
Abstract
Background
There has been rapid growth of chiropractors pursuing career opportunities in both public and private hospitals and other integrated care settings. Chiropractors that prosper in integrated care settings deliver patient-centered care, focus on the institutional mission, understand and adhere to organizational rules, and are proficient in navigating complex systems. The Council on Chiropractic Education Accreditation Standards do not outline specific meta-competencies for integrated care clinical training.
Objective
The purpose of this study was to develop preliminary integrated health care competencies for DC programs to guide the advancement of clinical chiropractic education.
Methods
A systematic literature search was performed. Articles were screened for eligibility and extracted in duplicate. Domains and seed statements were generated from this literature, piloted at a conference workshop, and evaluated via a modified Delphi consensus process. Of 42 invited, 36 chiropractors participated as panelists. Public comment period yielded 20 comments, none resulting in substantive changes to the competencies.
Results
Of 1718 citations, 23 articles met eligibility criteria. After 2 modified Delphi rounds, consensus was reached on all competency statements. A total of 78 competency statements were agreed upon, which encompassed 4 domains and 11 subdomains. The 4 domains were: 1) Collaboration, (2) Clinical Excellence, (3) Communication, and (4) Systems Administration.
Conclusion
We identified 78 preliminary competencies appropriate for preparing DC students and early career chiropractors for clinical practice in integrated healthcare settings. Educational programs may consider these competencies for curricular design and reform to strengthen DC program graduates for integrated practice, advanced training, and employment.
Introduction
Integrated health care delivery is a concept that aims to overcome fragmented patient care, particularly where disconnected care leads to a negative impact on a patient’s care experience and clinical outcome. The integrated health care approach is now commonly accepted, throughout the world, as the preferred model to patient care and healthcare system design. 1 Thus, there is an increasing need for health care trainees to be prepared to function within an interdisciplinary team.
Interdisciplinary team-based care has been shown to enhance productivity, safeguard a wholistic approach to patient care, and promote patient care innovation.2,3 Further, interdisciplinary team-based care has been shown to improve clinical outcomes, particularly in the care for non-communicable diseases.3,4 In addition, studies have illustrated improvements in patient care access, coordination, and patient safety.3,5
Chiropractic is the largest complementary integrative health profession in the United States 6 and focuses on the diagnosis and management neuromusculoskeletal conditions.7,8 Given the standardization and value of integrated health care, it is essential for all health care professionals to be competent and able to collaborate as part of an interdisciplinary team, working together for the common goal of patient-centered care. 9 This emerging need for team-based health-care delivery necessitates chiropractors – one of the most common health care professionals to be consulted for spine pain10-13 - to be prepared to engage in an interdisciplinary team.14,15 Chiropractors that excel in integrated care settings have been described to go beyond delivery of patient-centered care to align with the institution’s mission, understand the rules of the organization, adhere to the administrative requirements of the position, and understand how to work within the system of the institution. 16
The purpose of this study was to develop an initial set of competencies for chiropractic students preparing to work as part of an interdisciplinary team and enhance integrated care delivery. This project came about because the authors, who mostly practice and provide training for Doctor of Chiropractic (DC) students and post-graduate residents in integrated care environments, perceived that DC students and residents lack the competencies and skills to optimally function within an interdisciplinary team. In response to the authors’ observations, lack of Council on Chiropractic Education (CCE-USA) meta-competency outcomes specific to integrated care, we sought to develop a set of specific preliminary competencies suitable for DCs to function in integrated care settings and as part of interdisciplinary teams that extends across clinical care settings. Similar to public health competencies developed for the chiropractic profession, 17 this may establish an initial step in a pathway to allow CCE-USA and DC programs to consider these meta-competencies and competencies, respectively, when refining guidance and curricula in the future.
Methods
Human Subjects Considerations
The Logan University Institutional Review Board approved the project prior to initiation (#RD1005220595, October 5, 2022). All steering committee (SC), workshop, and modified Delphi panelist participants contributed voluntarily and without compensation. Informed consent was obtained from each Delphi panelist including an agreement to be acknowledged.
Project Steering Committee
The SC of 20 members consisted of chiropractors in practice within integrated healthcare settings, and DC program clinical education experts. Five SC members served as board members for Clinical Compass (https://www.clinicalcompass.org), a non-profit chiropractic evidence synthesis think tank. Regarding employment, 8 SC members practiced within VA, 5 practiced in non-VA hospitals, 3 practiced at FQHCs, and 3 were educators in DC program institutions. Additionally, 3 members of the SC were CCE-USA accredited DC residency program directors and 6 SC members graduated from a CCE-USA accredited DC residency program.
