
Abstract
Background
Pancreatoduodenectomy (PD) and distal pancreatectomy (DP) are painful procedures often accompanied by psychological distress. Music therapy interventions such as music-assisted relaxation and imagery (MARI) have demonstrated efficacy for acute pain but have not been examined within PD/DP. Gene expression mechanisms by which MARI may affect pain also remain poorly understood.
Objective
This study assessed the feasibility and acceptability of administering MARI, collecting dried blood spots (DBS), and collecting mobile-device patient-reported outcomes (MDPRO) among adults undergoing PD/DP.
Methods
In this single-arm study, patients undergoing PD/DP received a live MARI intervention that was subsequently provided as a recording for use until discharge. DBS and numeric rating scale (NRS) measures of pain, stress, and anxiety were collected pre- (T0), post- (T1), and 15-minutes-post-MARI (T2). Participants were asked to complete MDPROs 3 times/day until discharge and participate in an interview post-discharge.
Results
Of 22 patients approached, 5 (22.7%) were enrolled (60% DP) with 80% completing all procedures. All participants completed the live MARI intervention, ≥1 NRS measure from T0-T2, ≥1 listen to the MARI recording, and ≥1 MDPRO survey. DBS sampling success was variable (9/15 [60%] across attempts). Qualitative data revealed three themes: (1) MARI was beneficial and useful throughout recovery; (2) MARI should be longer; and (3) need to improve blood sampling and mobile device procedures.
Conclusion
Preliminary findings support feasibility and acceptability of live MARI, continued MARI listening through discharge, and MDPRO collection within PD/DP. However, modifications are needed in future studies to improve blood sample collection.
Key Message
This pilot study examined the feasibility and acceptability of tailored music-assisted relaxation and imagery interventions and data collection procedures among patients undergoing pancreatic surgery. Preliminary findings support feasibility and acceptability of the intervention and patient-reported outcome collection. However, design modifications are needed to improve blood sample collection.
Introduction
Pancreatoduodenectomy (PD) and distal pancreatectomy (DP) are known to have painful postoperative recoveries. 1 Despite pharmacologic management, patients often experience elevated stress, pain, and anxiety following these procedures. 1 Therefore, nonpharmacologic approaches such as music therapy (MT), the clinical and evidence-based use of music interventions by credentialed professionals (i.e., music therapist-board certified [MT-BC]), are warranted. 2 MT is distinct from other music-based interventions such as music medicine (recorded music not provided by MT-BCs). A 2015 systematic review of 72 perioperative music medicine randomized controlled trials (RCTs) found that these interventions reduced (standardized mean difference [SMD] and 95% confidence interval [CI]) postoperative pain (−0.77 [−0.99, −0.56]), anxiety (−0.68 [−0.95, −0.41]), and analgesia use (−0.37 [−0.54, −0.20]) while also improving patient satisfaction (1.09 [0.51, 1.68]). 3 Another 2023 meta-analysis found music interventions were effective in reducing post-operative blood pressure (mean difference [MD] −5.29 [−9.53, −1.06]), and heart rate (MD −6.13 [−11.69, −0.58]). 4
Music-assisted relaxation and imagery (MARI) is a specific MT intervention combining live music with guided relaxation, breathing, and imagery. 5 In an RCT among 200 inpatients receiving palliative care, those receiving a 20-minute MARI session reported greater reductions in pain than those receiving standard care (MD −1.39 [−1.95, −0.83]). 5 MARI can also be personalized to patients’ preferences, recorded live, and subsequently provided via recording to manage sickle cell disease pain. 6 Given the typically small MT-BC-to-bed ratio in most hospitals, providing MARI recordings following an initial live intervention may help scale MT for post-surgical symptom management. However, to our knowledge no such approach has been investigated.
