
Abstract
Background
Assessing the use and effectiveness of complementary and integrative health (CIH) therapies via survey can be complicated given CIH therapies are used in various locations and formats, the dosing required to have an effect is unclear, the potential health and well-being outcomes are many, and describing CIH therapies can be challenging. Few surveys assessing CIH therapy use and effectiveness exist, and none sufficiently reflect these complexities.
Objective
In a large-scale Veterans Health Administration (VA) quality improvement effort, we developed the “Complementary and Integrative Health Therapy Patient Experience Survey”, a longitudinal, electronic patient self-administered survey to comprehensively assess CIH therapy use and outcomes.
Methods
We obtained guidance from the literature, subject matter experts, and Veteran patients who used CIH therapies in designing the survey. As a validity check, we completed cognitive testing and interviews with those patients. We conducted the survey (March 2021-April 2023), inviting 15,608 Veterans with chronic musculoskeletal pain with a recent CIH appointment or referral identified in VA electronic medical records (EMR) to participate. As a second validity check, we compared VA EMR data and patient self-reports of CIH therapy utilization a month after survey initiation and again at survey conclusion.
Results
The 64-item, electronic survey assesses CIH dosing (amount and timing), delivery format and location, provider location, and payor. It also assesses 7 patient-reported outcomes (pain, global mental health, global physical health, depression, quality of life, stress, and meaning/purpose in life), and 3 potential mediators (perceived health competency, healthcare engagement, and self-efficacy for managing diseases). The survey took 17 minutes on average to complete and had a baseline response rate of 45.3%. We found high degrees of concordance between self-reported and EMR data for all therapies except meditation.
Conclusions
Validly assessing patient-reported CIH therapy use and outcomes is complex, but possible.
Introduction
The use of complementary and integrative health (CIH) therapies, such as yoga, meditation/mindfulness, and Tai Chi, has proliferated throughout healthcare systems, businesses, at home, and communities. CIH therapies are available through health systems at in-person classes, electronic applications (apps), and via telehealth formats. Although CIH therapies appear to affect a range of outcomes,1–13 the field has not coalesced around the dosing (eg, what amount of CIH therapies over what time period) required to have an effect, even more so when CIH therapies are often given in concert with other treatment therapies. Moreover, it is unclear whether patients’ self-reports or electronic appointment and billing data are more accurate depictions of patients’ CIH therapy use. Yet, it can be difficult to clearly write survey stand-alone (not verbally delivered) questions to elicit the details necessary to determine CIH therapy dosing (amount and timing), delivery format, and patient-reported outcomes.
The Veterans Health Administration (VA), the nation’s largest integrated healthcare system, is transforming to a Whole Health System of care. 14 This incorporates CIH therapies as part of Veterans’ routine care in addition to allopathic care, reflecting a major shift from episodic, disease-centered care to engaging and empowering patients throughout their lives to take charge of their life and health. The VA encourages appropriate CIH therapy use not only at the VA, but also at-home, or in the community. As such, there is a need for the VA to assess not only patients’ use of CIH therapies it provides as a part of the Veterans health and well-being plan, both in and outside the VA, but also patients’ use of the therapies at their homes or communities, and outcomes from using those therapies.
Two well-known surveys of CIH therapy use are the “Self Assessment of Change” by Rittenbaugh et al (2011) 15 and the Center for Disease Control and Prevention’s National Health Interview Survey (NHIS). 16 The former assesses patient-reported outcomes with 16 items but does not assess the duration, timing, format, or location of the CIH therapy provided. The NHIS survey assesses CIH therapy use frequency and reasons for use. But does not assess dosing, therapy format and location, and several important CIH-relevant outcomes.
Therefore, we developed the Complementary and Integrative Health Therapy Patient Experience Survey as part of a large-scale quality improvement effort collaboratively conducted by researchers and operational partners to support the ongoing monitoring of CIH therapy provision and effectiveness in the VA. This longitudinal electronic patient survey was designed to comprehensively assess CIH therapy use details (eg, amount, timing, location, and format), and patient-reported health outcomes. This paper describes the survey development process, content, and validation.
