
Abstract
Introduction
Hypertension is increasingly recognized as a biopsychosocial condition influenced by psychological distress and systemic inflammation. The potential of integrative mind-body approaches such as Heartfulness meditation and yoga to offer non-pharmacological benefits through neuroendocrine and immunomodulatory pathways is a source of hope and optimism in the field.
Objective
To evaluate the effects of a 12-week Integrated Approach of Heartfulness-based Yogic Practices and Meditation (IAHFNM & YP) on psychological distress, inflammatory cytokines and stress biomarkers in individuals with prehypertension or Stage 1 hypertension.
Methods
In this randomized controlled trial participants were allocated to either the intervention group (IAHFNM and YP) or the standard care group. Psychological distress was assessed using the Brief Symptom Inventory-18 (BSI-18). Blood samples were analyzed for cytokines (IL-6, IL-1β, TNF-α, IL-10, IL-18) and neuroendocrine stress markers (copeptin and corticotropin).
Results
The intervention group showed significant reductions in psychological distress, including anxiety, depression and somatization, as reflected by a marked decline in the Global Severity Index (P < .001). This reassures us about the study’s effectiveness. Inflammatory biomarkers IL-6, IL-1β, and TNF-α significantly decreased (P < .05), while anti-inflammatory IL-10 levels increased (P < .001). Stress-related biomarkers copeptin and corticotropin also showed significant reductions (P < .001), suggesting downregulation of the hypothalamic-pituitary-adrenal (HPA) axis. Although correlations between psychological scores and biomarkers were modest (R2 < 0.12), corticotropin showed the strongest association with BSI-18 scores (r = 0.389).
Conclusion
The findings demonstrate the efficacy of Heartfulness in improving psychological well-being and modulating inflammatory and neuroendocrine markers in prehypertension and hypertension. These results support integrating mind–body practices into hypertension management. However, small sample size, limited duration, and reliance on self-reported adherence may affect generalizability. Future studies with larger cohorts, objective adherence measures, and extended follow-up are recommended to establish sustainability and underlying mechanisms.
Introduction
Hypertension is a primary global health concern responsible for over 10 million deaths annually and affecting more than 1.3 billion individuals worldwide, with the most significant burden observed in low- and middle-income countries. 1 In India, the National Family Health Survey-5 (NFHS-5) reports a hypertension prevalence of 24% in men and 21% in women aged 15-49 years. 2 Despite the availability of effective pharmacological treatments, blood pressure (BP) control remains inadequate in a significant proportion of individuals, primarily due to factors such as chronic psychosocial stress, sedentary lifestyles, and poor adherence to therapy. 3 Recent studies show that less than 21% of individuals globally with hypertension achieve optimal blood pressure control despite treatment, underscoring the urgent need for holistic and sustainable interventions. 4
Emerging evidence shows that chronic stress plays a key role in causing hypertension. It activates the hypothalamic–pituitary–adrenal (HPA) axis and the sympathetic–adrenal–medullary (SAM) system. This leads to an increase in cortisol and catecholamines. These hormones increase blood pressure by enhancing cardiac output, promoting vasoconstriction, and increasing sodium retention.5,6 Copeptin is a stable glycopeptide released with vasopressin. It is a reliable marker of chronic stress. High copeptin levels are associated with elevated blood pressure and an increased risk of cardiovascular events.7,8 Furthermore, chronic stress induces low-grade systemic inflammation marked by elevated pro-inflammatory cytokines such as interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-α), and interleukin-1β (IL-1β), all of which contribute to endothelial dysfunction and vascular remodeling.9-11 While pro-inflammatory cytokines exacerbate vascular dysfunction, IL-10, a key anti-inflammatory cytokine, helps restore immune homeostasis and protect endothelial integrity. 12
Given these mechanistic pathways, integrative non-pharmacological approaches targeting both physiological and psychological components of hypertension are being increasingly advocated. Among these, yoga and meditation have shown particular promise. Yoga interventions have been shown to modulate autonomic function by reducing sympathetic tone, lowering cortisol levels, improving baroreflex sensitivity and enhancing endothelial health.13-19 A comprehensive meta-analysis encompassing 49 randomized controlled trials (RCTs) demonstrated significant reductions in both systolic and diastolic BP following yoga-based interventions in hypertensive populations. 20 Similarly, meditation practices including mindfulness and transcendental meditation have been effective in lowering BP, attenuating stress hormone levels, and improving psychological well-being.21,22 However, most existing studies focus on yoga or meditation as stand-alone interventions, with limited exploration of synergistic, integrated protocols combining both practices.
Heartfulness Meditation, a heart-centred Raja Yoga practice that incorporates relaxation, meditation, and rejuvenation techniques, has shown beneficial outcomes in recent research, including improvements in heart rate variability, cortisol reduction, and increased parasympathetic activity.23,24 To evaluate its application in hypertensive individuals, the Integrated Approach of Heartfulness Meditation and Yoga Protocol (IAHFNM & YP) module was developed by the Heartfulness Institute and validated by a panel of 40 experts. The tool, comprising 23 items, demonstrated strong content validity (CVR ≥0.29, I-CVI >0.79, S-CVI/Ave >0.9) and high internal consistency (Cronbach’s alpha = 0.95). A pilot feasibility study among hypertensive participants confirmed high retention rates, low attrition rates, and positive subjective responses, indicating that the module is valid, reliable, and feasible for clinical implementation. 25 Validated, scalable, and culturally compatible mind–body modules, such as IAHFNM and YP, could serve as cost-effective adjuncts to standard hypertension care in diverse Indian populations.
Despite the expanding evidence base, most studies have examined yoga and meditation as independent modalities. A critical gap remains in understanding the synergistic potential of Heartfulness Meditation and yoga, particularly in terms of their combined effect on hypertension through the concurrent assessment of neuroendocrine (cortisol, copeptin), inflammatory (IL-6, TNF-α, IL-10), cardiovascular, and psychological parameters. This study, with its unique focus on the combined effects of Heartfulness Meditation and yoga, aims to fill this critical gap in research using a randomized controlled trial framework to evaluate the integrated impact of these mind-body interventions on hypertension management.
