
Abstract
Keywords
Introduction
Despite having the highest per capita investment in health care in the world, the United States has alarmingly poor health outcomes, and this situation is getting worse. 1 An important and largely overlooked problem is our focus on treating diseases separately, once they occur, rather than making the upfront investment needed to maintain and restore the health of the whole person. Whole person health refers to the idea that every individual’s location on the health-disease continuum is the product of broad interconnectivity both within and across biological systems, health behaviors, social connectedness, and environmental factors. Indeed, complex adaptive systems, comprising interconnected factors at multiple levels from individual behaviors to broader environmental influences, shape public health issues like obesity. 2 Similarly, bio-psycho-social interactions underlie the effects of worker burnout and, more broadly, chronic stress.3,4 As such, there is a need to recalibrate our health care system toward a more integrated, whole person perspective.5-8 While the concept of whole person health is not new, our global health crisis underscores the importance of approaching health from the whole person perspective.
In this paper, we make the case for transforming our approach to health care from a disease-oriented model to a “whole person” biopsychosocial health model. We use an illustrative, hypothetical clinical case study to demonstrate the transformative impact that whole person health could have on the U.S. health care economy, as well as the well-being of patients.
Methods
We based our case on what can be considered as an amalgam of actual patient experiences. We describe a 40-year-old female patient who serves as our starting point for 2 different potential paths of care going forward. One follows a likely future path under conventional health care, and one follows a possible path under a whole person health care approach. Both paths follow our patient until she is 80 years of age and, although hypothetical, are built on underlying details about the patient’s likely health and health care utilization for each year. Narratives of these paths are described below. The full details are available in a supplemental file. This study was evaluated by the RAND Human Subjects Protection Committee and determined to be not human subjects research.
Health Care Cost Estimation
Two opposing health care models are contrasted: The first is a more reactive, disease-oriented, fragmented care approach that can be characterized by a greater number of specialist visits, diagnostic testing, prescription medicines and other treatment interventions. The second is a whole person, integrated, health promoting approach characterized by more proactive, holistic, skills-based interventions that are tailored to individual needs.
The details on health care utilization and unit costs underlying our 2 different care paths were laid out by a primary care provider with experience under both scenarios (see Supplemental Data). The detailed care paths were then reviewed by a second, independent primary care provider, also with experience in both scenarios. Given that both care paths were intended to represent generic trajectories and not extreme cases, both primary care providers were asked to use their best professional judgement to identify average health complaints, treatment options and outcomes in both trajectories. All health-related diagnostics and treatments outlined in this paper were consistent with current U.S. clinical guidelines. Several prescription drugs were included in the conventional care scenario (metformin, omeprazole, temazepam, hydrochlorothiazide and lisinopril), all of which are supported by U.S. clinical care guidelines for the respective conditions.9-12 The whole person care scenario incorporated several evidence-based nonpharmacologic interventions emphasizing health promotion and symptom self-management, including cognitive-behavioral therapy,13,14 deep breathing techniques,15-18 physiotherapy,19,20 health coaching, 21 and nutritionist consultations.22,23 The health care utilization underlying each care path was valued for each year using the same set of USD 2023 unit costs (prices). The stream of costs was then discounted using a real discount rate of 3 percent back to the beginning of our patient’s 40th (decision) year. Cumulative costs for each path were graphed for each year. Data analysis consisted of calculation of frequencies, sums and averages using Microsoft Excel. All raw data used in these analyses can be found in the Supplemental data spreadsheet.
The prices used and the health care utilization assumed for the conventional care path were both vetted against data from the 2020 MEPS 24 after those estimates were adjusted to 2023 costs using the medical care consumer price index. 25 The prices used were based on the average cost per unit across all payers (ie, costs paid by public and private insurers as well as by the patient and family) for each type of health care (eg, office visits, pharmacy, hospitalizations) and also compare favorably with Medicare national prices. 26 Because MEPS data do not include nursing home costs, our estimate of annual nursing home costs comes from an actual cost survey of 2438 residents of a county in Minnesota who did not have cognitive impairment. 27 We inflated their 2010 annual cost of full-time nursing home use ($75,257) to a 2023 cost of $105,360 using the medical care consumer price index. This estimate compared favorably to those found via web searches.