Methods
Overview
We developed an electronic longitudinal Complementary and Integrative Health Patient Therapy Experience Survey to assess individuals’ use of 8 CIH therapies ((1) yoga, (2) meditation, (3) mindfulness, (4) Tai Chi, (5) Qigong, (6) acupuncture, (7) therapeutic massage, and (8) chiropractic care) and to examine 7 patient-reported health and wellness outcomes related to that use. The survey instrument was designed to be used among Veterans with chronic musculoskeletal pain but includes other health outcomes that are highly prevalent in the general population, so the instrument can be used for almost all populations. We report below on the steps we conducted from October 2018 to January 2021 to develop the survey, using the Consensus-Based Checklist for Reporting of Survey Studies (CROSS) as guidance. 17 This included first reviewing the literature and engaging the 12-member Advisory Board of a VA-funded CIH therapy research study, which was comprised of nationally-known clinicians and researchers specializing in each of the 8 CIH therapies, to develop the survey. We also conducted cognitive and electronic survey format testing among Veteran patients utilizing CIH therapies in the VA. We then reviewed and iteratively modified the ordering of the survey items with the company administering the survey, given their expertise in electronic survey user-design. We also obtained input on pain measurement items from our colleagues in the NIH-DoD-VA Pain Management Collaboratory. 18 We fielded the survey from March 2021 to April 2023 among a target sample of 15,608 Veterans with chronic musculoskeletal pain. In May 2021, we conducted validity checks by interviewing Veterans whose self-reports of CIH use did not match what we found in the EMR and administrative records (appointment and billing data; “EMR” for short) to determine if additional revisions to the survey wording were needed. These details are provided below. The VA Greater Los Angeles Institutional Review Board determined this to be a quality improvement project, not a research study.
Measuring CIH Therapy Use
We first reviewed the literature to examine how other surveys described CIH therapies, and assessed CIH therapy dosing (frequency and timing), provider locations (community-based or VA-based), formats (eg, app, in-person, telehealth), and payors (self, insurance, VA). We then posed potential survey wording to the subject matter experts on the Advisory Board and study team members (ST, SZ, ARE, KL, AC) interviewed each clinician/researcher pair for each CIH therapy. Experts recommended collapsing Tai Chi and Qigong and collapsing meditation and mindfulness to reduce respondent burden, because although distinctive, they were similar enough in practice and should have similar effects. (Other researchers using this survey can easily opt to ask about these therapies individually.) These experts were also instrumental in determining survey questions related to assessing Veterans’ perceptions of CIH delivery formats and determining an effective “dose” for each therapy (the amount of CIH used over a specific time period that might have an effect). Especially important was determining how to most effectively structure the questions given that the electronic survey would require using complex skip patterns. The subject matter experts also advised on the frequency that the survey should be given to best assess CIH use and its relationship to patient-reported outcomes longitudinally.
Measuring Patient-Reported Outcomes and Potential Mediators
We first reviewed the literature and consulted the same subject matter experts to determine the health and well-being outcomes that might most be affected by CIH therapies, the measures that best assessed those outcomes, and a few potential mediators of the relationship between CIH therapy use and the outcomes. Study team members (ST, SZ, ARE, AC, CD, BL, AK, BB, BK, AW) then used an iterative consensus process to generate a draft list of survey items, prioritizing measures that were frequently used, had higher validity and were brief. Subsequently, we also added a final measure based on the results of the respondent cognitive interviews described below.
Testing and Validating Content
We conducted 4 phases of testing. First, we gave the draft survey to 9 Veteran patients who had received CIH therapies and conducted cognitive interviews. We asked them to identify health and well-being constructs affected by CIH therapies and asked for their feedback on and comprehension of the survey items for clarity and completeness of capturing their experience. When doing so, we used the “think aloud” method of survey validity testing, 19 which asks respondents to read the survey and talk out loud how they interpret it and how they might respond given their interpretation. This enabled us to determine which questions might be misunderstood or be too difficult to answer.
