #2. 5. End of Study – Final physician evaluation completed after all study sessions were complete.
Baseline Measures
Credibility and expectancy bias (Physicians and Patients)
Before each session, physicians and patients completed the CEQ, which yields credibility and expectancy scores (0-10) indicating perceived rationale and expected symptom improvement.
Sociodemographic Characteristics (Patients)
Patients reported sex, age, race/ethnicity, years of education, and socioeconomic status, and prior experience with medical intuition. Socioeconomic status was assessed on a 0-100 scale reflecting perceived access to material, social, and health resources.
Outcome Measures
Usefulness
Physicians
After each Usual Care (UC) and MedInt session, physicians rated how useful the information was to their clinical process on a 0-100 scale (0 = not useful; 50 = moderately useful; 100 = very useful/indispensable).
After MedInt sessions, they also rated the usefulness of the intuitive’s information about connections between life events and health using the same scale. Physicians further indicated whether the intuitive’s input validated aspects of diagnosis or treatment, suggested alternative diagnoses or treatments, or prompted additional testing; these 4 yes/no items were summed (0-4).
At study completion, physicians completed a short final survey assessing overall usefulness of MedInt sessions, likelihood of continued use of a medical intuitive (0-100), and willingness to recommend medical intuition to colleagues (four-point Likert scale).
Patients
After UC and MedInt session, patients rated the usefulness of the recommendations provided during both UC and MedInt sessions using a five-point Likert scale ranging from strongly disagree to strongly agree.
Qualitative Data Collection and Analysis
The patients’ post-usual care visit and medical intuition session surveys had an open-ended question, “Is there anything else you would like to share?” Physicians were asked this as well in their post-medical intuition session surveys. Additionally, prior to the study’s conclusion, physicians were encouraged to complete an optional 10-item open-ended survey, which all physicians completed. Four directly related to clinical care and perceptions of the medical intuition session are included here, and the remainder related to study design and process are available in Supplemental Data: (1) In what ways, if any, has the participation of a medical intuitive influenced your diagnostic or treatment approach for the patient(s) involved in the study? (2) In what ways, if any, did you find the information about the connection between the patient’s possible life events and health useful? (3) Based on your experience, do you see a future role for medical intuitives in the healthcare system, and in what capacity? (4) During the additional 15-minute session without the patient, were you able to address all your questions with the medical intuitive? How did this one-on-one time contribute to your understanding of the patient’s condition? Would you have liked more time with the medical intuitive without the patient present?
Analyses
Quantitative Analyses
HW conducted all analyses (ie, WC and LW did not interact with the data or conduct any analyses). Descriptive statistics were calculated to describe the patient sample. Categorical variables were described qualitatively. Kruskal-Wallis equality-of-populations rank test of significance was used to compare both physicians’ and patients’ credibility and expectancy of the 2 interventions. A repeated analysis of variance (ANOVA) was used to evaluate differences in physician usefulness of usual care and medical intuition sessions, and patients’ satisfaction. Because individual usefulness ratings were nested within 6 physicians, we conducted sensitivity analyses adjusting for clustering at the physician level using linear regression models with cluster-robust standard errors (clustered by physician). This adjustment addresses the non-independence of repeated ratings within physicians.
Qualitative Analysis
Textual answers from physicians’ and patients’ open-ended survey questions were first quantitatively described. To support analytic rigor, both authors (HW and ST) independently reviewed and coded responses, using an inductive approach to identify themes. Coding discrepancies were resolved through discussion, and a refined theme structure was developed (Please see Supplemental Data for method details). Given the exploratory scope, formal intercoder reliability was not calculated. Brief theme descriptions are included in the Results section. More detailed descriptions are available in the Supplemental Data, and datasets are available upon reasonable request of HW.
Results
Patient Characteristics

SD = standard deviation. Note. Patient's could choose more than one ethnicity and so percentages do not add up to 100%.
Credibility and Expectancy Before Study
Physician credibility ratings reflected a statistically similar degree of belief in both the usual care visit and medical intuition session to change patient symptoms (6.5, SD 2.7, 65% of total score for usual care; 5.6, SD 2.6, 56% of total score for medical intuition; X 2 = .52, P = .47). Patient credibility ratings were greater for the usual care visits than for the medical intuition sessions meaning that patients felt the former would be more effective at improving their symptoms than the latter (6.6, SD 1.5, 66% of total score for usual care; 5.6, SD 2.0, 56% of total score for medical intuition; X 2 = 6.4, P = .01). Although the magnitude of the credibility difference between usual care and medical intuition was similar for physicians and patients, the physician comparison did not reach significance due to the small sample size (n = 6), which limits statistical power. The larger patient sample (n = 40) allowed for detection of a statistically significant difference.