Despite several studies supporting music interventions’ efficacy for addressing post-operative pain, epigenomics underlying their analgesic effects remain poorly understood. Gene expression mechanisms associated with energy metabolism, mitochondrial function, and inflammatory response have been investigated within mind-body therapies,7-9 recreational music making,10,11 and classical music listening.12,13 However, to date no MT research has investigated the relationship between gene expression and acute post-surgical pain. To investigate such mechanisms within MT, protocols need to be refined for collecting blood samples pre- and post-intervention so that future mechanistic MT intervention studies can analyze blood samples for changes in gene expression among patients with acute post-surgical pain.
Given (1) the stress, pain, and anxiety levels associated with PD/DP; (2) the lack of studies investigating MT’s effects on post-operative recovery within this population; and (3) the lack of studies examining gene expression mechanisms by which MT affects pain, we launched this study to address this major gap in research. However, prior to examining mechanisms within a fully-powered RCT, we recognized the need to perform a feasibility study of the intervention and data collection procedures. The purpose of this mixed-methods pilot study was to determine the feasibility and acceptability of (1) a tailored MARI intervention; (2) mobile-device patient reported outcome (MDPRO) collection; and (3) collecting peripheral dried blood spot (DBS) samples among patients undergoing PD/DP.
Methods
Design
This study utilized a single-arm mixed-methods intervention design (see Figure 1).
14
Study procedures were planned to be completed with 20 participants, but limited to five due to slower-than-expected recruitment and funding constraints. A mixed-methods approach was chosen to enhance understanding of acceptability and uncover any changes that would need to be made to intervention delivery and data collection procedures prior to an RCT. Study Flow Diagram. Abbreviations: EHR, Electronic Health Record; MARI, Music-Assisted Relaxation and Imagery; MDPRO, Mobile-Device Patient-Reported Outcomes; NRS, Numeric Rating Scale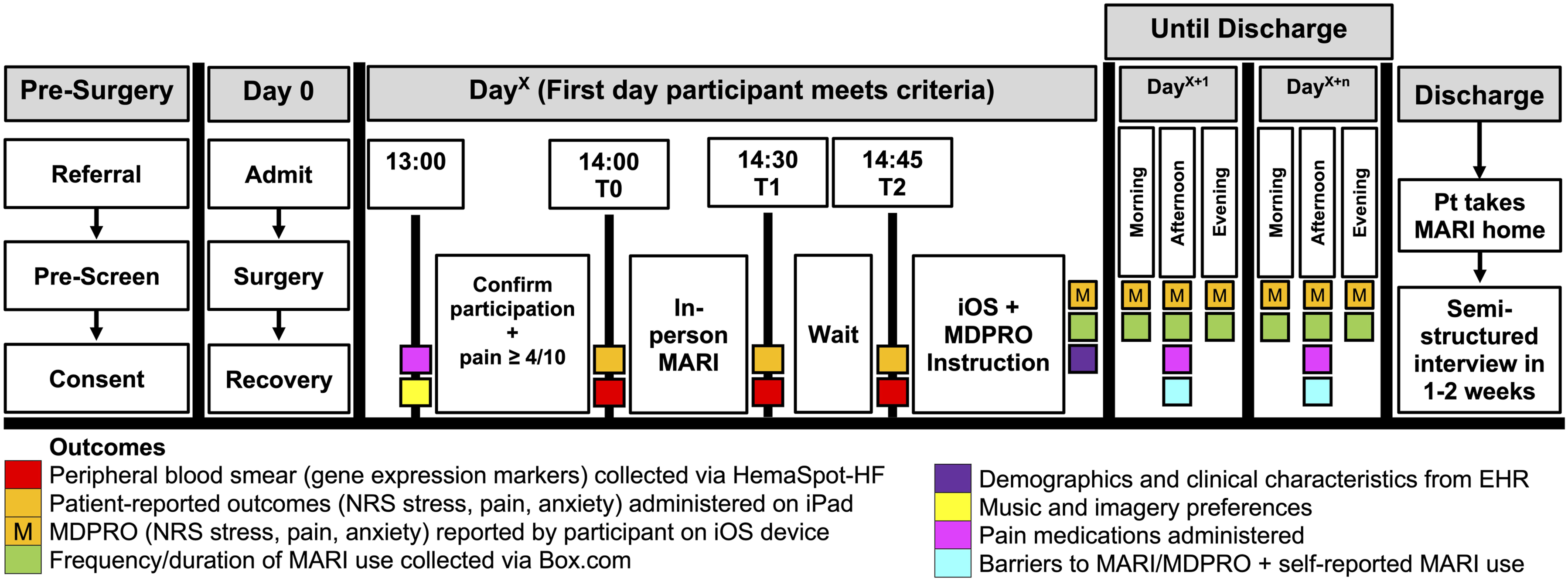
Participants
This study proceeded from February-December 2024 at a large Midwestern hospital. English-speaking patients 50-80 years old undergoing PD/DP were eligible if they rated their post-operative pain ≥4/10 on the numeric rating scale (NRS). Patients were excluded for significant visual impairment, hearing loss, or cognitive impairment. This study was approved by the University Hospitals Cleveland Medical Center Institutional Review Board (IRB) (STUDY20221489) and conducted in accordance with The Code of Ethics of the World Medical Association Declaration of Helsinki. This study was registered on ClinicalTrials.gov (NCT06123013).
