
Abstract
Background
Mindfulness in Motion (MIM) is a workplace resilience-building intervention that has shown reductions in perceived stress and burnout, as well as increased resilience and work engagement in health care workers.
Objective
To evaluate effects of MIM delivered in a synchronous virtual format on self-reported respiratory rates (RR), as well as perceived stress and resiliency of health care workers.
Methods
Breath counts were self-reported by 275 participants before and after 8 weekly MIM sessions. MIM was delivered virtually in a group format as a structured, evidence-based workplace intervention including a variety of mindfulness, relaxation, and resilience-building techniques. Participants counted their breaths for 30 seconds, which was then multiplied by 2 to report RR. Additionally, participants completed Perceived Stress Scale and Connor–Davidson Resiliency Scale.
Results
According to mixed effect analyses there were main effects of MIM Session (P < .001) and Weeks (P < .001), but no Session by Week interaction (P = .489) on RR. On average, RR prior to MIM sessions were reduced from 13.24 bpm (95% CI = 12.94, 13.55 bpm) to 9.69 bpm (95% CI = 9.39, 9.99 bpm). When comparing average Pre-MIM and Post-MIM RR throughout the MIM intervention, Week-2 (mean = 12.34; 95% CI = 11.89, 12.79 bpm) was not significantly different than Week-1 (mean = 12.78; 95% CI = 12.34, 13.23 bpm), but Week-3 through Week-8 demonstrated significantly lower average Pre-MIM and Post-MIM RR compared to Week-1 (average weekly difference range: 1.36 to 2.48 bpm, P < .05). Perceived stress was reduced from Week-1 (17.52 ± 6.25) to after Week-8 (13.52 ± 6.04; P < .001), while perceived resiliency was increased from Week-1 (11.30 ± 5.14) to after Week-8 (19.29 ± 2.58); P < .001).
Conclusion
Thus far, completion of MIM sessions has shown acute and long-term effects on self-reported RR, but more research is required to determine the extent of improved parasympathetic (relaxed) states. Collectively, this work has shown value for mind–body stress mitigation and resiliency-building in high stress acute health care environments.
Keywords
Introduction
Acute and chronic exposures to physical, emotional, and psychosocial stressors increases risk of various negative health outcomes including burnout, suicidal ideation, suppressed immunity, obesity, substance abuse, and cardiovascular disease. 1 When stress levels exceed an individual’s ability to manage or cope, allostatic overload (i.e., the cumulated effects of chronic stress on mental and physical health) may persist through various symptoms such as irritability, nervousness, feeling overwhelmed, and having difficulty concentrating or remembering.2,3 If allostatic overload persists, the physiological stress response system becomes activated easier, more frequently, and for longer periods of time.2,3 Unfortunately, the accumulation of stressors can reduce workplace retention, safety, and efficacy due to burnout, perceptions of emotional exhaustion and depersonalization (i.e., cynicism and reduced empathy), and a low sense of personal accomplishment from work. 4 The deleterious effects of chronic stress (e.g., anxiety, depression, and cardiovascular disease risk) may arise through the autonomic nervous system via elevated sympathetic states (e.g., arousal or stress) and diminished parasympathetic (e.g., vagal and relaxation) tone. 5 Therefore, intervention strategies for protecting against chronic stressors often aim to improve autonomic balance toward parasympathetic dominance and alleviated sympathetic tone by improving resiliency and coping mechanisms, 1 which warrants further investigation in occupations with continuously increasing demands such as first responders and health care providers.