Expectancy for both interventions was similar for physicians and patients, meaning that they both expected the usual care visit and medical intuition session would improve patient symptoms similarly (Physician ratings: 3.9, SD 2.3, 39% of total score for usual care; 5.3, SD 2.0, 53% of total score for medical intuition; X 2 = .92, P = .33; Patient ratings: 5.0, SD 2.0, 50% of total score for usual care; 4.8, SD 2.4, 48% of total score for medical intuition; X 2 = .54, P = .46).
Usefulness of Medical Intuition Sessions
Physician and patient perspectives of the medical intuition sessions are displayed in Table 3 Physicians’ average ratings indicated they found the medical intuition sessions highly useful. They also rated the information on the connection between a patient’s life events and their health as highly useful. Physicians reported willingness to continue using medical intuitives, and all physicians indicated that they would definitely or probably recommend the use of a medical intuitive to a colleague. Ratings of the medical intuitive’s influence on their clinical process were similarly high and comparable to ratings for the usual care visit. Sensitivity analyses using cluster-robust standard errors showed the same direction of effects as the primary models, although standard errors increased, as expected with only 6 clusters. These adjusted analyses did not change the overall interpretation that physicians rated the medical intuition sessions as highly useful.
Physician and Patient Perspectives of the Medical Intuition Sessions, (n = 40 Patients, n = 6 Physicians)

SD = standard deviation.
Notes. Usefulness ratings on 0-100 scales were interpreted using the following qualitative bands: very low (0-20), low (21-40), moderate (41-60), high (61-80), and very high (81-100).
aAlso, greater compared to 71.9 SD 15.2 for usual care, F(1,79) = 11.02, P = .001.
bInfluence on clinical process was rated on a 0-4 scale for both usual care and medical intuition sessions. Scores for the 2 conditions did not differ significantly (medical intuition:M = 3.6, SD = 0.71; usual care: M = 3.6, SD = 0.87, Z = −.30, P = .76), indicating that physicians perceived both types of sessions as having a similar level of influence on their clinical process.
Patient and Physician Perspectives of the Accuracy of and Satisfaction With the Medical Intuition Sessions
Patient and Physician Perspectives of Accuracy of and the Satisfaction With the Medical Intuition Sessions

SD = standard deviation.
