
Abstract
Background
Few studies have examined the menopausal transition in American Indian and Alaska Native (AI/AN) women; these reports indicate they are the most likely group to report bothersome vasomotor symptoms (VMS). Evidence demonstrates VMS may be a biomarker for chronic diseases. Thus, evidence-based interventions to improve VMS and other symptoms and health-screening rates for urban midlife AI/AN women are needed.
Objective
The objectives of this community-based project were to form a Community Advisory Board (CAB) with whom to: 1) conduct CAB meetings (similar to a focus group) with midlife AI/AN women to understand their lived health care experiences and needs during the menopausal transition; and 2) obtain guidance in creating a tailored intervention.
Methods
Eligible participants indicated they were registered members of American Indian Tribes, self-identified as a woman, aged 35 or older, and were recruited through the Urban Indian Center of Salt Lake and community outreach. Three CAB meetings were conducted via Zoom. A qualitative-descriptive approach was used for analysis, with the aim of staying close to the data to understand AI/AN women’s experiences and needs. Transcripts were iteratively coded using content/thematic analysis.
Results
Four themes emerged: 1) lack of and desire for information about the menopause transition; 2) barriers to accessing care; 3) matriarchal priorities impacting personal health outcomes; and 4) preferences for Indigenous and integrative medicine as first-line interventions, followed by conventional medicine.
Conclusions
Among this sample of urban AI/AN women, there was a great need for and interest in information about menopause, both for themselves and for their daughters and family. Integrative and Indigenous approaches were preferred. Proposed next steps include developing and pilot-testing a nurse-delivered health-education intervention with Indigenous, integrative, and conventional medical content.
Keywords
Background
Menopause is the natural cessation of menses that occurs as a part of a woman’s aging process. Hormone fluctuations during the menopausal transition (MT), a period of several years leading up to menopause, are associated with a range of symptoms. These symptoms include vasomotor symptoms (VMS) which vary by woman but can include hot flashes, night sweats, increased heart rate, palpitations, tingling in the fingers, or feelings of anxiety.1-5 Some women experience a chill as the hot flash subsides. 6 VMS are affected by social determinants of health, including education, socioeconomic status, underlying health condition, and cultural background.7-9 With respect to race, African American women report the longest duration of VMS with a median 10.1 years compared to the total sample median of 7.4 years. 10 VMS are more prevalent among Hispanic and African American women in the Study of Women Across the Nation (SWAN). 11 The SWAN study was specifically designed as a multiethnic longitudinal cohort study of women in the United States and recruited non-Hispanic Caucasian, African American, Chinese, Japanese and Hispanic women but did not recruit Indigenous women. 11
Furthermore, there are few other studies that have examined the MT as experienced by Indigenous 1 or AI/AN women. One of the few studies that includes Indigenous women in their sample focused on VMS experienced by premenopausal, racially diverse women; Indigenous women were the most likely to report having bothersome VMS and joint pain of any ethnic group. 12 VMS can be bothersome and can interfere with quality of life. In addition to bothersomeness, a growing body of evidence demonstrates that VMS may be a biomarker for chronic diseases including cardiovascular disease, 13 osteoporosis, 14 and Alzheimer’s dementia. 15 Indigenous women have a shorter life expectancy and higher mortality rates from chronic diseases, including heart disease, cancer, diabetes, and alcohol-related diseases 16 compared to non-Hispanic White (NHWs) women. Yet there are no extant published data on rates of chronic diseases experienced by Indigenous women with severe VMS.
More than 70% of Indigenous women live in urban areas and face unique barriers to accessing health care 17 and have lower utilization of health care screening.17-19 In addition to higher rates of chronic disease and mortality, urban AI/AN women experience higher rates of obesity, homicide, infectious disease, and tobacco use than urban non-Hispanic white women.17,20 Urban AI/AN women are also less likely to obtain preventive health care such as regular cervical-cancer screening and mammography compared to NHW women,19,21 and face unique barriers to screening. Further, AI/AN women have indicated a need for more information about menopause 22 and often distrust conventional care, such as surgical or pharmaceutical interventions. 23 Thus, designing evidence-based interventions to improve symptoms and health-screening rates for urban midlife AI/AN women is of critical importance. Interventions must be designed in collaboration with Indigenous midlife women to ensure the intervention is culturally relevant and congruent, and thus acceptable. Relevant interventions are more likely to be utilized and therefore more likely to reduce health disparities. Our team 2 has previously designed MENOGAP, a four-session group medical-visit series. The group medical visits include medical care, health education including both evidence-based conventional and integrative care, experientials, and social support. However, MENOGAP is designed for a general audience of midlife women. Recognizing the unique experiences of AI/AN women, we wanted to adapt MENOGAP to be culturally relevant and congruent, and thus acceptable. To realize this vision, we designed a community-based participatory research (CBPR) project with the main objective of developing a Community Advisory Board (CAB) of Indigenous midlife women with whom we conducted CAB meetings (similar to a focus group) to better understand their experiences and health care needs during the MT. We sought Indigenous women’s guidance in creating a culturally relevant and tailored intervention that provides Indigenous, integrative, and conventional health education, and health-screening referrals.