Procedures
Screening and Enrollment
Patients were initially approached about the study during outpatient visits with their surgical teams. During these visits, a nurse provided basic study information, shared an IRB-approved flyer, and asked patients if they would like to be contacted by the research team to learn more about the study. If patients were interested in learning more, the surgical team then emailed the research team to provide patients’ medical record numbers and upcoming dates for pre-admission testing (PAT) and surgery. Following a referral from patients’ surgical teams, study staff reviewed electronic health records (EHR) to confirm initial eligibility. Patients meeting initial criteria were approached via phone call. If interested, patients were enrolled virtually or in-person at their PAT visit.
Day of Surgery
Surgical procedures for PD/DP followed an Enhanced Recovery After Surgery (ERAS) protocol that included providing sufficient nutritional support, managing pain while minimizing opioid exposure, ensuring appropriate fluid management and hydration, and promoting early post-operative mobilization. 15
T0
On post-operative day 1 (POD1), participants were approached in the early afternoon to verify continued willingness to participate and eligibility (not in intensive care, pain ≥4/10). If participants were too overwhelmed or rating their pain <4/10, they could participate the next business day. At 14:00 (T0), baseline NRS measures were collected using a Research Electronic Data Capture (REDCap) instrument on an iPad. 16 DBS samples were collected using a lancet and a HemaSpot-HF, 17 a less invasive means of collecting capillary blood.
MARI Intervention
Following T0, the MT-BC delivered a standardized MARI intervention featuring live guitar accompaniment personalized to participants’ music preferences and a standardized script (see Supplemental Material) directing participants to release tension, take deep breaths, and explore a relaxing place. Prior to the intervention, the MT-BC verified that the music and imagery preferences the participant reported at the time of recruitment were appropriate to use for the upcoming MARI intervention. During the intervention (median length 9.32 min), the MT-BC first invited the participant to find a comfortable position in their chair or bed and take a few deep breaths in through the nose and out through the mouth. Then, with soft acoustic-electric guitar accompaniment adapted to align with the participant’s preferred genre(s), artist(s), and/or song(s), the MT-BC proceeded to verbally guide the participant to imagine a place where they felt at peace. The script encouraged participants to notice the sights, smells, sounds, and textures of this place and concluded with the MT-BC improvising a few lines of sung lyrics about the participant’s peaceful place. For example, the MT-BC improvised the following lines for one participant who preferred music by Bob Seger and chose being on the road riding a motorcycle as a peaceful place, “Now I just want to hit the open road. Me and my buddies yeah we just go. Two wheels going down to the Keys I know. Just want to hit that open road.”
Following this section, the MT-BC invited the participant to imagine a healing energy from that place moving through their body and relieving any tension. The intervention then concluded with a countdown from 5 to 1 to gradually bring the participant back to the present moment. The live MARI was simultaneously recorded within GarageBand using a portable studio. Following MARI, the MT-BC briefly processed participants’ experiences by asking them how they felt after MARI. The MARI recording was then exported to a Box.com folder that the participant could access using their chosen device.