Current evidence-based solutions to counterbalance allostatic overload include mind–body resilience-building interventions and mindfulness based interventions (MBI) which may include meditation, yoga, strength training, and aerobic activity.3,6,7 An example, Mindfulness Based Stress Reduction (MBSR), is a structured psycho-educational intervention (typically 8-week, 26 hour group structured) that employs mindfulness and meditation practices aimed to improve the mind–body response to a variety of health related concerns including accumulated stress.8-12 Being mindful generally involves sustained moment-to-moment awareness of physical sensations, perceptions, affective states, thoughts, and imagery. According to prior research, mindfulness training has demonstrated efficacy for promoting self-care and well-being while reducing stress in a variety of populations including but not limited to medical, social, educational, intercultural, first responder, and work-site settings.8,9,13 However, due to concerns involving the required time commitment of traditional MBSR for high stress occupations, such as first responders and health care workers, some have created and demonstrated the benefits of modified MBIs such as the Mindfulness in Motion (MIM) program at The Ohio State University. 6 The MIM program is based upon MBSR, but is less time intensive (1 hour group sessions over 8 weeks, daily 10 minute practices, and no retreat) and can be completed at work in work attire. Due to the variety of MBIs and modes of delivery (e.g., virtual vs in-person) continued research is required to establish support of specific interventions for improving stress and resiliency as well as relevant physiological markers.
Both MBSR and MBIs may impact parasympathetic tone, as mindfulness practices often involve some form of awareness to breathing 14 which modulates the vagus nerve and parasympathetic dominance. 15 Therefore, it is to be expected that heart rate variability (HRV) would increase and respiration rates would decrease as a result of mindfulness practices, which has been demonstrated in previous research.16-19 Considering the relation of respiration rates with sympathetic (fast breathing) and parasympathetic (deep slow breathing) states, it brings to question whether MBIs can influence breathing rates acutely (during the session) as well as chronically (slowed breath rates over time). Some previous researchers have observed slowed respiration rates during formal mindfulness practices, demonstrating successful acute effects of mindfulness on parasympathetic modulation.16,17,20,21 However, the impact on respiration rates may be driven by the level of attention to breathing during the mindfulness practice, as controlled respiration during practice will intently slow respiration rates by notable magnitudes. 20 Long term mindfulness practices have shown mixed results, as some have found chronically reduced respiration rates 18 while others did not observe attenuated respiration rates following formal mindfulness practices. 20 Traditional MBSR interventions,10,11,14 MBIs, and original mindfulness Buddhist traditions 22 contain forms of focused, deep and slow, controlled breathing that has been shown to be effective for calming the body and mind in healthcare settings15,23 likely from modulated parasympathetic states. 24
Although it appears evident that mindfulness practices may slow respiration rates during formal practices, it is still uncertain how respiration rates may be changed over the course of long-term mindfulness practices (i.e., 8-week MBSR programs). Further, biological evidence using respiration rates in conjunction with stress and resiliency outcome questionnaires will help understand the mind–body interplay within MBIs. According to a recent systematic review, evidence was considered limited and uncertain as to the effectiveness of MBIs for improving resiliency and reducing symptoms of depression and stress in healthcare workers. 25 Therefore, this work aims to evaluate 1) effects of a single mindfulness session (daily acute effect) on self-reported respiration rates, 2) the weekly changes (longitudinal chronic effect) in respiration rates across an 8-week mindfulness intervention, and 3) changes in perceived resiliency and stress to provide evidence of possible sustained mind–body well-being in healthcare workers. Further, the current study will evaluate acute changes in respiration rates during a mindfulness session across each week of the MIM 8-week intervention to determine if acute changes differ across weeks, which will identify whether focus on attentive breathing techniques impacts potential slowed respiration over time.
Methods
Study Design
Study design was a non-randomized single arm, pre/post study at Ohio State University Wexner Medical Center (OSUWMC). Study approval (study number 2017B0321) was obtained by The Ohio State University Institutional Review Board prior to participant recruitment.