Methods
Study Design
This study was conducted as a randomized controlled clinical trial following a two-arm, parallel-group design over 12 weeks. The primary objective was to evaluate the effects of an Integrated Approach of Heartfulness Meditation and Yoga Protocol (IAHFM & YP) in conjunction with standard pharmacological care on individuals diagnosed with hypertension. The trial was conducted in accordance with the CONSORT 2025 guidelines and included a CONSORT flow diagram (Figure 1) to illustrate participant enrollment, randomization, allocation, follow-up, and analysis
26
CONSORT Flow Diagram Illustrating the Trial Design for Hypertensive Patients Enrolled in a 12-Week Intervention Using the IAHFNM & YP. The Diagram Illustrates the Stages of Participant Enrollment, Random Allocation to Intervention and Control Groups, Intervention Delivery, Follow-Up, and Final Analysis, Including Dropouts and Adherence Monitoring
The study was conducted between July 2024 and May 2025. Seventy participants were enrolled and randomly assigned to one of two groups. The Standard Care Group (SCG) received conventional antihypertensive medication by clinical guidelines. The Interventional Group received the Integrated Approach of Heartfulness Meditation and Yoga Protocol (IAHFM & YP) in addition to standard care.
Randomization and Ethical Considerations
A computer-generated randomization method was employed to ensure a balanced allocation of participants between the intervention and standard care groups, maintaining a 1:1 allocation ratio. The research coordinator exclusively managed the allocation sequence, preventing bias in participant assignment. The trial received ethical approval from the Ethics Committee for Research on Human Subjects at MGM Institute of Health Sciences, registered under DCGI approval number ECR/457/Inst/MH/2013/RR-20 (Trial Ethical No. Ref. No. MGMIHS/R&D/ECRHS/03/2023/185, dated October 5, 2023). Written informed consent was obtained from all participants prior to enrollment. The study adhered to the Declaration of Helsinki, ensuring adherence to ethical principles in medical research involving human subjects. The trial was prospectively registered with the Clinical Trials Registry - India (CTRI/2024/01/061035) on January 1, 2024, ensuring transparency and compliance with regulatory standards (https://ctri.nic.in/Clinicaltrials/regtrial.php?trialid=94075&EncHid=25278.90730&modid=1&compid=19).
Participants
A total of 70 participants aged between 35 and 60 years were enrolled through random sampling. This specific age group was selected due to the increasing prevalence of primary hypertension and associated psychosocial stress within this demographic, especially in low- and middle-income countries. 25 Additionally, targeting this age range helped to minimize confounding variables arising from age-related comorbidities commonly observed in older adults. Participants were recruited from the General Medicine Outpatient Department (OPD) of MGM Hospital, Navi Mumbai. The inclusion criteria comprised individuals diagnosed with prehypertension (systolic blood pressure [SBP] 120-139 mmHg) or Grade 1 hypertension (SBP 140-159 mmHg) who were not expected to undergo any changes in their antihypertensive medication during the study period or within the 3 months preceding the study. Exclusion criteria included secondary hypertension, severe psychiatric disorders, recent cardiovascular events (within the past 3 months), such as myocardial infarction or stroke, New York Heart Association (NYHA) Stage I or higher heart failure, peripheral arterial occlusive disease (Stage ≥1), renal failure (Stage >2, glomerular filtration rate [GFR] <60 mL/min/1.73 m2), current participation in another clinical trial, regular yoga or meditation practice within the past 6 months, and pregnancy or breastfeeding.
Intervention Protocol
The intervention was a personalized 12-week IAHFNM and YP program, tailored to each participant’s needs and delivered in addition to standard pharmacological management for participants in the intervention group. 25 The aim was to assess the efficacy of this individualized mind-body approach in managing primary hypertension. The control group, referred to as the Standard Care Group (SCG), continued only with routine antihypertensive medication and received equivalent telephonic follow-ups to monitor adherence and lifestyle modifications.
Sessions were held in the morning, and participants were instructed to wear comfortable clothing and observe a minimum fasting period of approximately 60 min before each session. To familiarize participants with the practices, an In-Person Orientation Training was conducted at the beginning of the intervention, delivered over 3 consecutive days (2 h per day), and comprised both Heartfulness meditation and yoga asana instruction.
Orientation Training Sessions
• Day 1: Introduction to the morning routine, including yoga asanas, pranayama, and Heartfulness meditation. • Day 2: Review of Day 1 practices and introduction to evening rejuvenation technique. • Day 3: Consolidation of morning and evening practices; participants were provided with audio-visual recordings and access to live guided sessions for follow-up support.
Morning Practice (45 min)
Each morning session was structured into 6 components, totaling 45 min: 1. Centering and Yogic Breathing (5 min): Initiated with a short yogic prayer followed by deep yogic breathing to center the mind. 2. Warm-up Exercises (5 min): Three standing warm-up movements to prepare the body. 3. Yoga Asanas (20 min): A sequence of 13 asanas performed with attention to breath and posture alignment. (4) Relaxation (5 min): Guided Shraavana combined with Heartfulness relaxation technique. (5) Pranayama (5 min): Participants practiced 10 rounds of Anuloma-Viloma and five rounds of Sheetali pranayama, aiding in physical and mental stabilization before meditation. (6) Meditation (5 min): Dhyana or Heartfulness meditation guided by a certified trainer. Participants attended in-person sessions 3 times a week, while online guided sessions were provided for home practice on other days.
Evening Practice (15 min): Evening sessions included: 1. Bhramari Pranayama (5 min): To calm the nervous system and reduce mental tension. 2. Heartfulness Cleaning or Rejuvenation (10 min): A meditative technique unique to the Heartfulness tradition aimed at emotional detoxification and mental clarity.