As a check on our assumptions regarding health care utilization and prices, we compared our estimated costs each year (the sum of counts of each type of health care assumed to be used that year multiplied by its price) for the conventional care path to the average total health care costs in the MEPS data for women aged between 40 and 80 and with hypertension (a starting condition of our case study patient).
Clinical Case Study
Our patient, Mrs. M, is illustrated in Figure 1. This is her 40th birthday, and she is at a decision point. She has been using conventional medicine up to this point in her life, and at present she has been diagnosed with, and is on medications for, hypertension (hydrochlorothiazide) and knee osteoarthritis (ibuprofen and acetaminophen). She is also seeking help for persistent insomnia, heartburn, and weight gain. Note that her symptoms are common in this age group and indicate the involvement of several different body systems, which are often each treated separately. We follow her for the next 40 years from this point forward and examine her health and health care utilization as she experiences each of 2 alternate care paths/scenarios. The first is a continuation of a conventional health care approach. The second is a change to a whole person approach. Hypothetical case history of “Mrs. M”: diagnoses and medications at age 40 years.
Results
We will first describe what happens to Mrs. M under each of the 2 scenarios. Then we will present estimates of the costs to the health care system under each care path.
Conventional Care Scenario
In this scenario (Version A), Mrs. M continues under conventional care. At age 41, her blood pressure remains elevated, and she was started on an angiotensin converting enzyme inhibitor (lisinopril) in addition to hydrochlorothiazide. Although she was advised to lose weight at age 40, her body mass index increased from 28 to 30 in the last year, and her recent fasting blood sugars and HgbA1C have been slightly elevated. As efforts to improve her diet have been unsuccessful, she was started on metformin. At age 45, she underwent an upper endoscopy, was diagnosed with gastroesophageal reflux, and was started on omeprazole. She was also prescribed temazepam to take for sleep, such that she is now on a total of 6 medications (Figure 2-Version A). The figure also illustrates how each of Mrs. M’s medical problems is being treated separately. Two possible versions of Mrs. M’s health trajectory at age 45 years: Version A – conventional care (left panel) and Version B – whole person care (right panel). In the conventional care trajectory, by 45 years of age, Mrs. M is taking 6 different medications for 5 diagnoses. In the whole person care trajectory on the right, several factors influencing Mrs. M’s health have been identified, and she is consulting with a variety of health professionals in order to adopt healthier behaviors.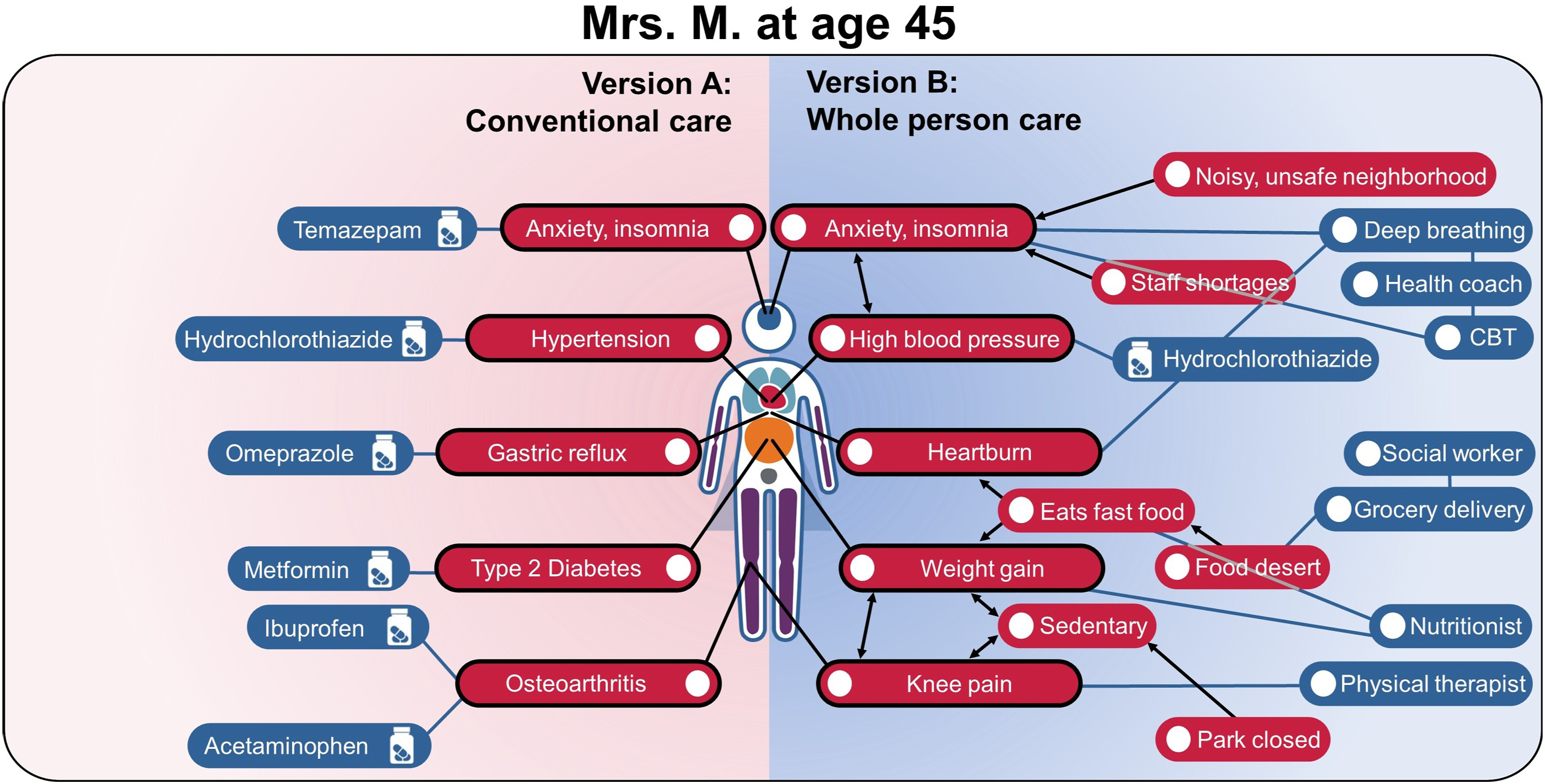
Thirty-five years later (Figure 3-Version A), at age 80, Mrs. M is in a nursing home. Her hypertension and diabetes are under reasonable control, but her insomnia and chronic knee pain are increasingly problematic. She has not been able to sleep without medication for many years. She has had some significant cognitive decline, daytime somnolence, unsteady gait, several falls, and worsening anxiety. She had a gastrointestinal bleed from erosive gastritis in her mid-60s and can no longer take nonsteroidal anti-inflammatory drugs, and she has needed stronger analgesics to control the knee pain, including occasional opiates for acute