Methods
To achieve the project’s goal, we decided to adapt MENOGAP, an evidence-based group medical-visit intervention designed to fill a GAP in MENOpausal women’s health care. MENOGAP contains evidenced-based conventional medicine, integrative health education, and self-care advice that is delivered in a group setting. Recruitment for a CAB for the study was carried out via community outreach, leveraging a collaborative community-academic-clinical partnership between the University of Utah’s MENOGAP AI/AN research team and the Urban Indian Center of Salt Lake (UICSL). UICSL is a non-profit that serves AI/AN who live within Davis, Salt Lake, Tooele, Utah, Cache, and Weber counties. The UICSL provides culturally competent health care programs and services for the whole family. The services are primary health care services, behavioral health care services, preventive/health screenings, and social services. The UICSL partners includes staff, an RN, and an operations director. The university team is comprised of faculty and undergraduate and graduate students with backgrounds in several disciplines (i.e., integrative health, health sciences, nursing, midwifery, women’s health, medical anthropology, public health, menopause). Thus, our team is a unique and close community-academic-clinical organization partnership (see footnote 2). Potential CAB members were identified and enrolled in the study by UICSL staff. Potential participants were contacted via phone calls and emails, providing them with study information and assessing their availability to complete the consent process and receive comprehensive details regarding the research. Eligibility criteria were 1) biologically female, 2) aged 35 or older, 3) AI/AN, and 4) living in the Wasatch Front urban corridor. Eight CAB members agreed to participate in focus-group discussions on their experiences with perimenopause.
The CAB meeting started with a brief slideshow providing information about menopause symptoms, timing and duration of the MT, and an overview of MENOGAP. A conversation was then conducted with the CAB using a focus-group interview guide that included questions used for previous MENOGAP intervention studies. Because previous MENOGAP studies included women of varying races and ethnicities, the questions were refined for cultural relevance for AI/AN women by the community-academic-clinical partners. The interview guide included the following sections: introductions of the research team; introductions of CAB members; why we are conducting this study (with slides shared); conversation regarding key symptoms and health needs experienced by AI/AN women, health care facilitators and barriers for AI/AN women to access menopause care, preferred aspects of integrative and conventional medical care, and group medical visits; open discussion of final thoughts and CAB member questions.
Three CAB meetings of the same content were conducted via Zoom. Note that CAB members could not all attend one meeting on the same date, so we provided the same slideshow and facilitated a conversation on the same topics on three occasions (labeled as CAB 1a, 1b, and 1c in the exemplar-quotes table). CAB members and the study team could all see one another, and some CAB members knew one another from the urban AI/AN community in the area. The CAB meeting was co-led by the study PIs (L.J.T.-S., S.A.), and research assistant (C.C.), with the majority of leadership provided by the research assistant, who is an enrolled member of an AI/AN Tribe and is a known, trusted community member among the urban AI/AN community. With CAB member permission, data collection included audio-recording the three 1 ½- to 2-hour CAB sessions. Field notes were also taken by one research team member (J.K.-M.). CAB meetings were attended by 2-3 research-clinical team members. Please refer to Appendix A for the interview guide. The recording feature of Zoom was used to enable the creation of transcripts. Transcriptions of the audio-recordings were created by a member of the research team and verified for accuracy by other team members. Video recordings were destroyed after transcription. We took extra steps to protect CAB members’ privacy given the historical abuses of AI/AN participants in research studies.
Lincoln and Guba’s trustworthiness guidelines were followed. 24 Thematic and content analysis was used within the Dedoose 9.0.107 software. A codebook was created consisting of deductive codes related to the interview guide, and inductive codes to capture novel insights made by CAB members. This codebook was applied to the transcripts by research team members (S.S., S.A., J.A.E., T.A., J.K.-M., L.O.K.). Codes were reviewed for and then organized by themes. The research team did a final review of coding and themes. Discrepancies were discussed, and final decisions were made by consensus. Importantly, Indigenous members of the research team provided cultural insights and oversight into the qualitative analysis.