T1-T2
Post-intervention NRS ratings and DBS samples were collected again at 14:30 (T1) and 14:45 (T2). Procedures for MARI listening and completing MDPROs 3 times/day until discharge were reviewed with participants. If borrowed from the research team, iOS devices were locked to participants’ tray tables to prevent being lost or stolen.
Procedures Until Discharge
Research assistants met with participants every weekday to troubleshoot and collect data on any participation barriers (eg, forgot, technical difficulties). Participants received three notifications/day to complete MDPROs. MARI recording use was tracked using Box.com file utilization measures.
Following Discharge
Upon discharge, iOS devices were retrieved, and MARI recordings were sent to participants via email for use post-discharge. Semi-structured interviews were completed over Zoom 1-2 weeks post-discharge. $25 gift cards were provided following interview completion.
Measures and Data Collection
Baseline demographics and clinical characteristics were extracted from the EHR. Patient-reported measures of pain, stress, and anxiety were assessed using the NRS, a validated and widely-used measure for acute pain intensity18,19 that has also been used to measure anxiety in observational studies of integrative medicine20-23 and stress in an RCT 24 and clinical effectiveness studies of MT. 22 NRS measures were collected at T0, T1, and T2 via an iPad-administered REDCap survey. All subsequent NRS measures were acquired either via a link on the study iPod or a link texted to participants’ devices. Oral, intravenous, and patient-controlled analgesia opioid medication data were extracted from the EHR and converted to oral morphine equivalents using guidance from McPherson. 25
Feasibility
Rates of recruitment, retention, MARI completion, DBS collection, MDPRO completion, and MARI listening were collected to evaluate feasibility. A running log was kept to document study challenges. These were reviewed in bi-weekly meetings, and modifications were made to the study protocol as deemed necessary.
Acceptability
Feasibility and acceptability were further assessed using semi-structured interviews. Interview guides included prompts for describing post-surgical pain, attitudes toward and perceptions of MT, and experiences with DBS collection, in-person MARI, MARI recording, and MDPROs.
Data Analysis
Descriptive statistics and boxplots were used to summarize demographics and clinical characteristics as well as feasibility measures including rates of enrollment, retention, intervention participation, MARI-recording use, DBS collection, and MDPRO completion. DBS collection feasibility was determined by quantifying whether enough blood was provided to fill the HemaSpot-HF. No formal hypothesis tests were conducted on changes in NRS data as this was a feasibility study. 26 Descriptive statistics, tables, and figures were generated using R Version 4.4.2 27 and RStudio Version 2024.09.1 + 394. 28
The second and senior authors independently analyzed interviews using conventional qualitative content analysis and NVivo software. Each transcript was reviewed line-by-line and independently coded using a constant, comparative method of qualitative data analysis. 29 All data from interviews that appeared directly related to study aims were extracted. Coded data were then organized into categories to identify themes. Findings from authors’ independent analyses were consolidated and presented to the study team. Finally, research team members reviewed findings for accuracy of generated themes, interpretations of data, and conclusions.
Results
Demographics and Clinical Characteristics
Supplemental Table 1 describes the demographics of the five participants. Median age was 61 years [range: 52-76], with 3 (60%) participants identifying as female and all 5 (100%) identifying as non-Hispanic white. Three (60%) participants were married or with a life partner, three (60%) underwent DP, and four (80%) had a mental health diagnosis. The median (interquartile range [IQR]) of mean oral morphine milligram equivalents (MME)/day administered over participants’ admissions was 36.48 (22.00-51.53).
Feasibility
Feasibility Measures

Abbreviations: DBS, dried blood spot; MARI, music-assisted relaxation and imagery; MDPRO, mobile device patient-reported outcomes; NRS, numeric rating scale.