As shown in Figure 2, when asked about specific medical intuitive accuracy, the majority of patients agreed or strongly agreed that the medical intuitive: located the specific area of their body related to their main physical health issue or concern (72.5%), described events from their life that were probable or possible (67.5%), helped them make a connection between probable or possible life events and how they may be potentially impacting their current issues or concerns (70%), helped them to identify potential underlying causes of their current issues or concerns (60.0%), and gave them useful recommendations (80.0%). Patient perspectives on medical intuition accuracy and usefulness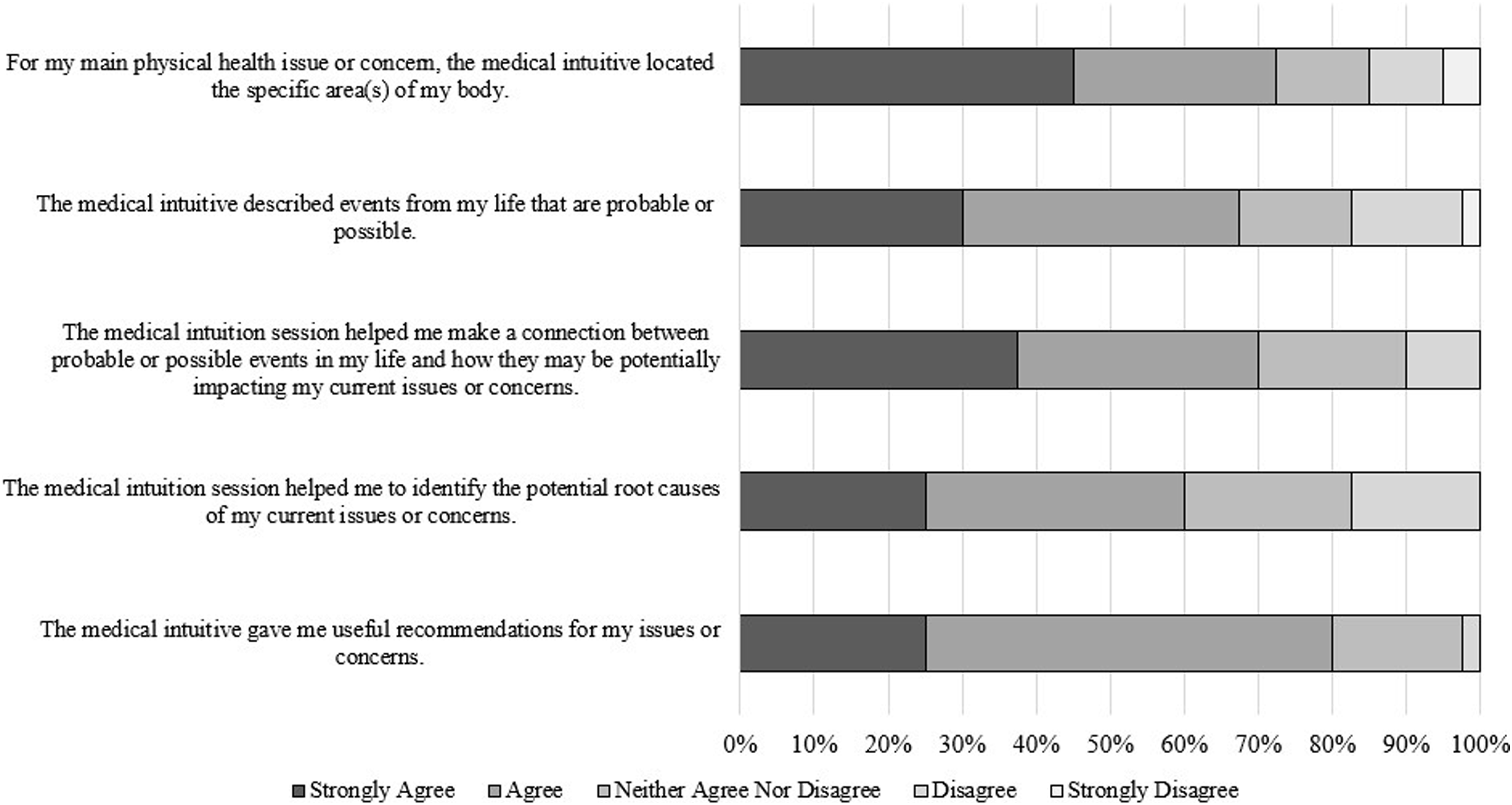
Qualitative Analyses
Physician Responses to Select Open-Ended Questions Survey at Study Conclusion
The text for each question was analyzed separately
Influence of Diagnostic or Treatment Approach
Several physicians noted that the participation of medical intuitives had a multifaceted influence on their diagnostic and treatment approaches. This included redirecting diagnoses and treatment, validating existing plans, reducing unnecessary testing, identifying potential emotional and life event factors, prompting follow-up testing, and encouraging the exploration of new options. Specific insights from medical intuitives led to more targeted evaluations. One physician shared, “When specific, it has been helpful to have ideas on particular areas of focus and labs/imaging to consider. This gave me diagnostic consideration and helped support working diagnoses.” The sessions often confirmed existing diagnostic and treatment plans, boosting physician confidence. One physician noted, “A lot of the information they provided was validating for our current plans.” Another stated, “This type of information helps limit unnecessary and expensive testing.” Additionally, the identification of potential emotional and life event issues was often beneficial. One physician mentioned, “In about half the people, the medical intuitive participation opened up either a previously unknown but relevant historical event that may have contributed to the patient’s condition.” The information sometimes led to follow-up testing and exploration of new options, with 1 physician stating, “About half the time, it generated follow-up testing that I may not have otherwise gone to next.” These influences enhanced the overall care and management strategies for the patients involved.
