
Abstract
Introduction
In the UK, around 2,500 adolescent and young adults (AYAs; aged 15–24) are diagnosed with cancer every year (Cancer Research UK, n.d) and incidence and survival rates are increasing. Experiencing and surviving cancer can impact developing identities and cognitive processes, for example, illness understanding and metacognition (Tutelman & Heathcote, 2020). However, relatively little is known about the psychological aspects of survivorship for this developmentally distinct group.
While navigating the unique challenges associated with their cancer, AYAs are also undergoing considerable normative psychological, emotional, physical, and cognitive development (Abrams et al., 2007; Blakemore & Choudhury, 2006). Compared with children, AYAs are expected to become more autonomous (Zimmer-Gembeck & Collins, 2003) and take increasing responsibility for their own healthcare (Paone et al., 2006). Compared with adults, AYAs have significantly different psychosocial needs (e.g., experiencing higher emotional, informational, physical, and financial distress; Smrke, 2020) and different perceptions toward life (Arnett, 2001). It is, therefore, unsurprising that facing cancer as an adolescent is associated with significant distress (Sansom-Daly & Wakefield, 2013), poorer mental health, and other negative psychosocial outcomes (e.g., missing school or work; Lauer, 2015; Park & Rosenstein, 2022; Zebrack, 2011). For some, the period following treatment is associated with unfavorable psychosocial outcomes (Moss et al., 2021; Parsons et al., 2012; Tai et al., 2012), and up to 34% experience posttraumatic stress disorder (PTSD), 13% clinical depression, and 8% anxiety (Kosir et al., 2019).
“Fear of cancer recurrence” (FCR) describes a fear or worry that cancer will return or progress (Vickberg, 2003) and is common in AYA cancer survivors, affecting approximately two in three (Thewes et al., 2018). It is the primary psychological concern of young adult cancer survivors (Li & Cheng, 2021) and can negatively affect the transition from “patient” to “survivor” identity (Jones et al., 2011) or from pediatric to adult services (Granek et al., 2012). High FCR in AYAs is associated with previous illness recurrence and worse mental health (Fonseca et al., 2010; Lane et al., 2019; Sun et al., 2019), cancer type (e.g., higher in breast cancer and malignant melanoma survivors; Vandraas et al., 2020), lower health-related quality of life (Thewes et al., 2018), and increased surveillance scan anxiety (Heathcote et al., 2022). For some survivors, FCR can become chronic and disabling (Simard & Savard, 2015). It has negative effects on social relationships and quality of life (Parsons et al., 2012), is associated with higher clinical costs (e.g., increased use of health services; Lebel et al., 2013; Vachon et al., 2021), and does not decrease in severity over time in cancer survivors of ≥5 years (Koch et al., 2013).
Illness perceptions influence how people respond to illness (Petrie & Weinman, 2006) and can range from negative (e.g., I have no control over my illness) to positive (e.g., I have control over my illness). Illness perceptions are a potentially malleable treatment target known to be associated with FCR in child and adult survivor populations (Fonseca et al., 2010; Kaptein et al., 2015) but have not previously been investigated specifically with AYA cancer survivors. In adult cancer survivors, more negative illness perceptions can be associated with worse FCR, increased cancer worry, and other negative psychosocial outcomes (Freeman-Gibb et al., 2017; Kaptein et al., 2015; Phillips et al., 2013).
The Common-Sense Model (CSM) of illness self-regulation (Leventhal, 1984; Leventhal et al., 1980) provides a strong theoretical rationale for investigating FCR and illness perceptions. The CSM suggests that cognitive beliefs and emotional representations/responses to illness influence health outcomes and coping strategies (McAndrew et al., 2019). The model proposes five core dimensions of illness beliefs (influenced by past experiences etc): cause, identity, perceived control, severity of illness consequences, and timeline (e.g., perceived risk of recurrence), as well as emotional representations (e.g., the level of worry that cancer will return; Fardell et al., 2016; Lee-Jones et al., 1997; illness-related distress; Hagger & Orbell, 2003; see supplemental information for clinical example). CSM predicts that more negative cognitive representations, alongside more negative emotional representations, lead to more negative illness perceptions and increased FCR. Although seemingly important to AYA cancer survivors based on their narrative accounts (e.g., around control and emotional representations of cancer; Kameny & Bearison, 2002; and how they identify with it; Jones et al., 2011), no prior research has empirically investigated the association between illness perceptions and FCR in this developmentally distinct population.
