
Abstract
Background
Posttraumatic stress disorder (PTSD) has higher prevalence in safety net settings, which also face structural barriers to the use of gold-standard, exposure-focused treatments. Somatic therapies (STs) are used to treat PTSD with a focus on sensations. STs may be a culturally relevant option not requiring exposure. They have not been rigorously studied.
Objective
Assess the acceptability of ST for patients with PTSD and staff in a safety net setting.
Methods
We conducted a qualitative study with interviews of patients and staff in a general internal medicine clinic within an urban safety net health system. Patients were eligible if they were seen between October 1st, 2022 and October 31st, 2023, had PTSD in their chart, had one past trauma-related visit with any psychotherapist, and were English-speaking. Staff were eligible if working in a patient-facing role for 6 months in primary care or integrated behavioral health. Transcripts were analyzed using the Consensual Qualitative Research approach.
Results
The 14 patients interviewed were diverse in terms of race and traumatic exposures, and most had a chronic pain condition. Childhood sexual abuse was the most common traumatic exposure disclosed. Analysis yielded five major themes: the somatic experience of PTSD, patient perspectives on exposure-based therapy, past experiences with mind and body practices, patient mind and body beliefs, and acceptability of ST. ST was congruent with many patients’ lived experiences and their beliefs about mental health. Challenges faced in seeking care for PTSD, including negative past therapy experiences and poor access, promoted openness to ST.
Conclusion
Patients with PTSD and staff found ST acceptable. Further work is needed to develop somatic interventions for PTSD.
Introduction
Posttraumatic stress disorder (PTSD) prevalence in the United States ranges from 4.7% to 6.1% in the general population. 1 PTSD prevalence in safety net care settings is as high as 23%, 2 and it is associated with increased all-cause mortality.3,4
Evidence-based treatments (EBTs) for PTSD include medications and psychotherapy, particularly cognitive processing therapy (CPT) and prolonged exposure (PE).5,6 CPT and PE are associated with moderate reductions in PTSD symptoms when patient successfully receive an adequate number of sessions, typically eight. 7 CPT and PE may not be compatible with safety net settings which face workforce shortages and may lack the necessary resources.8,9 People of color are seen disproportionately at safety net institutions, yet are underrepresented in the literature on these EBTs. 10 The minority stress model suggests that increased exposure to violence or trauma in this setting makes this omission particularly grave. 11 Exposure therapies are also not tolerated by all persons with PTSD, 12 and avoidance of traumatic memories is a barrier to therapy. 13 Since these are the principle EBTs in addition to medications, a large focus of health services research in PTSD is to improve implementation and uptake.14,15 Somatic therapy (ST) may be a treatment option for patients who do not tolerate exposure-based treatments, or those whose most debilitating PTSD symptoms are somatic symptoms, since STs engage somatic symptoms and other sensory experiences.
STs are a subcategory of mind and body therapies used to treat trauma and PTSD. Their true uptake, efficacy, and acceptability have not been thoroughly or rigorously studied, and there are few mentions of them in peer-reviewed literature. However, media accounts describe STs as increasingly popular. 16 STs emphasize interoception (sensing and interpreting signals from within the body), proprioception (sensing and interpreting body position), and kinesthesis (sensing and interpreting body movement). They include sensorimotor psychotherapy 17 and Somatic Experiencing® (SE™). 18 While cognitive behavioral approaches to trauma treatment aim to modify “automatic thoughts” and underlying beliefs, 19 somatic therapists support patients to “track” pleasant and unpleasant sensations within their window of tolerance. Those sensations are the primary entry point for intervention, and the practitioner helps the patient to actively notice them (ie, interoception) before engaging the meaning or emotions which may be attached to the sensations. 17 STs also frequently incorporate practices seen in other mind and body practices such as visualization, mindful noticing of one’s environment, active grieving, or supportive grounding exercises or “resources.”
Some have argued that somatic therapy can “fill a gap” in the treatment landscape. 18 However, research on somatic therapies and the integration of somatic approaches into other forms of therapy is relatively sparse, and there is no consensus on which therapy practices fall in this category. We know of no studies of the acceptability of STs.