Overview of Plan
A structured strategy for identifying competencies for US pre-licensure DC students was executed in 4 phases from August 2022 through November 2023. The phases of competency development were: In Phase I, the SC conducted a literature search synthesizing existing competency literature. During Phase II, members of the SC presided over an academic conference workshop to review search findings and to seek stakeholder feedback on proposed competency domains. During Phase III, proposed competencies were developed based on feedback from Phases I and II and a modified Delphi consensus process was undertaken. During Phase IV, public comment was sought to include additional stakeholders. (Figure 1) Study methodology timeline.
Phase I (Literature Search and Synthesis)
In September 2022, the SC conducted a systematic search and synthesis of existing chiropractic and other health profession competencies relevant to integrated clinical care. Results of the search and synthesis were used to draft competency domains to be presented in Phase II. The results of the evidence review were synthesized into initial drafts of candidate standardized terminology, definitions, and competencies.
Search Strategy
Literature Review Eligibility Criteria.

Article Selection
Search results were uploaded from Endnote to a website for organizing systematic reviews (Rayyan, Cambridge, MA). 23 After duplicate citation removal, a paired team (AZ, KM) of the SC independently screened titles and abstracts against the eligibility criteria. Those titles and abstracts that met the screening criteria were saved and a paired team (AZ, MK) of the SC independently evaluated full text manuscripts against the eligibility criteria. When consensus was not reached a third member of the SC (CD) adjudicated. The following data were extracted from included citations independently by 2 SC members (AZ, MK): author, year of publication, relevant profession/specialty/discipline, study methods, development target, domains, and competencies by domain.
The SC identified and analyzed domains and competencies from each included source. Members of the SC (CD, ZC, JN, RW) derived preliminary themes through inductive means using an iterative process. Extracted themes were preliminarily grouped into the following categories: Clinical Acumen, Collaborative Team, Digital Health, Interpersonal, Interprofessional, Practice-Based Learning, Professionalism, Roles and Responsibilities, and System/Organization Level.
Phase II (Workshop)
Workshop participant (n = 9) and Delphi panelist demographics (n = 36).

Phase III (Modified Delphi Panel)
Utilizing an iterative process, the SC evaluated materials developed from Phase I and Phase II to generate competency domains, subdomains, and seed statements. Workshop attendees from Phase II were invited to participate in the subsequent consensus process. Some of the invited stakeholders were cross trained as physicians, physical and massage therapists.
We followed the RAND/UCLA appropriateness methods for assessing the drafted statements by using a 1-9 ordinal scale (highly inappropriate to highly appropriate). 25 The modified Delphi process was executed until 80% consensus was reached with a median rating of at least 7 for each drafted competency statement. Panelists were emailed the draft competency statements, corresponding rating scales, and an open textbox to type comments. They were instructed that any ratings that were not appropriate (7-9) required a comment with rationale to support the rating. Inappropriate ratings (1-6) without an included comment were treated as incomplete and withheld from analysis.
Data Analysis
Delphi panelists were anonymous and codified to a number by the project coordinator (CE). Members of the SC were blinded to individual panelist names and their ratings were uploaded into SPSS (v.25) (IBM Corp., Armonk, NY). Each statement was assessed for median rating and percent agreement by an SC member (CH). The de-identified individual panelist ratings were distributed to SC members for review of statement ratings, percent agreement, and comments.