Adherence, Monitoring, and Dropouts
All participants were provided with a supportive environment to perform each intervention component under supervision. A total of 30 participants completed the full 12-week program and post-intervention assessments. Five participants withdrew during the intervention phase due to personal and time constraints; however, no adverse effects related to the intervention were reported. Participants were encouraged to continue practicing on their own over the weekends using the provided digital instructional materials. Weekly telephonic follow-up calls were made to maintain motivation and resolve participant queries. Adherence was tracked through supervised attendance logs. High adherence was defined as completion of at least 80% of the scheduled sessions.
Estimation of Outcomes
Psychometric Analysis
Psychological distress was assessed using the BSI-18, a validated psychometric tool that evaluates somatization, depression, and anxiety symptoms. Each of the 18 items was rated on a 4-point Likert scale, and raw scores were computed for subscales as well as the Global Severity Index (GSI), providing an overall measure of psychological distress 27
Biomarker Analysis
A 5 mL Blood sample was collected between 8:00-8:30 a.m. during a 10-12 h fasting period; blood was withdrawn using aseptic precautions from all the participants (at two-time points-baseline and after 12 weeks of intervention) in a plain vacutainer tube at dept of General Medicine OPD, MGM hospital, Navi Mumbai 410209 and then collected blood was transported to MGM Central research laboratory, MGM Institute of health science, Navi Mumbai, 410209. A blood sample was obtained from all participants enrolled in the SCG and the interventional group at baseline and after 3 months of intervention with IAHFNM and YP. The collected blood samples were kept at room temperature for one hour, which facilitated natural blood coagulation, followed by centrifugation at 3000 rpm for 20 min. The serum was then separated and stored at −80°C for further use. An ELISA kit was used for the analysis of biomarkers.
The blood biochemical markers were analyzed by using ELISA-based assay using the following kits respectively- Human IL-10 ELISA Kit (Elabscience-with sensitivity: 0.94 pg/mL and detection Range: 1.56-100 pg/mL), Human IL-1b (Elabscience-with sensitivity: 4.69 pg/mL and detection Range: 7.81-500 pg/mL), Human Adrenocorticotropic Hormone (Abbkine-with Detection Range: 7.5 ng/L-120 ng/L), Human TNF-α ELISA Kit (Abbkine with Sensitivity: 4 pg/mL and Detection range: 7.8 pg/mL-500 pg/mL), Human Copeptin hormone (Abbkine-with Detection range: 0.75 pmol/L-12 pmol/L), Human IL-6 ELISA Kit (Abbkine-with Sensitivity: 2 pg/mL and Detection range: 3.13 pg/mL-200 pg/mL) and Human IL-18 ELISA kit (Abbkine-with Sensitivity: 50 pg/mL and Detection range: 50 pg/mL-3200 pg/mL) by strictly following the manufacturer’s protocol. The participants were asked to visit twice for data and blood sample collection (at baseline and after 3 months).
Sample Size
The sample size was calculated using G*Power 3.1 software (Faul et al, 2007). 28 Assuming an effect size (d) of 0.75 for the difference in mean systolic blood pressure between the groups, with a power of 80% (1 - β = 0.8) and a significance level of 5% (α = 0.05), the required sample size per group was 29.29,30 Accounting for a 20% dropout rate, a total of 35 participants were targeted per group.