Mindfulness in Motion (MIM) is a modified MBI to deliver mindfulness practices in less time than traditional MBSR, in addition to enhanced use of yogic movement and relaxing music. The MIM program was created to address time commitment concerns in various populations, such as first responders and healthcare workers. Traditional MBSR protocols may require an orientation session, 8 weekly classes of 2.5–3 hours in duration, and a 7 hour retreat between week 6 and 7. Whereas, MIM requires a single 1-hour weekly group meeting and ∼10 minutes of mindfulness home practice at least 3 times per week for 8 weeks. The MIM protocol has been previously published and was developed as part of an organizational initiative to improve resiliency and work engagement of employees exposed to stress and at high risk of developing burnout. 6 For the purposes of this study, we have evaluated cohorts that completed MIM in synchronous virtual group-based formats aimed to further permit the use of mindfulness training for busy working adults in healthcare settings. Respiration rates were self-recorded by participants before and after each MIM session, while perceived stress and resiliency were measured 1 week prior to and within 1 week after completion of the 8-week MIM intervention.
The single one-hour structured group sessions included an emphasis on bodily relaxation with soft music in the background and discussion of mindfulness awareness of various cognitive, physical, relational, and communicative habits. Participants were able to individually engage in pragmatic daily mindfulness practices on a password protected web-based platform (https://mindfulnessinmotion.osu.edu/), via a variety of audio and video mindfulness practices (∼10 minutes, 3-4 × per week). The protocol was originally developed based on the premise of shorter MBIs yielding similar results to longer protocols of traditional MBSR.6,26 Additionally, MIM was designed to be easily implemented during work hours either seated or standing and without the need to change clothing or shoes.
Participants
Demographics of all Participants (n = 275) that Entered the Study.

Mindfulness in Motion Protocol
Each one-hour weekly session of the 8-week program followed the same general structured format outlined in Figure 1 and previous investigations.6,27 A MIM program fidelity checker assured that all sessions followed the same format across cohorts.
28
The prompts, educational material, and home practice directly related to each weekly theme (Table 2). In the beginning of the sessions, relaxing music was in the background to set the climate for MIM while the facilitator opened with the intent of the session and program: resiliency building and stress reduction through mindful awareness of habitual patterns of stress reactivity. Participants self-recorded their Pre-MIM breath counts and then were reminded of the prompts for the current session reflection. The educational materials were delivered in a 15-minute pre-recorded evidenced-based presentation on topics including stress and work-related stress, theoretical material related to mindfulness, the somatic mind/body connection, relaxation, yoga, meditation, self-awareness, and bodily cues relating to emotional reactivity and the relation of these topics to specific healthcare workplace stressors. Next, participants and the trained MIM facilitator engaged in a discussion about the mind–body prompt reflection for the weekly session. The discussion of the reflective prompt lasted 20 minutes and was voluntary and participants were silent unless they chose to verbalize their reflections to the class, which most participants chose to do. Lastly, participants were led through a mind body relaxation practice via a pre-recorded video (15 min) relating to the weekly theme. The sessions ended with the self-reported breath count and participants were reminded of their home practice for the next week. The home practice consisted of completing an individual 10-minute guided audio/video mindfulness practice at least 3 times, in addition to the respective weekly themed individual mindfulness practice (Table 2). Diagram of the approximate timelines for Mindfulness in Motion (MIM) sessions. Weekly MIM Theme, Group Activity, and Individual Home Practice.