Phase IV (Public Feedback)
For transparency and completeness, we sought public feedback on the competencies after they had reached panel consensus (November-December 2023). This allowed opportunity for stakeholders to contribute who were not involved previously. Clinical Compass assisted in public distribution of the competency statements through posting on their website 26 and circulated the statements via an email distribution list utilized in the development of prior clinical practice guidelines.27,28
Results
Systematic Search of the Literature
The literature search yielded 1718 citations. After applying the eligibility criteria, 23 articles remained.16,29-50 (Figure 2) Themes identified through article extraction resulted in 9 potential domains (Supplemental Table 2). Review flow chart. See Supplemental Table 3 for the list of excluded articles.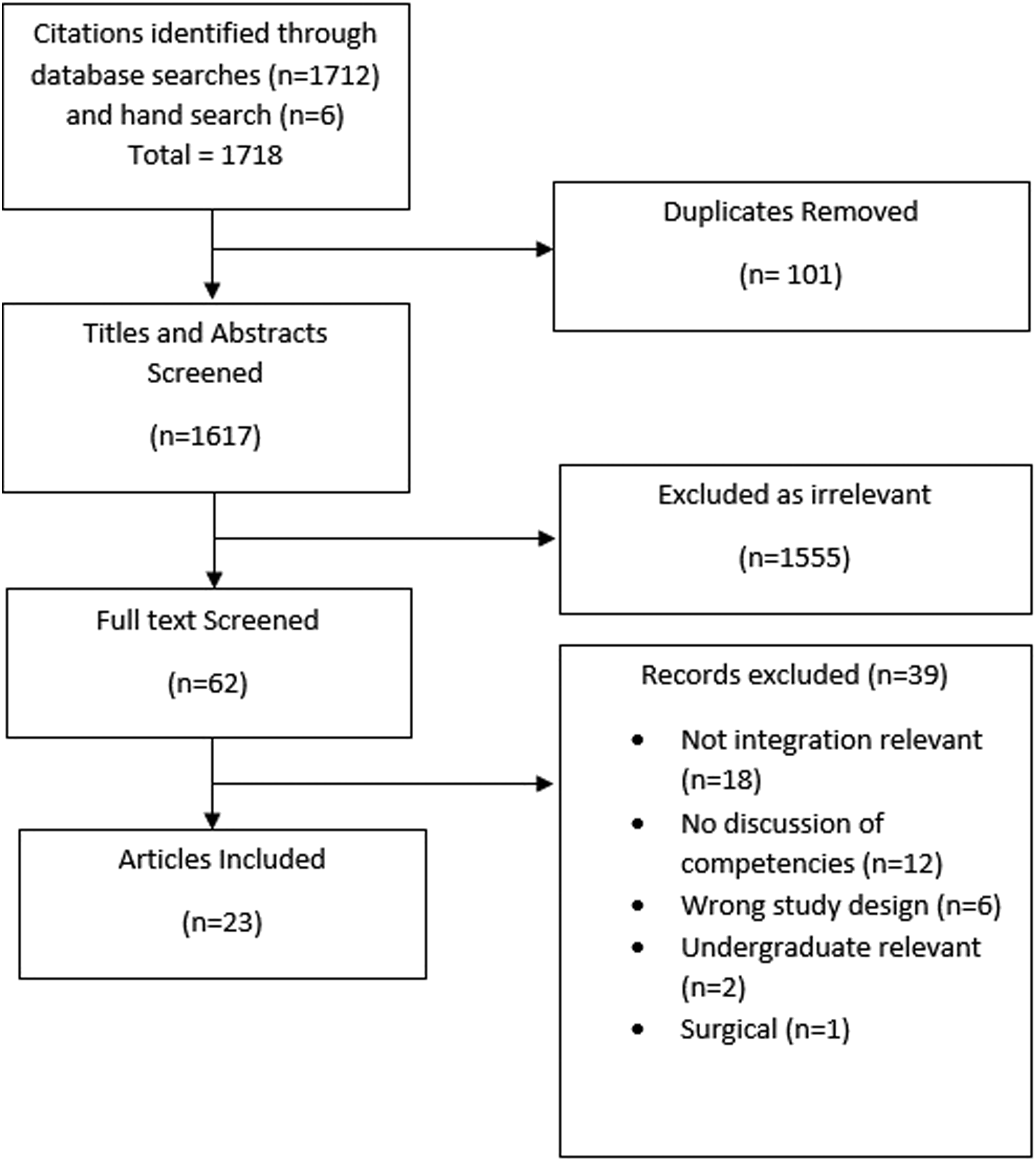
Domain and Seed Statements
Phase II and Phase III of the competency development process led to consolidation of the 9 initially drafted competency domains into 4 domains, 11 subdomains, and the generation of 78 draft statements for review in the modified Delphi process. After Phase III (2 modified Delphi rounds), consensus was reached on all statements.
Delphi Panel Characteristics
Of the 44 individuals invited to participate, 36 (82%) agreed. All panelists resided in the United States and held a chiropractic degree, with 1 participant dual-trained as a physical therapist. A total of 6 panelists had a PhD, and 16 had a master’s degree (e.g., MS, MBA, MPH). The panelists had a mean of 20.3 years in practice, with a median of 19 years (range 1-51). Most panelists self-identified as male (69%), and White/Caucasian (92%). Other races reported were: unspecified (1), Black/African American (1), and multiracial (1).
Seven panelists were DC residency directors for CCE-USA accredited programs. Twenty-three panelists had a faculty affiliation with a DC program, and 10 reported affiliations with non-DC health professional programs. Twenty-one panelists trained in integrated environments as a DC student and 8 as a post-graduate resident. Twenty-seven panelists worked in integrated settings: DoD (1), FQHC (1), private/public hospital (8), and VA (17).