Second, we iteratively tested the phone and computer versions of the draft survey among our project team and 9 additional Veteran patients who had used CIH therapies. The electronic format had skip patterns that reduced respondent burden when asking about details of 8 therapies, but we did not want those skip patterns to be burdensome. As such, we gave the online and phone interview versions of the draft survey to patients and again conducted the “think aloud” cognitive interviews to get their input on skip pattern complexity and survey content, and made additional survey revisions accordingly. The 18 Veteran patients participating in this testing represented the broad range of Veterans in age, gender and race/ethnicity.
The third validity check was conducted a month after we initiated the survey. We compared the percentage of patients reporting CIH therapy use at their VA medical facility vs the percentage of patients having CIH therapy use recorded in the VA’s EMR to determine the degree of discordance, given they ideally should match. We then interviewed 30 of the 45 patients for whom we observed discrepancies to determine the reason for the discrepancies. When the full baseline sample was collected, we conducted that discordance validity check a second time.
Distributing the Survey
We conducted the survey from March 2021 to April 2023 using a contracted survey company. The sampling frame included 15,608 Veterans with chronic musculoskeletal pain identified as newly initiating CIH therapies in the VA EMR. Using the Dillman method, 20 the survey company sent both an email invitation and a hard copy mailed invitation. This invitation included a cover letter, a $2 bill incentive, a prepaid return envelope for patients wanting to send completed baseline surveys, and information for opting out from further mailings via a tollfree telephone number or return postcard. The cover letter came from the Executive Director of the VA’s Office of Patient Centered Care and Cultural Transformation (author BK), and described the survey’s purpose and length. It also told them they would receive 4 surveys over 6 months, provided a personalized link to the electronic survey, gave respondents a phone number to call if they preferred conducting the survey over the telephone, and noted that completing the survey was voluntary. Veterans who did not opt out and did not respond within a 6-week period were mailed a second survey with a prepaid envelope and cover letter.
Results
Survey Content- CIH Therapy Use
How the Survey Assesses Use of CIH Therapies - CIH Descriptions, Amount, Timing, Location, Format, Provider Type, Payor, and Survey Timing.

Table 1 also shows the suggested survey timing to capture longitudinal use and outcomes. That timing was related to the dose that the subject matter experts thought might have an effect on pain and pain-related conditions. They agreed that scientists had not yet coalesced around what might be an effective dose. However, when pressed, they said a minimum of five-eight sessions of meditation, yoga, Tai Chi, or Qigong lasting at least 15 minutes over an 8-week period might have an effect. Likewise, a minimum of one-two doses of acupuncture, therapeutic massage or chiropractic care in a 4-week period might have an effect. As such, the baseline survey asks separately about the past 4 weeks and the 4 weeks before that. Breaking up the 8-week time period into 2 time periods also might improve respondent recall, as some respondents might more easily remember what they did in chunks of months, instead of 2 months. The survey wording changed slightly for follow-up surveys, asking about use since the last survey instead of during the past 8 weeks for the 1-month and 3-month surveys.
Survey Content- Outcomes, Mediators and Covariates
Constructs and Measures Included in the Survey to Assess Patient Reported Outcomes and Potential Mediators.
