
Abstract
Background/Objective
Few Spanish mindfulness interventions have been evaluated in Latinx patients with cancer. We culturally adapted a mindfulness intervention for Spanish speaking Latinx patients. The objective was to measure feasibility and acceptability as primary outcomes, with changes in anxiety, depression, and sleep as secondary outcomes.
Method
Spanish-speaking Latinx patients with breast cancer (n = 31) were randomized, between April 2021 and May 2022 to either intervention or wait-list control groups. The mindfulness intervention consisted of 6-weekly 1.5-hour sessions remotely delivered by a novice facilitator. Cultural adaptations included language, metaphor, goal, concept, trauma informed, and acknowledgement of spirituality. Feasibility was benchmarked as 75% of participants attending their first session, 75% of participants completing 4 of 6 sessions, and scoring ≥ 4 on a 5-point Likert feasability scale measuring ability to implement changes after 6-weeks. Acceptability was measured as scoring ≥ 4 on a 5-point Likert scale measuring usefulness and relevance of the mindfulness intervention for each session. An intention-to-treat, linear mixed model with repeated measures analysis examined changes in anxiety, depression, and sleep at week 6 and 18 (3 months post intervention).
Results
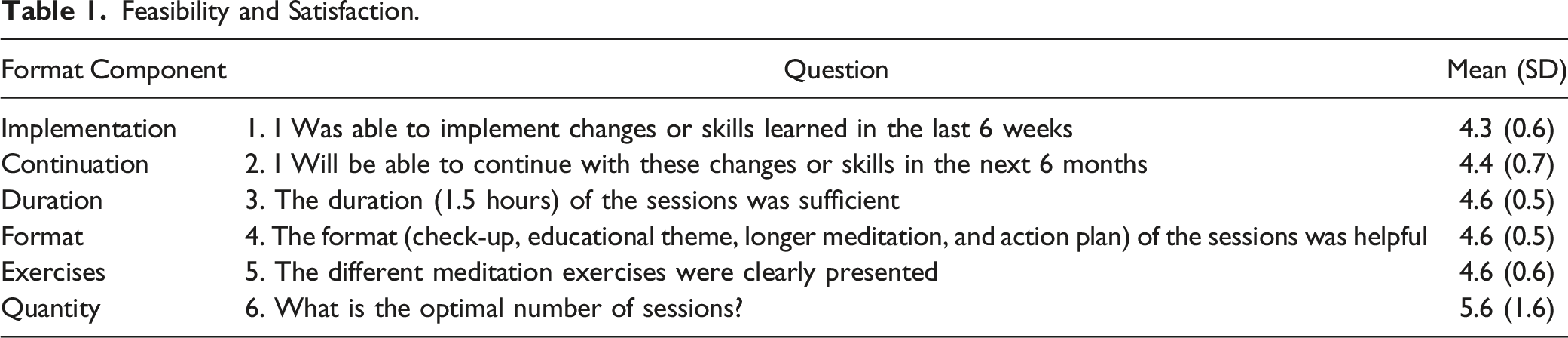
All three feasibility benchmarks were met with 75% of first session attendance, 96% of participants completing 4 of 6 sessions, and 94% scoring ≥ 4, on the feasibility scale (Mean (SD) = 4.3 (0.6)). Acceptability scores for both usefulness and relevance questions were ≥ 4 across all 6 sessions. Anxiety was significantly reduced at 3 months (−3.6 (CI -6.9, −0.2), P = .04), but is of unclear clinical significance given the small change. Depression scores declined, but not significantly, and there were no changes in sleep.
Conclusion
This culturally adapted, remotely delivered mindfulness intervention using a novice facilitator was acceptable and feasible and demonstrated associated reductions in anxiety amongst Spanish speaking Latinx patients with breast cancer.
Trial Registration
ClinicalTrials.gov ID# NCT04834154.
