
Abstract
Mindful Movement approaches have been a growing part of the Veterans Health Administration (VA). Innovations in tele-health technology had been an important initiative before the public health emergency to meet the needs of rural veterans as well as challenges in getting to a physical location for care. The onset of the COVID-19 pandemic accelerated this transition to tele-delivery of many practices including mindful movement. This paper aims to share lessons learned from virtual delivery of mindful movement as part of clinical and well-being programs in VA. Benefits of virtual care discussed include the convenience and decreased travel burden; accessibility for adaptive movement options; translation to home practice; and shifting the emphasis to interoceptive skills-building supportive of self-efficacy for exploring and identifying safe movement. Important challenges are also identified such as technology related barriers; teachers trained to meet the need of offering adaptations for a heterogenous population and supporting interoceptive skill-building; and supporting both physical and psychological safety. Examples are provided of medical groups incorporating virtual mindful movement within programs for diabetes and pain care to further explore the potential benefit of these practices being integrated within the care itself, rather than as a separate practice. It is hoped that the lessons learned will provide support for Veterans and staff, and the wider health care community, in what they need to participate in virtual care that is high quality, accessible, and meets the needs for greater health and well-being.
Introduction History and Current State of Virtual Mindful Movement in VA
Mindful movement, along with other complementary and integrative health (CIH) approaches, has been a growing part of Veterans Health Administration (VA) care since at least the 1990s. 1 Internal policy published in 2017 has supported more intentional and focused implementation of CIH, requiring that 8 approaches be made available as part of the Veterans Medical Benefits Package, if deemed appropriate by the Veteran and their care team as a part of their personal health plan as a part of a Whole Health System of care. These services include acupuncture, biofeedback, clinical hypnosis, guided imagery, massage therapy, meditation, Tai Chi, and yoga. In recent years, and especially with the onset of the COVID-19 pandemic, there has been rapid growth in the virtual delivery of CIH in VA, including mindful movement approaches.
VA has been a leader and innovator in delivery of care via telehealth technology given the rurality of many Veterans, and challenges in getting to a physical medical center for some.
2
In the mid-2010s, after recognizing the positive impact of CIH services on Veteran pain control, VA recommended that all facilities offer CIH services virtually; this investment in telehealth resources allowed for the VHA to develop tele-CIH programs in mindful movement.
3