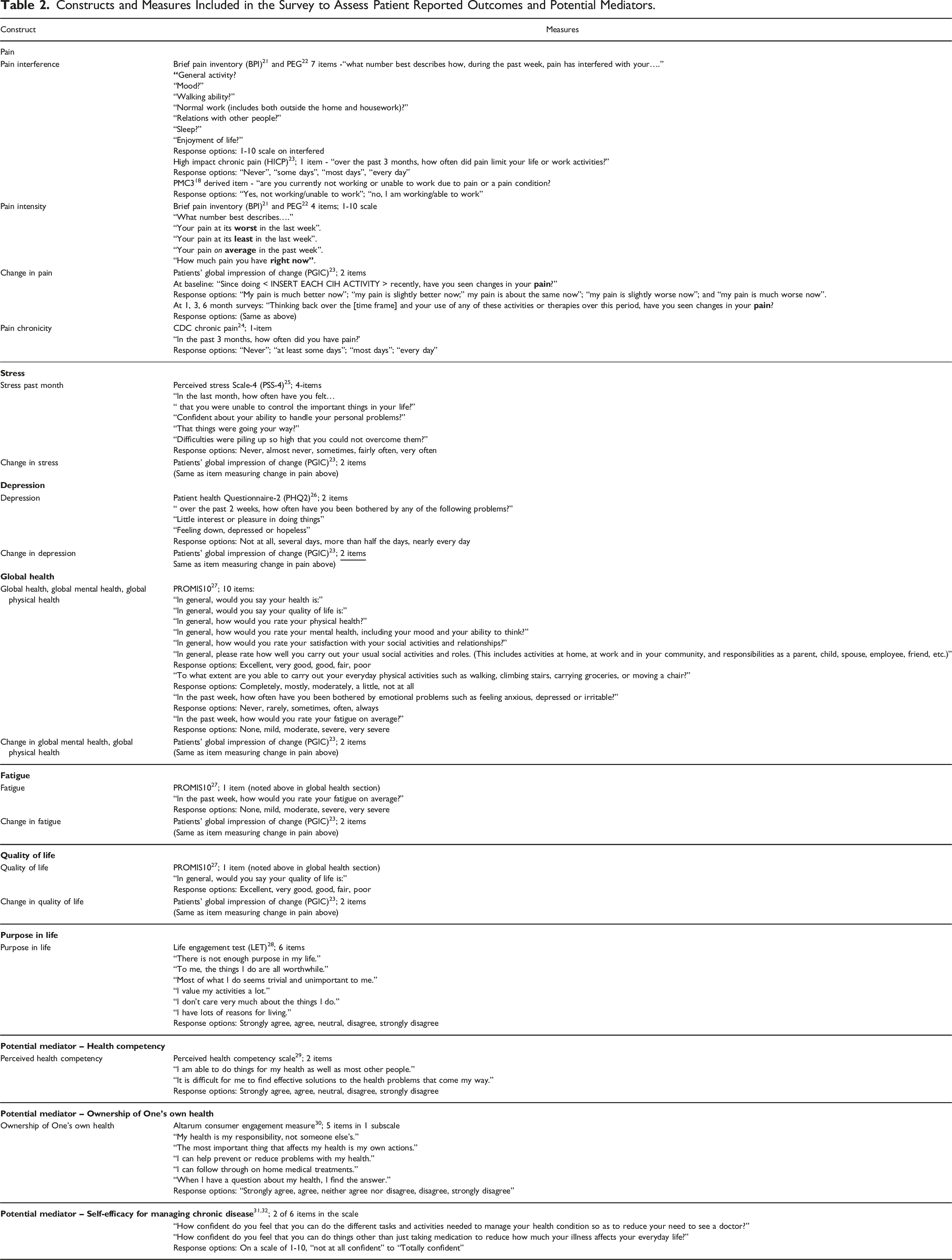
The full survey can be found in the Appendix.
Testing and Validating Survey Content
In both rounds of testing, the respondents appeared to understand the questions. The only substantial suggestion patients gave in the first round was to add a measure of purpose in life. The second round of testing showed the computer version took 16 minutes on average to complete and the mobile phone version took 18 minutes on average. It also showed the online questions and skip patterns were understandable and appropriate.