exacerbations. Two possible versions of Mrs. M’s health trajectory at age 80 years: Version A – conventional care (left panel) and Version B – whole person care (right panel). In the conventional care trajectory, by 80 years of age, Mrs. M’s health has continued to decline. She is taking a variety of medications, living in a nursing home, and experiencing cognitive decline, mobility limitations, and several other health issues. In the whole person care trajectory on the right, the early skills training has resulted in Mrs. M improving her nutrition, physical activity, stress management, and sleep. Her health concerns are minor, and she has retained good physical and mental health.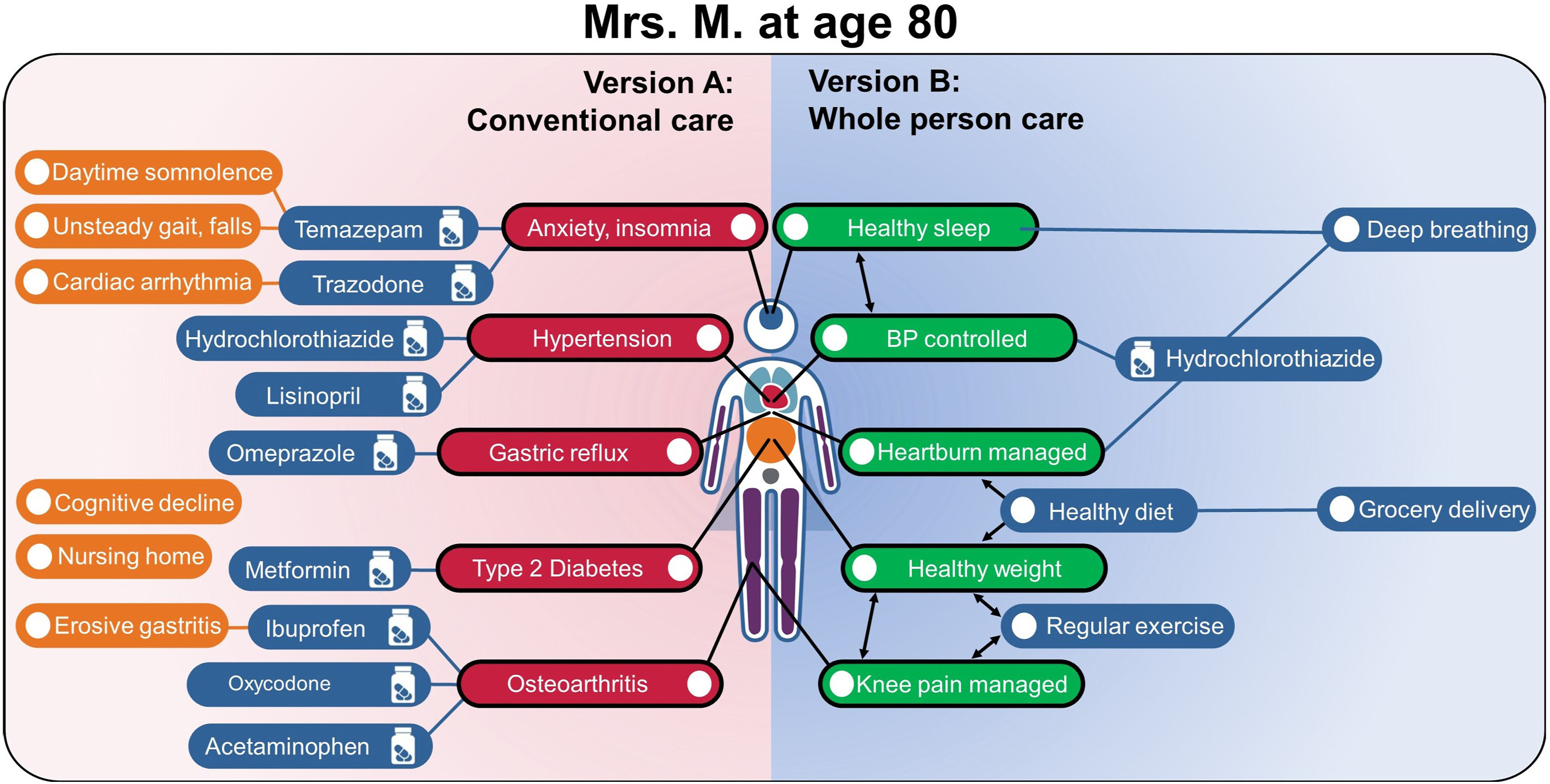
Whole Person Care Scenario
In this scenario (Version B), starting at age 40, Mrs. M’s care team starts by exploring possible connections between organs and systems, as well as across biological, behavioral, social, and environmental domains. Upon further questioning, Mrs. M reports that her neighborhood has become increasingly noisy and unsafe, which adversely affects her sleep. She notices that her blood pressure and heartburn are worse when she has not been sleeping well. She works as a receptionist at an urgent care clinic and has had to work extra shifts due to staff shortages. Her work is mostly sedentary, and although she used to go walking in a nearby park, recent construction made the sidewalk unusable, and she stopped going. She has gained weight in the last 5 years and feels the lack of exercise has contributed to her weight gain and worsening knee pain. Her diet consists of mainly what she can grab quickly at work or on the drive home. There are no grocery stores selling fresh fruits and vegetables within a convenient distance of her home.
