
Abstract
Background
Chronic low back pain is globally prevalent and associated with significant impairment in quality of life. Furthermore, people from historically marginalized communities are less likely to receive treatment, contributing to health inequities. Group mindfulness-based interventions improve pain and function, and virtual delivery has been demonstrated to be feasible. Little is known about how participants experience the virtual delivery of mindfulness-based interventions, especially participants from historically marginalized communities.
Objective
This study explored participant perspectives of a virtual mindfulness-based group medical visit for people with chronic low back pain.
Methods
Participants were recruited from the intervention arm of OPTIMUM, a study of virtual medical group visits using an adapted Mindfulness-Based Stress Reduction program for chronic low back pain. Semi-structured exit interviews were examined, and reflexive thematic analysis was used to compose key themes.
Results
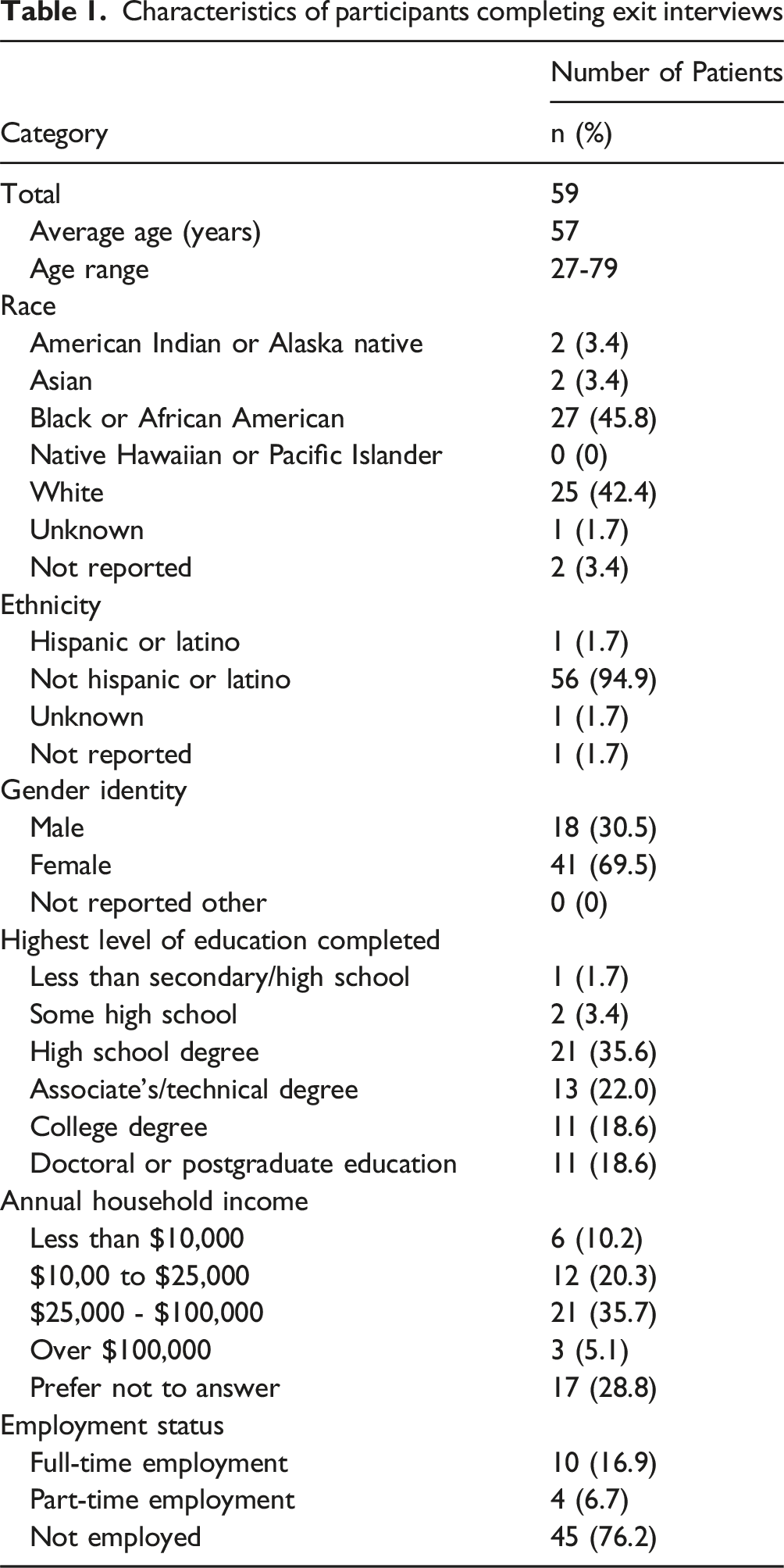
Interviews from 59 participants (mean 56 years, 69.5% women; 45.8% Black or African American) were examined. Two major themes were derived from analysis. The first theme was ‘effects of the external environment,’ ie, the physical location from which the participant engaged with the session. The subthemes were comfort, social demands in the home setting, and sharing personal spaces. The second theme was ‘navigating the virtual platform.’ Subthemes were ease, struggle, and levels of support.
Conclusion
Patient experiences varied substantially during the virtual mindfulness-based group medical visit intervention and this variation was influenced by social determinants of health. The key themes bring attention to the effects of the external environment and the technology itself on participation for people from historically marginalized communities. Basic tenets of mindfulness, such as present state awareness and equanimity, can provide a structure within which to navigate virtual participation amid home environments. Future studies are needed to explore differences in virtual and in-person mindfulness programs and to adapt virtual mindfulness programs.
Clinicaltrials.gov ID number
NCT04129450.