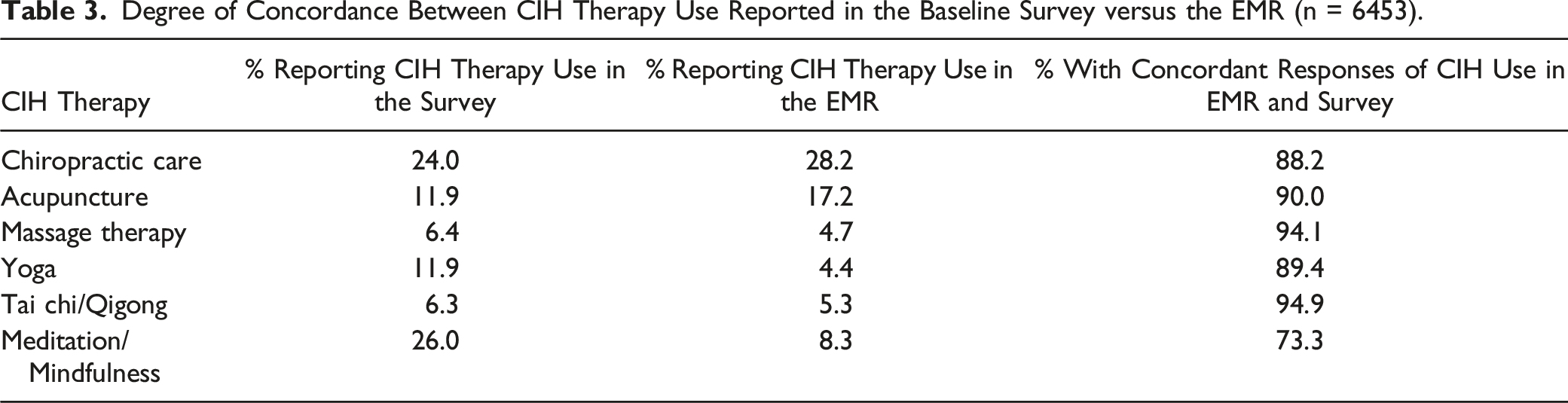
For the validity check conducted a month after survey initiation, we compared patients’ baseline self-reports of CIH therapies used at their VA medical facility vs what was recorded in the VA’s EMR to examine the degree of concordance between the 2. We found all but meditation had a high degree of concordance, so we called 45 Veterans with discordant information on meditation to determine the reason for the discordance. Of the 30 agreeing to speak to us, 47% (n = 14) reported using meditation at the VA but a week or 2 later than what was shown in the EMR, so their use was not showing in the EMR at first. The other half (53%; n = 16) said they did not use meditation at the VA when the EMR showed they did (4 said their survey was inaccurate, 8 said the EMR was inaccurate, 2 reported they signed up for meditation but ended up not using it, and 2 reported not being able to remember using it). The VA meditation clinical expert on the Advisory Board reported that many Veterans receive meditation as part of broader, multi-component VA programs and VA programs often provide meditation but call it something else (eg, “Stress and Relaxation”) to attract participants, so the patients might not have realized they received a meditation session. When we examined the medical records, we found many patients were indeed receiving programs in which some meditation was embedded, but those programs were not categorized as meditation classes (eg, they were wellness or pain relief classes).
Degree of Concordance Between CIH Therapy Use Reported in the Baseline Survey versus the EMR (n = 6453).
Characteristics of the Baseline Sample
Demographic Characteristics and Health Conditions of Baseline Survey Respondents and Nonrespondents.

aP values were obtained using a two-sample t test for continuous variables (eg, age), chi-square tests for categorical variables with more than 2 categories (eg, race, ethnicity, gender, urban residence, service connected), and two-sample tests of proportions for dichotomous variables (obesity, diabetes, hypertension, insomnia, anxiety, PTSD, depression).
bstd = standard deviation.
cAIAN = American Indian or Alaska Native, NHOPI = Native Hawaiian or Other Pacific Islander.
Discussion
With the input from a large group of nationally known CIH therapy research and clinical subject matter experts, patients who used CIH therapies, and VA national clinical operations leaders, we collaboratively developed, tested and fielded a 17-minute, 64-item, electronic survey, the Complementary and Integrative Health Therapy Patient Experience Survey, to measure patients’ longitudinal use of 8 CIH therapies and 7 longitudinal patient reported outcomes related to that use. We tested and applied the survey in the population of VHA healthcare system users with chronic musculoskeletal pain. Given these therapies are now being used in a variety of formats in healthcare systems, as well as in patients’ homes and in their communities, this survey addresses the need to comprehensively assess the amount, timing, format, provider, payor, and location of the use of CIH therapies. Our validity check comparing CIH use in the VA EMR vs self-reported VA care showed few discrepancies, demonstrating a high degree of validity for all CIH therapies except meditation. For meditation, we found self-reports were much higher than what was in the EMR, likely because patients were receiving meditation as part of a larger program and not necessarily receiving meditation stand-alone therapies.