After Mrs. M’s initial evaluation, she was referred to a health coach who instructed her on using an app for cognitive behavioral therapy/breathing exercise to help her sleep. She noticed that the abdominal breathing exercises helped with her heartburn as well as her sleep. At age 41, she was referred to a physical therapist for her knee pain and was able to increase her walking time, using a fitness tracking watch for motivation, and she was able to discontinue her prescription ibuprofen and acetaminophen. The following year (age 42), she was referred to a dietician for nutritional counseling and to a social worker who helped her sign up for a home food delivery program. With more energy due to her improved sleep, she is more motivated to start cooking meals, which she enjoys. Her weight stabilized, and her blood sugar began to trend down. Her successful behavior change was facilitated by a personalized approach, starting with what mattered most to her (wanting to improve her sleep), and gradually incorporating additional elements of physical activity and diet. She remained on only 1 medication, her antihypertensive (hydrochlorothiazide). Figure 2 - Version B shows where she is at age 45. Importantly, the lifetime habits and stress management skills that Mrs. M acquired in her 40s will be relevant for the rest of her life, allowing her to play a more active role in her health journey and contributing to a healthy aging process.
Fast forward 35 years, to age 80 (Figure 3 - Version B): Mrs. M has been living at her daughter’s home for the last 10 years, remains physically active, and helps care for her grandchildren, which she describes as adding meaning and purpose to her life. She continues to take a diuretic to control her blood pressure, and this remains her only medication. She eats mostly home-cooked food, and her weight and blood sugar have been stable. Her knee continues to bother her, mainly going up and down stairs, but she says the pain is “manageable.” She describes her overall health as “good” and is satisfied with her life.
Health Care Utilization and Costs
Healthcare Cost Estimates and Healthcare Utilization Across the Years for Mrs. M. Under Conventional Care and Under Whole Person Health Care.
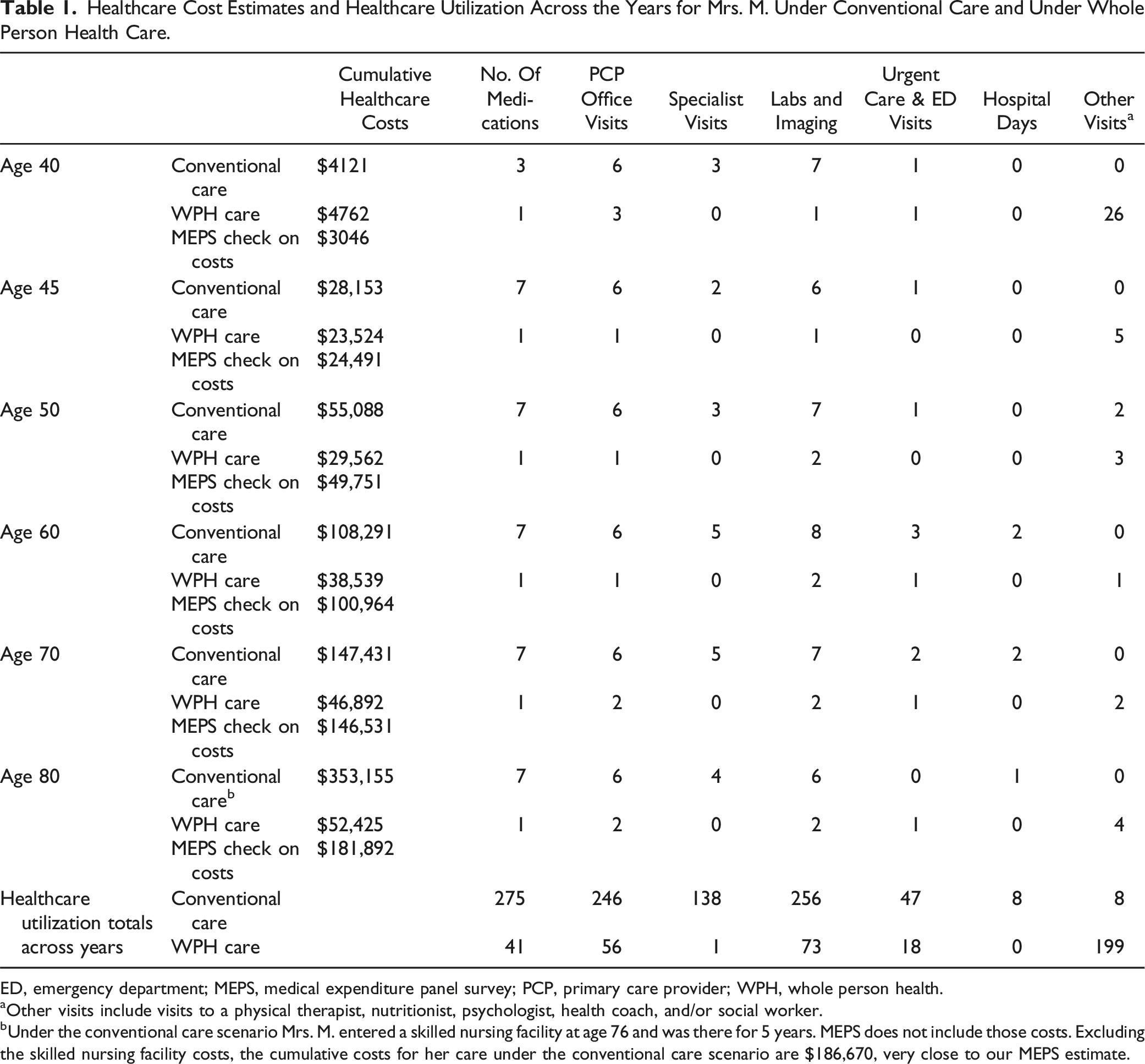
ED, emergency department; MEPS, medical expenditure panel survey; PCP, primary care provider; WPH, whole person health.