This study received ethics approval from both the University of Utah and the Indian Health Service Institutional Review Boards. UICSL staff assisted participants with study consent and participants received $110 in compensation. Additionally, this manuscript received approval from the Indian Health Service Institutional Review Board and UICSL for submission for peer review and publication.
Results
Demographics
Demographic Characteristics of CAB Participants.
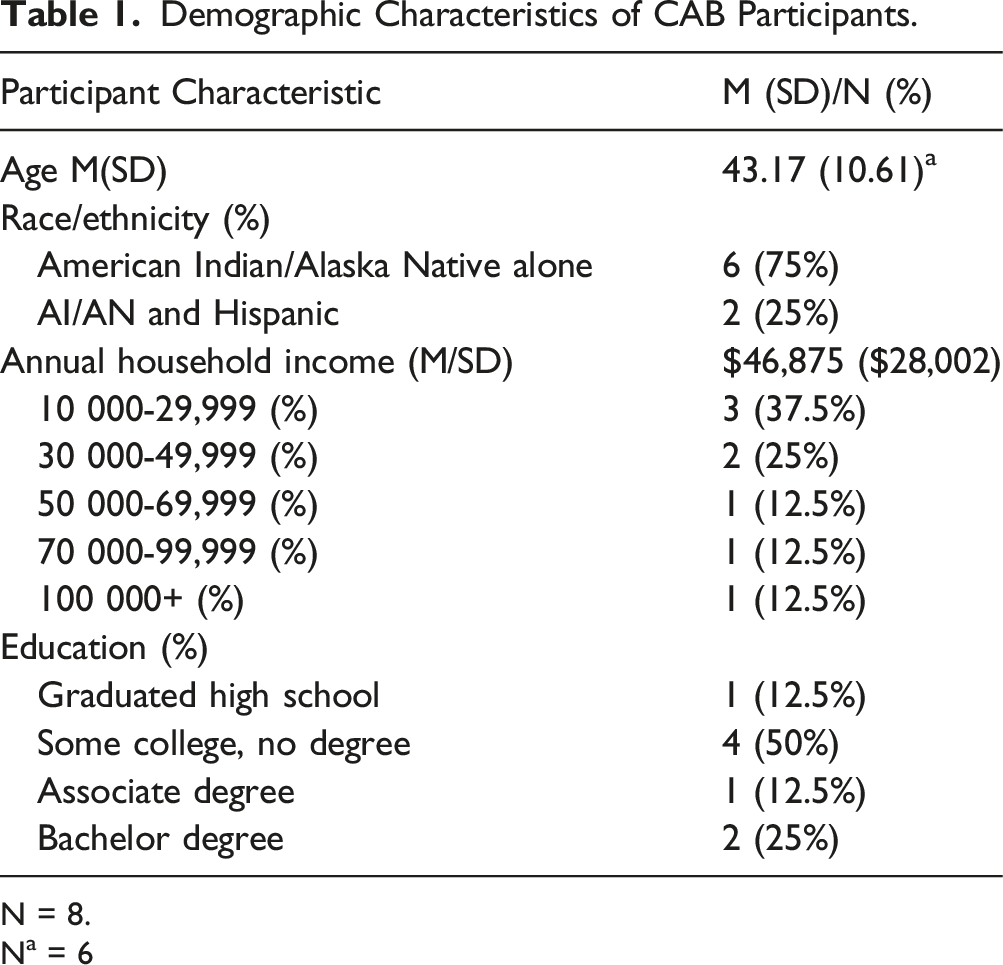
N = 8.
Na = 6
Additional Exemplar Quotes for Each Theme.