Introduction
Chronic low back pain (cLBP) is one of the most common pain conditions globally, affecting 619 million individuals, and it is associated with significant impairment in quality of life. 1 Furthermore, mechanisms underlying chronic pain are poorly understood and strictly biomedical therapies have demonstrated limited efficacy. 2 Integrative therapies, including mindfulness-based interventions (MBIs), can improve pain and function for patients with chronic pain, including chronic low back pain.3-5 Despite this demonstrated efficacy, many people with cLBP have limited or no access to MBIs. 6 Structural and societal factors like income inequality, and disparities in healthcare access and infrastructure may limit the reach of this effective therapy in target populations. 7 Patients in rural communities, Black people and people with lower incomes suffer a disproportionate burden of chronic pain and undertreatment of chronic pain. 8 Low socioeconomic status is also associated with a higher burden of chronic pain.9,10 Introducing MBIs into primary care settings could improve treatment of chronic pain, particularly among historically marginalized communities. Integrative group medical visits are an important model for treatment of chronic pain. In this setting, patients benefit from peer learning, social support, and clinician access.11-13 Moreover, this type of clinical encounter is covered by most insurers. Many benefits have been linked to the group medical visit model, including improved patient and provider satisfaction.14,15
Videoconferencing is an integral part of clinical care and health education in the post-COVID-19 pandemic era, and MBIs are feasible in virtual settings.16,17 As telehealth is now fully integrated into most healthcare settings, it is important to understand how this model affects participant experience. Evidence to date suggests participation in synchronous virtual group MBIs can improve mental health symptoms in adult populations18-20 and improve pain outcomes 30 days postoperatively. 21 People with chronic pain conditions may perceive virtual interventions as more accessible due to the challenges of seeking care when chronically ill.22,23 However, factors such as variable digital access and literacy, differences in acceptability, and concerns about privacy may affect experiences and outcomes. 24
Research is needed to inform the design, implementation and evaluation of virtual mindfulness-based group medical visits. From a health equity lens, group visits provide improved access to medical care, education, and peer support for low income and historically marginalized communities, who are more likely to experience worse outcomes from chronic pain. 25 To equitably increase access to MBIs, it is necessary to learn more about how people, especially those from historically marginalized communities, experienced this intervention in the virtual setting.
Using reflexive thematic analysis of post participation interviews, the study explored the experiences of participants with cLBP who were learning adapted Mindfulness-Based Stress Reduction (MBSR) 26 in a videoconference-based (ie, virtual) group medical visit format. A framework was developed to evaluate how differences in experience correlate with social determinants of health at multiple levels of the intervention (See Table 2).
Methods
Study Design
This qualitative study was part of Optimizing Pain Treatments In Medical settings Using Mindfulness (OPTIMUM) and was approved by a single Institutional Review Board, the University of Pittsburgh Institutional Review Board STUDY20110378. OPTIMUM is an ongoing pragmatic randomized controlled trial investigating the effect of an adapted MBSR intervention, vs usual primary care, on pain and function among primary care patients with cLBP. 27 The intervention entails an 8-week virtual group medical visit led by an experienced, trained MBSR instructor alongside a primary care clinician. The intervention was delivered over the Zoom platform (Zoom version 1.8.0.2305) from November 2021 to April 2024. The standard MBSR program was adapted to include brief visits with a healthcare provider via a private breakout room within each 2-h session, chair-based mindful movement, and, unlike traditional MBSR programs, did not include a retreat day. Guided mindfulness meditation audio-recordings were made available to participants for home practice. In addition, the 8 weekly sessions were each 2 h long and included time to accommodate individual breakout-room meetings with the primary care provider. This is distinct from the standard MBSR curriculum, which is 2.5 to 3 h long.
Participants were encouraged to identify a quiet, private, and regular space from which to establish their virtual connection. Earphones, tablets, and support for connectivity were available to facilitate participation. In addition to a brief introductory and technical troubleshooting session, staff were available to call and walk participants through the log-on in real time at the start of the session or in case of lost connections. Video participation was encouraged but not required for participants. Mindfulness instructors and clinicians remained on camera throughout the sessions and participants were reminded to turn their cameras on if they were able. However, they were not required to do so. Due to technical limitations, some people attended via audio connection or phoneline only. These within group intervention variations were consistent with the pragmatic clinical trial design that asks whether the intervention can work under usual conditions vs an explanatory trial that asks whether the intervention works under ideal conditions. 28
Participants in the OPTIMUM intervention were invited to complete an optional post-intervention one-on-one interview. As part of these semi-structured exit interviews, participants were asked about their experience of the virtual aspect of the mindfulness intervention (see Appendix A).
Study Population
English-speaking, non-pregnant adults with chronic low back pain were recruited from primary care practices including one Federally Qualified Health Center in central North Carolina and three academic health systems from Pittsburgh, Pennsylvania, Boston, Massachusetts and Chapel Hill, North Carolina. 27 People with worsening pain, or unexplained fever or weight loss during the past month, and people with metastatic cancer were excluded from the OPTIMUM trial.
Data Collection
Groups ranged in size from 4 to 13. Upon completion of the group, OPTIMUM intervention participants were contacted by phone, text or email by the research teams and invited to participate in audio-recorded virtual semi-structured exit interviews via teleconference platform. Given the size and multi-site design of the trial, it was more pragmatic for each site to identify their own interviewers. Interviewers utilized a common interview guide to help minimize bias. Interviews were conducted by 4 female MDs, one male MD, and one DrPH all of whom were trained in semi-structured interview techniques. Interviewers’ self-identified racial identities included: Mixed Race, Black or African American and White, and White. Their self-identified ethnic identities included: Latina, Hispanic, and Non-Hispanic. Some interviews included a second researcher who was training to conduct interviews. Some participants had a working relationship with these interviewers throughout the enrollment and intervention process. Interviews at one site were conducted by an independently contracted qualitative research center. Interviewers followed a pilot-tested guide that included prompts to describe participants’ experience in the program, their expectations about the program, their use of mindfulness skills in daily life, their motivations to continue to participate in the sessions, and their feelings about the virtual group format. For example, the guide included questions regarding the use of technology, facilitators and challenges, privacy concerns, and about having the clinician present (See Appendix A). Interviewers encouraged participants to speak openly about their experiences and informed them that de-identified feedback would be used to improve the program for future participants. Participants were compensated $50 for completion of the approximately 20-min interview. Most participants joined the virtual interview from a private space in their home. However, some participants joined from their work setting, car, or yard. In total, 59 participants provided exit interviews. The 59 interviews were transcribed verbatim, de-identified and uploaded to ATLASti (ATLASti version 7). Exit interviews were collected from 59 out of 122 participants. Transcripts were not returned to participants, and participants did not provide feedback on the findings, because there was concern about the frequency with which participants were already asked to provide data (monthly for 12 months).