aOther visits include visits to a physical therapist, nutritionist, psychologist, health coach, and/or social worker.
bUnder the conventional care scenario Mrs. M. entered a skilled nursing facility at age 76 and was there for 5 years. MEPS does not include those costs. Excluding the skilled nursing facility costs, the cumulative costs for her care under the conventional care scenario are $186,670, very close to our MEPS estimate.
Although the starting point for Mrs. M is the same in both scenarios (Figure 1), the differences between the approaches are obvious from the start. The biggest difference is that, in Version B (whole person care), she has a total of 26 visits with various providers in the first (40th) year: 12 visits with a psychologist, 12 visits with a health coach, and 2 visits with a social worker. Physical therapy is added in her second (41st) year and a nutritionist in her third (42nd) year. This one-on-one support continues but tapers over the next few years. This support is expensive, and total health care costs are higher in the first 4 years for whole person care than for the conventional approach. However, that support quickly pays off as conventional care costs continue to increase over time.
The principal differences in health care utilization are evident in the last 2 rows of Table 1, where the units of health care resources used across the years are summed. The whole person care approach resulted in far fewer years taking multiple medications than conventional care did—one medication across all years for the whole person care scenario vs moving from 3 to 7 medications in years 40 to 45 and continuing at 7 for the remaining years under conventional care. The conventional care scenario also involved many more primary care and specialist visits, more laboratory tests and imaging, more urgent care and emergency department visits, and a total of 8 days of hospitalization, whereas the whole person care scenario included no hospitalizations. Note that Mrs. M did continue to receive conventional care under the whole person care scenario. She still visited her primary care provider once or twice a year, had regular blood tests done, and even visited urgent care a few times over the years. But she benefited from the support she received from her annual visits with a health coach plus visits with physical therapists, nutritionists, and psychologists as needed: a total of 199 visits with these providers over the years.