…I have these symptoms, like, I’ll be getting hot and I'm like going, “I’m so young, but I feel like I'm going through menopause.” I’ve never [known] the symptoms. That’s not something my mom talked about. We barely talked about periods. … It’s just, you don’t know where to get this kind of information. I didn’t. And then, my age, I go to the doctor. Tell him. [He replies], “[At] your age?” Like, “Oh, no. You can't be going through menopause.” I don't know. What is menopause? (CAB 1a, Participant 2)
Friends were sources of menopause-transition support for CAB members. A different participant said: Going back to my grandmother and my mom, they had no idea. They weren't taught and we were not taught that we're going to go through this menopause. It’s kind of like the unknown. So, when I was going through it, I was asking friends, “Is this normal? Do you feel like this? I feel like my heart is gonna jump out. Does that happen to you at night?” So, I was just, you know, asking around what was going on with me. (CAB 1a, Participant 3) Women reported being unsure about where to get information about the menopause transition. Some said they wanted to break the trend of silence and stigma surrounding menopause for their daughters and were interested in sharing the MENOGAP class materials with them. A participant shared, “I have two girls. … Maybe I share a little bit too much, but I like to tell because I haven’t got those talks.” (CAB 1a, Participant 2)
I think a lot of doctors are not really, you know, experienced [in seeing], you know, Indigenous different Tribes. So, I kind of felt uncomfortable about that because a lot of times, to me, I feel like they just give you that medication. “Here take this, take this,” and I didn't want to do that to my body because I don't even take an aspirin. (CAB 1a, Participant 3)
Participants were also concerned with the rushed nature of doctor’s visits and felt pressure to explain their health concerns quickly. A few CAB members said they felt more comfortable with female providers, who were able to relate to them as women, and less comfortable with male providers. Several said they had to speak up and advocate for themselves. For example, a participant stated: I’ll go into a doctor's office, and sometimes they'll be surprised that I know what I know. … I'll come with a notepad and be like, “I have these questions.” And that will surprise them and they'll treat you with a little bit more respect because of how I tried to project myself. … Sometimes I just think, “Why do I have to … do that to get something that should be available for all of us. Why does it have to be so hard?” (CAB 1b, Participant 2)
One woman discussed the additional barrier of weight stigma in the health care setting, requiring her to persistently advocate for her health needs. Participants also reported that traditional Indigenous treatments were difficult to access. One CAB member said she believed IHS “services aren’t as successful [in the Western states of the U.S.] as they are on the east coast” (CAB 1c, Participant 1). Additional barriers to the access of care included the cost of services, travel and cost associated with transportation to appointments, insurance issues, difficulty securing referrals to specialized care, lack of access to educational resources, inability to access provider appointments on short notice, and juggling multiple responsibilities as a mother and wife that conflicted with the prioritization of health. This last barrier is relevant to the third theme, Matriarchal priorities and resulting health outcomes, where matriarchal priorities impacted CAB members’ health outcomes.
I’m [Indigenous] as well, and in my family unit, us females have to be the strong ones and the backbone of everyone in our household. And, we do have to put a lot of what, what our, what emotions and whatever we’re going through behind on the back burner, and act like it’s not happening. And that has a lot to do with, for me, I feel like it has a lot to do with, um, how we seen our grandma, you know, how we seen our mom, as we were growing up. And so, we felt like that is what us as females in my family have to do, is put a lot of our worries, symptoms, and everything on the back burner… (CAB 1a, Participant 1)
Another CAB member summarized this dynamic when discussing her financial and insurance difficulties in securing needed dental care: Whether feeding your kids food, or a meal on the table versus getting insurance taken out of my check, I’m going to go with the food. A mom can survive. We’re always like, my god… With Native ways, I feel like… “We tough! Shake it off. (laughs) It’s alright. Smiles.” My mom always says, “Smiles every day, body’s still the same. Mommy’s still the same.” (CAB 1a, Participant 2)
I’ve only had one experience with acupuncture and I don't know. I'm not familiar enough with it. It would be interesting to try. I know massage therapy is wonderful. Chiropractic care is also wonderful. … There’s so many different forms of therapy that would be really useful … Meditation practices. … Breathing exercises. That's like, what I turn to when my heart starts racing. It's just trying to find that… recenter myself. (CAB 1c, Participant 1)
Participant preferences for Indigenous treatments included remedies made by an Indigenous herbalist, and access to a medicine man/healer. Regarding a medicine man, a participant stated: Someone said that they are thinking of hiring a medicine man or healer. I think that's a great idea. I definitely see a lot of people on the Facebook group for Natives wondering when they can get one or talk to one because it sounds like there's, there's not many at all here in the area. And I'd love to have access to that (CAB 1b, Participant 2).
Another participant said: I did really consider going back to Navajo land to get an herbalist to get a Navajo lady to do some herbs for me. I gave it a short time, and I says, if I don't feel better, you know, if I'm not feeling up to myself, then I was gonna go drive down there and see if somebody would get me some herbs that I can start taking (CAB 1a, Participant 5).