Statistical Analysis
All data were analyzed using IBM SPSS Statistics version 27.0. Continuous variables were expressed as mean ± standard deviation (SD). The normality of data distribution was assessed using the Kolmogorov-Smirnov test. Between-group comparisons of continuous and categorical baseline characteristics were performed using the Mann-Whitney U test for continuous variables and the chi-square test for categorical variables, respectively at the pre-intervention stage. For within-group comparisons, the Wilcoxon signed-rank test was applied due to the non-normal distribution of data. Between-group differences post-intervention were analyzed using the Mann-Whitney U test. Correlations between variables were assessed using Spearman’s rank correlation coefficient. A P-value <.05 was considered statistically significant.
Results
Sociodemographic Characteristics of Hypertensive Patients in the 12-Week Study of Integrated Approach of Heartfulness Meditation and Yoga Intervention (IAHFNM & YP) in the Interventional Group and Standard Care Group (SCG)
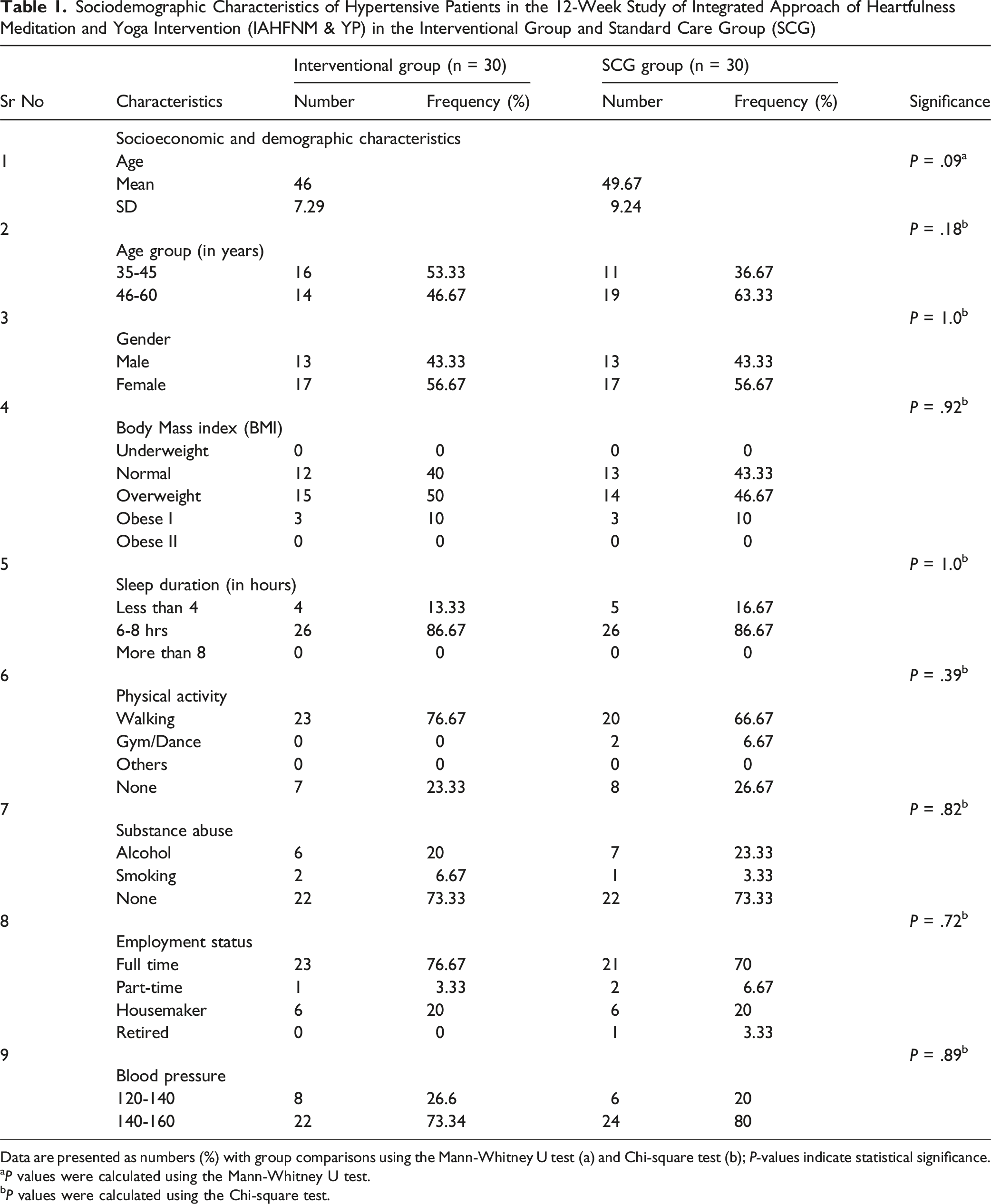
Data are presented as numbers (%) with group comparisons using the Mann-Whitney U test (a) and Chi-square test (b); P-values indicate statistical significance.
aP values were calculated using the Mann-Whitney U test.
bP values were calculated using the Chi-square test.
These findings confirm both groups were comparable at baseline, supporting the validity of subsequent analyses.
Estimation of Outcomes
Psychometric Analysis
Psychological distress was assessed using the Brief Symptom Inventory-18 (BSI-18), a validated self-report questionnaire evaluating somatization, depression, and anxiety symptoms over the preceding 7 days. The Global Severity Index (GSI) was used as an indicator of overall symptom burden, with higher scores signifying greater psychological distress.
Figure 2 illustrates the pre-and post-intervention BSI-18 total scores and subscale scores for somatization, depression, and anxiety, analyzed across the intervention and standard care groups (SCG). A significant reduction in total BSI-18 scores was observed in the intervention group post-intervention (P < .001), whereas no significant change was noted in the SCG (P = .294; ns). Subscale analyses revealed significant reductions in somatization (P = .001), depression (P = .002), and anxiety scores (P = .002) in the intervention group, while the SCG exhibited no significant improvements (somatization: P = .432; depression: P = .721; anxiety: P = .198). Pre-and Post-Intervention BSI-18 Scores and Subscale Assessments—(A) Total BSI-18 Score, (b) Depression, (C) Somatization, and (D) Anxiety Across Standard Care and Intervention Groups. Error Bars Represent the Standard Error of the Mean (SEM). Statistical Significance was Assessed Using the Wilcoxon Signed-Rank Test for Pre-Post Comparisons. ns Indicates Non-Significant Differences, P < .01 Denotes Moderate Significance, and P < .001 Indicates High Statistical Significance