Our aim for this study was to understand the acceptability of STs for PTSD delivered in primary care. We conducted a qualitative study of a diverse group of patients with PTSD and clinical staff at a large safety net primary care clinic.
Methods
Setting
This study was conducted in a General Internal Medicine (GIM) clinic within Boston Medical Center (BMC), a large safety net health system. The clinic features colocation of a broad interdisciplinary clinical team who provide comprehensive adult primary care. Integrated Behavioral Health (IBH) is a service which integrates psychiatry, psychology, and clinical social work into clinic operations. The majority of patients are low-income and on Medicaid, and the population is racially and ethnically diverse. Patients behavioral health needs are high: many face complex psychosocial stressors. Clinical data has shown that 23% of BMC GIM patients meet criteria for PTSD. 2 This research was approved by the Boston Medical Center and Boston University Medical Campus Institutional Review Board.
Participants and Recruitment
Participants were patients receiving primary care at GIM from October 1st, 2022 to October 31st, 2023 and GIM staff. Patient participants met the following eligibility criteria: (1) had a primary care appointment at GIM during the above period, (2) had at least one past visit with a psychologist, psychiatrist, or other behavioral health clinician for PTSD or trauma treatment, (3) were English-speaking, and (4) were 18 years of age or older. A list of potentially eligible patient participants was generated from electronic health records. Patient participants were recruited through an opt-out letter or by telephone recruitment conducted by the first author. Additional recruitment letters were sent to younger patients and Hispanic patients, who were initially underrepresented among patients who consented. Staff participants met the following eligibility criteria: (1) providing care to patients in GIM for at least 6 months, and (2) practicing in GIM, Integrated Behavioral Health (IBH), or Psychiatry. Staff participants were recruited through email listservs.
Research Team
The research team included an internal medicine physician with training in SE™, a type of ST (Author 1), a psychologist specializing in trauma therapy (Author 2), and an internal medicine physician with expertise in the implementation of mind and body therapies in primary care (Author 3). Interviews were conducted by A1, data analysis and interpretation were completed by A1 and A2. All team members provide care to the population from which patient participants were recruited, but not to the specific participants.
Interviews
Qualitative interviews occurred between June 1st and August 31st, 2023 and were conducted by A1. Interviews were conducted and audio recorded using HIPAA compliant and encrypted Zoom software. Participants decided whether to be on camera, no personal identifiers were recorded, and transcripts were de-identified for analysis. Transcripts were saved on a HIPAA compliant and encrypted server only accessible to the study team. Patient interviews lasted approximately 1 h. The 18-question interview guide elicited patient’s past experiences with trauma therapy, physical PTSD symptoms, beliefs about the relationship between mind and body, exposure to mind and body practices, and their responses to a short description of ST (Supplement 1). Staff Interviews were conducted in 90-minute focus groups with three to five participants. The 27-question staff interview guide focused on their experiences diagnosing and treating PTSD, physical symptoms of PTSD, and patient experiences with psychotherapy (Supplement 2). It included the same description of ST presented to patients.
Data Analysis
Preliminary analysis followed rapid coding procedure 20 consistent with conventional content analysis where data is continuously compared throughout the data collection process. 21 The team met regularly to construct themes and reach consensus on prototype subthemes and domains, iteratively returning to transcripts in order to resolve discrepancies. The conduct of interviews and the analysis were conducted according to the principles of Consensual Qualitative Research (CQR). CQR is a phenomenological approach commonly used in the psychology literature, 22 and is well suited to the study’s focus on inner experiences, attitudes, and beliefs. While interviews guides helped achieve a degree of uniformity across interviews, CQR views the co-creation of meaning between the researcher and participant as a natural and inevitable aspect of qualitative research. Richness of data is achieved through probing follow up questions which invite participants to describe their inner experience. Saturation was defined on the basis of novel codes generated. Data collection stopped when no new information for a theme was identified. 23 We used NVivo Version 1.7.1 for analysis. Patient and staff interviews were analyzed separately. The study was conducted following the Standards for Reporting Qualitative Research. 24 (Supplement 3)
Results
Patients
Patient Participant Characteristics

IQR, interquartile range; COPC, chronic overlapping pain condition.