Discussion
Overall, the results from this study revealed that among this sample of urban Indigenous midlife women who comprised a CAB, there was a great need for and interest regarding information about the menopause transition and menopause. The CAB members wanted to know more about the menopause transition for themselves and also for the purpose of teaching their daughters and family members. Indigenous women who participated in the study were interested in integrative and Indigenous approaches as first-line care. The results of this study are aligned with the scant literature on AI/AN women’s experiences of menopause, indicating AI/AN women have insufficient information before menopause 22 and distrust of conventional care. 23 Four themes emerged from this process, as follows. CAB members identified that 1) they lacked knowledge regarding the menopause transition; 2) they were faced with barriers to accessing care; 3) there were multiple family and work needs, making it hard to prioritize their own health; and 4) they did not like or trust many of the treatment options offered by conventional medicine.
Community Advisory Board Sessions
To create a culturally tailored version of the MENOGAP intervention, we collaborated with a CAB to integrate community feedback and perspective. CABs are increasingly being used as a means to enhance health through the tailoring of translational research. 25 For example, CABs have been used with Indigenous populations to improve health outcomes in postpartum depression 26 and oral health, 27 to address health disparities experienced by Indigenous women with disabilities, 28 and to understand the social-support resources of Indigenous women cancer survivors. 29
In our study, we collected data via Zoom through a CAB comprised of eight Indigenous women who gave feedback on a presentation given by the academic team. The group setting of the CAB sessions facilitated rich discussion among CAB members, where the women were able to elaborate on experiences that were similar or divergent in nature. Offering the CAB sessions by Zoom allowed the CAB members to join from their preferred environment. This supported individual comfort and safety and therefore promoted open discussion. Additionally, offering three CAB sessions allowed for insights to be collected from a wider group of CAB members, all of whom were midlife women balancing multiple responsibilities.
Strengths and Limitations
This study contributes a clearer understanding of Indigenous women’s experiences of the menopause transition (MT). The findings are strengthened by using qualitative data-analysis techniques to create themes from the CAB sessions. Saturation of themes was reached, and a thick, rich description of MT was given by the participants. A diverse health care team which included integrative health, nurse-midwives, public health, and medical anthropology experts reviewed the findings of this study. The team included researchers, nurse-midwives, and a licensed acupuncturist. There are several limitations. First, the AI/AN women who participated in the discussion may be different than those who did not participate as they were willing to discuss the MT. An additional limitation is that no rural or frontier-dwelling women were enrolled and that the sample may not be generalizable to midlife Indigenous women living outside urban areas. Furthermore, women were only sampled from one area of the Intermountain West and most women were in the menopausal transition, thus have not yet experienced post-menopause and this may limit our generalizability to post-menopause. Future nationwide surveys are needed that include a sample of Indigenous women from all areas of the United States.
Clinical Implications
Health organizations and clinicians should consider the value of using integrative and or Indigenous therapies when caring for diverse groups of women during the MT. A 2022 article noted that optimal care of midlife women incorporates racial/ethnic differences and preferences in menopause treatment. 30 This aligns with what our CAB reported—that Indigenous and integrative health modalities are sought as first-line care. Additionally, clinicians should be aware of racial/ethnic differences in treatment preferences when counseling patients on treatment options for menopausal symptoms to provide optimal care. The integrative health concept of “body-mind-spirit” is congruent with AI/AN culture and traditional health promotion practices. Indigenous traditional healing is identified as a whole medical system that encompasses a range of holistic treatments used by Indigenous healers for many acute and chronic conditions or to promote health and wellbeing. 31
Clinicians should also be aware that there are taboos regarding MT. Stigma32,33 and shame 34 surround the MT and some women feel uncomfortable discussing the MT. Of note is that Canadian First Nations women indicated there is not a uniform word for menopause in Ojibway or Oji-Cree languages. A common phrase is “that time when periods stop”. 35 This taboo and lack of language to describe menopause adds to the lack of knowledge regarding menopause for some women.
Research Implications
There is limited published research regarding menopause for Indigenous women. This study offers a community-based participatory approach to conducting CAB meetings with Indigenous midlife women. This research design offers insights to Indigenous midlife women’s lived experiences. Future research is needed regarding AI/AN women’s experience of MT symptoms and access to Indigenous, integrative, and conventional health care providers. The next steps in this research propose the development and pilot-testing of a nurse-delivered health-education intervention with Indigenous, integrative, and conventional medical content for feasibility and acceptability.
Conclusions
In summary, this CBPR study provides information for future practice in designing approaches to providing culturally congruent and relevant menopause care. Indigenous women are interested in using integrative and Indigenous care as first-line approaches. This study demonstrates the importance of using integrative medicine to reduce health disparities for Indigenous women and advancing health equity through whole-person, culturally appropriate care for vulnerable populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Nursing Research; 1F31NR020431-01 and University of Utah Vice President for Research; Intramural; American Indian and Alaska Native Midl.