At baseline, the mean BSI-18 GSI was comparable between the SCG (1.29) and intervention group (1.24). Following the intervention, the GSI in the intervention group significantly decreased to 0.62 (P < .001), whereas no significant change was observed in the SCG (1.25; P = .286). These findings suggest that IAHFNM & YP had a significant positive impact on psychological distress, particularly in reducing somatization, depression, and anxiety symptoms in hypertensive individuals. Statistical analyses confirm the effectiveness of the intervention in improving psychological well-being.
Biomarker Analysis
Median and Interquartile Range (Q1-Q3) of Inflammatory, Oxidative Stress and Stress-Related Biomarkers in SCG and Intervention Group, Pre and Post 12-Week Intervention of IAHFNM&YP

Within, Between-Group Comparisons and Group × Time Interaction
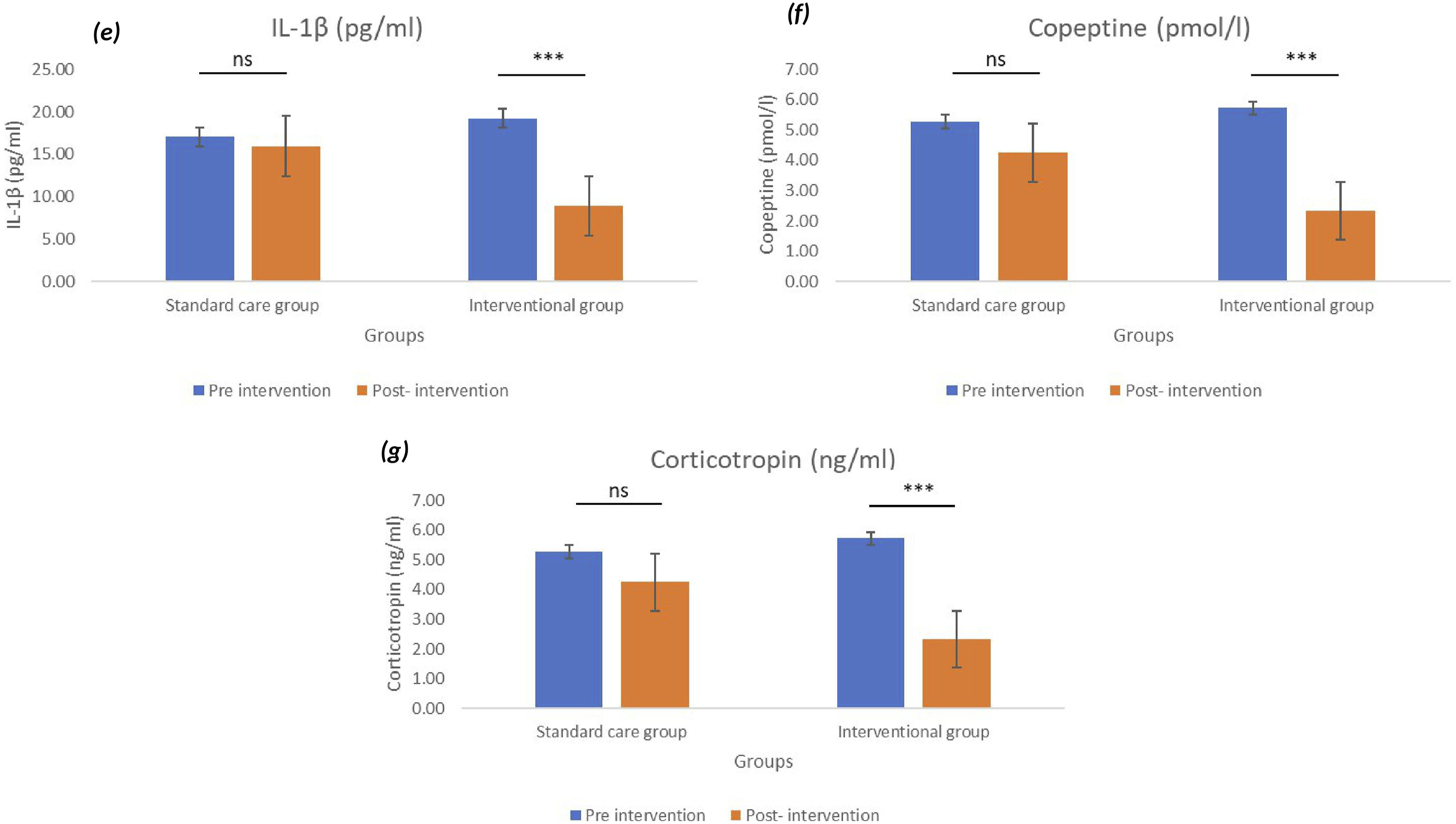
The effects of the IAHFNM & YP intervention on inflammatory and stress-related biomarkers revealed significant physiological changes in the intervention group. Post-intervention analysis revealed a significant reduction in IL-6 levels (P < .01), indicating a decrease in systemic inflammation, whereas the standard care group (SCG) showed no significant change. Conversely, IL-10 levels increased significantly (P < .001), suggesting an enhanced anti-inflammatory response in the intervention group. Additionally, TNF-α levels were significantly reduced (P < .05), whereas no notable changes were observed in the SCG. IL-18 levels showed a decreased mean value in the interventional group (baseline = 1046.24; post-intervention = 711.94); however, no statistically significant change was observed in either group. Further assessment of stress biomarkers indicated a significant decrease in IL-1β levels post-intervention (P < .001) in the intervention group, while the SCG showed no measurable changes. Similarly, copeptin and corticotropin levels significantly declined (P < .001), reflecting reduced physiological stress. These findings highlight the potential immunomodulatory and stress-reducing effects of Heartfulness Yoga and Meditation in individuals with hypertensionas assessed using the Wilcoxon signed-rank test (within-group analysis) and are illustrated in Figures 3 and 4. Comparison of Pre-and Post-Intervention Levels of Inflammatory Markers: (A) IL-6, (B) IL-10, (C) IL-18, and (D) TNF-α Across Standard Care and Study Groups. Data are Represented as Mean ± SEM. Statistical Significance Between Pre- and Post-Intervention Values: ns = Not Significant; *P < .05; **P < .01; ***P < .001 Comparison of Pre-and Post-Intervention Levels of Pro-Inflammatory Markers and Stress Biomarkers, Respectively: (e) IL-1β, (f) Copeptin, and (g) Corticotropin Across Standard Care and Interventional Groups. Data are Represented as Mean ± SEM. Statist: ns = Not Significant; ***P < .001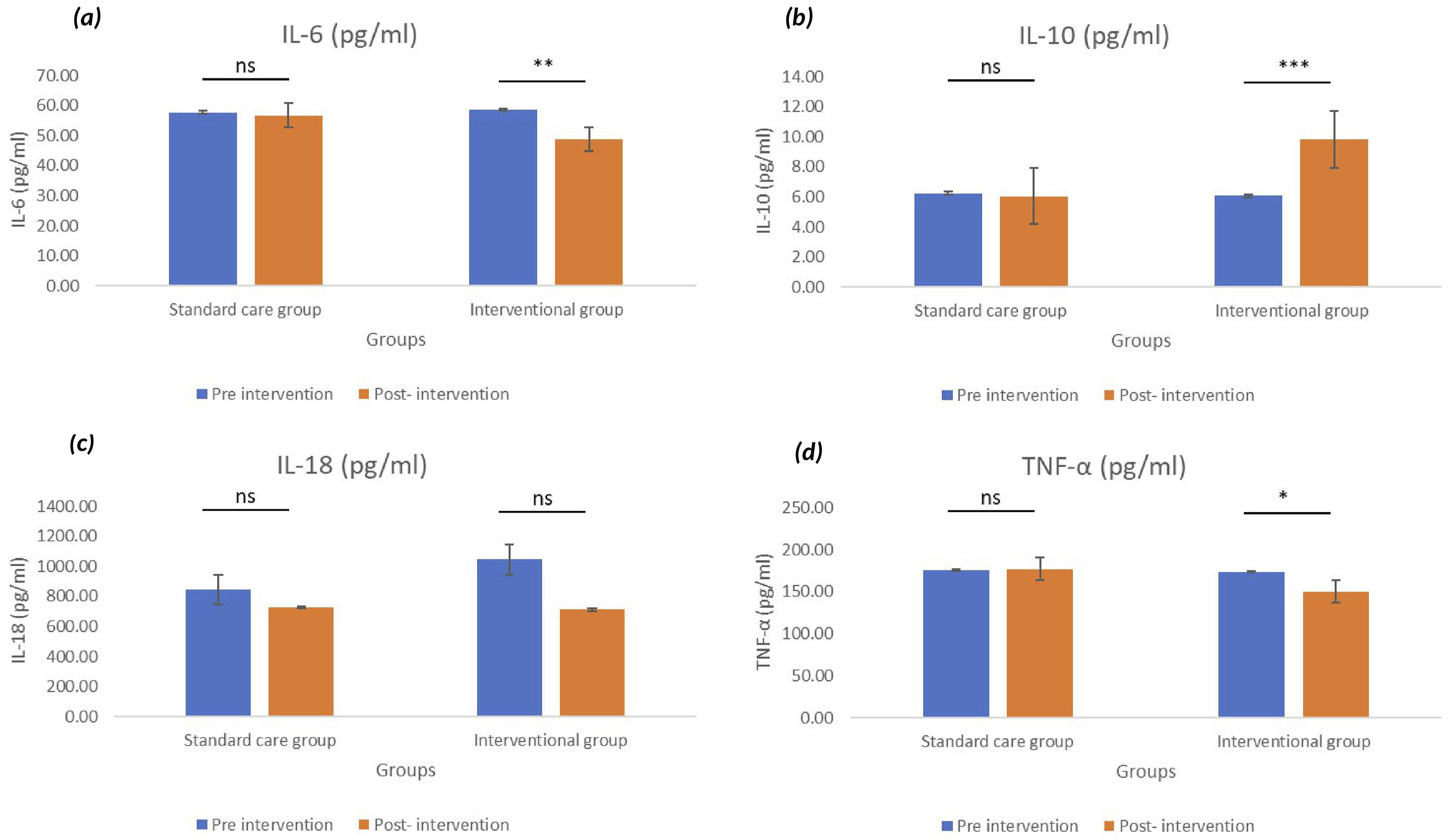
At baseline, Mann–Whitney U test results revealed no significant differences between the intervention and standard care groups (SCG) across any biomarker (P > .05), confirming comparability between groups. Following the 12-week intervention, however, significant between-group differences emerged. Participants in the intervention group demonstrated higher IL-10 levels (P < .001) and lower concentrations of IL-6 (P < .05), TNF-α (P < 0.05), IL-1β (P < .001), copeptin (P < .001) and ACTH (P < .001) relative to controls. IL-18 also differed modestly between groups (P < .05). These results suggest that the intervention improved biomarker profiles by enhancing anti-inflammatory activity while simultaneously attenuating pro-inflammatory and stress-related markers.