Delphi Process
Consensus was reached on all competency statements after 2 rounds of a modified Delphi process. Following round 1, only 1 statement did not reach a consensus rating of ≥80% (median rating = 9 on a 1-9 scale). After reviewing the ratings and panelist comments, the SC revised 1 statement that did not reach consensus. The SC substantially changed 11 additional statements based on Delphi panelist feedback. These 12 statements were revised and included in round 2 of the modified Delphi process. In round 2, consensus of the panelists (≥80%) was reached on all 12 statements.
Public Comments
We received 20 comments following the public comment period. The comments were from 6 practicing chiropractors and 1 chiropractic academic (Colorado, Florida, Ohio, Oklahoma, Texas, Washington, and Australia). The SC carefully reviewed all statements and found the majority of comments were generally supportive. Most comments were typographical or stylist in nature and none provided feedback warranting substantive change to the consensus statements.
Consensus Competencies (Figure 3)
Competency Domain 1 – Communication
Subdomain 1.1: Interprofessional
1. Understand the importance of using common language, terminology, and communication (e.g., diagnostic and prognostic terms, outcome assessment tools) amongst the integrated healthcare team. 2. Proficient in communication strategies to facilitate health care team interactions for patient care coordination (i.e., oral, written, and electronic). 3. Proficient in describing patient case presentation (i.e., oral, written, and electronic) to members of the integrated health care team. 4. Demonstrate timeliness in record keeping and communication for care coordination. 5. Respect patient confidentiality in all forms of communication consistent with HIPAA privacy rules.
51
6. Receptive and responsive to constructive feedback from various stakeholders (e.g., patients, supervisors, health care team members). 7. Demonstrate proficiency in conflict management (e.g., disagreement among health care team professionals regarding treatment plans). 8. Educate patients and stakeholders regarding standards of care, and case management that is concordant with guidelines and best practices. Final competency domains and subdomains. (Image created by Zachary Cupler, DC, MS, Robert Trager, DC, Clinton Daniels DC, MS).

Subdomain 1.2: Interpersonal
1. Exhibit emotional intelligence through a capacity to understand the emotional expression of others, awareness of one’s own emotions, and emotional self-regulation.
16
2. Demonstrate cultural and professional humility, and respect for beliefs and practices. 3. Develop a trusting relationship with patients and other health care team members while maintaining appropriate boundaries. 4. Demonstrate active listening with the patient to foster a therapeutic relationship (e.g., facilitate goal setting, understand barriers and facilitators to care). 5. Use communication strategies that are conducive for positive patient behavioral change (e.g., motivational interviewing). 6. Encourage patient commitment to use of appropriate self-care practices (e.g., diet, exercise, mind-body practices). 7. Acknowledge patient perception and experiences when developing a therapeutic relationship (e.g., trust, openness, attentiveness, cultural awareness). 8. Differentiate patient education to align with patient’s presentation and health literacy levels.
Competency Domain 2 – Clinical Excellence
Subdomain 2.1: Patient Safety
1. Deliver and document appropriate informed consent process inclusive of procedure description, potential treatment benefits, material risks or alternative management options, and answering all patient questions. 2. Identify when to modify evaluation procedures based on patient presentation and potential risk (e.g., patient is a high fall risk, acute spinal antalgia). 3. Demonstrate knowledge of patient safety best practices (e.g., occupational health regulations,
52
infection control, local clinical standard operating procedures, equipment cleaning procedures). 4. Ability to apply operational standards of safety in various clinical scenarios and settings (e.g., disaster preparedness, medical emergency response). 5. Recognize signs of risk to patient safety which would warrant referral (e.g., depression, post-traumatic stress disorder,
53
substance use disorder,
54
intimate partner violence,
55
suicidal
56
or homicidal ideation). 6. Recognize signs and symptoms of potential contraindications to manual therapies or other interventions and refer when appropriate.
57
Subdomain 2.2: Professional Literacy
1. Understand the role of scientific evidence, practitioner experience, and patient preferences in pragmatic management of health conditions. 2. Demonstrate ability to use scholarly databases and point-of-care medical resources to aid clinical decision making. 3. Critically apply peer-reviewed literature to case management with attention to quality and level of evidence. 4. Implement chiropractic and relevant musculoskeletal care clinical practice guidelines.27,28,57-66
Subdomain 2.3: Clinical Acumen
1. Understand the importance and limitations of scope of practice. 2. Demonstrate the ability to obtain a comprehensive health history.57,66 3. Perform a patient evaluation consistent with a biopsychosocial approach.