Usefulness of Information about Connection between the Patient’s Possible Life Events and Health
Physicians found this information validated their intuition and current practices, allowing them to re-evaluate diagnosis and treatment, address emotional and life event factors, and potentially bring about transformative change. Some appreciated how the information validated their existing intuition regarding emotional and life event impacts on health. The connection between life events and health was seen as a potential pathway to transformative change as long as the patient recognized and acted upon the insights. One physician emphasized, “This kind of information is particularly helpful if it’s accurate, and even more so if a person can recognize that a decision made in their past can be changed or updated later in life.”
Usefulness of One-on-One Session with Medical Intuitive
Physicians found the one-on-one sessions with medical intuitives valuable for clarifying statements, confirming intuitions, discussing specific treatments, and gaining crucial insights. They also noted the need for more structured follow-ups. One physician stated, “This was helpful in clarifying things that I needed help with.” Others valued the opportunity to confirm their own intuitions and align their clinical insights with the input from the medical intuitive. The sessions also enabled discussions about specific treatments using clinical terminology that might be complex or unfamiliar to patients, proving beneficial. Occasionally, these sessions provided crucial and impactful insights essential to understanding the patient’s condition. As 1 physician shared, “The information I received was absolutely crucial to understanding the patient.” 1 physician felt the usefulness varied depending on the medical intuitive. One physician suggested that the sessions could be more effective with structured follow-ups to better integrate the insights.
Future Role of Medical Intuitives in the Healthcare System
Physicians recognized the potential benefits of integrating medical intuitives into the healthcare system. These benefits included reducing unnecessary diagnostics, validating patient symptoms, and understanding underlying emotional and spiritual factors. While some physicians were optimistic about this integration, others acknowledged it may be a significant challenge to achieve widespread acceptance. One physician stated, “There is no question that medical intuition would be of great benefit to healthcare... Decreasing laboratory and other diagnostic evaluation by targeting underlying causes of health issues based on medical intuitive insights.” Some physicians saw a role for medical intuitives as ancillary to licensed healthcare physicians, emphasizing that proper integration with traditional medicine could yield positive outcomes. One noted, “If it does yield improvements in patient outcomes, I will embrace a role for medical intuitives in the healthcare system for selected people who either ask for them or we as physicians ask for them.” Another mentioned the importance of patient involvement in the process suggesting that greater patient engagement could effectively leverage medical intuitive insights.
Physician Free-Text Answers After Medical Intuition Sessions
Physicians generally received the medical intuition sessions positively, appreciating the detailed descriptions and practical diagnostic and therapeutic suggestions. They found the sessions beneficial for clinical insights and noted that much of the information often validated known symptoms. Five themes emerged:
Quality of the Information Received
One physician found the information easy to understand, and 2 others praised its level of detail.
Clinical Process
One mentioned they received “several specific suggestions that I can now consider both independently and on my own with my patient.”
Variation in Medical Intuitives
Two mentioned that some medical intuitives gave more specific details than others. One said they would continue using the medical intuitive after 2 sessions with them.
Gratitude and Appreciation
Three expressed gratitude and appreciation for the medical intuition sessions, highlighting specific observations and detailed descriptions from the medical intuitives, which gave the physicians valuable diagnostic and therapeutic insights. They described their experiences as excellent, helpful, and filled with valuable guidance, citing “Great work! I appreciate this guidance,” “Very positive experience,” and “Great detail and descriptions.”
Session Procedure Feedback
One reported insufficient time with the medical intuitive, and another felt that asking questions in a specific way yielded more useful information.
Patients’ Free Text Answers After Medical Intuition Sessions
Twenty-four of the forty patients entered free text about the study, which was analyzed separately for themes.
Session Procedure Feedback
Some participants commented on the session procedures, noting the influence of the physician’s presence and the desire for more frequent and longer sessions to uncover more information. One participant said they might have asked more personal questions without the physician present, while another mentioned that the physician’s input might have inadvertently misdirected the session.
Quality of the Information Received
Many found the sessions confirmed their existing knowledge and validated their perceptions and those of their healthcare physicians. One patient shared, “The medical intuitive is dead-on accurate with currently known information.” Another said, “The medical intuitive read me like a book. I cannot believe how accurate my reading was; it was almost eerie but very confirming.” However, some offered mixed feedback. Four patients noted that some information did not resonate with their experience, and 3 expressed that they wanted more detail. For example, 1 participant remarked, “While some of the information shared did not hit the target, enough of it rang true to give me some helpful recommendations on how to balance my mindset and care for myself through the healing process.”