The total cumulative health care costs in each year for each scenario are shown in Table 1, the supplemental file, and Figure 4. As can be seen in Figure 4, our assumptions of health care utilization under the conventional care scenario are validated by the match between our estimated cumulative health care costs and the average cumulative costs found in MEPS for women of each age except where these estimates diverge starting at age 76. Under the conventional care scenario, Mrs. M goes into a skilled nursing facility at age 76, and MEPS data do not include these costs. If skilled nursing facility costs are removed from our estimates, our match to MEPS estimates occurs for all years. Overview of the 2 health care trajectories: version A – conventional care (top) and version B – whole person care (bottom). While whole person care is somewhat more expensive at early time points, expenditures slow as Mrs. M acquires healthier habits and enjoys better health. Conventional care shows steady increases in health care costs over time, with generally poorer outcomes, compared to whole person care.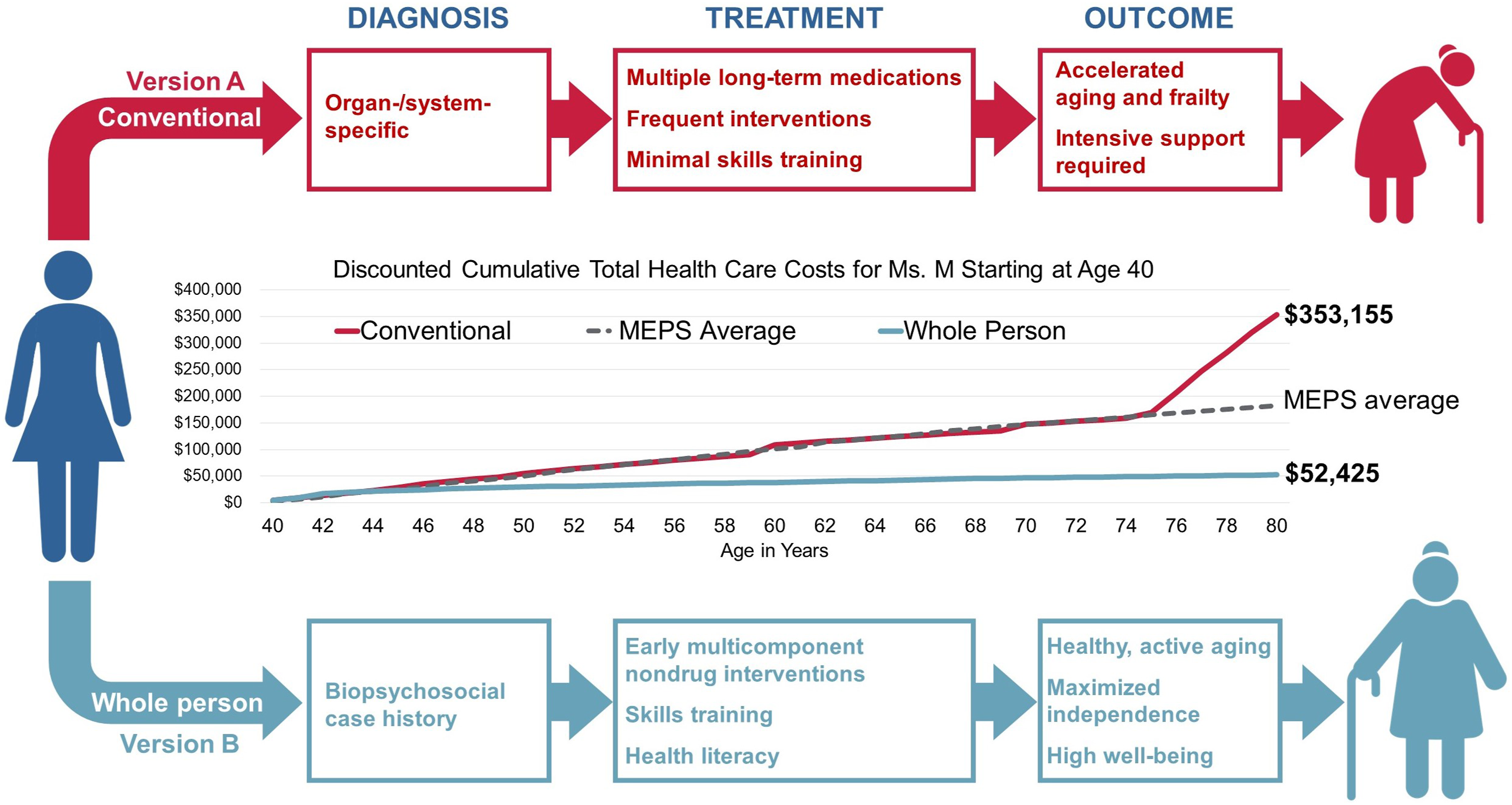
Also shown in Figure 4, total cumulative health expenditure from age 40 to 80 was $353,155 for Version A (conventional care) compared with $52,425 for Version B (whole person care). Health care costs rise dramatically over the years for Mrs. M under the conventional care scenario with multiple long-term medications and associated side effects, frequent provider visits and interventions, and minimal skills training. The cumulative effect is accelerated aging, frailty, and poor quality of life. In contrast, under the whole person care scenario, she benefits from early and robust investments in behavioral and lifestyle interventions in her 40s, which allow her to remain active and independent at age 80.