Like FCR, illness perceptions have also been linked to mental health outcomes (e.g., negative illness perceptions to increased stress; Miceli et al., 2019; and negative illness perceptions to depression; Sansom-Daly et al., 2018; Thong et al., 2018; Wroot et al., 2020). Husson et al. (2020) found significant differences in illness perceptions of AYAs compared to older populations of thyroid cancer survivors, although regardless of age, more negative illness perceptions (particularly illness timeline) were associated with more distress.
Despite the theoretical rationale and evidence of associations between FCR, illness perceptions, and mental health in other age groups, and indications that both FCR and illness perceptions are important to AYAs, limited empirical research has examined these constructs. We aimed to bridge that gap by investigating the associations between FCR, illness perceptions, and mental health in this developmentally distinct population. We hypothesized that:
High FCR would be associated with more negative illness perceptions. High FCR and more negative illness perceptions would be associated with poorer mental health (depression and anxiety). The association between high FCR and poorer mental health (depression and anxiety) would be mediated by illness perceptions.
Method
Design and Sample
Cross-Sectional, Correlational Design
A web-based survey was administered via Qualtrics Survey Software®. Participants were a convenience sample of AYA cancer survivors, recruited over 14 months (November 2020–January 2022), and were included/excluded based on specific criteria (aged between 16 and 30, treated for cancer between 13 and 24 years, having completed active cancer treatment, and been in remission for 6+ months; see supplemental information for further details). We used the CHERRIES checklist to improve the quality of the web-based survey (Eysenbach, 2004; see supplemental information).
Measures
We gathered demographic and clinical data and used validated measures to assess the variables of interest:
Illness perceptions: Brief Illness Perception Questionnaire (BIPQ; Broadbent et al., 2006). FCR: Fear of Cancer Recurrence Inventory–Short Form (FCRI-SF; Simard & Savard, 2009). Mental health outcomes: Patient Health Questionnaire (PHQ-9; Kroenke & Spitzer, 2002) assessed depression and the Generalized Anxiety Disorder Scale (GAD-7; Spitzer et al., 2006) captured anxiety.
See supplemental information for descriptions of measure validity and rationale.
Procedure
Social media study adverts were posted on Twitter, Facebook, Instagram, and TikTok, which included a video of the researcher and a person with personal experience (PPE) of cancer discussing the research or a picture of the project poster. Adverts were also shared via several charities (e.g., Shine) and support groups (e.g., Trekstock). Those who were interested could directly follow an anonymous Qualtrics link from the advertisement or email the research team. Clicking on the link took participants to the online research platform, where they were presented with information about the study, the research team's contact details in case of questions, and a consent form. Subsequently, they filled out study measures. The study took 15 to 30 min to complete, although participants could complete this within a week (using unique IP addresses ensured participants could only participate once).
Demographic and clinical questions were presented first and ensured inclusion/exclusion criteria were met before proceeding to the remaining questionnaires. Qualtrics was set to ensure all questions were completed and participants could review and change responses before submission. Participants could opt into a prize draw to receive an online voucher (one of five £20 Amazon vouchers) and could email the researcher to ask for a summary of the research findings.
Ethical approval was gained from the University of Bath Psychology Research Ethics Committee (reference number: 20-213). The research was anonymous (with an email address recorded only if participants chose to leave it) and confidential with all information relating to research participants and their data obtained and stored in line with EU General Data Protection Regulations (2018). It was not expected that completion of the questionnaires would have any negative effects for participants. However, following responses to question 9 on the PHQ-9 (which refers to suicidal/self-harm ideation) and at study completion, participants were signposted to various mental health resources (e.g., Mind, Samaritans, and Macmillan cancer support). Throughout each stage of the research (e.g., project development, recruitment, data collection, and analysis), we consulted with PPE to discuss the research and ensure changes reflected service-user perspectives.