While virtual yoga and Tai Chi classes have been occurring for a number of years, national tracking of tele-CIH, and more broadly, tele-Whole Health (which also includes health and wellness coaching, education, and Whole Health clinical care), started formally in 2017 with the development of a working group and resource/implementation guide. National administrative data has shown steady growth in the use of tele-Whole Health with large increases in Fiscal Year (FY) 2020 and the years following (FY18: 4323 encounters for 977 unique patients; FY19: 12,058 encounters and 3679 uniques; FY20: 129,657 encounters and 29,522 uniques; FY21: 426,337 encounters and 76,425 uniques; and FY22: 561,426 encounters and 105,585 uniques). Mindful movement approaches of yoga and Tai Chi are in the top 5 Whole Health services delivered via telehealth and have also seen growth year over year (Yoga encounters: FY19: 3357; FY20: 14,789; FY21: 54,058; FY22: 61,293. Tai Chi encounters: FY19: 2991; FY20: 13,328; FY21: 50,369; FY22: 61,516). (Figure 1) TeleWholeHealth encounters fiscal year 2019-2022.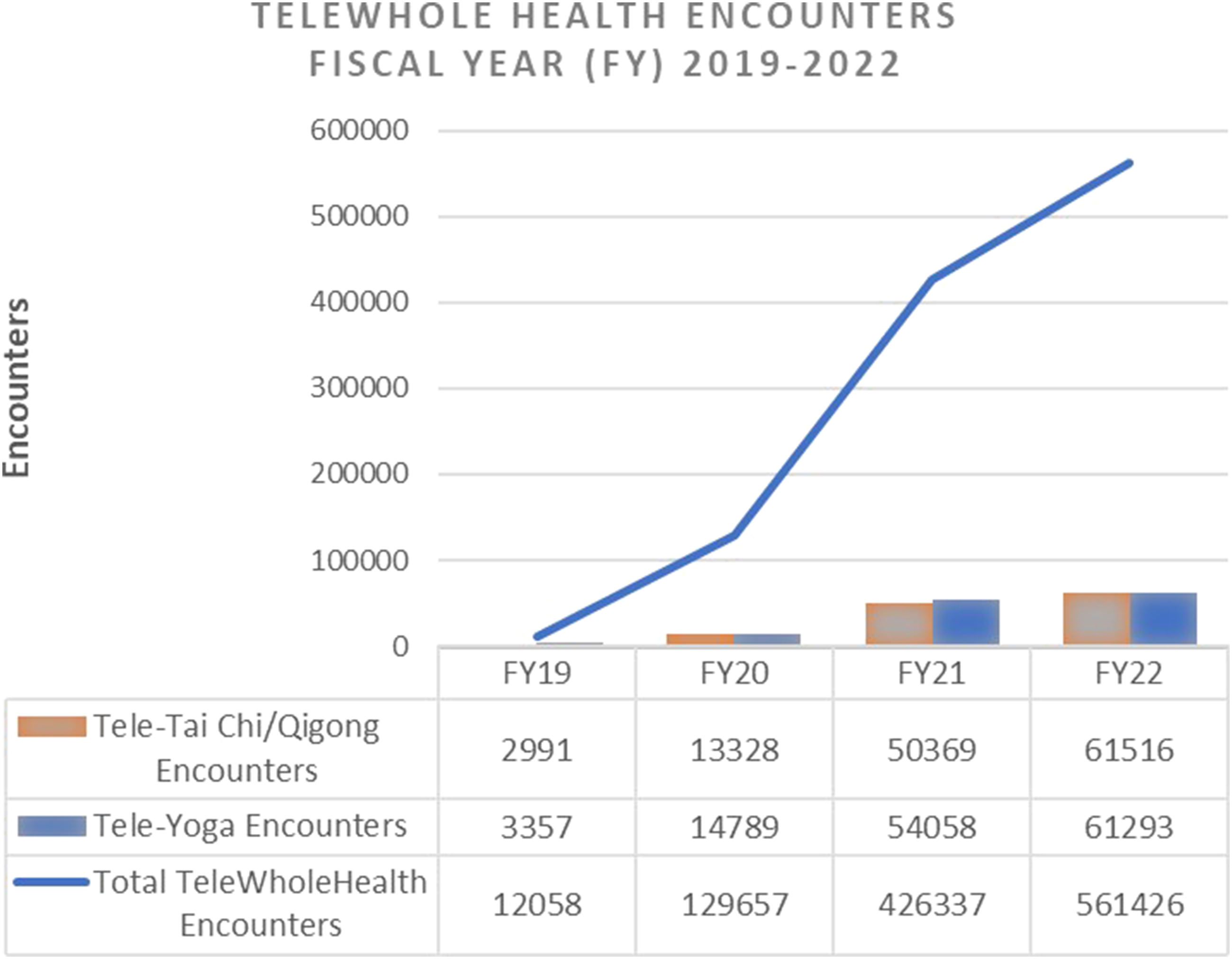
Given the rapid adoption of telehealth since the onset of the COVID-19 pandemic, we aim to share lessons learned from remote delivery of mindful movement as part of clinical care and wellness programs in the VA and discuss opportunities for the future. In this article, we highlight examples of virtual mindful movement within VA based on our collective experience implementing and evaluating tele-CIH including mindful movement modalities as clinicians, researchers, and national Whole Health champions and CIH program lead. Although the VA supports a variety of mindful movement modalities, we/the authors share a common background as yoga teachers and yoga therapists. The examples that follow/or that have informed what follows include remote delivery of mindful movement as part of a multisite tele-yoga program focused on well-being, within diabetes/hypertension clinics, and the multimodal Step-3 Tele-Pain Empower Veterans Program (EVP).
Benefits of Remote Delivery of Mindful Movement within an Integrated Health care System
Convenience and Decreased Travel Burden
Remote delivery of mindful movement provides opportunities to increase access to modalities that might otherwise be inaccessible to Veterans due to challenges traveling to a VA facility. In addition to addressing barriers for rural-dwelling Veterans such as travel distance and cost, the convenience of accessing tele-mindful movement extends to those for whom travel causes increased pain or stress with prolonged driving or riding including those who also live in metropolitan areas impacted by traffic and long drive times. Virtual sessions enable the participant to attend from where they are, “as they are,” such that regardless of location, if they are having a flare up or difficulty getting out of bed, they can still join and take part in the class to the extent possible in that moment. This ability to join the class regardless of how much they can participate supports motivation and engagement to continue to try movement rather than feel discouraged on a day they cannot travel to attend.