Discussion
This study highlights one of the major challenges in demonstrating the cost-effectiveness of prevention and lifestyle interventions: the long time-horizon required to achieve the return on investment for this model of care. In other words, interventions such as health coaching, physical therapy, and nutrition counseling cost money, and they may even cost more initially than pharmacological interventions. However, the benefits of improved health over a lifetime dramatically reduced health care costs over the long term. Indeed, from age 40 to 50, health care costs were nearly the same for Mrs. M under both scenarios and were even slightly higher for whole person care from age 40 to 43. After age 50, however, health care spending for the whole person care scenario remained essentially flat, while spending under conventional care climbed steadily thereafter, accelerating after age 75 when a skilled nursing facility was required. This illustrates how an investment beginning in early middle age to support a healthy diet, physical activity, and stress management can not only lead to improved health and well-being but also reduce health care spending over the remaining lifespan. Additionally, in Version B, Mrs. M’s own self-care contributes and “adds value” to her health at no additional health care costs. As mentioned, the whole person care approach may involve greater up-front expenditures aimed at supporting skills training and adherence to healthy lifestyle choices. However, our findings show long-term expenditures to be substantially lower than the conventional care model, due largely to avoiding costly care associated with disease progression, development of comorbidities and adverse events. Moreover, given the better mental and physical health outcomes, the whole person care model could reasonably be expected to result in a greater number of years lived without disability, or disability adjusted life years (DALYs). However, this was not assessed in the current work.
Although our case study relies on an “imagined” case, it is based on 2 versions of a typical case history, with all expenses itemized in detail. We also validated the prices we used for the various health care resources against data from the average cost per unit in MEPS and from Medicare pricing, and we validated our assumptions on health care utilization under the conventional care scenario by comparing to the average annual costs for women of the same age in the MEPS data. Our conventional care cost estimate ($353,155) also closely matches that found in a study of lifetime health care costs, including nursing facility costs ($314,093), after adjusting to our age range and putting their estimates into 2023 USD. 28 As such, we feel that Version A and B cost estimates accurately reflect the 2 scenarios. Nonetheless, it must be stated that even if our Version B costs were double our estimate, this would still represent approximately one third of the cost of Version A (conventional care).
Summary and Conclusion
Mrs. M Versions A and B illustrate 2 contrasting approaches to patient care. In Version A, Mrs. M suffers from the common problem of having been broken down into separate body parts and disease diagnoses. Each problem is treated separately, and by age 80, the resulting polydiagnosis and polypharmacy have created an additional layer of iatrogenic, drug-induced pathology. Failure to understand the importance of seeing Mrs. M as a whole person has led to her being treated using a fragmented, disease-focused model that relies on pharmacological control of separate diseases and conditions rather than addressing the underlying factors and restoring health. In contrast, Version B illustrates a whole person approach to health care that seeks connections across body systems, as well as across biological, behavioral, social, and environmental domains, focusing on nonpharmacologic interventions and support for behavior change.
A whole person biopsychosocial health model beginning at age 40 could plausibly result in substantial health care savings over the following 4 decades. Adopting a whole person approach to health even earlier in life could be expected to result in even more meaningful impacts on health and health care costs. In our model, although support for lifestyle and behavioral interventions cost money initially, these costs were more than offset by a reduction in health care spending in later years.
Supplemental Material
Supplemental Material - Making a Case for Whole Person Health
Supplemental Material for Making a Case for Whole Person Health by Patricia M. Herman, Mark H. Pitcher, and Helene M. Langevin in Journal of Global Advances in Integrative Medicine and Health.
Footnotes
Acknowledgments
The authors would like to thank Sekai Chideya, M.D. and Amy Locke, M.D., for their valuable input on the health care utilization assumptions underlying the analyses described in this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclaimer
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the National Institutes of Health or the United States Government.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.