CONSORT Diagram. Abbreviations: MARI, Music-Assisted Relaxation and Imagery; NRS, Numeric Rating Scale
Challenges and Solutions

The median MT session length was 20 min (range 17-25 min) and included a brief assessment, the MARI intervention (median 9.32 min), and a brief evaluation. No interruptions or adverse events were reported. Across participants, the median (IQR) listens to MARI over the hospital admission was 5 (3-7), which made up 50% (40-60) of total admitted days.
Regarding data collection, the overall median of total MDPROs completed per participant was 5 (3-6). This was higher (8.5 [6-11]) among the two participants who used their personal device compared to those who used the study iPod (3 [1-5]). DBS sampling success was variable with a success rate of 9/15 (60%) across all sampling attempts. Notably, one T2 NRS and DBS sampling procedure did not occur because the participant fell asleep. Changes in NRS measures of pain, stress, and anxiety from T0-T2 are visualized in Figure 3. Between T0-T1, participants reported reductions (mean ± SD) in pain (−1.60 ± 1.52), stress (−2.40 ± 0.89), and anxiety (−1.75 ± 0.96). Boxplots of Pain, Stress, and Anxiety Measures From T0 to T2. Abbreviations: NRS, Numeric Rating Scale. Diamonds Represent Mean Values. The Orange Horizontal Line Represents the Threshold for Moderate Symptomology at NRS = 4/10. The Red Horizontal Line Represents the Threshold for Severe Symptomology at NRS = 7/10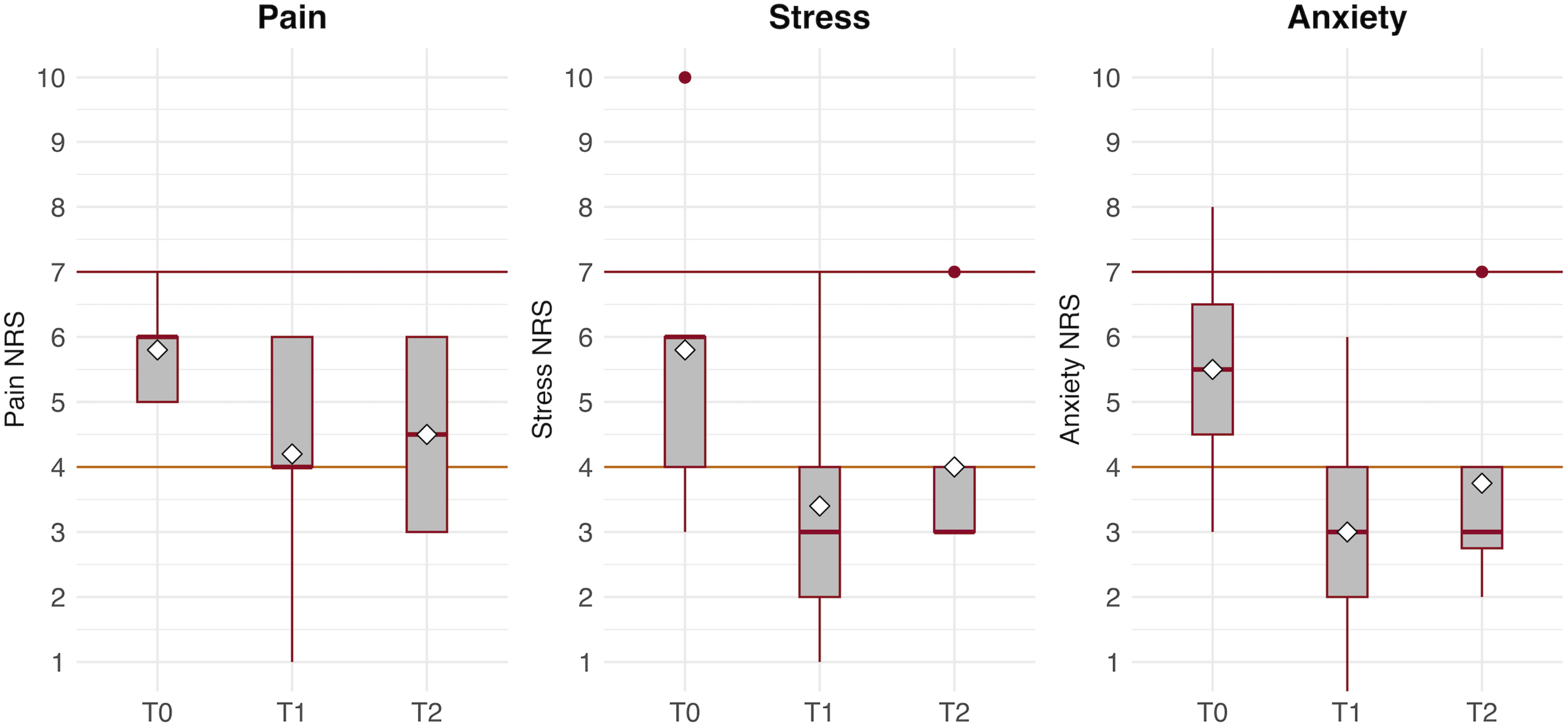
Acceptability
Qualitative data supported intervention acceptability and revealed opportunities for improvement with three emerging themes: (1) MARI was beneficial and useful throughout surgical recovery; (2) the live MARI intervention should be longer; and (3) need to improve blood sampling and mobile-device procedures.
Theme 1: MARI was Beneficial and Useful Throughout Surgical Recovery
Participants described MARI interventions as enjoyable, novel, and a break from typical hospital staff or stress. “It wiped everything out of me and made me lay back and let everything go.” “It’s different. That was, like I said, new, but it was pretty good. He asked me some questions and made up the song… he kind of used my motorcycle-riding and stuff like that in it. Like I said, I thought it was gonna be just him playing music or something. It was surprising that he sang a song and stuff like that, but, yeah, it was fine…it just surprised me, but it was different and I liked it.” “It just