The convenience of virtual mind-body movement was highlighted by participants in a recent evaluation of multi-site tele-yoga program focused on wellness, funded by the VA Office of Rural Health. A program evaluation survey administered to tele-yoga participants with ≥2 or more encounters between October 2021 and March 2023, with 166 survey respondents. Veterans rated convenience highly (mean 3.6, SD .7 on a 4-point scale; 1 [poor] to 4 [excellent]). 65% reported that the online format made it “a great deal” easier to attend than traveling to a facility (mean 9.0, SD 2.0 on a 10-point scale; 1 [not at all] to 10 [a great deal]. Prior to participating in VA tele-yoga classes, only 15% of these Veterans were engaged in a regular yoga practice at the time of the survey, 44% had done yoga in the past, and 41% had never tried yoga. Compared to urban and younger Veterans (<65 years), rural and older (≥65 years) had significantly higher rates of engagement/attendance rates. While there is a possible shift in the way that social interaction is experienced, some may appreciate the ability to connect through the virtual environment even when they are unable to leave their home. A consideration for these virtual classes becomes how to support social connection through this forum and the examples of program below illustrate this inclusion.
Increased Accessibility Through Movement Options and Translation to Home Practice
Accessibility for virtual delivery extends beyond travel burden to the options for movements themselves. In-person group classes can be restricted in the options and adaptations for movements due to limitations of the space. Examples include the need for adequate wall space, or chairs, or tables, for balance and support of standing postures. Another important example is incorporating supine movements in group classes in which people with mobility limitations may be unable to access if there are limited tables/plinths for a higher surface and the person is unable to get up and down from the floor. At-home classes enable the person to access these supine postures from their bed or couch. This allows them to experience the benefits of varied supine or side lying positions which alter the relationship to gravity and can decrease muscular effort, enhance relaxation, and help to focus a movement on a discrete area of the body. This level of accessibility of position provides greater adaptations and modifications for movement and can be empowering for the person to maintain the motivation to participate in classes as they can find a version that suits their needs. Finding the supports and props to do these movements at home can also provide insight for the translation of these practices into their everyday life.
Increased Focus on Cultivating Interoceptive Awareness
Mindful movement modalities are well-suited to support the person in cultivating interoceptive awareness, which is the process of sensing, interpreting, and regulating inner bodily signals. 4 Prior to COVID-19, using hands-on assists with mindful movement may have been a more common practice, particularly when taught by practitioners who are also manual therapists. The virtual environment helped provide the impetus for building interoceptive skills for safe movement aligning with supporting inner bodily awareness in mindful movement. The participant can explore and experience their own optimal alignment and safe movement in a process of self-discovery. Rather than relying on the teacher’s adjustment or external guidance, the participant is empowered to find their own unique ways to move safely. This focus on building interoceptive skills and empowering the person to move based on their own internal guidance aligns with a trauma-informed and patient-centered approach that supports patients/participants to develop awareness of what they need for safe movement for both virtual and in-person classes.

Special Considerations and Challenges with Virtual Mind-Body Movement
Technical and Logistical Challenges
Technology-related barriers, including internet connectivity and difficulty with audio-visual aspects of are commonly noted challenge with telehealth. 5 Remote delivery of mind-body movement poses an added challenge in that participants and facilitators are mobile during the class, and not always sitting close to their device’s camera or microphone. It is therefore imperative to ensure that movement facilitators have high quality microphones and cameras and adequate lighting to optimize the audio-visual experience for participants, some of whom might access the virtual groups from devices with small screens such as tablets or smart phones. The home environment of participants has been identified as a potential barrier to virtual mind-body movement. 6 Unlike other telehealth providers, mindful movement facilitators must also have a large enough physical space to conduct remote classes so they can be far enough away from their camera to have a full-body view. Similarly, participants may need some creative ideas as to how to utilize their space and available items that can be used as props (eg, sofa cushion for bolsters, plastic containers for blocks, stable chairs, etc.). In addition, a private physical space for movement facilitators is also needed to protect patient privacy and have private conversations with participants. Likewise, a private space for the participants is encouraged for the privacy of others in the class.