Beneficial Outcomes
Sixteen patients expressed overwhelmingly positive sentiments regarding their medical intuition sessions, noting feelings of amazement, gratitude, and satisfaction with the insights and recommendations provided by the medical intuitives. Many found the sessions beneficial for their emotional and mental well-being, confirming their perceptions and providing valuable guidance. The experience was described as enlightening, confidence-boosting, and highly accurate, with participants expressing a desire for continued engagement. One shared, “I really enjoyed the experience. It was very interesting, not stressful, and most of it was very accurate and relevant to me,” while another remarked, “A very powerful session - blown away.” 7 patients mentioned specific health outcomes, particularly mental and emotional, saying the sessions were “extremely beneficial and confidence-boosting” and “helpful and affirming mentally and emotionally.” 4 patients found immediate practical recommendations useful and relevant, such as, “The medical intuition session was very informative and provided recommendations that could be beneficial.” However, a few patients expressed uncertainty about how to practically implement the insights, with 1 stating, “Although it was very helpful and affirming mentally and emotionally, I guess I’m just not sure what to do with that information on a practical level,” and another noting, “Not really sure how helpful this is unless/until I have time to follow up and try some of the things she suggested.”
Future Implementation
Finally, several patients spoke about their use of medical intuition outside of the study, including registering for medical intuitive training, engaging medical intuitives again outside of the study, recommending medical intuition to others, and feeling it should be integrated into mainstream medicine. For example, several patients asked if it were possible to have additional sessions with their medical intuitives and requested their contact information.
Discussion
This study examined the usefulness and accuracy of, and satisfaction with, using medical intuitives virtually in medical visits. The findings support the potential value of medical intuition sessions in a clinical setting.
Before having the medical intuition sessions, patients did not believe the medical intuition sessions to be as credible as usual care visits and did not have very high expectations for the sessions, reflecting a relatively unbiased patient sample (eg, a biased sample would have had greater scores for the medical intuition sessions). However, afterward, they rated the medical intuition sessions to have high overall accuracy and high to very high accuracy regarding specific health issues. They also reported very high levels of satisfaction. Patients’ qualitative reports showed generally positive experiences with the medical intuition sessions. Patients who engaged in the sessions felt validated, emotionally supported, and curious, finding the sessions insightful or transformative. Many wanted additional time to delve deeper into their personal inquiries. However, a few expressed skepticism of the session or uncertainty regarding the practical application and long-term advantages of the sessions. While we did measure credibility and expectancy, there are 3 additional, unmeasured potential factors that may have influenced the patient’s skepticism: 1) whether the patient’s personal beliefs about healing are aligned with a medical intuition approach, 2) skepticism around a novel approach to their healthcare that they may not have experienced before or understood, and 3) a potential time lag medical intuitives have often noted between the medical intuition session and the patient’s assimilation of the assessment, including recollections of life events, that may help them integrate the information more fully and potentially take action.
Physicians reported the medical intuition sessions to have high levels of usefulness and very high accuracy and an ability to connect life events to patient issues, findings which agree with the work of Colter & Mills (2020). Physicians reported high to very high levels of satisfaction and said they would recommend medical intuition sessions to their colleagues. Physicians’ free text responses indicated that medical intuition sessions often helped them redirect diagnosis and treatment, validated existing plans, reduced unnecessary testing, identified potential emotional and life event factors, generated thoughts for follow-up testing, and encouraged the exploration of new options. Several physicians felt that the information might reduce unnecessary diagnostic testing or suggest more targeted evaluations. These reports reflect physician perceptions rather than measured changes in diagnostic behavior, as the study did not track ordering patterns or clinical outcomes. Nonetheless, the perceived potential for streamlining clinical decision-making highlights an area warranting systematic evaluation in future studies.
The very high and high accuracy ratings from both physicians and patients, respectively, are noteworthy, especially given that the medical intuitive had no previous knowledge of the patient’s identity or health information. It is important to emphasize that these ratings reflect perceived accuracy rather than objectively verified diagnostic correctness. Physicians’ ratings were informed by their clinical knowledge of the case, including access to patient charts and medical history, while patients’ ratings drew from their own personal experience. It is important to note that medical intuitives report that a client may not perceive the intuited life event or health information as resonant until well after the session date. Additionally, medical intuitives may perceive health information that has not yet manifested in a client’s experience, and may therefore be perceived by the client as inaccurate. Future longitudinal studies should assess these aspects. Within this subjective framework, both groups consistently reported that the intuitives described information that aligned with their knowledge of the case. This perceived resonance may help explain why both physicians and patients highlighted potential clinical value, particularly in identifying connections between life events and health symptoms. However, objective measures, such as independent clinical adjudication, chart review by blinded experts, or physiological outcomes, were not included and remain essential for future research.