Background
One in ten Latinx women will be diagnosed with breast cancer 1 and are often diagnosed at a later stage compared to non-Latinx White women. 2 Tumors are more aggressive and survival rates are lower in Latinx patients compared to white non-Latinx patients with cancer. 3 The prevalence of depression and anxiety in Latinx women compared to non-Latinx White women with breast cancer is significantly higher 4 and can persist throughout the course of their treatment causing patients to sub-optimally participate or abandon treatment.5,6 These rates of mental health disparities are also accompanied by disparities in treatment rates for Latinx patients.
While equal numbers of Latinx and non-Latinx white patients with breast cancer reported needing psychosocial services, non-Latinx white patients had more frequent psychosocial visits despite Latinx patients preferring non-pharmacological management (Costas-Munoz, 2017). Mindfulness based interventions (MBIs) are an innovative non-pharmacological alternative for depression and anxiety. In the general population, MBIs reduce anxiety and depression. 7 Additionally, a 6-week MBI program, Beyond Stress, developed for primary care patients, was associated with significant reductions in anxiety (GAD-7 score reduction, P < .0001) and depression (PHQ-9 score reduction, P < .0001). 8 This program transitioned to a telemedicine format during the COVID-19 pandemic and demonstrated good feasibility and acceptability. 9 MBIs also reduce anxiety and depression among cancer patients10,11 and specifically breast cancer patients.11,12 Amongst breast cancer patients, MBIs also improve sleep. 13 Remote MBIs for breast cancer survivors reduce depression and anxiety symptoms supporting remote delivery of MBI programs’ feasibility and acceptability. 14 Finally, national recommendations for MBI’s for adult cancer patients in active treatment with anxiety and depression are now established. 15
Mindfulness based interventions (MBIs) delivered in Spanish across Spain, Latin America, and the US reduce stress, depression, and psychiatric distress at moderate to large effect sizes. 16 Spanish MBIs are comparable to English MBI’s in reducing depression and increasing levels of mindfulness. 17 Spanish MBIs for patients with breast cancer demonstrate reduced depression 18 and stress. 19
However, Latinx engagement in MBIs is significantly lower than for non-Latinx White patients. 20 This may be due to implementation barriers in Latinx communities such as Spanish speaking facilitators and/or material, 21 and the time and cost associated with instructor training. 22 Delivery of MBIs in community-based settings may reduce barriers to engagement, 23 and increase access to mental health services. 24 For example, health care staff trained as a novice MBI facilitator at a community based federally qualified clinic had comprable reductions in depression compared to an experienced MBI facilitator. 22 These community-based studies using novice facilitators across diverse populations highlight a potential mechanism to increase engagement and reduce mental health disparities.
Engagement may also improve by implementing specific cultural adaptations when delivering MBIs in diverse populations. 25 These factors include reduced duration of formal practice which could accommodate long working hours or multiple medical and family obligations, and encouraging mindfulness focused on the body given ease of adaptation by Latinx populations. 25 Given the importance of faith and religion in the Latinx community, being aware of participants’ religious preference and emphasizing the common theme of contemplative practice in MBI’s is also an important cultural adaption. 21
As modifications are made to MBIs focused on increasing engagement in diverse populations, evaluation of the MBIs, and not assuming cultural appropriateness across populations, will be important. 26 One evaluation method is measuring feasibility. MBI feasibility has been measured in various forms including evaluation of recruitment rates, 27 consent and retention rates, 27 and the number attending at least 4 out of 6 or 8 sessions.27,28 Benchmark feasibility rates have been reported at 75%. 28 Another MBI evaluation measure is acceptability. Acceptability has been measured by evaluating program satisfaction, usefulness, relevance to cancer patients and likelihood to recommend the program.28,29 Measuring adoption of a mindfulness practice or other behavioral change after the MBI training has also been used to evaluate acceptability. 27 Acceptability benchmarks have been set at ≥ 4 on a 1-5 point Likert scale. 28
The primary objective of the current study was to evaluate the feasibility and acceptability of a culturally adapted MBI known as Más Allá del Éstres (Beyond Stress), delivered in Spanish by a community health worker in a community-based organizations for Spanish speaking Latinx patients with breast cancer. The secondary objective was to evaluate the impact of Más Allá del Éstres on changes in anxiety, depression, and sleep.