made me a little bit more of a patient person…I remember there was one day, I started counting the visits, and by about lunchtime, I had had 42 visits from various staff during the day, and that was one of the things, that the pain would get to me, because I knew I could never simply lay back and expect and hour of peace and quiet… [MARI] made me a little more peaceful, I guess is the simplest way I can put it…it kind of slowed down what was going on inside me.”
All interviewees confirmed that their MARI intervention aligned with their preferences. Although not a study requirement, some participants reported using MARI recordings post-discharge: “This morning I got up and it was probably the worst I’ve felt in the time since I have got home, so I added this back into my little things I do in the morning.” “It was easier simply on my phone to sit the phone right next to me, you know, and listen to it. One of the things I never thought I’d say, but even it brought back nice memories of my time in the hospital.”
Theme 2: MARI Should be Longer
Though maximum MT intervention time was described as 30 min in the consent form, in practice, the MARI intervention itself was around 9.32 min. One participant expressed frustration with this discrepancy. “I found the music therapy experience disappointing and frustrating because they had said that it was going to be 30 min of music, and it was only like seven minutes of music…It was too short.”
Another participant described how intervention brevity prevented them from having a longer relaxation experience. “Well, for me, he could’ve just kept on playing...I mean maybe about 15 min longer (and it seems like you just got into the relaxation and then you’re being pulled back out of it) would’ve been nice.”
Theme 3: Need to Improve Blood Sampling and Mobile-Device Procedures
Though participants described low discomfort with DBS procedures, one discussed how its unreliability caused frustration. “The girl who was administering the study…had problems with the finger stick, which they did multiple times and it was more frustrating than helpful… The finger prick is nothing, pain wise. It just seemed incompetent”
Participants described MDPRO collection frequency as acceptable, with one even expressing appreciation for being able to express how they were feeling. “Ooh, actually I wish more people would’ve asked me how I was feeling.’ It actually was very, very helpful and kept me paying attention to how I was feeling.”