The majority of patients also either agreed or strongly agreed with the assessment made by the medical intuitive regarding the link between life events and health symptoms, a view also corroborated by the physicians as useful information. The qualitative data also emphasized the potentially transformative nature of these connections for both the patient and physician, thereby suggesting a potential role for medical intuitives in enhancing patient care that addresses the entire spectrum of the patient’s well-being, insights that might be inadvertently neglected using traditional approaches. These narrative reports highlighted that, for some participants, exploring such connections felt validating or potentially transformative. While these impressions do not constitute objective clinical outcomes, they suggest avenues for future research on how intuitive or narrative-based assessments may intersect with patient engagement, emotional well-being, or mind–body frameworks within integrative care.
This study had limitations that warrant consideration. Although this study included only 5 professional medical intuitives, they were selected using consistent vetting and preparation procedures, which may influence reproducibility in future studies. All professional medical intuitives should be able to intuitively assess the physical body and biofield, as per the definition of a “medical intuitive,” according to the NIH Institute of Medicine. 7 This sample size also limited the ability to examine practitioner variability, an issue that should be explored in future research. This study did not measure inter-rater reliability among medical intuitives, as the intuitives did not evaluate the same patients. Future studies should incorporate designs that enable the formal assessment of reliability across practitioners. Physicians’ moderate credibility and expectancy scores suggest a potential bias toward medical intuition than an average physician, in that physicians who agreed to participate were more likely open to the possibility that medical intuitives may offer clinical benefits. However, their scores for medical intuition were not statistically greater than the usual care credibility and expectancy ratings, reflecting their view that both interventions would perform similarly (ie, they were not more biased towards medical intuition). In addition, none had used medical intuition in their practices previously, and their belief in medical intuition varied. These factors may limit generalizability, and future studies should recruit a broader physician sample from standard medical settings.
The study did not include objective measures of diagnostic accuracy or changes in diagnostic testing; all ratings reflected physician and patient perceptions. Future research should incorporate objective validation methods such as blinded chart review, biomarker confirmation, or tracking diagnostic test ordering. To protect confidentiality across virtual clinical sites, the research dataset did not include patients’ specific diagnoses, detailed symptom histories, or other protected health information. Consequently, case-level clinical descriptions could not be provided. Treatment resistance was determined and documented by the referring physicians based on their clinical knowledge of the patient and access to the medical record. Future studies could include structured diagnostic data with appropriate consent. The study design was also limited in that the use of a randomized controlled trial, clinical outcome assessment over time, and more validated instruments would have produced more robust results. The pragmatic design provides ecological validity but restricts causal inference.
This study was not designed to isolate the unique contribution of intuitive perception from other factors such as extended time, reflective dialogue, or empathic engagement. Because sessions involved exploration of personal history and psychosocial context, similar insights could emerge from other supportive modalities (eg, health coaching, extended interviews, or AI-assisted tools). Participants’ reports of helpfulness may therefore reflect non-specific therapeutic effects rather than intuitive perception itself. Without mechanistic control conditions or objective clinical outcomes, the study cannot determine which components account for perceived benefits. Future trials should include comparison groups capable of distinguishing intuition-specific effects from general supportive processes.
Qualitative data consisted of brief, open-ended comments rather than structured interviews; therefore, the resulting themes are exploratory and not intended to map directly onto theoretical models or predefined research questions. Because of space constraints and the pilot nature of the study, some methodological details (eg, extended selection criteria, qualitative coding procedures) are summarized in abbreviated form in the manuscript and elaborated in the Supplemental Data. The study also did not control for potential confounding variables, further limiting causal interpretation. Although our definition of “medical intuition” aligns with NIH Institute of Medicine descriptions, practitioner variability may influence reproducibility and should be examined in future research.