Data Analysis
For this manuscript, the interview data were analyzed using a reflexive thematic analysis approach. 29 This approach was chosen as it is a flexible methodology that aims to identify patterns of shared meaning across participants’ experience, while also recognizing and valuing the influence of the researchers’ subjectivity in this process. We approached the data from a constructivist/interpretive standpoint. From this view, there is no one ‘reality’ to uncover, but rather, reality is dependent on interpretation. Thus, we acknowledge that the patterns of meaning identified here represent one of many ways to understand participant experience. Furthermore, due to this standpoint, we refrained from methods that aim to eliminate bias (eg, inter-rater reliability, data saturation) as these are not appropriate in a reflexive approach. For example, Braun has discussed the pitfalls of reporting inter-rater reliability and data saturation when utilizing reflexive thematic analysis. 30 Instead, we acknowledge the subjectivity and perspectives of the participants and the researchers and the role that this subjectivity plays in co-creating this analysis.
Initial rounds of coding were conducted by authors RR, JB, JLB, EH, CL, and IR, who developed a codebook containing 22 codes. This initial phase of analysis was described in detail in the manuscript, “Pragmatic approaches to team-based qualitative analysis of exit interview data in a pragmatic clinical trial.” 31 Then, analysts MGC, CL and JLB built their analysis upon this initial work.
JLB is a Family Medicine physician and researcher at a large academic research center who studies group-based interventions for chronic pain and post-COVID conditions. MGC is an academic Family Medicine physician embedded in a Federally Qualified Health Center with a specific interest in mind-body medicine, addiction care and chronic pain. CL is a former physician and current researcher who examines interpersonal relationships, mindfulness and self-compassion. Given that all 3 researchers had experience in clinical medicine, their perspectives regarding the clinician-patient relationship and healthcare communication influenced the analysis process. This included determining what data were meaningful to the research topic and what thematic groupings were most important.
Their coding process was iterative and included inductive coding (derived from the data) and deductive coding (derived from the interview questions). They began by analyzing segments of interviews coded as “virtual experience” and ultimately re-read the interviews and re-coded the segments relevant to research questions. Coders chose meaningful portions of text that appeared relevant to the research aims. Some codes were descriptive (eg, “convenience”), while other codes were latent (eg, “role strain”). We followed 6 steps as suggested by Braun and Clark. 29 (1) First, all 3 coders familiarized themselves with the transcripts by reading through them several times and creating reflective memos with observations for each transcript. (2) Next, coders applied codes to segments of text in a subset of 6 transcripts. The coders met to discuss coding and include diverse perspectives on code development. Coding continued for the remaining transcripts. (3) An initial set of themes were generated by going back and forth between the codes, selecting key quotes, and re-coding segments as needed as part of theme development. Discussions between the 3 coders and reference to their memos continued to play an important role in this process. (4) Themes were developed with attention to key quotes, and then (5) refined and defined through discussion. (6) The last step was manuscript development, with re-engagement with the transcripts to ensure quotes were placed in context. Finally, to enhance the quality of reporting, authors used the COnsolidated criteria for REporting Qualitative research (COREQ) checklist (Supplement 1). 32
Health Equity Framework
In seeking to understand the role of social determinants of health upon participant experience of virtual MBSR training, we drew heavily upon the research framework published by the National Institute on Minority Health and Health Disparities. 33 Our analysis utilized this structure to consider factors affecting participant experience by the domain of influence (social determinant) and the level upon which that domain exerts influence (individual to societal). Examples of these factors with relevant participant quotes are presented.
Results
Characteristics of participants completing exit interviews
Major themes and subthemes from reflective thematic analysis

Effects of External Environments
The first theme described the effects of the “real world” or physical space that each person inhabited during the mindfulness-based group medical visit. Most participants were in their home; however, a few joined the session from their yard, a vehicle or a public space. For some participants, location varied by week, adding uncertainty to the experience. The space either enhanced or detracted from each person’s ability to engage with the session. The subthemes were comfort, social demands, and sharing intimate spaces.
Comfort: “Just the Very Same in My Home”
Overall, participants valued the opportunity to connect from home. Participants’ social location affected their degree of comfort or ease with the virtual experience. For participants employed outside the home, and for whom private space at home was available, the virtual experience was often one of comfort and ease. For example, a participant noted, “I felt like I was in person, just the very same. But just to know that it was done to my convenience. After a long day at work, I was able to come home. I was able to be a part of the study, just the very same in my home, in my own space, and everything where I’m comfortable.” (35-year-old Black, Non-Hispanic female, ID 8)
An important component of the MBSR curriculum involves practicing meditation at home between classes since regular practice is associated with improved outcomes.