To further examine temporal patterns, repeated-measures ANOVA was conducted. Significant group × time interaction effects were observed for IL-10 (P < .001, η2 = 0.518), IL-1β (P < .001, η2 = 0.446) and copeptin (P = .005, η2 = 0.239) indicating that improvements in these biomarkers were substantially greater in the intervention group compared with the SCG. Trends toward significance were observed for IL-6 (P = .071) and ACTH (P = .058) suggesting possible but less robust intervention-related effects. No significant interaction effects were detected for TNF-α (P = .182) or IL-18 (P = .309).
Collectively, these findings indicate that while several biomarkers improved within the intervention group, only IL-10, IL-1β, and copeptin exhibited statistically notable differential changes over time relative to controls, underscoring their sensitivity to the Heartfulness-based intervention. IL-6, corticotropin, and TNF-α showed moderate effects, suggesting that with a longer duration of intervention, these markers may also achieve statistical significance. In contrast, IL-18 demonstrated no significant differences between groups.
Correlation Between Psychometric Analysis and Biomarker
To assess the relationship between psychological distress (as measured by BSI-18 scores) and inflammatory or stress biomarkers, simple linear regression analyses were conducted. Figure 5 illustrates scatter plots with trendlines for the biomarkers IL-6, IL-10, IL-18, TNF-α, IL-1β, copeptin, and corticotropin with BSI-18 scores. A weak negative association was observed between BSI-18 scores and IL-6 (R2 = 0.008; β = −0.32, r = −0.034), IL-18 (R2 = 0.013; β = −8.67, r = −0.268), and copeptin (R2 = 0.002; β = −0.01, r = −0.053). Conversely, weak positive associations were noted for IL-10 (R2 = 0.012; β = 0.03, r = 0.084), TNF-α (R2 = 0.003; β = 0.18, r = 0.176), and IL-1β (R2 = 0.073; β = 0.19, r = 0.288). Notably, corticotropin demonstrated a comparatively stronger positive correlation with BSI-18 scores (R2 = 0.111; β = 0.37, r = 0.389), suggesting a potential link between psychological distress and hypothalamic–pituitary–adrenal (HPA) axis activation. Scatter Plots Showing the Relationship Between BSI-18 Scores and Serum Biomarker Levels in Study Participants. The Panels Represent (A) IL-6, (B) IL-10, (C) IL-18, (D) TNF-α, (E) IL-1β, (F) Copeptin, and (G) Corticotropin. Each Plot Includes a Linear Regression Line, Along With the Regression Equation and the R2 Value. The Analysis Shows Weak Linear Associations Between Psychological Distress (BSI-18 Scores) and Inflammatory or Stress-Related Biomarkers. These Findings Suggest a Minimal Correlation Between Perceived Psychological Distress and Biological Marker Levels. The Data Include Values From Both the Pre-and Post-Intervention Phases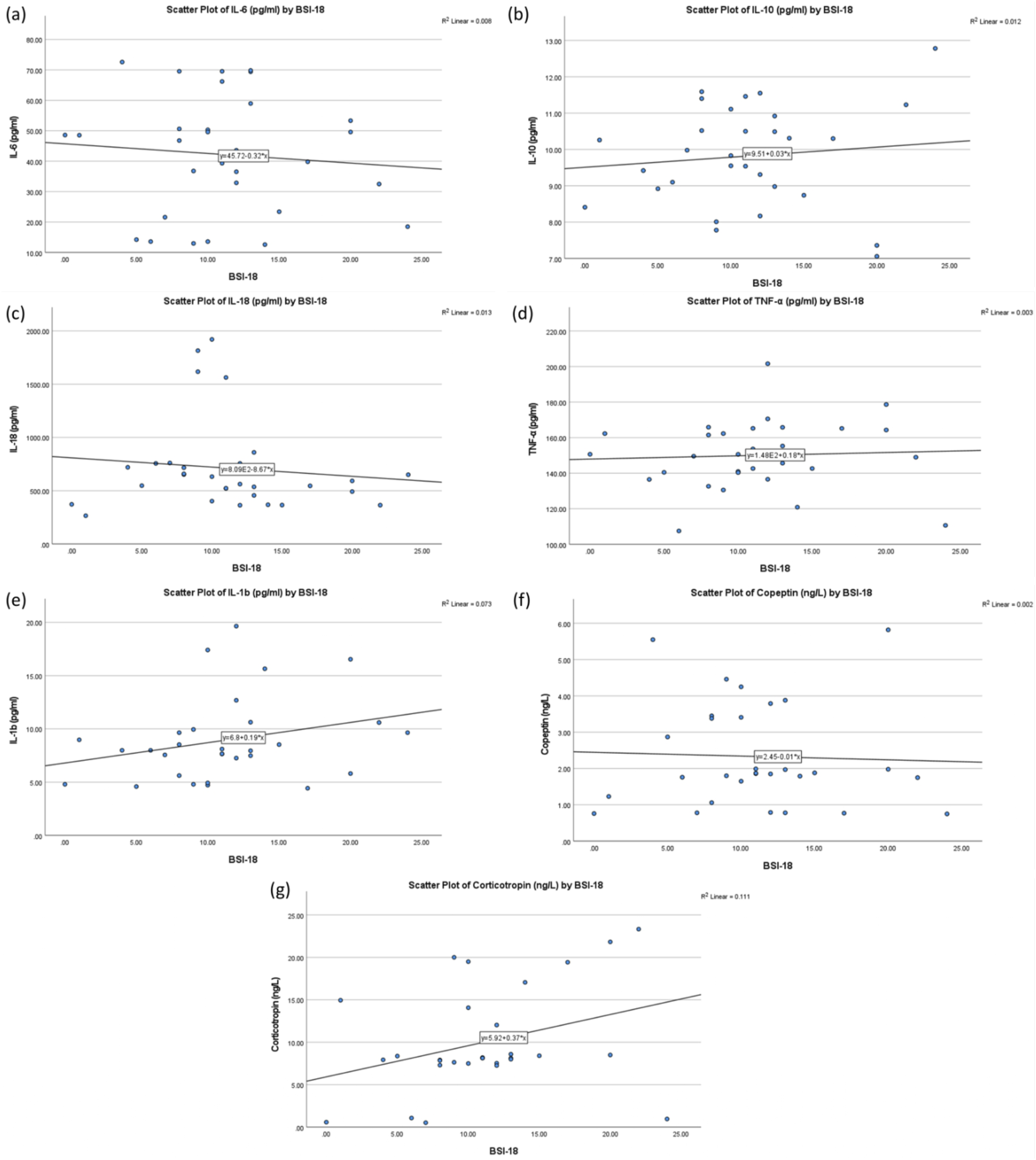
Pearson correlation coefficients (r) indicate the direction and relative strength of these associations; the low R2 values across all biomarkers demonstrate that only a small proportion of the variance in biomarker levels is explained by BSI-18 scores. Specifically, R2 values ranged from 0.002 to 0.111, indicating that psychological distress accounted for less than 12% of the variability in biomarker concentrations.