Statistical Analysis
The data analysis plan was preregistered on December 16, 2021 (https://osf.io/xec57/). Statistical analyses were conducted using SPSS Version 27. Descriptive statistics were performed for participant demographic information, clinical characteristics, and all outcome measures. A hierarchical multiple linear regression, with mental health as the dependent variable, and FCR and illness perceptions as the independent variables, including covariates (age and gender) then examined the proportion of the variance in mental health accounted for by FCR and illness perceptions. Gender and age were first added to the regression models, followed by FCR and finally illness perceptions. In addition to the preregistered protocol, post hoc linear regressions were completed, which included the illness perception subscales, instead of overall illness perception scores. Subscales were added to the regression models one at a time. Mediation analyses (using the PROCESS macro) finally investigated if any associations found between FCR, and depression/anxiety were mediated by illness perceptions. The final data set was retrieved from Qualtrics on January 18, 2022.
Results
Participant Characteristics
Of the 214 participants who accessed the survey, 124 did not meet inclusion criteria or were excluded for not fully completing the survey. The final sample consisted of 90 (42% completion rate) AYA cancer survivors, aged 16 to 30. The mean age was 22.42 years (SD = 2.98), most participants identified their ethnicity as from the UK (91.1%), the majority identified as single (67.8%), and the most frequent highest education achieved was A-Levels (41.1%). Additionally, participants were most frequently recruited via Instagram (53.3%; see supplemental information for more detail): 93.3% of participants showed clinical levels of FCR on the FCRI-SF, 38.9% showed moderate or severe anxiety on the GAD-7, and 35.6% showed moderate or moderately severe depression on the PHQ-9. Further descriptive statistics for illness perceptions, FCR, anxiety, depression, quality of life, and functioning impairment can be found in Table 1.