34
Providing instruction at home enabled participants to learn mindfulness in the setting where they would be practicing it. This participant explained, “If you think about it, you’re using the practice online and you’re in your own home and that’s where you’re going to practice it. So, it’s easier to apply instead of going to the office and [saying], ‘oh I’m gonna go home and try this.’” (44-year-old Black, Non-Hispanic female, ID 6)
Social Demands in Home Setting: “No One Would Let Me Have It”
By contrast, the home environment detracted from the experience in some cases. For some participants, the home lacked space, structure and/or privacy. This introduced a conflict between being present with others at home and engaging in the session. Participants’ social location affected their ability to create a home environment conducive to practicing mindfulness. Participants described attempting to set boundaries with family and friends and to remove themselves to private parts of the home, only to be interrupted by people asking for their help. These interruptions and caregiving duties were particularly prevalent during the early evening when the occupants and the functions of the home were shifting. This participant described attempting to isolate herself in one part of the home, only to be repeatedly interrupted by company: “I’d tell people I’m on Zoom -- and no one would let me have it. The company was turning over. [It’s just] the time of day … somebody would stop by and then run to the room.” (69-year-old Black, Non-Hispanic female, ID 27)
For participants in smaller living spaces with more occupants, it was not possible to find a private space. Some participants joined from outdoors or from their cars to find privacy. The time of day was particularly problematic for some participants: “[It] was at dinnertime and there was just too much confusion in the kitchen and that was really the only place I could go and sit.” (65-year-old White, Non-Hispanic female, ID 3)
Another participant described the challenge of prioritizing attention to the virtual session when interrupted by an in-person interaction. She could silence a phone call during a virtual session but turning away from an in-person interaction evoked loss. The moment juxtaposed what we expect to give and get in a virtual vs in-person interaction. “I can always look at my phone and say, ‘I think I can call you back later’, you know? But then somebody starts knocking at your door, that makes you stop and see who’s at the door, you know? … [They] might catch me off guard and we start talking about something and then lead to something else. And they’re more people coming in. Before you know it, I forgot what I was supposed to be doing for myself.” (60-year-old Black, Non-Hispanic female, ID 12)
Several participants described competing demands which they attempted to resolve by shifting attention between the home and the virtual session to meet expectations of both. One participant described the tension between her role as a homemaker and wife and her desire to attend the group from home: “I don’t really get to see my husband that much because of his job. And then he’s at home, and to him it’s like, “my goodness, why you going to be on the phone for such a time” … You know, I just hate to just close the door. [laughs] So, I was having my phone on mute, and unmute it and mute it, and unmute it. And I [said] to him ‘So, honey, this is a class I’m in. I’ll be off in a few minutes, baby. Give me time, okay. Your food is already fixed, and I’ll be off soon’. He’s really not used to that because he’s – when he comes home, I greet him at the door, and it just it wasn’t quite like that. [laughs]” (70-year-old Black, Non-Hispanic female, ID 30)
While participants would have weighed social obligations and opportunities against attendance in both in person and virtual training, the flexibility inherent in virtual encounters introduced more opportunities to weigh the benefits and costs of attendance. For example, this participant described getting caught up in a series of events that eventually resulted in her not attending the group. The participant’s quote illustrated the interconnectedness of family in her social context. For her this meant that her most important social responsibilities and demands globally affected her availability to participate but also provided enduring support – a reason to prioritize them continually. “[Some] days when my family come and get me, I had to go to the doctor’s office, you know? Then we might be at a restaurant getting something to eat after we leave the office. You know we want something to eat. Or somebody wants to stop at Ross you know, get just some outfits for the kids. I mean, I didn’t try [to miss the virtual session]. I would be with my family. And then before you know it, I said, ‘oh, look at the time. My phone is dead and I have missed the appointment.’” (60-year-old Black, Non-Hispanic female, ID 12)
This participant described the tension among comfort, convenience, and distraction stating “the pro was I didn’t have to find a babysitter. I can be in my house. And the same time, that’s – you know, the same con. My older kids come in, mom, they did this, why is it doing that? You know, so it was hard to find that quiet peace, but it was also nice that I can do it in my own home … I think if I did it in a doctor’s office, I wouldn’t have been able to relax and meditate the way I was able to do at my home.” (35-year-old White, Non-Hispanic female, ID 20)
Sharing Intimate Spaces: “People Seeing How I Live”
Some participants did not have a quiet, private or comfortable area within the home from which to join the session, requiring them to move to a more personal space. This introduced inequity in the level of intimacy involved in attendance. For example, a participant discussed having the camera on in their bedroom, “I just didn’t feel comfortable in my own room. I just didn’t. I didn’t want to have that stress on my head [of] what they could see and couldn’t see. I can see enough right here on your screen that you all could see enough in my room. And that’s just above your head, so.” (69-year-old Black, Non-Hispanic female, ID 27)
With technical assistance, some inequities can be mitigated. For example, when the participant was shown how to blur the background, she felt more comfortable: Interviewer: If we had been able to teach you [how to blur the background], do you think that might have helped?” Interviewee: “Yeah. That would have helped. I like that. Because it is blurred, you know, as and you don’t know what you’re looking at. Because in my bedroom I mean, I got everything in there.” (69-year-old Black, Non-Hispanic female, ID 27)
Leaving the camera off was one way to preserve privacy and comfort when there were limited options in the home environment. However, many participants wanted to be seen. This participant lived with her mother in a small home, and she described foregoing comfort and privacy in preference for being seen on video: “My space is limited where I’m living, how I’m living. I’m living with my mother in her house. So, I have one bedroom, and she doesn’t have like a kitchen table or chairs. Her setup is different. So, I really had no place to sit in the chair, and it was hard to really figure out where I was going to put the computer so I could show up on Zoom. I could have done it the whole time without showing up on Zoom, but I thought it would be more fun just to be seen and heard too. So, that was the challenge. The challenge for me was just my space, my limited space.” (63-year-old Black, Non-Hispanic female, ID 10)

Navigating the Virtual Platform
Navigating the virtual platform refers to participants’ experiences using technology to engage with others in this potential space that is co-created and mediated by technology. The virtual space was new to many, but not all, participants. The most striking finding about participants’ experiences navigating the virtual platform was the heterogeneity of experiences often influenced by participants’ social position. Subthemes included ease, struggle, and levels of support.
Ease: “It Was Just so Simple”
Many participants commented on their comfort with the technology and the ease of use. For example, a participant said, “It was just so simple. You picked up your phone or your computer or whatever you were going to use, and you did it. You had the class. It was very, very simple.” (54-year-old White, Non-Hispanic female, ID 34) Another participant shared a similar sentiment, “I knew that there wasn’t much to prevent me from being able to look at a phone and talk to people. You know, it’s not like I had to stand on my head or balance myself on one foot and hold the phone up…you’re not asking a lot.” (58-year-old Black, Non-Hispanic male, ID 2).