As shown in Figure 5, the relationship between BSI-18 and inflammatory biomarkers exhibits a weak association, with R2 values ranging from 0.003 to 0.013, indicating minimal variance explained by BSI-18 scores.
Discussion
This randomized controlled trial provides evidence supporting the effectiveness of a 12-week, structured IAHFNM & YP intervention in reducing psychological distress, modulating pro- and anti-inflammatory cytokines, and lowering stress-related biomarkers in individuals with prehypertension or Grade 1 hypertension. The findings align with and extend those of prior meta-analyses conducted by Park and Han (2017) and Goyal et al (2014),20,31 both of which emphasized the therapeutic potential of meditation and yoga in managing psychological and cardiovascular outcomes. Participants in our study demonstrated significant reductions in psychological distress, as measured by the Brief Symptom Inventory-18 (BSI-18), including its depression, anxiety, and somatization subdomains. The Global Severity Index (GSI) declined markedly from 1.24 to 0.62 (P < .001) after the intervention, while no significant changes were observed in the standard care group. These findings align with earlier research on mindfulness-based and transcendental meditation interventions, which have shown efficacy in lowering psychological distress and improving coping mechanisms among individuals at risk for hypertension. 32
These results also corroborate the conclusions of Goyal et al (2014), 31 who performed a comprehensive meta-analysis of 47 randomized trials and found moderate evidence that mindfulness meditation programs, including Mindfulness-Based Stress Reduction (MBSR) and Mindfulness-Based Cognitive Therapy (MBCT), significantly reduce symptoms of anxiety, depression, and psychological distress in both clinical and non-clinical populations. Specifically, their analysis revealed that these interventions yielded effect sizes ranging from 0.3 to 0.5 for psychological outcomes, with improvements sustained for up to 6 months following the intervention. Furthermore, the psychological improvements observed in our trial were consistent across gender and age subgroups, suggesting broad applicability across demographic profiles.
The mental health benefits observed in our trial may be explained by the activation of parasympathetic pathways and improved emotion regulation, which is consistent with the neurobiological mechanisms proposed in prior studies. Practices such as Heartfulness meditation and yogic breathing are known to stimulate the vagus nerve and limbic circuits, thereby reducing hypothalamic–pituitary–adrenal (HPA) axis hyperactivity and lowering cortisol output, which fosters psychological resilience.33,34 Emotional stress is a known risk factor for hypertension and cardiovascular disease, contributing to sympathetic overactivation, endothelial dysfunction, and vascular inflammation. 35 By addressing psychological stress, Heartfulness practices may offer a dual therapeutic benefit, including emotional regulation and vascular protection.24,36,37 This dual mechanism reinforces the biopsychosocial model of health, in which psychological well-being has a direct influence on physiological and biochemical functioning.