Analysis of patient interviews yielded five major themes: the somatic experience of PTSD, patient perspectives on exposure-based therapy, past experiences with mind and body practices, patient mind and body beliefs, and acceptability of ST. (Figure 1) Conceptual Model for the Acceptability of Somatic Therapy for Patients With PTSD
The Somatic Experience of PTSD
Thirteen of 14 participants described responses to trauma-related triggers or perceived threats in terms of their somatic symptoms. Among these, six emphasized symptoms related to the “fight or flight” response and autonomic pathophysiology, such as palpitations, diaphoresis, or dizziness 26 : “I’ll start sweating really heavy and I’m dizzy and […] It usually comes on like a smell, something that I smell, just all of a sudden brings me back to that place.”
Patients also described the body as a site for emotional states, often using images or other metaphors to do so. One patient described a somatic response to a trauma-related trigger including tears and physical arousal: “All [my friend] knew was I started crying, and then I explained it to her...I held it in for over 40 years, you know. So, that’s what triggered it, and then I had to tell her what happened. I was ready to go on a warpath. I was ready to fight.”
Two patients described their somatic symptoms as the most severe and distressing manifestations of their PTSD. One tied his somatic symptoms directly to a body-based trauma narrative: “That [trauma] lived with me my whole childhood. The nightmares, the sleep, the worry about my parents, the fear of them dying.”
Patients also expressed various ideas about the relationship between their experiences of physical pain and trauma-related stress. Stress was commonly experienced as a factor exacerbating pain, but one patient described an inverse relationship in which anger-related “adrenaline” desensitized her to pain: “When I calm down, that’s when I feel all the pain.” Patient beliefs about PTSD and pain are further discussed below.
Patient Perspectives on Exposure-Based Therapy
Most participants believed that revisitation of traumatic memories is important and worthwhile. Many also described challenges associated with it, such as this patient’s experience with written exposure therapy: “I wrote down, like about three pages of stuff that I could think about and all that came back to me and that was pretty difficult to do.” This patient rarely engaged with such intense exposures, even though it was an important experience for him. Another patient described a sense of empowerment related to group therapy involving exposure: “...After [group therapy], I didn’t care, because I want my story to be heard, because I felt like, after that, I could help somebody.”
Two patients felt very strongly that exposure-based therapy is not for everyone. One patient was overwhelmed by current and ongoing stressors. His goal for therapy was to manage current stressors rather than past traumas: “What I think what I find is helpful is - what’s on my mind right now. Where am I right now?” Another patient described her desire not to engage with the trauma memory: “I know the act in and of itself was bad, but there’s something else there and I don’t want to remember. I don’t need to because I know how I felt. So I don’t want to go there…”
Domain 3 – Past Experience With Mind and Body Practices
While most participants had no formal experience with ST, they were exposed to components of it in other contexts. Participants had experiences with tai chi, reiki, Buddhist chanting, breathing exercises, mindfulness, meditation, spiritual direction, and massage. Some patients engaged in these activities for general wellness, while in others cases, they were recommended or performed by a psychotherapist, or independently pursued to address trauma symptoms. One participant described an experience with reiki performed by a therapist as a transformative form of sensation-based exposure therapy: “It actually brought me to actually remember the smell, remember the feel of what took place.” It left him “feeling better.” Similarly, one patient who engaged in (longstanding spiritual direction practice) felt that the description of ST provided resonated strongly with her positive experiences in spiritual direction, which she found after many negative and stigmatizing experiences in therapy and healthcare more broadly. She describes how this practice helped her attune to and manage the embodied rather than cognitive aspects of trauma and PTSD:
“I’ve always thought about this thing about ‘the feeling,’ how the body feels. I know that when I start getting really depressed, my body just feels so heavy and when I start getting that heaviness, I know that this is the beginning of something. And so I’ve learned now it’s like not run to shop -- not go do anything else but to sit with it and let it come forth and now with the groups that I have, I know which person that I wanted to have like a really more intense conversation who, amongst the people that I’m with that I can call on.”