Respiration Rates
Respiration rates were obtained by asking participants to count their inhalations for 30 seconds while placing their right hand over their chest. The MIM facilitator timed the breath count to allow participants to focus on counting their breath. Participants recorded their self-reported breath counts (counting inhales only) at the start and end of each MIM session. The 30-second breath counts were multiplied by 2 and reported as respiration rates in breaths per minute. These methods were included in the mindfulness practice itself since it raises self-awareness, serves as an additional calming technique, and was similarly used in prior research. 29 Breath counting has been found to be a valid physiological and behavioral measure in mindfulness training when compared to respiratory belts as the tracking tool, and this remained true over various tests up to ∼18 minutes in duration. 30
Perceived Stress and Resiliency
Perceived stress was measured using the 10-item Perceived Stress Survey (PSS) which is intended to determine the degree to which individuals perceive life events as excessively stressful relative to their ability to cope. 31 Participants rated each of the 10 questions from 0 to 4 (Never – 0, Almost never – 1, Sometimes – 2, Fairly often – 3, Very often – 4) indicating how often the statement applies to them during the last month. Questions included: 1) “How often have you been upset because of something that happened unexpectedly?”, 2) “How often have you felt that you were unable to control the important things in your life?”, 3) “How often have you felt nervous and stressed?”, 4) “How often have you felt confident about your ability to handle your personal problems?”, 5) “How often have you felt that things were going your way?”, 6) “How often have you found that you could not cope with all the things that you had to do?”, 7) “How often have you been able to control irritations in your life?”, 8) “How often have you felt that you were on top of things?”, 9) “How often have you been angered because of things that happened that were outside of your control?”, and 10) “How often have you felt difficulties were piling up so high that you could not overcome them?”. Scores for items 4, 5, 7, and 8 were reversed and then scores for all items were summated for a total stress score, which is considered valid and reliable. 32
Perceived resilience, referred to as the ability to maintain good functioning in face of stress or trauma, was evaluated using the 10 items version of the Connor-Davidson Resiliency Scale (CD-RISC). 33 Participants rated each of the 10 statements from 0 to 4 (Not true at all – 0; Rarely true – 1; Sometimes true – 2; Often true – 3; True nearly all the time - 4) indicating how often the statement applies to them. Questions included: 1) “I am able to adapt to change.”, 2) “I can deal with whatever comes my way.”, 3) “I see the humorous side of things.”, 4) “I believe coping with stress strengthens me.”, 5) “I tend to bounce back after illness or hardship.”, 6) “I believe I can achieve my goals.”, 7) “Under pressure I can focus and think clearly.”, 8) “I am not easily discouraged by failure.”, 9) “I think of myself as a strong person.”, 10) “I can handle unpleasant feelings.”. The scores for each item were summated to obtain a total resiliency score for analysis. The 10 items version of the CDRISC is considered valid and reliable (alpha = .85). 34