Descriptive Statistics of Key Study Variables (N = 90)
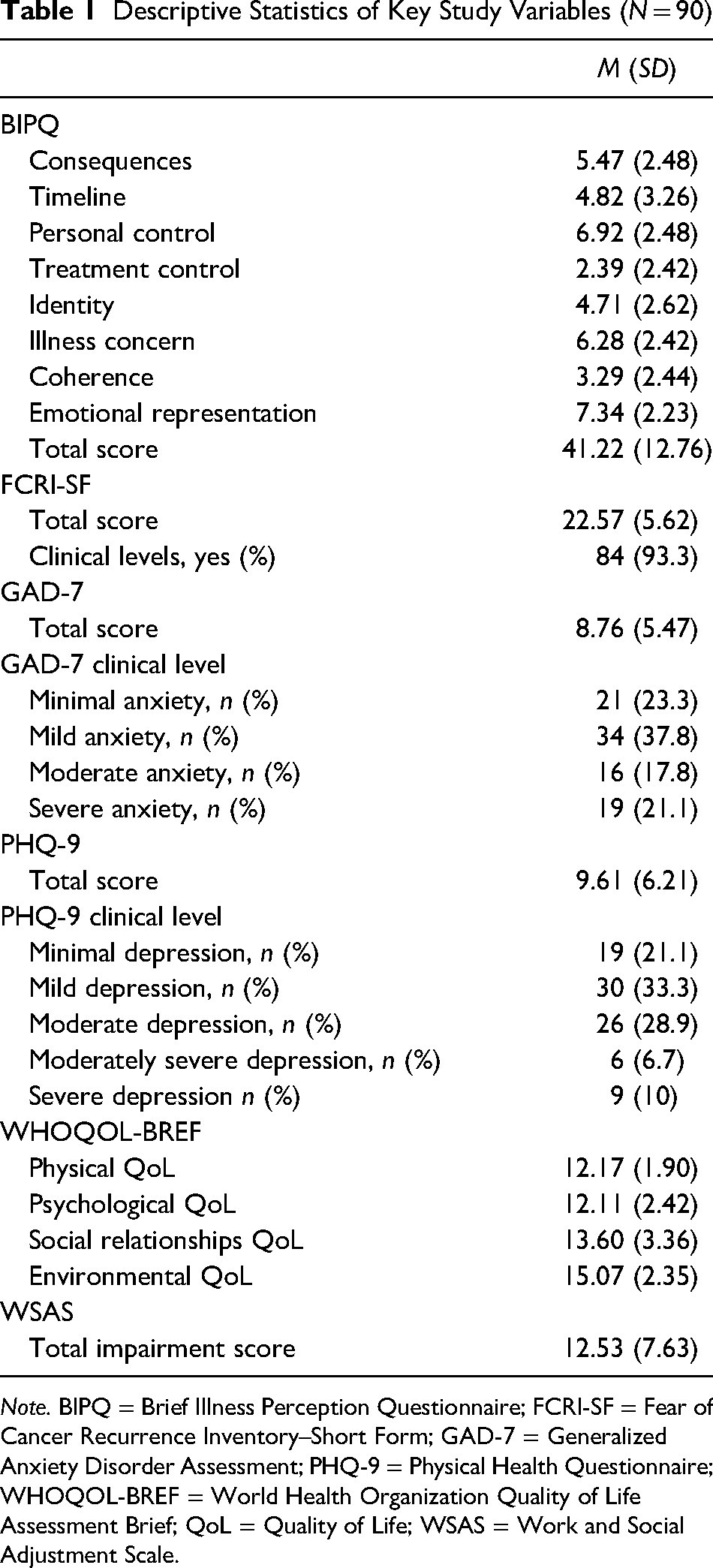
Note. BIPQ = Brief Illness Perception Questionnaire; FCRI-SF = Fear of Cancer Recurrence Inventory–Short Form; GAD-7 = Generalized Anxiety Disorder Assessment; PHQ-9 = Physical Health Questionnaire; WHOQOL-BREF = World Health Organization Quality of Life Assessment Brief; QoL = Quality of Life; WSAS = Work and Social Adjustment Scale.
Clinical Characteristics
Most participants had experienced either lymphoma (46.7%) or leukemia (20%). The most common stage of cancer at diagnosis was stage 2 (35.6%), with most participants having received chemotherapy as treatment (93%). Time from diagnosis to remission was most commonly ≤2 years (86.7%), while time in remission at study participation was variable (e.g., >1 year = 21.1%; 1–2 years = 20%; 2–3 years = 16.7%). See supplemental information for more detail.
Question 1: What Are the Associations Between FCR, Illness Perception, and Mental Health?
Correlation analysis
Tests for normality of distribution were conducted, which indicated that the data was not normally distributed. Therefore, Spearman's correlations were performed to analyze the associations between the study's target variables. Significant associations were seen between all the target variables. Specifically, high FCR is associated with more negative overall illness perceptions (r ≥ .6), with the specific perceptions of consequences, illness concern, and emotional representation being particularly strongly associated with high FCR (r ≥ .5). Both a high FCR and more negative illness perceptions were also associated with poorer mental health on the GAD-7 and PHQ-9 (r ≥ .4; Table 2).
Regression analysis
Hierarchical multiple regression analyses were conducted to investigate the potential interaction of illness perceptions on the FCR–mental health association. The data were checked and met the eight assumptions needed for completing a multiple hierarchical linear regression (see supplemental information).