She went on to describe the de-emphasis on cognitive processes: “The [spiritual direction approach] is of a spiritual nature more than an intellectual [approach].” Though participants had substantial exposure to mind and body practices outside the healthcare system, many (7) participants said their psychotherapy was always “talk therapy.” These experiences were generally described in positive terms, but rarely incorporated mind and body practices. One participant underlined this distinction after hearing about the theory of ST: “See, everything else feels like talk, talk, talk, and talk, talk, talk, talk.” She believed that ST would be effective for her: “I think that it would be [effective for me], because what’s going on right now ain’t doing nothing.”
Domain 4 – Patient Mind and Body Beliefs
Patient beliefs about the mind and body had many different influences. A prominent influence was the experience of PTSD and pain, including the dismissal of pain complaints by medical professionals. A participant with a history of pelvic inflammatory disease said her pain was initially misdiagnosed as “psychosomatic” pain: “[…] as a Black woman going in for medical treatment it’s like, ‘It’s all in your head.’”
For some patients, their pain symptoms were a separate matter from their PTSD, and stated so explicitly: “Yeah, the pain is physical. The PTSD is emotional.” For other patients, PTSD, stress, and pain were connected:
“Because when I’m upset and I’m crying and I’m going back thinking about all the, the tragedies and things that I’ve been through and stuff, it has my blood pressure high. I have inflammation in my body. I have osteoarthritis so the inflammation goes in my body. My knee swells up, my hand swells up. I had two surgeries on both of my hands. I had carpel tunnel and arthritis surgery. So everything affected my physical. Whatever was going on in my brain, it was affecting, definitely affecting my physical.”
The majority of patients articulated some belief that PTSD affects both the mind and the body, and that their illness experiences reflect this. These beliefs often translated into a belief in the effectiveness of mind and body interventions generally, and interest in ST specifically. This was one patient’s immediate response to the description of ST:
“It [ST] is giving words to what it is that I’ve been thinking and feeling and trying to understand… I know that there’s so many people that will not go in for talk therapy, for psychotherapy, for psychoanalysis. I know that they will not and it’s how I deal with people a lot is to really talk with them about what they’re feeling...because I make that distinction...between -- ‘I feel happy,’ and feeling like ‘I’m feeling like inside, something just not right.’ Those are two different ‘feelings’ to me and this [ST] sounds like it is something that can make that distinction.”
Domain 5 – Acceptability of Somatic Therapy
All participants were open to trying ST, but with varying degrees of enthusiasm. Some were eager to try it, while others expressed openness to new therapies in general. One participant’s openness to trying an unfamiliar therapy was tied to a sense of desperation, having tried many medications and therapies: “I think some of it [ST] could help...Sometimes I just want to feel better and sometimes a lot of the things that I have tried, they don’t work and I get frustrated because it’s been so long...I don’t want to just feel good just for the day, the next couple of days. I want to kind of find something that works for me without having bad thoughts or feelings.” Two participants with relatively muted interest became more enthusiastic with follow up discussion – this included additional information about the neurobiology of trauma, and examples of questions a somatic therapist might ask to elicit therapeutic interoception.