Statistical Analysis
Statistical procedures were performed in R version 4.1.2 (R Foundation, Vienna, Austria, https://www.R-project.org) with an alpha level of P < .05. To understand the influence of MIM on respiration rates, mixed effect analyses were used. The fixed effect of Time (8-week intervention, level 1) was nested within subjects (level 2, random effect), while MIM effect from Pre-to Post-MIM session served as the conditional explanatory variable. If a significant effect was identified, post-hoc analyses were conducted using the “emmeans” function with Tukey method P-value adjustments. Additionally, Wilcoxon Signed Rank tests and their respective effect sizes were used to determine statistical differences from Pre-MIM to Post-MIM for perceived Stress and Resilience.
Results
Respiration Rates (RR) Per Minute for Weekly Mindfulness in Motion Sessions by 275 Participants.

*, Indicates statistically significant difference compared to Week-1 Baseline at P < .001.
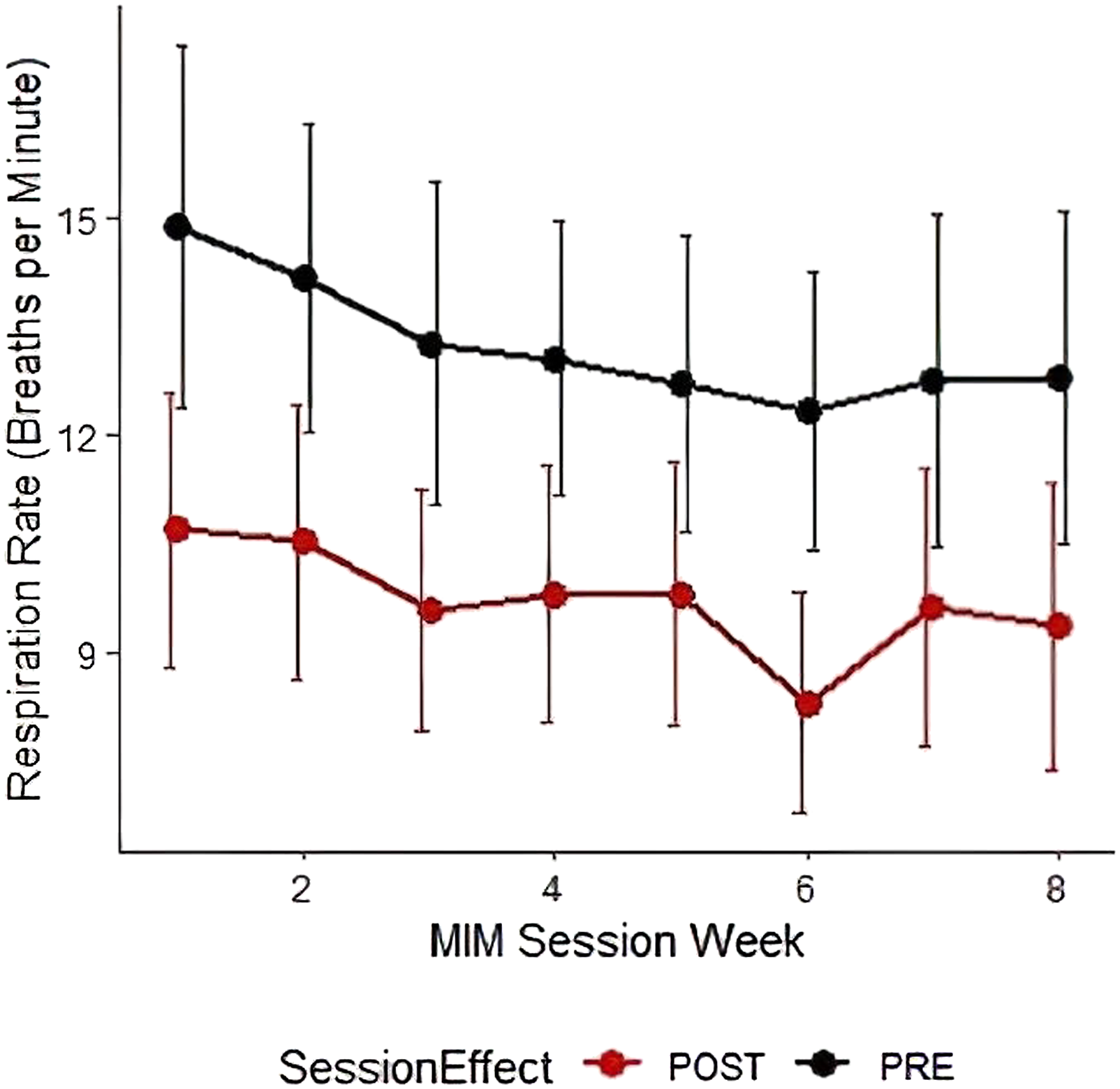
Respiration rates per minute across each week at the start (PRE) and end (POST) of Mindfulness in Motion (MIM) sessions.
Participants’ perceived stress had significant, small (Effect Size = .299) reductions from Week-1 (17.52 ± 6.25) to after Week-8 (13.52 ± 6.04). Furthermore, participants reported significant, large improvements of resiliency after completing the 8-week MIM intervention (CD-RISC: Week-1 = 11.30 ± 5.14, Week-8 = 19.29 ± 2.58; Effect Size = .727).
Discussion
Despite stress being an important aspect for psycho-physiological adaptations, unaccustomed acute stressors or chronic accumulations of stressors are associated with mental and physical illnesses (i.e., depression, anxiety, and cardiovascular disease). Hence, the importance of investigating interventions that may alleviate negative responses to stressors through improved resilience and modulation of parasympathetic nervous system responses. Thus, the current study aimed to investigate the effect of MIM, on self-reported respiration rates, as well as perceived stress and resiliency. In agreement with the original hypothesis, self-reported respiration rates were reduced following individual MIM sessions. Further, self-reported respiration rates at each session (Pre-MIM and Post-MIM) were lower in weeks 3–8 compared to baseline (Week-1; Table 3). The pre-MIM self-reported breath count decreased by 4 breaths over the 8 weeks, which points to a sustained lowering of the participants baseline respiration rates over the course of the 8-week intervention. Interestingly, the week with an activity most focused on mindful breathing (Week 6-straw breathing) resulted in the largest magnitude of reduction in respiration rates albeit not significantly different than other weeks (Table 3; Figure 2). The MIM intervention also had positive influence on perceived levels of stress and resiliency. One major strength of the current findings is their ecological validity since data were collected virtually in healthcare settings. Thus, the MIM program improved self-reported respiration rates, as well as perceived stress and resilience, while participants were in real world healthcare environments handling exposures to complex stimuli.