Methods
This one-year pilot randomized controlled trial was based in San Jose, California in partnership with Latinas Contra Cancer (https://www.latinascontracancer.org/), a community-based organization that provides support for the Latinx community dealing with cancer. This study was approved by the Stanford University Panel on Medical Human Subjects (IRB #57111). Signed consent was obtained from all participants. A Consort Statement for reporting group randomized trials can be found in Supplement 1. 30
Design
Eligible participants were randomized to either a mindfulness intervention or wait-list control group. Block randomization was implemented, with random block sizes of two, four, and six. We prepared the random allocation sequence table stratified by the block factor of endocrine (y/n) before the enrollment and allocated the enrolled participants in sequence based on the table. The allocation sequence was generated by the project statistician, and participants were enrolled and assigned to the wait-list control or intervention groups by the project research coordinator. The block randomization with variable block sizes was applied to increase unpredictability of the blocks, and as such the statistician and co-PI of the study were blinded to randomization. The research coordinator, facilitator, and PI were not blinded due to their involvement in the implementation of the study. The wait-list control group was assigned to care as usual to make as few demands during the patients’ treatment regimen as possible, and to offer them the full intervention at time of study completion.
Outcome measurements were obtained at baseline, week 6 and 18 (3-months post intervention). Participants were compensated $25 for completion of outcome measurements at each time point. Recruitment terminated at the end of the grant period.
Participants
Spanish speaking Latinx patients with breast cancer were recruited between April 2021 and May 2022 from Latinas Contra Cancer, local and regional public medical centers and clinics, community non-profits, and social media via recruitment fliers, referral from treating medical providers, nurses, and social workers. Participants were eligible to join if they met the inclusion criteria: adults aged 18 or older, Spanish speaking, self-identified as Latinx, self-reported diagnosis of breast cancer and currently or within last 12 months in active treatment (surgery, chemotherapy, or radiation) or on endocrine therapy, self-identified anxiety (persistent worry or nervousness), depression (feeling sad, little interest or pleasure in doing things, or hopeless), or sleep disturbance. Exclusion criteria included: (1) other cancer diagnosis or breast abnormalities (ie, fibroadenoma, abnormal mammogram without a cancer diagnosis, patients with other non-breast cancers), (2) comorbid bipolar affective disorder or psychotic disorder (as self-identified by patient after asking “do you have any other psychiatric conditions”), (3) inability to physically or psychologically participate for 1.5 hours on zoom, or (4) patients currently participating in a stress reduction or mindfulness group or intervention.
Intervention
Más Allá del Éstres is a 1.5-hour weekly, 6-week remotely delivered synchronous intervention that was originally designed to be delivered in person and was transitioned and offered for remote delivery due to the COVID-19 pandemic. The remote group format included: (1) a short breathing meditation, (2) individuals sharing their previous week’s meditation practice, stressors, and behavioral goals (‘check-ins’), (3) an educational topic, (4) a longer meditation, (5) review of the meditation practice experience, and (6) development of individual behavioral goals for the subsequent week.
Weekly educational topics included (1) identifying and defining stress, (2) identifying stress symptoms, (3) describing the stress response, (4) meditation types and benefits, (5) barriers to meditation, and (6) lifestyle interventions (exercise, diet, social support). As part of the weekly educational discussions, participants were asked to share their stressors, symptoms of stress, beliefs and definition of meditation, barriers to meditation, and describe other behavioral activities that help manage their stress.
The weekly meditation practices included (1) mindful breathing, (2) body scan, (3) guided imagery, (4) self-compassion, and (5) two gratitude meditations. Sessions were held 6-7:30 PM weekday afternoons or 10-11:30 AM weekend mornings to accommodate working schedules and medical appointments.
The PI attended all sessions to ensure fidelity of the program.