27
4. Develop a differential diagnosis that recognizes pain classification subgroups (e.g., nociceptive, nociplastic, neuropathic).27,58-61 5. Recognize clinical indications for diagnostic imaging and testing consistent with American College of Radiology
67
and American College of Occupational and Environmental Medicine guidelines.
68
6. Consider relevant imaging and testing findings for correlation with clinical presentation to construct a differential diagnosis, prognosis, and treatment plan. 7. Identify appropriate clinical indications to collaborate with other health professionals (e.g., specialist consultation or referral). 8. Manage complex patients (e.g., patients with multiple comorbidities
69
) through team-based interprofessional shared decision-making. 9. Develop treatment plans that are evidence-informed, patient-centered, and goal-oriented.70-75 10. Employ active care educational strategies which promote self-care management and optimizes patient-independence. 11. Recognize the impact of how contextual factors (e.g., words used, attire, environment, body language) influence a patient’s experience and clinical outcomes.76,77 12. Knowledgeable of health screening and disease prevention guidelines for health promotion (e.g., US Preventive Service Taskforce recommendations).78,79 13. Advocate for health promotion relevant to primary, secondary, tertiary, and quaternary prevention of musculoskeletal conditions.28,78 14. Understand the unique clinical needs of special populations (e.g., pediatrics, older adults, various racial and ethnic groups, individuals with disabilities, lesbian, gay, bisexual, transgender, queer, intersex, asexual (LGBTQIA+), pregnant, veterans). 15. Appreciate the influence of social determinants of health on health and wellness (e.g., discrimination, education access, healthcare access, economic stability, neighborhood environment).
79
Subdomain 2.4: Ethics
1. Demonstrate high standards of personal and professional ethical conduct. 2. Place the patient at the center of healthcare delivery.
80
3. Possess an understanding of the professional legal obligations (e.g., mandatory reporting) consistent with jurisdictional licensure and regulations, healthcare system policies (e.g., credentialing and privileging). 4. Responsibly use existing and burgeoning technology for patient care when appropriate (e.g., health technology, electronic health record systems, artificial intelligence). 5. Proficient in ethical diagnostic and procedural coding that is commensurate with services rendered.
Competency Domain 3 –Collaboration
Subdomain 3.1: Roles and Responsibilities
1. Understand the roles, responsibilities, and contributions of each healthcare team member. 2. Demonstrate and communicate the importance of teamwork in patient-centered care. 3. Recognize how one’s uniqueness (e.g., experience level, culture, hierarchy) impacts interprofessional working relationships. 4. Communicate effectively with health care professionals and health-related agencies. 5. Communicate assessment and care plan recommendations to healthcare professionals. 6. Develop effective relationships with referring, consulting, or collaborating healthcare team members. 7. Articulate professional opinions with competence, confidence, and respect, using inclusive and shared language that avoids chiropractic-specific language.
Subdomain 3.2: Cooperation, Respect and Engagement
1. Seek out, integrate, and value the input of healthcare team members. 2. Engage healthcare team members to develop strategies to meet specific health and healthcare needs of patients and populations. 3. Share accountability for patient outcomes when co-managing with other clinicians. 4. Ability to give timely, sensitive, and constructive feedback to colleagues.
Subdomain 3.3: Self-Reflection
1. Practice critical self-appraisal to identify training gaps for development. 2. Engage in evidence-based continuing education and self-guided learning. 3. Consider one’s own health and well-being as fundamental to healthcare delivery. 4. Demonstrate a commitment to continuous professional and personal self-improvement.
Domain 4 - Systems Administration
Subdomain 4.1: Digital Health
1. Be knowledgeable in the practices of virtual healthcare delivery (e.g., patient preferences, patients that live in rural areas, lack transportation). 2. Be familiar with evidence-based digital format patient education resources. 3. Interact professionally with colleagues and patients through electronic communication and messaging (e.g., e-mail, patient portal, virtual visits). 4. Interact professionally and in alignment with evidence-based practices when utilizing social media.
81
5. Adhere to jurisdictional and facility standards regarding timeliness in record keeping, communicating diagnostic findings, and using decision support tools. 6. Engage with systems to track performance, productivity, and outcomes for continuous quality improvement.