Spearman's Correlation Analysis
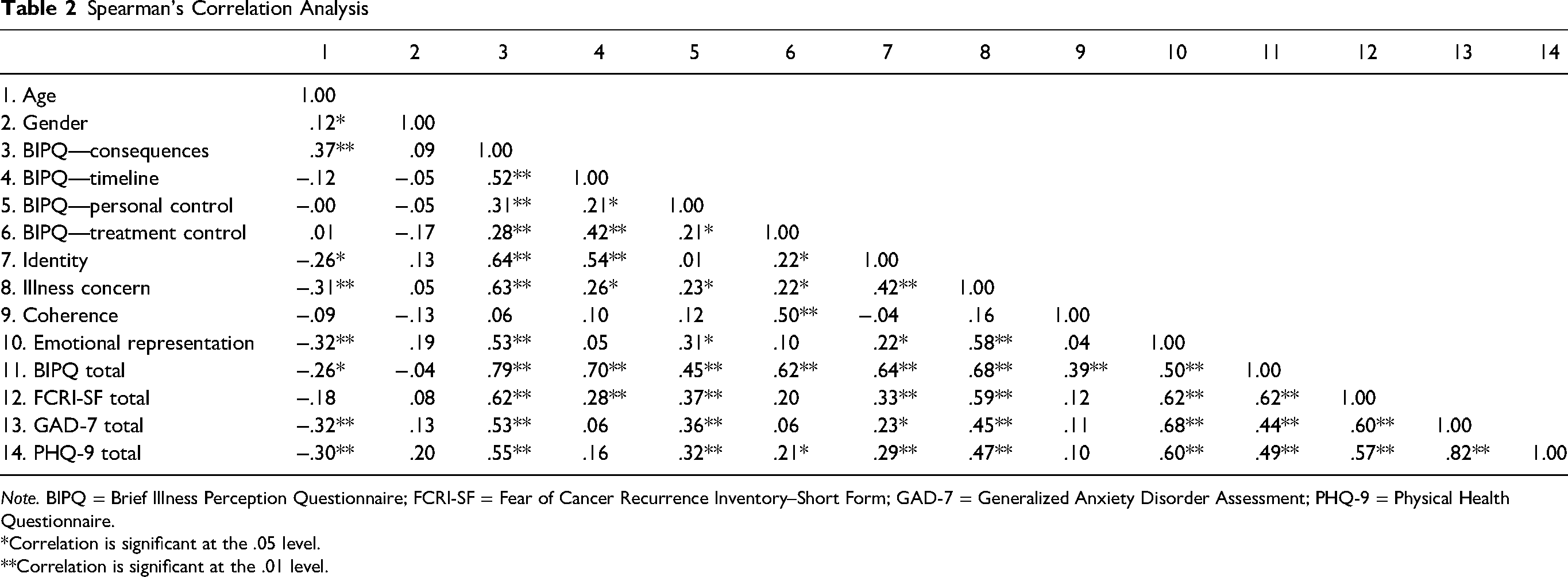
Note. BIPQ = Brief Illness Perception Questionnaire; FCRI-SF = Fear of Cancer Recurrence Inventory–Short Form; GAD-7 = Generalized Anxiety Disorder Assessment; PHQ-9 = Physical Health Questionnaire.
*Correlation is significant at the .05 level.
**Correlation is significant at the .01 level.
Anxiety
The first set of regression models explored the potential interaction of overall illness perceptions on FCR–Anxiety (GAD-7). Model 2, which included total FCR score, age, and gender, explained 41.1% of the variance in total GAD-7 scores. However, adding overall illness perception scores did not significantly increase the amount of variance explained (Model 3; Table 3).
Hierarchical Linear Regression for Anxiety, Including Age, Gender, FCR Scores, and Total Illness Perception Scores
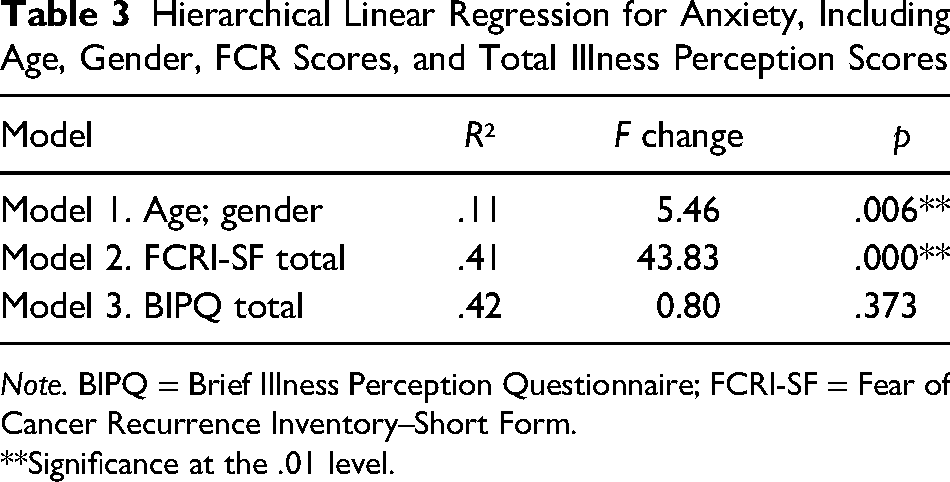
Note. BIPQ = Brief Illness Perception Questionnaire; FCRI-SF = Fear of Cancer Recurrence Inventory–Short Form.