Several participants expressed frustration with the study iPod’s poor user interface, with one describing how it prevented them from accessing the recording. “One day I was so sick…and I couldn’t find it to save my life. I didn’t listen to it. I think that would’ve calmed me enough, a couple of times listening to it during the day,’ but I said, ‘There’s got to be an easier way…you give this to an 85-year-old person, it’s not gonna happen.’”
This participant suggested that investigators allow future participants to use their own devices. “If you just show them and they have a little icon on there or a telephone where they could just push it themselves, they would know, or, like I said, family members, and they could push it for their loved one. It would help make it a lot easier for them.’”
Discussion
This study assessed feasibility and acceptability of administering a tailored MARI intervention, collecting MDPROs, and collecting DBS samples post-PD/DP. Despite a small sample and recruitment challenges, lessons learned can inform future research. When the study began, two participants were subsequently withdrawn due to either reporting pain intensity <4/10 or being too overwhelmed to participate in POD1 activities. Therefore, the study protocol was amended to enable approaching the participant on another day if on POD1 the participant rated their pain <4/10, indicated their pain was too high to participate, or was unable to rate their pain due to cognitive/physical limitations. Following the first successful MARI and DBS collection, additional modifications were made to improve mobile device procedures. The pre-surgical visit protocol was updated so that participants were asked about their music and imagery preferences, given the choice of using their own device or a study iPod for study procedures, and educated on how to listen to MARI and rate MDPROs.
Our sample was similar to prior PD/DP investigations. All participants received opioids throughout their admission (median 5 days), consistent with prior DP studies. 30 Unlike a 2023 analysis of 1305 patients undergoing pancreatic surgery where 16% had a pre-existing mood disorder, 31 most (80%) participants in this study had such diagnoses. Addressing patients’ mental health concerns are important given their contributions to increased risk of 90-day readmission (42% vs 31%, P = .001) within this population. 31
While prior studies involving mobile-device administered integrative modalities featured high recruitment rates among post-surgical populations, such as one Icelandic feasibility study boasting a 93.75% recruitment rate (105/112), 32 our recruitment rates were not as high as initially planned. This was due to factors including: (1) patients withdrawing after surgery due to feeling overwhelmed or not reporting sufficient pain; (2) recruiting solely from a population undergoing two rare procedures from a small number of surgeons; and (3) scheduling conflicts. For example, several patients had Friday surgeries when staff were unavailable on weekends for POD1. Future studies may benefit from recruiting patients undergoing a broader set of surgical procedures and either limiting recruitment to only those surgeries early in the week or budgeting for weekend staff.
All live MARI sessions were completed, and all participants listened to MARI recordings ≥1 time before discharge. One innovation was using file tracking capabilities within Box.com, a cloud-based storage solution, to track recording utilization during hospitalization. Such procedures could be useful for measuring adherence to other post-surgical mind-body interventions. Participants reported enjoying the intervention and listening to it even after discharge. Interestingly, qualitative analysis revealed a desire for longer MARI interventions. Thus, future research should consider longer in-person MARI or combining it with other music interventions (eg, preferred music, breathing exercises) to extend the potential benefits of the intervention. 33 Given limited MT capacity within hospitals, recording a personalized MT intervention within an initial live session and administering recordings thereafter may help scale MT interventions to reach more patients. This kind of service delivery model could potentially (1) be more cost-effective for hospitals than having MT-BCs provide daily in-person sessions following surgery, and (2) help MT-BCs target their in-person session time toward patients with more challenging psychosocial needs. Immediate reduction in NRS measures from T0-T1 was consistent with prior MT studies among patients with hematologic/oncologic 34 conditions, community hospital inpatients, 35 and inpatients receiving MARI within palliative care. 5 Overall, our quantitative NRS changes were consistent with qualitative findings that MARI was beneficial for postoperative pain. Our data provide early evidence for MARI’s use as a post-surgical symptom management tool with this population. However, more research is needed to test scalability and effectiveness.