Biochemical markers measured in our study further support the hypothesis that Heartfulness practices have systemic anti-inflammatory effects. Significant reductions were observed in pro-inflammatory cytokines, including IL-6 (P < .01), TNF-α (P < .05), and IL-1β (P < .001), while the levels of IL-10, an anti-inflammatory cytokine, increased markedly (P < .001) in the intervention group. IL-18 levels remained unchanged, which may reflect the cytokine’s dual role in inflammatory and adaptive immune responses. These findings are consistent with prior literature, including the meta-analysis by Innes et al (2005) (Mirhafez SR,2014),38,39 which reported reductions in systemic inflammation among individuals practicing yoga or meditation, and with the mechanistic model proposed by Harrison et al (2011), where chronic low-grade inflammation plays a central role in the pathophysiology of hypertension through endothelial injury and arterial stiffness.
Stress-related biomarkers also demonstrated significant improvement. Both copeptin and corticotropin—surrogate markers of vasopressin and ACTH-mediated stress—decreased substantially (P < .001), suggesting HPA axis stabilization. 40 Elevated copeptin is associated with increased cardiovascular risk and blood pressure due to its vasoconstrictive and water-retentive effects via the vasopressin pathway.41,42 Similarly, high corticotropin levels reflect chronic stress and sympathetic overdrive. 40 The reduction in these biomarkers indicates that Heartfulness practices may modulate neuroendocrine responses and promote physiological relaxation. These findings align with Benson’s relaxation response theory, which posits that meditation induces a physiological state opposite to stress, characterized by decreased oxygen consumption, heart rate, and blood pressure.43,44 Importantly, distribution-based MCID analysis showed that improvements in IL-6, IL-10, TNF-α, IL-1β, copeptin, and ACTH exceeded clinical relevance thresholds, whereas IL-18 did not. Thus, the intervention demonstrated both statistically significant and clinically relevant benefits.
Although regression analyses in our study revealed only weak correlations between psychological distress and biomarkers (R2 < 0.12), the strongest association was between corticotropin and BSI-18 scores (r = 0.389). This moderate relationship suggests a partial link between perceived emotional stress and neuroendocrine function, consistent with psychoneuroimmunological models that describe bidirectional communication between the brain, immune system, and endocrine axes.42,45 However, the modest strength of the associations underscores that other factors, such as genetics, sleep, diet, and lifestyle, also contribute to cytokine and hormone regulation. 46
Our findings are also in alignment with Park and Han’s (2017) 20 meta-analysis of 13 randomized controlled trials (n = 753), which demonstrated that both yoga and meditation significantly reduced systolic (SBP: −7.37 mmHg for meditation; −4.59 mmHg for yoga) and diastolic blood pressure (DBP: −5.43 mmHg for meditation; −3.65 mmHg for yoga). Notably, their subgroup analysis revealed that meditation was more effective in older adults (>60 years) while yoga was more effective in younger populations (<60 years). Given that our participants had a mean age of 47 years, the combination of yoga and meditation through the HFN protocol likely maximized the benefit. The fixed-effects model in their analysis showed minimal heterogeneity for yoga in younger individuals (I2 = 0.0%), suggesting robust and consistent benefits across studies. Moreover, none of the studies in Park and Han’s review or our own reported adverse events, confirming the safety and acceptability of mind-body interventions.
From a public health perspective, our study supports the integration of Heartfulness Yoga and Meditation into standard hypertension care. These practices are non-pharmacological, low-cost, and scalable, making them suitable for both urban and rural healthcare systems. They address multiple dimensions of health, psychological, immunological, and endocrine, making them uniquely suited for managing chronic, stress-related disorders such as hypertension. Additionally, their accessibility and cultural acceptability in the Indian context makes them ideal for integration into AYUSH-based wellness programs and community health initiatives. Future research should replicate these findings in multicenter trials with larger sample sizes, longer follow-up durations, and additional objective endpoints, such as ambulatory blood pressure, heart rate variability, and cortisol awakening response, to fully elucidate the underlying mechanisms. Moreover, mechanistic studies using neuroimaging, metabolomics, and transcriptomics may further unravel the biological pathways influenced by Heartfulness-based interventions.
Limitations and Future Research
This study has several limitations that should be taken into account when interpreting the findings. Firstly, the relatively small sample size and short duration of the intervention may limit the generalizability of the results and restrict insights into the long-term effects of the intervention. Secondly, the absence of significant correlations between psychological measures and biomarker changes might be attributable to limited statistical power or the presence of complex, multifactorial underlying mechanisms that were not fully captured. Thirdly, the study relied on participants reporting their adherence to the intervention, which may have introduced bias and made it difficult to measure how well they followed the protocol accurately. Future research should address these limitations by including larger and more diverse participant groups, extending follow-up periods to assess sustained outcomes, and incorporating objective methods to measure adherence, such as electronic monitoring, biochemical markers, or wearable device data. Moreover, comparative studies assessing the intervention alongside established therapeutic modalities—such as cognitive-behavioral therapy, mindfulness-based stress reduction, and pharmacological treatments are necessary to elucidate its relative efficacy.
Footnotes
Acknowledgments
This research was fully self-funded. We extend our heartfelt appreciation to the compassionate and committed volunteers with hypertension who not only participated in the study but also diligently maintained their practice. Their involvement was crucial to the project’s success. We are grateful to the Heartfulness Centre in New Panvel for providing the necessary facilities to conduct the intervention. Our thanks also go to the Central Research Laboratory at MGM School of Biomedical Sciences for their support in providing infrastructure for conducting experiments before and after the intervention. We also acknowledge the support of MGM Hospital for facilitating the recruitment of participants, which was an important aspect of this study. Finally, the authors express their sincere gratitude to Kamlesh D. Patel, M. Pharm, Global Guide of Heartfulness, for his insightful guidance and advisory support throughout the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trial Registration
CTRI No: CTRI/2024/01/061035.