Subdomain 4.2: Organizational Responsibility and Safety
1. Demonstrate understanding of organizational structure, chain of command, and role within a system. 2. Understand institutional credentialing and privileging concepts. 3. Demonstrate an ability to understand and communicate the financial impact of musculoskeletal conditions on healthcare facilities and healthcare systems. 4. Provide services that are consistent with facility service line agreements, functional statements, and/or memorandums of understanding. 5. Identify and report near-misses, accidents, and/or adverse events per facility standards. 6. Demonstrate ability to identify and report disruptive behavior in the workplace per facility standards. 7. Demonstrates knowledge of equipment safety standards. 8. Utilize proper techniques to prevent clinician environmental risks and injury. 9. Understand and apply relevant clinical care pathways.61,65,70 10. Facilitate efficient care coordination within the healthcare system. 11. Demonstrate understanding of various factors and limitations on a healthcare system (e.g., care access, inefficient or ineffective consultation triaging, physical space availability, commercial insurance reimbursement).
Discussion
This study identified 78 preliminary competencies related to clinical chiropractic education that, ideally, are embodied by DC students, graduates, and DC’s seeking post-graduate training and/or employment within an integrated health care setting. The 78 competencies are organized within 4 domains and 11 subdomains that reflect on Communication, Clinical Excellence, Collaboration, and Systems Administration. The authors are not familiar with any prior efforts to identify competencies associated with chiropractic practice within an integrated health care setting and view this as the first step of a continuous process towards refining competency development. Many of these identified competencies may overlap with existing CCE-USA competencies, which should be evaluated and refined in future studies. 82
Similar to the public health competencies that Madigan et al proposed for DC students, 17 we propose unique competencies for the integrated care setting. We advocate for the public health competencies previously proposed and find they align well with our domains of Clinical Excellence and Systems Administration. Rather than propose competencies, a prior study described a conceptual model highlighting specific attributes of the chiropractor who excels in the integrated care setting. 16 Our competencies presented here build upon those concepts and themes. Through key stakeholder interviews and a qualitative analysis, they identified 5 domains (i.e., patient-centeredness, professional, interpersonal, interprofessional, and organization) with themes that typified the chiropractor who excelled at interprofessional teamwork.
Many of the preliminary competencies are appropriate for preparing DC students for both integrated and private practice settings. The preliminary competencies that are particularly unique to integrated settings are focused on the complexities of team dynamics, understanding roles, and systems-based practice. The development and consensus of competencies for preparing DC students for integrated care settings is only the first step to ensure students are given opportunity to achieve the above described competencies.83,84 Future efforts may include refinement and validation of these preliminary competencies, addressing redundancy with current DC program competencies, identifying metrics to measure and track student performance of these competencies, obtaining input from non-DC stakeholders, and further characterizing competencies unique to integrated care settings.
United States chiropractic education has held to traditional didactic lecture methods of teaching followed by a clinical training phase. 83 A majority of clinical training experience occurs at DC program campus clinics and a cadre of independent private practices affiliated with the DC programs, which provide limited opportunities for interprofessional socialization with other health care disciplines. In some select instances, chiropractic student training opportunities are available within integrated healthcare systems, such as within Veterans Affairs healthcare settings.83,85 This approach is similar to other countries, such as the United Kingdom, Denmark, and Switzerland, which has transformed the delivery of chiropractic training with immediate socialization with other healthcare disciplines through shared coursework and clinical experiences.86-89
Strengths
Our systematic search of the literature and iterative process of competency domain and seed statement development was augmented by the participation of chiropractors with unique experience in integrated care clinical education. We used a rigorous Delphi methodology yielding high agreement and anonymized participant feedback. As part of this process, we collectively leveraged the forefront of individuals with experience in post-graduate chiropractic education. Of the 10 CCE-USA accredited chiropractic residency sites, 3 residency directors contributed as SC members (JN, RW, CD) and the remaining 7 residency directors participated as Delphi panelists. In addition, the residency directors of 2 private hospitals pursuing CCE-USA accreditation for DC residency programs participated as a SC member (EK) or as a Delphi panelist.
Limitations
Many of the competencies represent the ideal DC trainee or early career chiropractor. Given the current approach to training DC students, widespread achievement of these competencies may not be addressed with the current structure of DC education. Postgraduate residencies are an ideal setting for chiropractors to deepen the knowledge, skills, and abilities of the competencies we have outlined. Residencies remain a rare opportunity for chiropractors and therefore we focused on DCPs to promote a standard of integrated competencies upon graduation. Training of DC students in integrative care competencies could benefit from administrators and educators within DC programs designing curricula that provides an immersive and diverse clinical experience. Due to the complexities of the identified competencies, new evaluation procedures may require development, such as entrustable professional activities, to assess competencies we have outlined. 90 It is our collective experience that these competencies are not currently being achieved in a widespread manner by DC students and early DC graduates. Thus we suggest DC programs move toward a horizontal and vertical integration of these competency concepts into DC education curricula.91,92 We present a set of competencies derived from the literature and expert opinion. Strategies to translate these competencies into authentic professional tasks (e.g., entrustable professional activities) was beyond the scope of this Delphi consensus project. The large number of competencies in and of itself may be a barrier to implementation and likely will not be addressed in any singular iteration of curricular revision. Some competencies were crafted in a way that they are not clearly measurable and others had overlap between domains, which suggest the need for additional refinement through further research efforts. For example, a next step might interview stakeholders from DC programs and accrediting bodies to determine both the importance of the proposed competencies and how best to foster development and assessment of these skills that are consistent with existing CCE-USA meta-competency outcomes designs. In addition, we anticipate future iterations to be organized in a consolidated manner.