Our results support MDPRO collection feasibility, particularly when administered on participants’ own devices. Participants appreciated the opportunity to rate how they were feeling. Notably, the first participants mentioned challenges with using the study team’s iPod. This device presented several user interface challenges that likely hindered early MDPRO collection. These included the device being (1) smaller than a typical smartphone and thus harder to navigate; (2) configured by the health system to only use a slow restricted browser; (3) housed within a rubberized case that hindered the interface; and (4) locked to participants’ tray tables. Thus, researchers seeking to measure acute post-surgical symptoms longitudinally must pay careful attention to the user interface.
Despite initial expectations that DBS procedures would be less invasive and thus more feasible, they presented several challenges. The 60% blood sample collection rate found utilizing HemaSpot-HF is too unreliable for use in future research seeking to examine gene expression mechanisms by which MT affects pain. While qualitative data revealed this is a low-discomfort procedure, inconsistent blood collection can be frustrating for participants and adversely affect patient experience. More importantly, DBS are generally not preferred for gene expression analysis since prolonged storage contributes to DNA degradation. 36 Further, lancet blood collection may not be a good option due to post-surgical anemia. 37 Future studies should consider a more reliable blood sampling tool such as PAXgene tubes.
Study limitations included small sample size, which limited our understanding of feasibility within PD/DP. All study procedures were carried out at a single site, a National Cancer Institute-Designated Comprehensive Cancer Center. Thus, generalizability to other sites may be limited. Without a comparison group, our findings do not inform retention or data collection rates that may be expected in an RCT. Study strengths included partnering with MT-BCs to deliver interventions within the real-world hospital setting, novel use of music technology to provide MARI recordings and measure their use during hospitalization, and the nuanced understanding provided through integrating quantitative and qualitative data.
Conclusion
Preliminary findings support the feasibility and acceptability of a live MARI intervention, continued use of MARI recordings over the course of hospitalization, and MDPRO collection among adults recovering from PD/DP. However, design modifications are needed to improve blood sample collection. This study provides valuable data for study procedures in future RCTs, where investigators should consider expanding eligibility beyond PD/DP to increase recruitment rates, ensuring staff availability throughout the week, extending the MARI intervention, and using a more robust blood collection procedure than the DBS.
Supplemental Material
Supplemental Material - Music Therapy in Patients Undergoing Pancreatic Surgery (MUSIC PUPS): A Mixed Methods Pilot Study
Supplemental Material for Music Therapy in Patients Undergoing Pancreatic Surgery (MUSIC PUPS): A Mixed Methods Pilot Study by Kayleigh Risser, Seneca Block, Jessica Surdam, Haitong Yu, Susan J. Doh, Slate Bretz, Richard S. Hoehn, Samuel N. Rodgers-Melnick in Global Advances in Integrative Medicine and Health
Footnotes
Acknowledgments
We thank the individuals who participated in this study. We would also like to thank the team members who made this study possible including: (1) study coordinators Hayley Sluka, BSN, RN; Aja Patterson; Kathryn DiFrancesco, BA, ACRP-CP; and Tracy L. Segall, MSHS; (2) music therapist Hope Ezell, LPMT, MT-BC; (3) transcriptionist Tracey L. Baker; (4) laboratory storage aid from Sarah Scott; (5) study design recommendations from Jeffery A. Dusek, PhD and Manoj K. Bhasin, PhD, MS; and (6) the pancreatic surgery team of Christina Seafler; Jordan Winter, MD; and Lauren McCaulley. We especially appreciate the support of the Smith Foundation.
Ethical Considerations
This study was approved by the University Hospitals Cleveland Medical Center Institutional Review Board (STUDY20221489) and conducted in accordance with The Code of Ethics of the World Medical Association Declaration of Helsinki.
Consent to Participate
Participants gave written consent before entering study procedures.
Consent for Publication
Informed consent for publication was provided by the participants during consenting procedures.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the GRAMMY Foundation and the Smith Foundation. Neither foundation had any role in the study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication. The REDCap platform at University Hospitals is supported by the Clinical and Translational Science Collaborative of Northern Ohio (UM1TR004528).
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Trial Registration
This study was registered on ClinicalTrials.gov (NCT06123013).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.