Staff
Staff participants in 3 focus groups included 2 medical assistants, 2 general internists, 1 family nurse practitioner, 1 nurse, 1 patient navigator, 1 clinical pharmacist, 1 clinical social worker, 2 psychiatrists, and 1 clinical psychologist. Analysis of staff interviews yielded 4 major themes: staff perspectives on available PTSD treatments, staff experiences treating trauma and PTSD, structural challenges to PTSD treatment, and staff perspectives on ST. (Figure 2) Conceptual Model for Clinical Staff Perspectives on Somatic Therapy for PTSD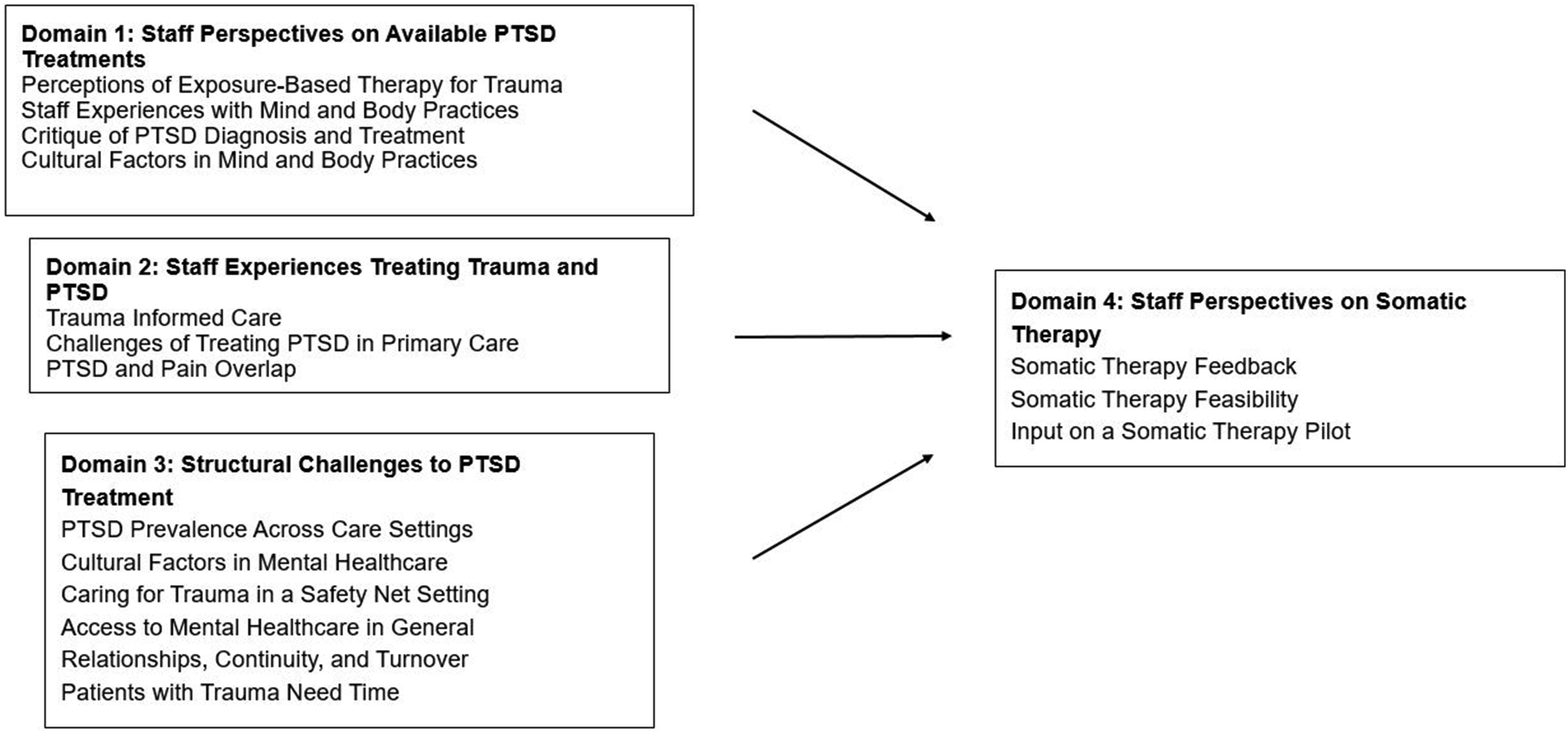
Domain 1 – Staff Perspectives on Available PTSD Treatments
Staff participants across social work, psychiatry, and psychology disciplines used a variety of techniques in their therapy practice. While they incorporate some mindfulness techniques, they reported an emphasis on cognitive therapy in their training: “[I’m] primarily psychodynamically trained. And then we all learn CBT in a formal sense.” However, these practitioners viewed ST and exposure-based therapy as not mutually exclusive, stating that the body is often a site of trauma: “Exposure to just feeling their body again and in a slow careful way and experiencing their body again.”