The opportunities available to United States based DC program trainees in the form of integrated care settings may vary greatly from chiropractic training programs around the world. The competencies developed from this study may not be translatable to other countries. Although dual-trained individuals were invited to participate on the Delphi panel, we did not invite participation from non-chiropractor healthcare professionals (e.g., physicians) who work in integrated settings and provide clinical education to healthcare trainees. We also did not invite participation from DC students, the lay public, or chiropractic patients to include their perspectives. Future integrated care competency development for DC program trainees should consider other healthcare professionals’, students’, and patients’ viewpoints. Finally, the project was not developed in conjunction with accreditors or DC program officials responsible for curricular design and competency assessment. Both of these stakeholders would be reasonable collaborators for future work in development of integrated care competencies for DC students.
Within this study, there was a lack of diversity of race and ethnicity within the SC and Delphi panel and the panelists may have been under representative of female chiropractors, which may leave out important perspectives. The chiropractic profession is 25.4% female and 90.8% White/Caucasian.93,94 Future updates to these competencies should take a concerted effort to partner with gender, racial, and ethnic minority chiropractic professional associations.
Conclusion
Using a systematic evaluation of the literature followed by a Delphi consensus process, we developed 78 competency statements aligned within 4 domains preparing DC students for practice in integrated healthcare settings. As these are foundational competency statements produced and scrutinized through expert consensus, additional work is required to validate the proposed statements and to implement them within a chiropractic curriculum. These statements may be used for DC program curricular design, and future scholarly work exploring clinical benefits when DCs are trained using these competencies as a guide.
Supplemental Material
Supplemental Material - Development of Preliminary Integrated Health Care Clinical Competencies for United States Doctor of Chiropractic Programs: A Modified Delphi Consensus Process
Supplemental Material for Development of Preliminary Integrated Health Care Clinical Competencies for United States Doctor of Chiropractic Programs: A Modified Delphi Consensus Process in Clinton J Daniels, DC, MS, Zachary A Cupler, DC, MS, Jason G Napuli, DC, MBA, Robert W Walsh, DC, Anna-Marie L Ziegler, DC, MM, MS, Kevin W Meyer, DC, Matthew J Knieper, DC, Sheryl A Walters, MLS, Stacie A Salsbury, PhD, RN, Robert J Trager, DC, Jordan A Gliedt, DC, Morgan D Young, DC, Kristian R Anderson, DC, MS, Eric J Kirk, DC, Scott A Mooring, DC, Patrick J Battaglia, DC, David J Paris, DC, Amanda G Brown, DC, Justin M Goehl, DC, MS, and Cheryl Hawk, DC, LMT, PhD in Global Advances in Integrative Medicine and Health
Supplemental Material
Supplemental Material - Development of Preliminary Integrated Health Care Clinical Competencies for United States Doctor of Chiropractic Programs: A Modified Delphi Consensus Process
Supplemental Material for Development of Preliminary Integrated Health Care Clinical Competencies for United States Doctor of Chiropractic Programs: A Modified Delphi Consensus Process in Clinton J Daniels, DC, MS, Zachary A Cupler, DC, MS, Jason G Napuli, DC, MBA, Robert W Walsh, DC, Anna-Marie L Ziegler, DC, MM, MS, Kevin W Meyer, DC, Matthew J Knieper, DC, Sheryl A Walters, MLS, Stacie A Salsbury, PhD, RN, Robert J Trager, DC, Jordan A Gliedt, DC, Morgan D Young, DC, Kristian R Anderson, DC, MS, Eric J Kirk, DC, Scott A Mooring, DC, Patrick J Battaglia, DC, David J Paris, DC, Amanda G Brown, DC, Justin M Goehl, DC, MS, and Cheryl Hawk, DC, LMT, PhD in Global Advances in Integrative Medicine and Health
Supplemental Material
Supplemental Material - Development of Preliminary Integrated Health Care Clinical Competencies for United States Doctor of Chiropractic Programs: A Modified Delphi Consensus Process