Some participants described value that was added with the technology. For example, this participant explained, “No, I don’t mind the camera at all. I think it’s kind of fun sometimes to see people in their own environment, like in their own habitat! Like this environment, or even if you’re laying down, or you know, it’s okay. It makes you more comfortable with people. I don’t mind it at all.” (63-year-old Black, Non-Hispanic female, ID 10) For participants who were socially isolated and unlikely to seek in-person care, virtual access was largely positive. For example, this participant who is unemployed and on disability shared, “It felt like I was being taken care of. It felt like as if I was going to a doctor’s appointment, but it was so much cooler!” (51-year-old Black, Non-Hispanic female, ID 35) For some, the virtual environment increased comfort and safety in the group setting. Differences in education level and social skill may have been less pronounced. One participant noted: “I’m nervous talking to multiple people. If I’m not there, it’s better if it’s on a telephone, when I’m there in person, my anxiety goes to the roof. And that’s because I did terrible in school, and everything reminds of sitting in school and being on spot.” (59-year-old White, Non-Hispanic female, ID 28). Personality factors and preferences also played a role in comfort level, as is highlighted by this participant: “I liked it online, because I’m kind of a not-a-crowd person. And since I’m not sitting there looking at people, I felt freer to talk, express my opinion. But if we were face-to-face, I might be held back some.” (62-year-old White, Non-Hispanic female, ID 16).
Socialization at a distance was particularly comforting during the pandemic when the prospect of contagious illness was a large threat. For participants with weakened immune systems, the virtual platform expanded access to care: “I liked it better online and you know, I could see them if they wanted to be seen, they could see me, but not be close enough to where if they sneeze, they would not get on me. I mean, I’m not a germaphobe or nothing like that, but because of COVID and you know like I said, I had cancer, so my immune system is down you know from all the treatments, so this was actually a really fun way to meet the other people, the other ladies and stuff that were in the group.” (49-year-old American Indian or Alaskan Native, Non-Hispanic female, ID 11).
Researchers anticipated disparities in virtual access and provided tablets to participants without virtual access. The pragmatic clinical trial design also included flexibility to approximate real-world conditions, such as accommodating participants who chose to keep their cameras off. This was important to some participants. As described by one person: “You had the option to put yourself on video, or if you didn’t want to be on video. So, that was very calming for me, because even if I’m talking and I wanted to turn off the video on the tablet that was provided to me on this study. I had the option to do so.” (35-year-old Black, Non-Hispanic female, ID 8) The use of break out rooms where participants interacted in smaller subsets was a highlight for some: “It was nice to get the breakout rooms and speak with other people and stuff… And like I said, everybody was really nice. And it was a nice thing to do.” (52-year-old Black, Non-Hispanic female, ID 13).
Some participants would not have attended the intervention if it were in-person at a clinical site due to heavy caretaking responsibilities, long travel times and the cost of hiring a caretaker. For example, this participant whose daughter is disabled explains, “I was able to do it. If it was not online and it was in person, I wouldn’t have been able to because…going somewhere, and having my daughter, getting somebody here to take care of her. And me having to go somewhere is more time. [It] would take me an hour to get [to the physical location]. So, that’s an extra 2 h …” (44-year-old White, Non-Hispanic female, ID 38).
Struggle: “I Don’t Really Want to be Online for Two Hours With Nobody”
Meanwhile, for other participants, the increased distance created by the virtual platform felt like a barrier to connection compared to in-person experiences. This participant lamented the loss of physical touch: “And also, the ability to feel connected to the other people. If I were in the same room with him, I’m just imagining this for a minute. We were sitting in a circle in the same room. There are probably times during the discussion that I would have actually touched them, touched the other people in the group. And that human connection as simple with touch is part of good communication for me. So, yeah, we’re robbed. Zoom robs us of at least one aspect of how we communicate with each other.” (72-year-old White, Non-Hispanic male, ID 46) The sentiment of having lost out was commonly expressed, “I would love it to be able to be there and do this and be with the same people that I was with. That I was feeling their energy you know to make you want to really get this done… oh I would love that if that was to ever happen.” (58-year-old Black, Non-Hispanic female, ID 5) “There’s definitely a difference between doing it in person and doing it on the [Zoom]. I would think that ideally, it would be wonderful for people to do that in person. For one thing, it’s easier for people to share and talk to each other when they’re in the same room. Even people who are more hesitant to talk … when you’re looking at this little teeny, square person on the screen, it’s hard to make connections. It would really be better if it was done personally. Wherever possible.” (70-year-old White, Non-Hispanic female, ID 26).
Others commented on the increased level of concentration and energy expenditure required compared to in-person experiences. For example, this participant found the pace ‘a little fast’ and the cognitive load heavy: “I’ve never had this at a doctor’s office, but I don’t know if it will be more effective in person, maybe, but the thing is, it just felt long. It felt long to me… and a little fast. If I’m being honest, I don’t really want to be online for 2 h with nobody.” (52-year-old Black, Non-Hispanic female, ID 13). Meanwhile, for others, the energy input was balanced by valuing the experience: “So, for me to sit on the computer or my phone on a Zoom meeting for an hour and a half, almost two sometimes, was a lot for me, but it was worth it.” (67-year-old female, race and ethnicity undisclosed, ID 4).
Levels of Support: “Where There is a Will, There is a Way”
Participants had varying levels of experience and comfort with technology. For many participants, this was their first experience using video-conferencing technology to attend a virtual group. Others were well acquainted with the format through work and social connections, and this contributed to their positive experience: “I love Zoom now. That’s because with this pandemic, I belong to a sorority, and we’ve had our Zoom meetings. I was already in tune on how to use them, how to get out and go into the breakout room, how to leave the breakout room, how to stop my video if I needed to, how to turn up my volume. I didn’t have a problem at all.” (63-year-old Black, Non-Hispanic female, ID 23). Similarly, another participant expressed this ease: “I was fine with doing it online. I really was. I also should add, though, I spent the last 19 years of my working life working remotely and, in fact, managing it for the last 8 of those years, I was managing a huge team of people spread all across the country and had to do it all remotely. It was no change for me. I mean, it was not a big deal.” (70-year-old White, Non-Hispanic female, ID 26).