**Significance at the .01 level.
Model 3 (which included overall illness perception scores, total FCR scores, age, and gender) was a significant predictor of anxiety scores, F(4, 85) = 15.20, p = .000. Within this, FCR (β = 0.49, p = .000) and age (β = −0.32, p = .045) showed a significant main effect, with gender (β = 1.18, p = .246) and BIPQ total not showing significance (β = 0.04, p = .373). This indicates that FCR predicted anxiety scores above and beyond gender and overall illness perceptions.
Despite the total illness perception score not being a significant predictor of the anxiety and FCR association, the correlational analysis showed associations between the illness perception subscales and both anxiety scores and FCR scores. A post hoc regression was therefore completed to investigate if any of the specific illness perception sub-scales explained any variance in the FCR–anxiety relationship. Model 9 (which included the eight individual BIPQ subscales scores, total FCRI scores, age, and gender) was significant and explained 57.1% of the variance in total GAD-7 scores (Table 4).
Hierarchical Linear Regression for Anxiety, Including Age, Gender, FCR Scores, and Individual Illness Perception Subscale Scores
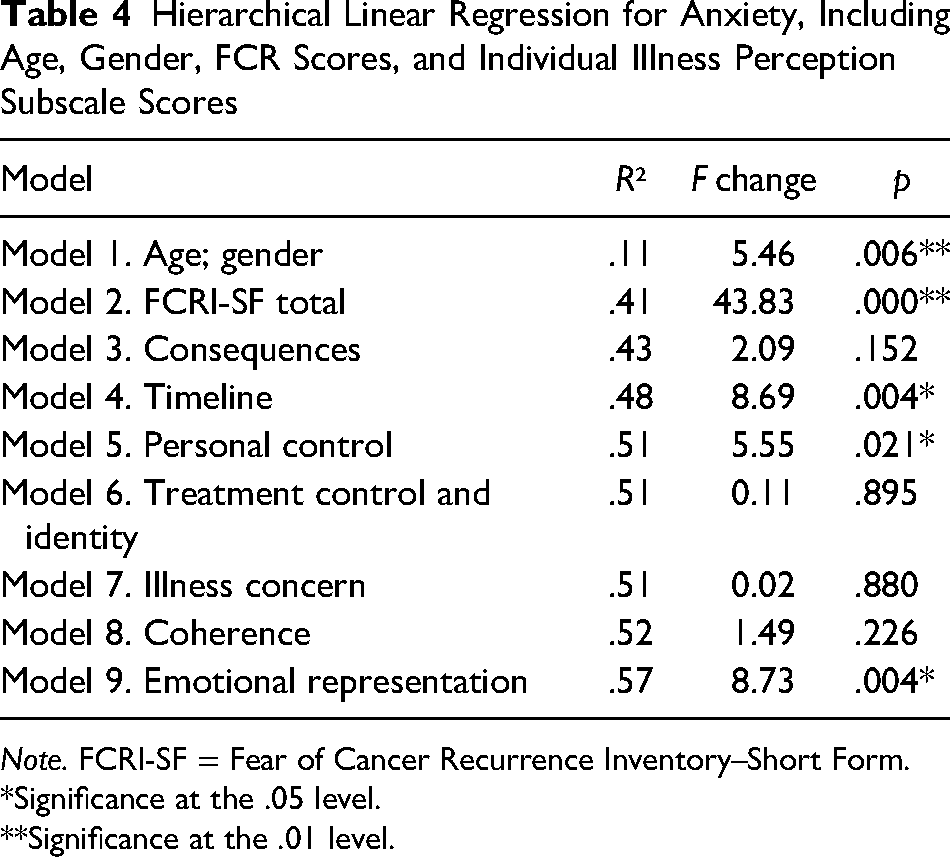
Note. FCRI-SF = Fear of Cancer Recurrence Inventory–Short Form.