We faced some challenges in designing this survey. We struggled with how to best assess the frequency of CIH therapy use, which was difficult given the field has not yet agreed on the dose (what amount over what time) needed to have an effect for each CIH therapy, as noted above. Another complexity was determining which of many possible outcomes to assess, given CIH therapies appear to affect many. We narrowed it down to a range of commonly studied health and wellness patient reported outcomes. We also wanted to find the right balance between creating a lengthy burdensome survey and having a sufficient number of items to comprehensively capture use. Finally, determining the best user-centered design was especially difficult given the complex skip pattern required to keep the survey from being extraordinarily lengthy. Nevertheless, we observed a relatively good response rate of 45.6% at baseline. This response rate was similar to that of the 2022 NHANES survey of CIH therapy use among the general population (49.6%) 33 and much higher than other recent national surveys of Veterans’ healthcare and health status (23.5%). 34
This survey also has some limitations. First, we oriented it to persons with chronic pain and 7 pain-related conditions instead of the general population. As such, we could have assessed other health conditions. However, the outcomes we did assess affect the majority of the general population, so others researching the effects of CIH therapy use may also be able to utilize this survey instrument. Additionally, we limited the survey to 8 CIH therapies. However, we believe researchers can easily substitute other provider-delivered or self-guided CIH therapies. In spite of these issues, we feel confident in our survey due to our extensive development process involving many experts in CIH therapy delivery and research, experts in electronic survey design, and patients who receive CIH therapies. We also feel confident due to the results of our validity checks.
In conclusion, we developed a longitudinal, electronic survey that comprehensively and appropriately captures actual CIH therapy use and key health and wellness outcomes from patients’ perspectives. The survey can be used by any healthcare organization, or anyone interested in assessing CIH therapy use, and patient reported outcomes. Future research will use data from this survey to examine CIH therapy effectiveness.
Supplemental Material
Supplemental Material - Measuring Patient-Reported Use and Outcomes From Complementary and Integrative Health Therapies: Development of the Complementary and Integrative Health Therapy Patient Experience Survey
Supplemental Material for Measuring Patient-Reported Use and Outcomes From Complementary and Integrative Health Therapies: Development of the Complementary and Integrative Health Therapy Patient Experience Survey by Stephanie L Taylor, PhD, A Rani Elwy, PhD, Barbara G Bokhour, PhD, Scott S Coggeshall, Amy Cohen, PhD, Claudia Der-Martirosian, PhD, Taona Haderlein, PhD, Jolie Haun, PhD, Benjamin Kligler, MD, Alex T Kloehn, MA, Karl A Lorenz, MD, MSHS, Briana Lott, MPH, Marlena H Shin, JD, MPH, Tammy Schult, PhD, Joy Toyama, DrPH, Alison M Whitehead, MPH, Xiaoyi Zhang, MS, and Steven B Zeliadt, PhD in Global Advances in Integrative Medicine and Health.
Footnotes
Acknowledgments
The authors wish to thank the APPROACH Study Advisory Board members: Jeffery Dusek, PhD; Ansgar Furst, PhD, MSc; Christine Goertz, DC. PhD; David Kearney, MD; Anthony J. Lisi, DC.; Louise Mahoney; Juli Olson, DC, LA; Pam Pence; Friedhelm Sandbrink MD; Robert Saper, MD; Greg Serpa, PhD; Peter Wayne, PhD; Claudia Witt, MD. We also are grateful to Dr Jolie Haun’s research team who performed the cognitive and pilot testing of the survey: Lisa Ballistrea, Lisa Ballistrea Goff, Julie McMahon-Grenz, and Maisha Standifer.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the Department of Veterans Affairs: Office of Patient-Centered Care and Cultural Transformation and Quality Enhancement Research Initiative (grant #PEC 16-354). The views in this paper are the views of the authors and do not represent the views of the Department of Veterans Affairs or the U.S. Government.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.