Cultural Adaptation
Several cultural adaptations 31 were made from the original English version of the intervention. Language adaptation was achieved by first translating the intervention into Spanish and then back translating into English with the research team (one from Central America and two of Mexican descent, all with Spanish as their first language). Our intention was to accommodate participants’ diverse educational levels and dialects. Metaphor adaptation was addressed in sessions 1 and 2. In these sessions, participants were asked to share their own stressors (session (1) and symptoms of stress (session (2) to accurately represent the cultural context. Goal adaptation was achieved by attempting to accommodate busy schedules including family caregiving, work, and treatments. Participants were encouraged to use shorter interventions (gratitude lists, taking 5 deep breaths) in times of stress, in addition to a more formal daily practice. Concept adaptation included understanding the importance of family (familismo) in the Latinx community. 32 Familismo was acknowledged by encouraging participants to develop their own practice so they could be more available for family relationships and activities. Understanding the prevalence of trauma in the Latinx community,33,34 a trauma informed meditative practice was encouraged that acknowledged physical sensations and encouraged mindfulness techniques that did not induce anxiety (ie, meditating with variety of postures such as sitting or standing, using a soft gaze with eyes open, focusing on external stimuli and not the breath, trying movement mediation such as a 5-minute YouTube yoga instead of a sitting meditation). Finally, given the importance of spirituality and faith in the Latinx community, 35 during week 4 discussions of meditation, we acknowledged meditation could be a form of contemplation and reflection. As such meditation could be available to those with a spiritual practice as well as those without.
Facilitator Training
The study facilitator was a community health advocate. Training included reviewing the English curriculum in one-hour sessions with the PI, then attending a 6-week English Beyond Stress program led by the PI. After each weekly session, post-session reviews of the material were conducted with the PI. The facilitator also attended a virtual Facilitator Training series through the Integrative Center for Group Medical Visits (https://www.icgmv.org/). Finally, the facilitator was encouraged to develop their own mindfulness practice.
Outcomes
Demographic data included age, date of diagnosis, and stage of treatment (diagnosed, but not yet started treatment, active treatment [surgery, radiation, chemotherapy], or endocrine therapy]).
Feasibility benchmarks were set as (1) 75% of participants attending a first session, (2) 75% of participants completing 4 of 6 sessions, and (3) scoring ≥ 4 on a single item of the study Feasiblity and Satisfaction scale (“I was able to implement changes or skills learned over the last 6 weeks”) administered at week 6, and scored using a 5-point Likert scale ranging from “Not at All Useful (1)” to “Very Useful (5)”. Higher scores represented greater feasibility.
Acceptability benchmark was set as scoring ≥ 4 on a two-item Acceptability scale (“This session was useful”, and “This session was relevant to my life or situation”). Items were rated using a 5-point Likert scale ranging from “Not at All Useful (1)” to “Very Useful (5)”. Higher scores represented greater acceptability.
Anxiety was evaluated using the Generalized Anxiety Disorder-7 (GAD-7), a seven-item self-administered questionnaire.
36
The seven-item scale Likert scores are “not at all (0)”, “several days (1)”, “more than half the days (2)”, and “nearly every day (3)”. Scores range from 0 to 21 with higher scores indicating higher levels of anxiety. Scores
Depression was measured using the Center for Epidemiological Studies –Depression (CES-D) self-administered questionnaire.
37
The twenty-item scale Likert scores are “rarely or none of the time (0)”, “some or little of the time (1)”, “moderate or much of the time (2)”, and “most or almost all the time (3)”. Scores range from 0 to 60 with higher scores indicating greater depressive symptoms. Scores
The Participant-Reported Outcomes Measurement Information System (PROMIS) Adult Short Form: Sleep Disturbance (PROMIS-SD), is an eight-item scale examining sleep quality, disturbances, and satisfaction for the past seven days on a 5-point Likert scale with scores ranging from one to five. Raw scores were converted into t scores ranging from 28.9 to 76.5, with higher scores indicating greater sleep disturbance. 38
IT Support
Participants were called a week prior to the start of the first session to verify receiving the zoom links, ability to log onto zoom platform, and answer questions regarding the remote platform. Weekly reminders with zoom links were texted for the remaining sessions. Text containing links to assessments were sent to participants weekly for acceptability, week 6 for feasibility, and week 6 and 18 (3-month post-intervention) for the secondary outcomes questionnaires. Additionally, research staff facilitated completion of online assessments by calling and reviewing verbally over the phone when preferred by participants.