IBH providers shared a critical view of PTSD as a diagnostic category, citing its creation as a byproduct of the Vietnam War, its limited applicability for patients “in an environment of chronic trauma,” and the underdiagnosis of complex PTSD and other trauma-related syndromes. This was connected for some to a diagnostic approach for trauma accounting for a variety of psychological and somatic symptoms, rather than a “rigid diagnostic model” which may not reflect patient circumstances.
Multiple staff described how cultural and historical factors shape the use of mind and body interventions for trauma. In many cases this was related to cultural fit and stigma. For example, one internist argued that ST and other mind and body therapies resemble some Central American healing practices: “these are practices that are somewhat similar, they have other names.”
Domain 2 – Staff Experiences Treating Trauma and PTSD
Trauma informed care was an important concept for all participants. Medical assistants in particular described the importance of de-escalation and other aspects of trauma informed care - they are often the first staff bringing up mental health in a visit through routine screenings.
Staff across disciplines described primary care as a setting with opportunities and challenges in diagnosing and treating PTSD. The relationships built into primary care enable disclosure of traumatic experiences and access to appropriate services. Primary care providers and staff of ancillary services like clinical pharmacy consultations, the nursing triage line, and patient navigation had at times directed patients to IBH services. An IBH social worker said that this a common pathway by which trauma is initially disclosed prior to a PTSD diagnosis.
Many providers noted experience with patients with PTSD and comorbid chronic pain. Two primary care internists shared a strong sense that these patients suffered because their care for these conditions is fragmented: “The notes that I see, they’re like, ‘Oh, they’re doing well on their [psychiatric] medications, they’re fine.’ Nothing else to do. And every time they come to see me, it’s like, ‘I’m not doing well, I’m feeling very anxious, very depressed and my pain is worse.’”
Domain 3 – Structural Challenges to PTSD Treatment
The collection of clinical services offered by the psych department allowed for a nuanced discussion of PTSD presentation across care settings. Some providers suspected that PTSD is underdiagnosed in primary care. This was complicated by a sense that complex PTSD (which is part of the ICD11, but not the DSM-5) is a prevalent condition in this clinical environment. However, these distinctions are rarely made in primary care. The circumstances of diagnosis are further complicated by administrative barriers to social supports for vulnerable patients such as refugees. Staff thus shared a sense that the questions around PTSD epidemiology extend beyond the precision of prevalence estimates.
Stigma and other cultural factors created barriers for primary care providers in meeting the needs of the population they serve. Two providers described patients who were able to discuss trauma and related issues only with them because of trust built over years and additional effort by those clinicians. The unavailability of language concordant therapists was emphasized as a major hindrance to care: “I cannot imagine having therapy with an interpreter. I can’t imagine that. I know some people try to do that, but I think it’s just very hard. So my patients tell me, ‘If there’s no Spanish speaking therapist, just don’t refer me. I’m not going to have therapy with an interpreter.’” Many staff noted poor access to mental healthcare in general, suspecting that related harms are especially severe in the safety net setting.
All staff emphasized the importance of the therapeutic relationships, and felt it was particularly important not to rush conversations about PTSD. While continuity was felt to be important in both primary care and psychotherapy relationships, turnover of psychotherapists was brought up as a particularly common and severe hindrance to the care of PTSD patients.
Domain 4 – Staff Perspectives on Somatic Therapy
Staff generally were supportive of ST based on the description provided or, for some, their prior experience. One psychiatrist noted: “So often we’re overly cognitively oriented, and we don’t pay attention to emotional and physical states….I love the idea of doing therapy modalities that focus more on just paying attention to your body.” Others were drawn to the idea of therapy not requiring exposure, and also believed that ST could address some point of connection between trauma and chronic diseases, particularly chronic pain. The main concerns raised related to resources including time, staffing, and space – factors which constrain the care currently received by their PTSD patients.