The MIM program is an MBI, created to facilitate resiliency and healthy strategies for processing stressors in health care settings. Since stressors promote physiological reactions including sympathetic nervous system responses of rising blood pressure, heart rate, and respiration rate, the purported counteractions of MBIs include parasympathetic modulations. However, a recent review of MBSR has indicated that various studies support that it can decrease systolic and diastolic blood pressure but have not demonstrated substantial and consistent effects on heart rate variability or respiration measures. 35 They suggested that respiration rates may show the greatest responses during mindfulness practices. Since mindfulness practices bring awareness to one’s breath, 14 respiration rates expectedly decrease acutely.16-19 It is evident that standardized controlled breathing during mindfulness practice will intently slow respiration rates. 20 For example, one study showed that self-reported breath counts (for 30 seconds) were decreased by 2 breaths per minute after learning and practicing mindfulness breathing techniques during 2 regularly scheduled 30-minute staff meetings with respiratory therapists. 29 Thus, the amount of focused awareness directed towards breathing within a mindfulness session is an important factor to consider. Focusing on breath throughout weekly lessons and counting breaths at the start and end of each session may have evoked further awareness to the breath and increased longitudinal respiration rate responses to MIM compared to what some prior literature has found utilizing MBSR. 35
The current findings suggest that average self-reported respiration rates in health care providers decreased throughout the 8-week intervention and Post-MIM breaths were slower than Pre-MIM within each MIM session (Table 3, Figure 2). Averaged session (Pre-MIM and Post-MIM) self-reported respiration rates were slower during weeks 3 through 8 compared to week 1 (Table 3, Figure 2). This main effect and lack of significant interaction would suggest that both Pre-MIM and Post-MIM respiration rates decreased similarly across the intervention (average change from Pre-MIM to Post-MIM ranged from 2.9 to 4.1 bpm). The Pre-MIM respiration rates were considered resting levels since they were taken under similar conditions within individuals prior to the MIM session. Thus, although these conclusions should be taken cautiously, these initial findings may be suggestive of more dominant parasympathetic states by the end of the program which may begin to occur as early as 3 weeks into the program. As seen in previous research, the longitudinal decreases in respiration rates may be a result of attentive focus on breathing and modulating one’s physiological arousal to surrounding stimuli. 18 Experienced meditators, who are presumably more self-aware, may be more able to accurately sense respiration responses (e.g., more rapid breathing). 36 Novice mindfulness practitioners have also noted greater decreases in respiration rates, compared to control groups, when focusing attention on respiratory sensations. 37 In general, mindfulness training seems to promote the ability to sense and alter physiological responses to environmental stimuli via respiration patterns. However, further investigation into physiological responses throughout other parts of the day and follow-ups to the intervention are warranted to determine stronger evidence of chronic physiological improvements over the duration of the intervention, and possibly beyond intervention end.