Choice of video platform can greatly impact user experience of remotely delivered mindful movement. During the rapid shift to telehealth during the COVID-19 pandemic public health emergency, regulations around telehealth were greatly relaxed, with health care systems allowing the use of nonclinical platforms such as Zoom, FaceTime, and SKYPE for clinical care. 7 The VA’s secure telehealth platform, VA Video Connect, was not initially designed for groups and underwent several platform upgrades to improve the user interface for group visits. Ideally, platforms used for movement-based groups allow the instructor to pin or spotlight their video for participants, permit remote muting of participants, and allow for separate microphone and audio sharing to facilitate any music that instructors may use during the class. Technology-related barriers are important to address, as these are substantial contributors to participant drop-off. Among survey participants in the above-mentioned tele-yoga evaluation, those who dropped off after only 1 encounter were more likely to use a smaller device (phone/tablet vs laptop/desktop) than those with continued engagement. However, despite some technological challenges, 96% of the survey respondents rated the quality of the classes as “good to excellent.”
Teaching Mind-Body Movement Modalities Remotely
Especially in tele-mindful movement classes focused on well-being, one challenge for instructors is that classes are often heterogeneous and include participants with different health conditions, mobility, and varied ages. As such, it is important for movement facilitators to develop skills for tailoring classes to ensure that all participants benefit from the class. Despite the challenge facing instructors to tailor classes for a wide variety of participants, survey results from Veterans participating in the ORH tele-yoga program indicated that 88% of respondents agreed that instructors are knowledgeable in adapting poses and movements to their specific needs. Another challenge to remotely delivered care is that mindful movement instructors may or may not have training in teaching in an online format and in how to support participants to develop interoceptive skills. In part to address these challenges, VA is developing a national 200-hour yoga teacher training for VA staff with provision of yoga in their scope of practice, that will be fully remote and emphasize both technical aspects and teaching of interoceptive skills to be successful in the remote environment.
Physical and Psychological Safety
Both physical and psychological safety are important to consider for virtual mindful movement. Assessing physical safety in a virtual group movement class can present unique challenges for instructors. 8 Safety features are present within the VA Video Connect (VVC) system, the secure telehealth delivery platform in the VA, so that if an emergency arises there are steps that can be taken to support the participant. Mindful-based movement approaches like yoga and tai chi are relatively low-risk physical activity and in an online setting a more conservative approach is indicated and needed. In addition, some sites require medical clearance. Having participants position their cameras appropriately to observe alignment during the practice is often preferred by instructors and a common challenge to teaching in the virtual space. 6 However, instructors must also consider the privacy and safety concerns of participants who prefer to practice without a camera or with the camera turned off. While personal spaces can provide added insight and clues into a persons’ life, participants may not want to share these spaces in a group environment. Offering participants the ability to blur their virtual background may alleviate these concerns to an extent, but may not be enough for psychological safety. In addition, the person may not feel comfortable doing movement with their cameras on for a variety of reasons. We have found that some people may also prefer virtual classes if they feel self-conscious about their body or about moving in front of people. This opportunity to support a return to movement from the safety of one’s own space may be another benefit of virtual classes. This need for a trauma-informed approach and supporting physical and psychological safety again calls for the virtual mindful movement facilitator to understand how to support interoceptive skills building and self-efficacy for safe movement.
See Table 1 for summary of potential benefits and challenges of remote delivery of mindful movement within health care systems (Table 1).