Analysis
SAS statistical software was used to generate the random allocation sequence.
Feasibility and Acceptability mean scores and standard deviations were computed at week 6 and weekly, respectively.
The analyses of the between-group differences for the secondary outcomes included all participants with follow-up data at week 6 and 18. Participants were analyzed based on the group to which they were assigned. Tests of group × time interactions in repeated-measures mixed-effects linear models were performed. The fixed effects of each model included baseline value of the outcome, treatment stage, group (intervention or control), time point (week 6 or 18), and group × time interactions. The random effects accounted for repeated measures with a compound symmetry covariance matrix.
All analyses were conducted using SAS version 9.4 (SAS Institute Inc). Statistical significance was defined as a 2-sided P value <.05.
Sample Size
The trial was powered on the co-secondary outcomes-GAD-7 and CES-D. A sample of 20/arm had 80% power to detect a standardized 1.12 mean difference (Cohen’s d) between the intervention and control groups at α = 2.5% (2-sided), assuming at least 85% retention at 6 weeks based on our prior data 8 and other similar studies. 39
Results
Thirty-one participants were randomized. After randomization, one participant in the control group withdrew after consenting due to personal reasons (Figure 1). Sixteen participants were randomized to the intervention group, and fourteen participants were randomized to the wait-list control group. Four individuals from the control group and five from the intervention group were in active cancer treatment. Additionally, ten participants in the control group and eleven in the intervention group were receiving endocrine therapy. The analysis was by original assigned groups. Flow diagram outlining the sequential steps in a community mindfulness based intervention for Spanish speaking patients with breast cancer. Inclusion criteria were 18 years or older, Spanish speaking, self-identified as Latinx, self reported diagnosis of breast cancer and currently or within last 12 months in active treatment (surgery, chemotherapy, or radiation) or on endocrine therapy, self-identified anxiety, (persistent worry or nervousness), depression (feeling sad, little interest or pleasure in doing things, or hopeless), or sleep disturbance.
The mean age (SD) was 51.5 (8.0), and all participants were Spanish speaking Latinx patients with breast cancer. Baseline anxiety and depression scores were higher in the control group compared to the intervention group despite randomization (mean [SD] for intervention vs control: 6.8 [4.3] vs 9.8 [4.8] for GAD-7, and 14.4 [8.7] vs 22.9 [17.4] for CESD-R score).
Feasibility and Satisfaction.
Acceptability.

Secondary Outcomes.

Abbreviations: GAD, generalized anxiety disorder; and CESD-R, Center for Epidemiologic Studies Depression Scale (CESD)- Revised.
aAdjusted analysis for intervention vs control: the adjusted difference in means and their 95% CIs were obtained from the linear mixed model. Mixed-effect models that accounted for random effects of repeated measures were adjusted for baseline of the outcome of interest and treatment stage.
bGAD-7 score, total scores of the 7 items ranging from 0 (no symptoms) to 21 (most severe symptoms).
cCESD-R score, total scores of the 20 items with a range of 0 (not depressed at all) to 60 (extremely depressed) after converting score = 4 to score = 3 for each item.
dSleep disorders T-score, a population-based scale ranging from 25 (not at all) to 80 (extreme disturbance) converted from the crude total score of the 8-item questionnaire. A score of 50 represents the average of the calibration sample that was generally most enriched for chronic diseases.
Discussion
This pilot study of a culturally adapted Spanish MBI, delivered in a community-based setting by a community health worker was feasible and acceptable in Latinx women with breast cancer. The high satisfaction findings could relate to the cultural congruence of this MBI for Latinx populations. Additionally, women who engaged in the MBI experienced significantly greater improvement in anxiety symptoms compared to women in the control group at three months. The reduction in anxiety symptoms of 3.6 points represents a clinically mild reduction in symptoms. Women who participated in the MBI also experienced a reduction in depressive symptoms compared to the control group, although it was not statistically significant. There were no differences in sleep disturbance between women who took part in the MBI and women in the control group.