For others, it was essential that technical assistance was provided. Flexibility and persistence on the part of participants and researchers was important to support equitable participation. For example, this participant explained, “Although I haven’t got it on the [screen] – there was a way, and they would hook me up and make sure I was included. It was like one way or the other. Wherever there is a will, there is a way!” (70-year-old Black, Non-Hispanic female, ID 30) Similarly, this participant noted, “I have no problems with it. I’m new to all this technology and stuff and I’ve just given that up to the staff that I’m working with, you know, for that part of the job…I could be anywhere, and I’ll try this, try that.” (58-year-old Black, Non-Hispanic male, ID 1).
In summary, participants expressed missing out on in-person experiences balanced by benefits of the virtual experience. There was a range of comfort with video-conferencing technology, with some having “never done a Zoom thing ever in [their] life” while others having to shift to online “professionally and personally” and thus “having no issue with it being online.” Meanwhile, the truly mixed experience was summed up nicely by one participant: “So, getting comfortable and not having that real connection that you do with folks, person to person, there’s that energy, there’s that feel that you take for it. So, I think that was a part that I probably missed out on… but it was also nice that I didn’t have to travel anywhere, there was no stress of parking or traffic or anything else like that. So, being able to do it in a comfortable environment and space like that, … it was always a wash at the end of the day.” (38-year-old White, Non-Hispanic male, ID 18).
Discussion
In the post-COVID era, more research is being published with recommendations and guidelines for virtual engagement in a wide variety of contexts.38,39 This study included participants across the socioeconomic spectrum and provided insights about the contribution of social determinants of health to the disparities in access and effort required to participate in virtual group mindfulness trainings (see Table 3). 40 Some of these disparities were represented by the quotes and themes explored in this manuscript, while other disparities can be explored in future work.
This qualitative analysis described the complexity underlying the experience of virtual mindfulness-based group medical visits. Participants simultaneously navigated varying external and virtual environments, resulting in differential obstruction and facilitation of the virtual experience. The experience of comfort, convenience and ease of use for some was juxtaposed with technological challenges, competing demands in the home and a desire for privacy.
Hidden Complexities
Video-conferencing technology presented each participant as a square on a screen. This flattened context lacked the depth and subtlety of in-person engagement, where a broader range of nonverbal communication is available. However, these interviews suggested a hidden complexity, or dimension, to virtual groups compared to in-person groups. As Figure 1 illustrates, during an in-person mindfulness-based group medical visit, participants shared a single external environment (classroom, break room, etc.) and individual internal experiences. The virtual experience had an additional layer for the individual, as each person navigated a separate external environment while participating in the creation of the virtual session. Ultimately, participants’ experiences were influenced by 3 environments: external, internal, and virtual. This competition for participants’ attention may have increased cognitive load. At the same time, learning mindfulness in the middle of life with its competing priorities offered the opportunity to practice present moment awareness and equanimity while meditating. Equanimity refers to “an even-minded mental state or dispositional tendency toward all experiences or objects, regardless of their origin or their affective valence (see Figure 2).” Complexity introduced by virtual vs in-person group mindfulness training.
42
Observing mind and body across physical and virtual environments with equanimity.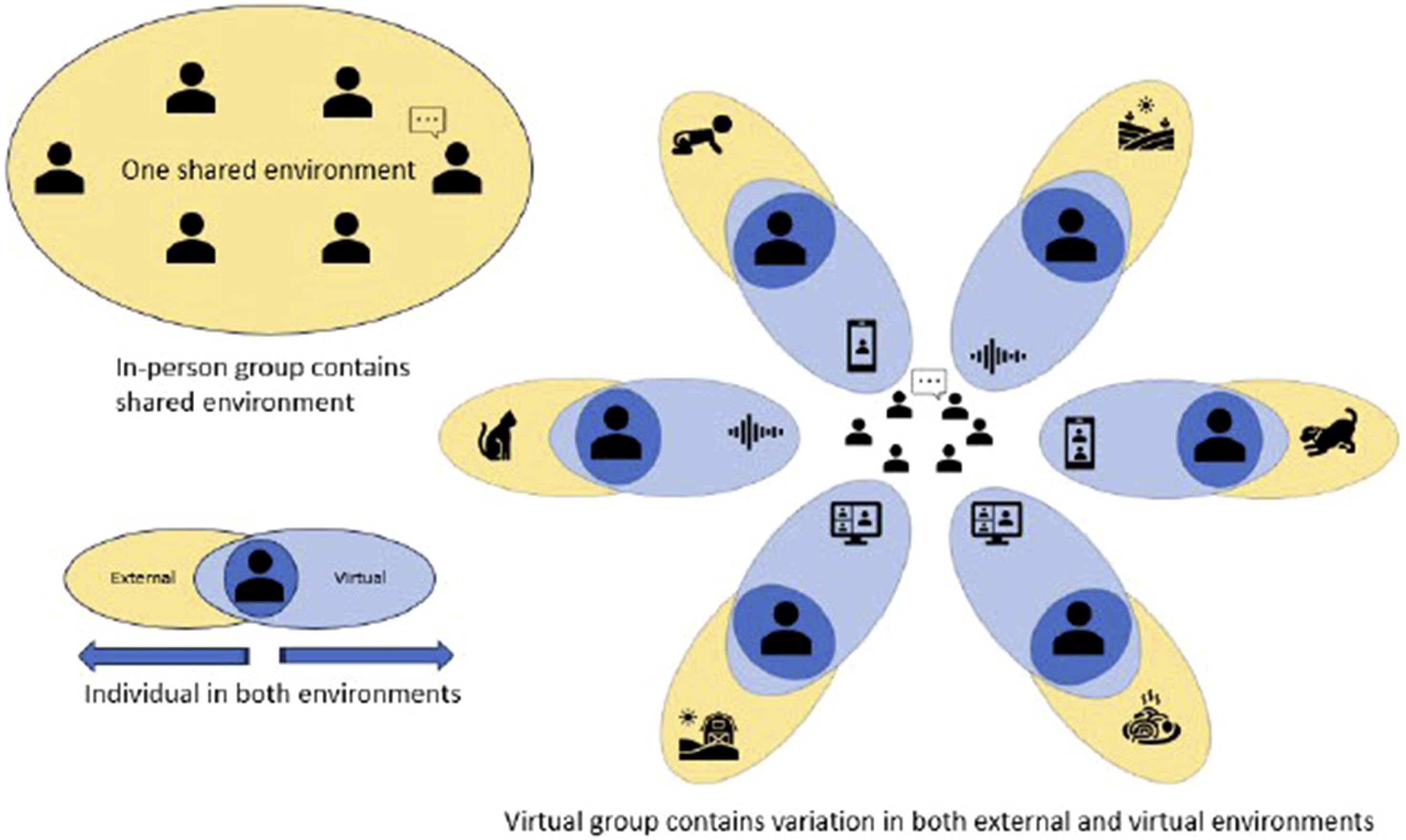

By examining the variety of experiences occurring in the external and virtual environments, researchers saw a more robust picture of the hidden complexities inherent to this model. Additional variation was introduced since each person’s virtual environment was mediated by their technology. Each instance of variation in patient experience was an opportunity to consider whether social determinants of health were at play and whether the variation present could result in more or less health equity.