Over time, MBIs are thought to provoke improvements in habitual reactions to life experiences including stressors. Initial MIM cohorts, which were on-site in healthcare settings, noted increased perceptions in resiliency and well-being along with decreased stress and self-reported respiration rates. 6 The current findings, that include the MIM program delivery in a virtual format, suggest similar outcomes of reduced stress and increased resiliency in addition to the slowed self-reported respiration rates. In other populations, such as elite football athletes, mindfulness training once a week for 8 weeks improved resiliency, self-confidence, and emotion regulation. 38 According to a recent systematic review, MBIs (majority of which were delivered in-person, 29/44) were generally identified as effective for improving resiliency and reducing symptoms of depression and stress immediately following interventions of more than 12 hours or sessions (18 of 44 articles). 25 However, the authors noted the evidence was still limited and uncertain and suggested further research be conducted to improve the strength of the findings especially for longer-term impact. Chronic impact of MBI was found in an academic healthcare center, where participants noted improvements in happiness, satisfaction with life, gratitude, mindfulness, spirituality, and stress immediately after and 3 months following a 12-week in-person Stress Management and Resiliency Training program. 39 Whereas other researchers have found traditional MBSR to be effective at reducing short-term perceived stress in healthcare workers, but not at the 4-month follow-up. 40 Considering the undue burdens of burnout and related symptoms in healthcare workers, continuing to understand and verify the effectiveness of MBIs on stress and resiliency is warranted. 41 The current findings provide further support that MBIs, such as MIM which also requires less time commitment compared to traditional MBSR, can serve as a tool to improve healthcare worker mental health and resiliency and reduce potential burnout amongst other negative health consequences from chronic stressors.41,42
These findings are not without limitations. These include lack of randomization and controls, participants counting their own breath as a measure of respiration rates, and uncontrollable confounding factors such as varying levels of participation in extracurricular mindfulness activities. Healthcare workers often assess respiration rates by counting patient’s breath, which has received criticism for this method’s potential inaccuracies. 43 However, self-reported breath counting has shown to be a physiologically valid measure for mindfulness sessions when compared to respiratory belts as the criterion measure, 30 and has been previously used to assess mindfulness training outcomes in healthcare workers. 29 The aforementioned investigation also reported mind wandering to negatively influence the accuracy of breath counting during lengthier durations of ∼15–18 minutes. 30 For this reason, the team originally chose to have participants count their breath for 30 seconds to reduce the potential impact of mind wandering on breath count accuracy. Due to the high stress nature of health care environments resulting in limited time availability, others have also explored valid respiration rate solutions within 30 seconds.44,45 With additional supporting research for further validation, self-reported breath counts may be an efficient cost-effective solution for monitoring effectiveness of mindfulness training interventions. These environments include virtual settings while also bringing concentrated attention to one’s own breath. With the evolution of this work and improvements of remote monitoring systems (eg, wearable sensors), we have fostered a multidisciplinary team and necessary equipment to evaluate the effect of MIM on various physiological measures (e.g., respiration rates, heart rate variability, and sleep) at various timepoints (e.g., before, during, and after MIM, daily resting measures). Using these technological devices will verify or dispute the accuracy of self-reported respiration rates as an accurate method of data collection.
Conclusions
It appears evident that respiration rates remain an important factor in mindfulness training research and resultantly should continue to be investigated as it is a prominent part of the practice. These psycho-physiological adaptations can be used to supplement the information gained from perceived self-report scales as these measures may have a degree of bias. 35 To summarize the current study, the findings included significant reductions of self-reported respiration rates from Post-MIM to Pre-MIM when collapsed across weeks. These findings may be interpreted as showing significantly slower self-reported breath rates at Post-MIM compared to Pre-MIM for each session. Secondly, averaged Pre-MIM and Post-MIM self-reported breath rates were significantly slower at weeks 3 through 8 compared to week 1. These findings suggest similar changes in self-reported respiration rates across weeks for Pre- and Post-MIM timepoints. In conclusion, completion of MIM slowed self-reported respiration rates from Pre-MIM to Post-MIM each session and across the 8-week intervention. These findings are concomitant with statistically significant reductions in perceived stress and large increases in perceived resiliency after completing the 8-week intervention. Verification of self-reported respiration rates in future studies via a wearable device will add support to the value of MIM as a pragmatic intervention valuable for slowing respiration and improving resiliency for healthcare workers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received financial support for the analysis, authorship, and publication of this article from the Ohio Bureau of Worker’s Compensation Award: AWD-112970.