Many cultural adaptations, including language, metaphor, goal, and concept adaptations16,40 were made from the original English version of the MBI. Language adaption was addressed as we translated the intervention into Spanish with consideration of different Spanish dialects and participant educational levels. By asking participants to describe their own stressors and symptoms of stress in sessions 1 and 2, we gained metaphor adaptation. Our goal adaptation was to be conscious that participants had many obligations and would have little time to meditate, so we encouraged recognizing the stress and using short interventions (creating gratitude lists or taking five deep breaths during treatments or other times of stress) in addition to encouraging a regular daily mindfulness practice. Concept adaptations included acknowledging familismo or importance of the family, while still encouraging participants to take time to meditate and care for themselves so that they could be more present for their families. Acknowledging spirituality also facilitated concept adaptation making meditation available to those with and without a spiritual practice. Assuming some participants had experienced trauma either from medical treatment, immigration, or social situations, we also encouraged participants to find comfortable forms of meditative practices that did not induce panic or anxiety (meditating with soft gaze or using movement meditations). These adaptations to the intervention, we believe, provided the cultural congruence needed to successfully implement in the Latinx community.
In addition to these cultural adaptations, the intervention met several criteria for an equitable mindfulness program including accessibility, inclusivity, knowledge sharing and acknowledgement of different perspectives. 23 Accessibility was impacted by providing the intervention at no cost to participants and recruiting from a variety of community-based clinics, nonprofits, and county hospitals. Inclusivity was met by our diverse recruitment across many community-based organizations and not limited to patients in large hospital settings. Equitable mindfulness also requires knowledge sharing and increased awareness. Knowledge sharing of the intervention included providing psychoeducation on stress, mechanisms of stress and meditation, increasing awareness of both the effects of stress and meditation on the body and illness. Knowledge sharing was also a key component of the weekly ‘check-ins’ allowing participants to share their own stories including their stress, illness, treatments, and mindfulness practices over the preceding week. During these weekly check-ins, participants shared knowledge regarding not only barriers and difficulties but also successes to developing a mindfulness practice. This was also a time participants could witness and acknowledge different perspectives of living and managing both the cancer and associated stress. Using different mindfulness meditations across the six sessions enabled participants to have increased awareness of various practice types. We believe the cultural adaptations along with the strong feasibility and acceptability findings strengthen generalizability to other Latinx cancer populations. Future studies are needed to determine if results will be generalized to non-cancer Latinx populations.
The significant reduction in anxiety at three months is consistent with other MBIs,41,42 but given the small clinical change warrants further evaluation in studies with larger samples. Previously reported sustained effects on anxiety have not correlated with levels of mindfulness at follow-up 42 suggesting other mediating factors. In the current study, confidence in maintaining their practice is a potential mediating factor, as participants highly rated their ability to continue changes made or skills learned in the subsequent six months (mean 4.4 [SD 0.7]. This transition to action and potentially maintenance stages of change are best achieved with social support and exposure to others who have successfully made changes 43 both situations are found in group MBIs. Another potential mediating factor is stress resilience. 44 Participants reported increased ability to recognize stress and implement adaptive behavioral changes (breathing prior to procedures or when anxious) (personal reports during group weekly review of their practice), but quantification of these behaviors is needed to evaluate the role of stress resilience as a mediating factor. Finally, decreased rumination 45 and increased self-compassion 46 are important proposed mediating factors for effectiveness of MBIs, and they warrant further evaluation in future studies.
This is the first study to our knowledge to train and employ a non-clinical, community health worker through a community-based organization. The current training protocol included many aspects of other MBI trainings, including (1) foundational training (personal engagement in a MBI program), (2) basic teacher training (personal experience in the context with which they will teach the MBI, and the pre- and post-session meetings with the PI), (3) advanced training (ongoing engagement in a regular supervision process with an experienced MBI teacher), and (4) continued professional development (evaluating MBI outcomes). 47 Additionally, a novice MBI facilitator training protocol, using several similar training components as the current study, found greater reductions in depression, functioning and stress compared to the experienced MBI facilitator in a under-resourced federally qualified community clinic. 22 Therefore, this model of training a non-clinical novice MBI facilitator, using clear structured protocols, may be a mechanism to increase MBIs in community-based organizations serving under resourced populations.