Supplemental Material for Development of Preliminary Integrated Health Care Clinical Competencies for United States Doctor of Chiropractic Programs: A Modified Delphi Consensus Process in Clinton J Daniels, DC, MS, Zachary A Cupler, DC, MS, Jason G Napuli, DC, MBA, Robert W Walsh, DC, Anna-Marie L Ziegler, DC, MM, MS, Kevin W Meyer, DC, Matthew J Knieper, DC, Sheryl A Walters, MLS, Stacie A Salsbury, PhD, RN, Robert J Trager, DC, Jordan A Gliedt, DC, Morgan D Young, DC, Kristian R Anderson, DC, MS, Eric J Kirk, DC, Scott A Mooring, DC, Patrick J Battaglia, DC, David J Paris, DC, Amanda G Brown, DC, Justin M Goehl, DC, MS, and Cheryl Hawk, DC, LMT, PhD in Global Advances in Integrative Medicine and Health
Footnotes
Acknowledgements
Our sincere gratitude to project coordinator Cathy Evans for managing panelist, consents, blinding data, and general organizational efforts. We would also like to thank the Delphi panelist for their participation and expertise: Shery Assal, DC, TPS, NBC-HWC; Gina M. Bonavito-Larragoite, DC, MBA, FIAMA; Wren M. Burton, DC, MPH; Michael B. Clay, DC, MPH; Jesse C. Cooper, DC; Andrew S. Dunn, DC, MEd, MS; Jonathon Egan, DC, MPH, PhD; Stanley Ewald, DC, MPH, MEd; Bart Green, DC, MSEd, PhD; Stephanie M. Halloran, DC, MS; Nathan Hinkeldey, DC, DACRB; Valerie Johnson, DC, DABCI, DACBN; Robert C. Jones, DC, APC; Jeffrey Kamper, DC, MHPE, DCBCN; Jeff King, DC, MS; Matthew H. Kowalski, DC; James Joseph Lehman, DC, MBA, DIANM; Anthony J. Lisi, DC; Michele Maiers, DC, MPH, PhD; K. Sean Mathers, DC, DPT; Jude A. Miller, DC, MS, CCSP; Ryan D. Muller, DC, MS; Ian Paskowski, DC; Charles W. Penza, DC, PhD; Charles R. Portwood, DC, RMSK; Morgan R. Price, DC; Lindsay Rae, DC; Alec L. Schielke, DC; Dean Smith, DC, PhD; Carina A. Staab, DC, MEd; Samuel Staula, DC; John S. Stites, DC, DACBR, DACO; Stephanie Sullivan, DC, PhD; William Tellin, DC; Holly A. Tucker, DC, MPH, CHES; Timothy J. Williamson, DC, MS. We also thank participants from our in-person workshop at the WFC ACC 2022 education conference.
Author’s Note
Portions of this work were presented at the World Federation of Chiropractic Association of Chiropractic Colleges Education Conference (Logan University, Chesterfield, MO, USA) in November 2022, and a Rehabilitation Medicine department meeting at University of Washington in July 2023, and the International Congress on Integrative Medicine & Health conference (Cleveland, OH) held in April 2024. 95
Author Contributions
JN was the primary investigator, participated in concept development and planning, workshops, draft competency statement generation, and attained Institutional Review Board approval. CD co-drafted this manuscript, secured funding, participated in project planning, workshops, literature search development, oversaw extraction, generated draft competency statements and analyzed data. ZC co-drafted this manuscript, participated in project planning, workshops, literature search development, and generated draft competency statements. RW participated in project planning, workshops, draft competency statement development. SW developed search strategy and carried out the search. AZ screened and extracted articles, participated in draft competency statement development. KM screened articles and participated in draft competency statement development. MK extracted articles and generated draft competency statements. CH analyzed data, provided modified Delphi methodology expertise, and participated in draft competency statement generation. SS, MY, KA, PB, AB, JAG, JMG, EK, SM, DP, and RT all provided expertise and participated in draft competency statement generation. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted with financial support from Clinical Compass (formerly Council on Chiropractic and Guidelines Practice Parameters).
Ethical Statement
Other Disclosures
CD, DP, SM, CH are board members for Clinical Compass, CD is a member of the Washington State Health Technology Clinical Committee. KA is on the Board of Governors for the American Chiropractic Association.
Disclaimers
The contents of this study are solely the responsibility of the authors and do not necessarily represent the official views of affiliate institutions, Veterans Health Administration, Department of Defense, or the U.S. Government.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.