One concrete example of the difference between in-person and virtual groups is to compare the process of arriving to in-person vs virtual group mindfulness training. There is a paradox here that virtual care is simple and yet its practice is complex. The discrete process of arriving and being physically present during in-person mindfulness training is not replicated in the virtual setting. Complexity exists in the varied external environments of all participants, in the movement of concentration and attention among different stimuli, and in each participant’s relationship with and response to technology. In-person mindfulness training sets the stage with a common external environment, that is arranged to promote attention and focus, whereas virtual mindfulness training involves sustaining attention toward or perpetually re-engaging with a shared virtual space. With in-person mindfulness training, participants experience a transition - they leave their prior setting and physically arrive for mindfulness training. Verbal and nonverbal cues communicate participants’ level of engagement. Rather than investing energy upfront with travel, time, etc., virtual attendance begins in an instant by clicking on a link. The lack of transition time to reorganize the internal environment and the lack of a physical transition to mark the start of the session can collapse the space for mental and physical preparation for mindfulness training. Attending to one’s environment to minimize distractions is helpful but is not always possible. In this manner, virtual mindfulness training occurs in the “real world” where competing stimuli vie for one’s attention. Arrival and presence are dynamic factors. There is an inward movement involved in arriving and maintaining presence during virtual mindfulness training that is individualized and largely unknowable by instructors and other participants. This is another area where virtual mindfulness training reflects the real world more directly than in person training, because people are engaging with mindfulness from their homes. They are in home environments when they attend, and they are not removed to a classroom or retreat center.
Pedagogical Implications
Conveying the work of mindfulness presents a unique challenge. The process is internal and individual, and the product is also internal and not easily assessed by an outside observer. In teaching mindfulness, instructors offer guidance that alternately brings attention to the internal and external environments, prompting participants to explore connections from the liminal space in between. In this process, participants can begin to conceptualize separately the observed environments (internal and external) and the place from which they observe. The virtual setting adds a third dimension to the teaching and practice of group mindfulness. It challenges present-moment awareness in specific ways – first by removing the teacher/observer from the physical space which distances the learner from social cues and accountability, second by an implicit suspension of day-to-day interpersonal rules, and third, the unacknowledged interface (camera, connectivity, and screen) that filters the experience. An important need for virtual group mindfulness practice is to provide a structure that can organize the real and virtual spaces. Naming the presence of the virtual platform, introducing its role and function, and accepting interference are key to acknowledging the adaptation. By naming the role and function of the technology, the instructor can help shift participants’ focus to the supportive role it can play in accessing and practicing mindfulness. Where interference might occur, instructors can name the distractions and pitfalls to virtual instruction and thereby normalize the inevitable challenges.
A final consideration is the language used to discuss a virtual interface for mindfulness. Technology and personal devices have the negative connotation of interfering with the ability to be present and mindful, so resolving the role of technology in attention and mindfulness practice is important. Guidance is needed for how to bring focus to the mindful group space, but not to the device itself or other apps like internet browsers or social media. Furthermore, instructors could address the pull of digital tasks and cues while working via a virtual platform. In addition to outlining individual and group norms for engagement in this environment, this can extend mindful awareness to the presence of a virtual space even outside of the session. 43
Implications for Future Research
The physical space where the participant is located during the mindfulness training can enhance or detract from the participants’ experience and is vastly different from in-person programs. The process of arriving and being present during in-person mindfulness training differs from arrival to and participation in a virtual space. Other qualitative studies of synchronous virtual group mindfulness interventions have likewise described the mixed cost/benefits of remote participation.41,44 However, to our knowledge, this paper was the first to explore specific factors in the physical environment—including physical comfort and safety, conflicts with other household members who are unwilling to give up the space, and disruptions from children and people at the door— that may influence and integrate with other aspects of the training experience. As mindfulness training includes acceptance of difficult emotions, thoughts and experiences, its practice in stimulating or stressful environments may facilitate learning about how to work with and through these inevitable challenges using mindfulness. These findings can inform approaches to teaching mindfulness virtually.