Transition from in person to a remote MBI program was necessitated by the COVID-19 pandemic. While there is high mobile internet use and interest in remote health services in the Latinx community, 48 several procedural modifications were made to support the current remote MBI program, including providing IT support prior and during the intervention to assist with session participation and completion of the assessments. Future studies and program implementation may benefit by providing similar technical support. Funding for mobile devices was not provided in the current study but may also increase feasibility in future studies.
There were several limitations to the study. The first limitation was a small sample size. While we anticipated recruiting forty participants, we were able to successfully recruit thirty-one. We believe the disproportionate impact of the COVID-19 pandemic on the Latinx community 49 may have contributed. Our community partner noted a change in requested services during the pandemic from medical case management and behavioral health support to case management for housing and food insecurity. This shift in community priorities may have also affected interest in a behavioral health intervention. A methodological limitation is the lack of blinding to the intervention and wait-list control groups by the participants, facilitator, and lead PI. This could potentially overestimate the effects of the intervention. 50 Another limitation is disproportionately higher rates of depression, anxiety and sleep disturbance in the control compared to the active intervention group, despite randomization. Larger sample sizes in future studies will be needed to avoid similar distribution of outcome measures at baseline. Finally, the training protocol may not be adoptable in all community-based organizations due to time and resources needed to train. However, we designed the training protocol involving the CHW specifically to facilitate generalizability to other similar organizations. Future evaluations of shorter protocols are important. These protocols will need to evaluate not only different training procedures, but also types of personnel best suited to function as facilitators. Despite these limitations, the intervention was not only feasible and acceptable, but demonstrated a significant reduction in anxiety at 18 weeks.
Finally, there are several clinical implications from the current study increasing applicability of the intervention and protocol. First, many cultural adaptations were made to facilitate engagement by Spanish speaking Latinx participants, increasing the ability to deliver more behavioral health services to this underserved population. Second, components of the intervention were evaluated by the participants (via the Feasibility and Acceptability surveys) to determine if any structural or contextual changes were recommended. The current format is acceptable and may be implemented in other settings with similar patient populations. Third, the study adds to the limited research evaluating novice MBI facilitators. As utilization of novice facilitators can increase access of behavioral health services to underserved communities, further research is warranted. Fourth, the remote format allows for participation despite transportation and remote location barriers. Fifth, this is the first study to our knowledge demonstrating MBIs delivered through a community non-profit and facilitated by a community health worker are feasible and acceptable, increasing the potential of non-clinical settings to provide much needed behavioral health services.
Conclusion
The 6-week MBI, Más Allá del Éstres, was feasible and acceptable in Spanish speaking Latinx women with breast cancer when delivered remotely, using a novice MBI facilitator. Anxiety levels also significantly reduced after 18 weeks. These findings are encouraging for addressing mental health disparities in Spanish speaking Latinx populations with cancer. Larger randomized control trials are needed to further evaluate changes in mental health outcomes.
Supplemental Material
Supplemental Material - A Randomized Controlled Trial of a Culturally Adapted, Community-Based, Remotely Delivered Mindfulness Program for Latinx Patients With Breast Cancer is Acceptable and Feasible While Reducing Anxiety
Supplemental Material for A Randomized Controlled Trial of a Culturally Adapted, Community-Based, Remotely Delivered Mindfulness Program for Latinx Patients With Breast Cancer is Acceptable and Feasible While Reducing Anxiety by Maria Juarez-Reyes, Erica Martinez, Lan Xiao, and Lisa Goldman Rosas in Global Advances in Integrative Medicine and Health.
Footnotes
Acknowledgements
The authors would like to thank Nancy Villarreal for her dedication, commitment, and partnership with the study investigators. We thank Latinas Contra Cancer for their partnership and dedication to this underserved population of patients with cancer. A special thank you to all the participating community hospitals and clinics for their generous referral of patients and commitment to serving this population. Finally, to our participants, thank you for your commitment to change, interest in the intervention and generous advice for dissemination.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was support by an Innovation Award from the Stanford Cancer Institute, a NCI-designated Comprehensive Cancer Center.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.