The study did not assess whether physicians discussed each medical intuition session with their patients, nor did it capture paired discrepancies between physician and patient evaluations of the same session. As such, we cannot draw conclusions about concordance or divergence in perceived value at the individual-session level.
Finally, both physicians and patients desired more time to interact with the medical intuitive. The inclusion of a follow-up visit for the physician and patient to debrief after the medical intuition session would have fostered the integration process.
Conclusion
The integration of medical intuition into healthcare has promising potential, particularly in validating patients’ symptoms, and enhancing comprehension of the emotional and spiritual contributions to disease. Medical intuition sessions appear to provide valuable supplementary health insights that can augment traditional clinical practices. Subsequent research could continue to move the field forward by using larger patient, physician, and medical intuitives sample sizes, long-term follow-up, a diverse patient sample, and a more generalizable physician sample recruited from standard hospitals and clinics or standard medical professional organizations.
Supplemental Material
Supplemental material - Physician and Patient Perspectives of the Usefulness and Accuracy of Medical Intuition: A Prospective Pragmatic Trial
Supplemental material for Physician and Patient Perspectives of the Usefulness and Accuracy of Medical Intuition: A Prospective Pragmatic Trial by Helané Wahbeh, Sitara Taddeo, Wendie Colter and Leonard A. Wisneski in Global Advances in Integrative Medicine and Health
Footnotes
Acknowledgements
We are very grateful for the participation of the medical intuitives, patients, and physicians in this study. We also are grateful to Mary Coan, MD, Lloyd Costello, MD, Midge Murphy, JD, PhD, Sandy Robertson, RN, MSN, CMIP, CHTP, and Stephanie L. Taylor, PhD, for their support in making this study possible.
Ethical Considerations
The study protocol and associated procedures were approved by the IONS Institutional Review Board [IORG#0003743].
Consent to Participate
Participants were consented verbally, and provided them with an electronic consent form to sign.
Authorship Contribution
Dr. Wahbeh contributed to conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, supervision, writing - original draft, writing - review and editing.
Ms. Taddeo contributed to data curation, writing – review and editing.
Ms. Colter contributed to conceptualization, including study measure development, methodology, recruiting and vetting the medical intuitives, writing - review and editing
Dr. Wisneski contributed to conceptualization, methodology, writing - review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by an anonymous funder. Role of the study sponsors - The study sponsors provided initial feedback on the draft study design but had no further involvement after the protocol was finalized. They did not participate in execution, recruitment, data collection, analysis, or manuscript preparation. They did provide feedback on the conflict of interest statement. All research activities and reporting were conducted independently by the research team, ensuring the integrity and impartiality of the study.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have completed the ICMJE uniform disclosure form at ![]() and declare: WC has been paid as the founder/CEO of the for-profit The Practical Path, Inc., a medical intuition training organization, maintains a paid private practice as a medical intuitive, and has received royalties from Watkins Publishing as the author of the book Essentials of Medical Intuition. WC is President of the nonprofit National Organization for Medical Intuition in an unpaid position. WC recruited and vetted the medical intuitives for the study, including practitioners drawn from networks affiliated with The Practical Path, Inc.; they were paid by IONS for their work in the study. WC had a role in the study design and manuscript preparation. WC was not involved in choosing the physicians in the study, any study visits, data collection and management, and analysis. LW is on the Advisory Board of the nonprofit National Organization for Medical Intuition in an unpaid position. WC and LW were paid for their consultation on this study by the Institute of Noetic Sciences.
and declare: WC has been paid as the founder/CEO of the for-profit The Practical Path, Inc., a medical intuition training organization, maintains a paid private practice as a medical intuitive, and has received royalties from Watkins Publishing as the author of the book Essentials of Medical Intuition. WC is President of the nonprofit National Organization for Medical Intuition in an unpaid position. WC recruited and vetted the medical intuitives for the study, including practitioners drawn from networks affiliated with The Practical Path, Inc.; they were paid by IONS for their work in the study. WC had a role in the study design and manuscript preparation. WC was not involved in choosing the physicians in the study, any study visits, data collection and management, and analysis. LW is on the Advisory Board of the nonprofit National Organization for Medical Intuition in an unpaid position. WC and LW were paid for their consultation on this study by the Institute of Noetic Sciences.
Data Availability Statement
The data supporting the findings of this study are available upon reasonable request.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work, the author(s) used Grammarly in order to catch grammar, punctuation, readability errors. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.