The participant’s internal mindset may influence how they engage with virtual mindfulness programming, including their capacity to remain committed in the face of the competing needs of close others in their lives. Some participants who had caregiver roles for spouses, children, or other family members described feeling strained when family member needs conflicted with the virtual mindfulness training. This tension may have been more prominent given participants were physically present with family members during the virtual mindfulness sessions. Others, meanwhile, seemed to develop a greater sense of self-compassion through the mindfulness training. They began to recognize their own needs as valid and worthy and were better able to maintain the interpersonal boundaries needed to take care of themselves (eg, hire a sitter to allow participation). Indeed, self-compassion is implicit in mindfulness training and entails awareness of one’s own feelings, thoughts, needs in connection with others; self-compassion is linked to relational authenticity and compromise in conflict (as opposed to self-subordination or self-prioritization). 19 Moreover, self-compassion has been linked to less pain disability through greater self-efficacy, making it a measure to include for future work with participants with chronic pain. 20 The virtual interface was described by some as a preferred mode of engagement, by others as less optimal compared to in-person formats, and by a few as a mixed experience with no clear preference. This preference is influenced by many factors, including personality traits like interpersonal orientation. Although not specific to synchronous virtual group MBIs, previous research suggests individuals who are high in extroversion and/or agreeableness prefer group-based intervention, while those who are more introverted prefer more structured and/or one-on-one intervention formats. 45 In this study, the virtual group format provided a buffer for some presumably more introverted participants, who found greater ease in interacting with others. Meanwhile, some who are energized by interpersonal interaction found the virtual interface an obstacle to connection and perceived needing to exert greater effort to remain engaged. Future work is needed to explore the range of individual, community and systemic factors that moderate outcomes in the virtual vs in-person formats. This may allow participants and referring providers to make an informed choice about which format is best suited to each person.
On the one hand, video-conferencing platforms can create more access for historically marginalized groups by decreasing cost, transportation, and time barriers. On the other hand, without an overt strategy in place to address other barriers, this intervention’s expansion is unlikely to substantially decrease health disparities. For example, the equitable large-scale implementation of virtual MBSR training in primary care settings would require accommodation for differing effects of social determinants of health across multiple levels of influence (as presented in Table 2). Some of these accommodations include greater access to internet services, technical support for all users, sufficient interpersonal trust, and reliable access to primary care.
Limitations
This reflexive thematic analysis told part of the story, but it is not the complete story. Exit interviews were collected from 59 out of 122 participants. Participants who declined to be interviewed could have additional vantage points not reflected in this sample. On a few occasions, participants knew the researcher conducting the interview, which could affect what participants disclosed. There is also more analysis to be completed to better understand how socioeconomic status affected participant experiences. The main study outcomes are not yet available, so it is not currently possible to link qualitative interview themes with quantitative results. The OPTIMUM study included only virtual groups due to the pandemic, thus this project cannot compare in-person vs virtual MBSR. We conducted fidelity assessments and found that the MBSR groups were engaging to participants, and key features of MBSR were consistently included in sessions. 46 Completion of the parent study and analysis of primary study endpoints will also inform future qualitative analysis.
Despite these limitations, this analysis of 59 exit interviews contained rich content and the results of the thematic analysis contribute new insights into the complexity of virtual MBSR training and the ways in which a person’s social status may affect their experience. As virtual delivery of MBSR continues to develop, understanding these differences in patient experience will help inform program development.
Conclusion
This analysis highlighted how virtual settings are simple and complex, mirroring the practice of mindfulness. A virtual setting appears with the press of a button. However, on closer look, there are multiple variables at play that differentially affect how participants interact with the virtual setting. Similarly, in essence, mindfulness involves simply being present in the present moment. On closer examination, holding one’s attention in the present moment is complicated. Key themes were ‘effects of the external environment’ and ‘navigating the virtual platform.’ Within the external environment, subthemes were comfort, social demands in the home setting, and sharing personal spaces. With regards to the virtual environment, subthemes were ease, struggle, and levels of support. Where possible, differences in participant experience were analyzed by considering the role of social determinants of health and the level of influence (individual to society). In this manner, researchers developed a framework to evaluate the health equity implications of virtual as opposed to in-person MBSR training.
Supplemental Material
Supplemental Material - The Hidden Complexity of Virtual Mindfulness-Based Group Medical Visits: Comfort, Challenge, and the Influence of Social Determinants of Health
Supplemental Material for The Hidden Complexity of Virtual Mindfulness-Based Group Medical Visits: Comfort, Challenge, and the Influence of Social Determinants of Health by Jessica L. Barnhill, Gabriela Castro, Christine Lathren, Elondra Harr, Isabel Roth, Jose E. Baez, Ruth Rodriguez, Suzanne Lawrence, Paula Gardiner, Carol M. Greco, Holly N. Thomas, Susan A. Gaylord, Graham Dore, Anita Bengert, and Natalia E. Morone in Journal of Global Advances in Integrative Medicine and Health.
Supplemental Material
Supplemental Material - The Hidden Complexity of Virtual Mindfulness-Based Group Medical Visits: Comfort, Challenge, and the Influence of Social Determinants of Health
Supplemental Material for The Hidden Complexity of Virtual Mindfulness-Based Group Medical Visits: Comfort, Challenge, and the Influence of Social Determinants of Health by Jessica L. Barnhill, Gabriela Castro, Christine Lathren, Elondra Harr, Isabel Roth, Jose E. Baez, Ruth Rodriguez, Suzanne Lawrence, Paula Gardiner, Carol M. Greco, Holly N. Thomas, Susan A. Gaylord, Graham Dore, Anita Bengert, and Natalia E. Morone in Journal of Global Advances in Integrative Medicine and Health.
Footnotes
Acknowledgments
OPTIMUM Community Advisory Board members: Nicole Elam, Amy Goldstein, Demond Hamer, and Sarah Kirshenbaum. National Center for Complementary and Integrative Health. Dr Paul Mihas, Odum Institute, University of North Carolina at Chapel Hill for qualitative analysis consultation. The Community Advisory Board for the OPTIMUM study. The National Institute for Complementary and Integrative Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:This work was supported within the National Institutes of Health (NIH) Pragmatic Trials Collaboratory through the NIH HEAL Initiative under award number UG3/UH3 AT010621 administered by the National Center for Complementary and Integrative Health. This work also received logistical and technical support from the PRISM Resource Coordinating Center under award number U24AT010961 and UG3 AT010621 from the NIH through the NIH HEAL Initiative. The content is solely the responsibility of the authors and does not necessarily represent the official views of the [Institute, Center, or Office providing oversight] or the NIH or its HEAL Initiative.
Ethical Statement
Data Availability Statement
The data is not publicly available as the main trial is ongoing.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.