Discussion
Patients with PTSD at a safety net primary care clinic with diverse trauma exposures described interlocked psychological and somatic symptoms of PTSD. Their beliefs about the mind and the body reflect these experiences and are expressed through their personal narratives. They actively seek a variety of treatments, and are generally open to trying ST. This is in part because they have faced stigma, long waitlists, therapist turnover, and at times, therapy which does not reflect their worldview or the full extent of their symptoms – previously documented phenomena.8-10 Multidisciplinary staff in this setting struggle to provide the best care to their patients with trauma, noting system-level limitations which correspond with local patient experiences and published literature. 13
McFarlane and Graham argue that PTSD is a somatic disorder and that somatic symptoms should be included in its diagnostic criteria. 27 In their latent class analysis of veterans with severe trauma symptoms, distinctions between three somatic symptom classes were predicted by lifetime trauma exposure, suggesting the possibility of different somatic phenotypes. The embrace of a mind and body perspective by patients with PTSD is well-aligned with this analysis.
ST may differ from traditional exposure-based therapies in two key ways: it does not require the retrieval of traumatic memories, and it stimulates the sensory nervous system, the site of somatic symptoms. Primary care clinicians noted significant limitations in the treatment of comorbid PTSD and chronic pain, which was common among the patients interviewed. Primary care settings with integrated behavioral health may be an ideal setting for developing and testing somatic or other mind and body interventions tailored for PTSD patients with a high burden of somatic symptoms or pain.
Patients with PTSD are diverse in terms of their exposure to trauma and its effects, and there is a substantial literature critiquing the limitations of EBTs given this diversity. 28 Improving the care of patients with PTSD will require both improved implementation and availability of current treatments and support for established and novel mind and body approaches. A key challenge to overcome in further translational research on STs is a lack of consensus on their key distinguishing features. Ogden et al 17 explicitly describe the procedures which distinguish the somatic approach of sensorimotor psychotherapy from cognitive and exposure-based approaches. However, mindfulness-based approaches, which are effective for PTSD, 29 and trauma-informed pain treatments such as emotional awareness and expression therapy30,31 may also have points of overlap. Patients with PTSD will benefit from further work to distinguish key components of these techniques and define clinical scenarios in which they are most beneficial. This will require piloting ST interventions using replicable protocols.
Our study has several limitations. We interviewed patients actively engaged in primary care and with identified PTSD – our findings may not apply to patients exposed to trauma with subclinical or undiagnosed PTSD or those not engaged in care. Refugees are a large proportion of the PTSD population, and they were not represented in our study. Interviews were only conducted in English. Finally, patients were asked for their thoughts on ST after learning about it, but not getting to experience it. There is a risk that patients would be biased in favor of the technique through the educational process. This was mitigated with a simple description of the relative lack of ST research. It was also mitigated by inviting and validating perspectives which don’t necessarily support its use, such as the perspective of the participant quoted above who described PTSD as strictly “emotional” and separate from their physical pain symptoms. Along with the CQR approach, this helped assure that a range of perspectives were elicited from the relatively small number of participants.
This study confirms that ST, and a mind and body approach to PTSD more broadly, is acceptable and perhaps culturally relevant to diverse patients with PTSD in an urban safety net setting. Findings encourage broader interdisciplinary efforts to characterize the burden of somatic symptoms and chronic pain among patients with PTSD, define testable somatic interventions, and measure their efficacy in PTSD.
Supplemental Material
Supplemental Material - The Acceptability of Somatic Therapy for PTSD Among Patients at an Urban Safety Net Primary Care Clinic
Supplemental Material for The Acceptability of Somatic Therapy for PTSD Among Patients at an Urban Safety Net Primary Care Clinic by Karim Sariahmed, Nuha Alshabani, and Natalia Morone in Global Advances in Integrative Medicine and Health.
Footnotes
Ethical Considerations
This research was approved by the Boston Medical Center and Boston University Medical Campus Institutional Review Board.
Consent to Participate
Participants provided verbal consent to participate prior to interviews and focus groups.
Consent for Publication
Verbal consent included consent to publish anonymized quotations from interviews and focus groups
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the National Center for Complementary and Integrative Health K24AT011561 [identifiable funding information provided with submission]
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is not available for sharing for patient privacy.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.