Opportunities for Integrating Mindful Movement within Tele-CIH Medical Groups
Virtual mindful movement and tele-CIH provide a unique opportunity to incorporate these approaches as part of clinical treatment plan. The use of mindful movement has been shown to improve health outcomes in patients with chronic pain, chronic stress, and chronic disease, but participating in mindful movement within a well-being group or in a general class can often be challenging for this population. Patients with chronic disease and disability require significant modification of instruction and reassurance for physical and psychological safety that can be difficult to accommodate within a well-being group model. Additionally, patients with significant medical disease already struggle to maintain the number of clinical visits and appointments scheduled for their medical care. While telehealth and virtual visits certainly assist with the burden of travel for these visits, the sheer number of clinical encounters these patients require makes the addition of any virtual CIH well-being group an added burden. Furthermore, a virtual mindful movement and tele-CIH embedded within a clinical care model allows patients to understand the health impact of these mind-body approaches specific to their disease process which has been shown to improve health outcomes. 9 In the ORH tele-yoga program evaluation survey, 79% of respondents agreed that attending tele-yoga for wellness through the VA helped them to engage more in their health care overall. Because virtual mindful movement, and a Whole Health approach to care, have been shown to improve engagement with health care, these approaches are specifically well suited to incorporate into health care settings. 10
Example: Incorporating Yoga Into Virtual Whole Health for Diabetes Group Visits
One example of virtual CIH embedded within a clinical care model is the Whole Health for Diabetes group clinic. This 2-hour virtual shared medical appointment that introduces and teaches the concepts of Whole Health and CIH within the context of comprehensive diabetes care. Led by a diabetes specialist and a yoga instructor, this 2-hour group clinic allows veterans to learn about the positive impact of mindful movement on both glycemic control and diabetes-related distress. 11 After didactic and group discussion, the group is then led through a mindful movement practice followed by an opportunity to debrief and reflect on the impact of the CIH practice in real-time, with a group of peers. The group clinic model of virtual mindful movement allows patients to engage in the practice within a community that understands the specific benefit of these approaches on their medical care. This model has been shown to improve glycemic outcomes. 12 In the future, pairing virtual mindful movement with clinical care also offers the opportunity to leverage digital wearable technology into CIH delivery. While the data is still emerging, the use of a continuous glucose monitor may provide a real-time biomarker represents a novel approach to evaluate the impact of virtual mindful movement in clinical care.
Another benefit of incorporating virtual mindful movement within a medical model of care is that it allows participants to enjoy a tailored experience that is specific to their health needs. In this way, patients with chronic disability from their medical condition are less likely to be excluded and feel safer to engage in mindful movement modalities. This provides an opportunity for patients to meet others and to share experiences and insights along the way.
Example: Use of Mindful Movement Within the Tele-Pain Empower Veterans Program
The Empower Veterans Program (EVP) is a Step-3 Tele-Pain interdisciplinary remotely delivered program for veterans with high impact chronic pain. 13 The 10-week program is delivered for 3 hours a week, 1 day a week and includes 3 classes each session: (1) Whole Health and Mindfulness training; (2) Acceptance and Commitment Therapy; and (3) Mindful Movement. The mindful movement class is led by physical therapists who are also yoga teachers and integrates an experiential body-based learning of the topics in the other 2 classes with pain neuroscience education and interoceptive skills-building. 14 For example, participants explore their own personal values throughout the program and the mindful movement classes focus on how the experience of connecting to one’s values affects the body (muscle tension, breath, quality of movement) and can set the stage for safe movement. The mindful awareness and self-compassion taught in the other 2 classes also become the lens through which movement is explored and “tried on” to find safer ways to move. Integrating the topics of the other classes into mindful movement helps the person to gain insight into how thoughts, emotions, outer stimuli affect the body (muscle tension, posture, breath) and how changing what is happening in the body can shift mood and relationships to outer stimuli for greater body-mind-behavioral regulation. The class provides a safe place to learn to adapt movement, provide insight into the importance of movement for whole person well-being and how to integrate mindfulness with movement. Ultimately the person is supported in learning that they have the tools to continue safe movement in daily life and attending community movement classes if desired. The group format also enables the shared experience to be highlighted and learnings from 1 another to be shared.
Future of TeleWholeHealth and Virtual Care at VA
The COVID-19 public health emergency provided an opportunity to better understand the potential benefits and challenges of virtual care. Since then, a blended model of virtual and in-person care seems to be an optimal choice to best support the needs of patients with complex and chronic medical conditions. An internal strategic plan and goals were developed by key stakeholders in VA to provide a more strategic way forward for the vision of TeleWholeHealth in VA and to ensure that TeleWholeHealth is not a siloed effort. The overarching focus of the plan is to ensure virtual services provided Veterans and staff are easy to understand, accessible, and high quality.
The opportunities presented by virtual mindful movement have been discussed in this paper including increased access for groups historically not represented or served by classes in community studios or for whom traveling to health care facilities is inaccessible. The rapid adoption of virtual mindful movements also brings challenges to implementation and the lessons learned from the VA’s transition to virtual care highlight the importance of providing appropriate support to both Veterans and staff. These learnings can also be used by the wider health care community to consider and develop further best practices in outreach for tele-delivery of mindful movement for various patient populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Dr Nicosia is supported in part by the VA Office of Rural Health, Veterans Rural Health Resource Center-Iowa City (NOMAD PROJ-03602).