*Significance at the .05 level.
**Significance at the .01 level.
Model 9 (which included the eight individual BIPQ subscales scores, total FCRI scores, age, and gender) was a significant predictor of anxiety scores, F(11, 78) = 9.42, p ≤ .000. Within this, FCR had a significant main effect (β = 0.28, p = .008), as did the illness perceptions of timeline (β = −0.39, p = .023), personal control (β = 0.41, p = .040), and emotional representation (β = 0.80, p = .004). This indicates that these three specific illness perceptions predicted the relationship between FCR–anxiety.
Depression
The second regression model explored the potential interaction of illness perceptions on the FCR–depression (PHQ-9) link. Model 3 (which included total FCR scores, overall illness perception scores, age, and gender) was significant and explained 41.9% of the variance in total PHQ-9 scores (Table 5).
Hierarchical Linear Regression for Depression, Including Age, Gender, FCR Scores, and Total Illness Perception Scores
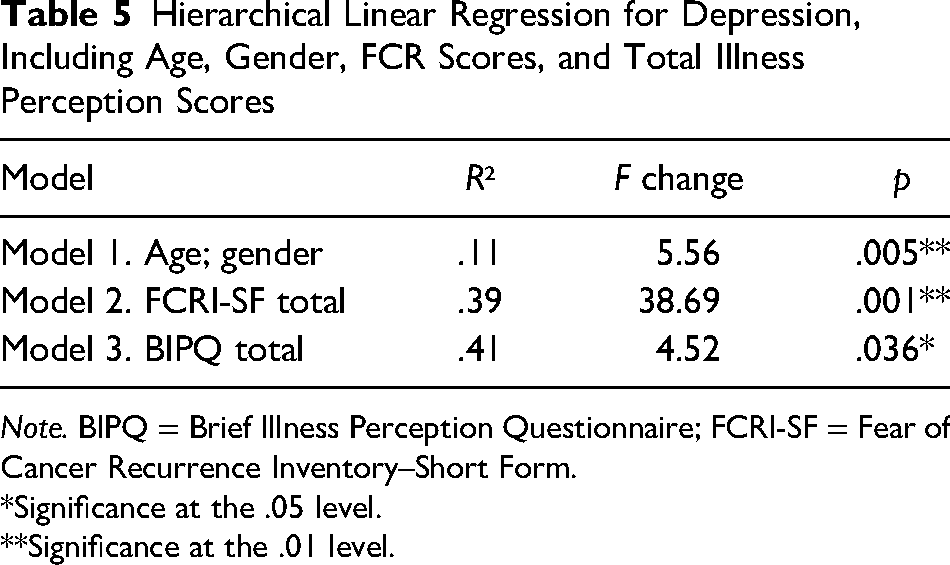
Note. BIPQ = Brief Illness Perception Questionnaire; FCRI-SF = Fear of Cancer Recurrence Inventory–Short Form.
*Significance at the .05 level.
**Significance at the .01 level.
Model 3 (which included total FCR scores, total BIPQ scores, age, and gender) was a significant predictor of depression scores, F(4, 85) = 15.34, p = .036. Within this, FCR (β = 0.45, p = .000), BIPQ total (β = 0.11, p = .036), and gender (β = 2.35, p = .044) showed a significant main effect, with age (β = −0.25, p = .173) not showing significance. This indicates that both overall illness perceptions and gender predicted the relationship between FCR–depression.
A post hoc regression was completed to investigate whether any specific illness perceptions were significant predictors of FCR–depression. Model 3 (which included total FCR scores, the consequence illness perception subscale, age, and gender) significantly explained 42.3% of the variance in total PHQ-9 scores. However, individually adding the other seven illness perception subscales did not significantly increase the amount of variance explained (Model 9; Table 6).
Hierarchical Linear Regression for Depression, Including Age, Gender, FCR Scores, and Individual Illness Perception Subscale Scores
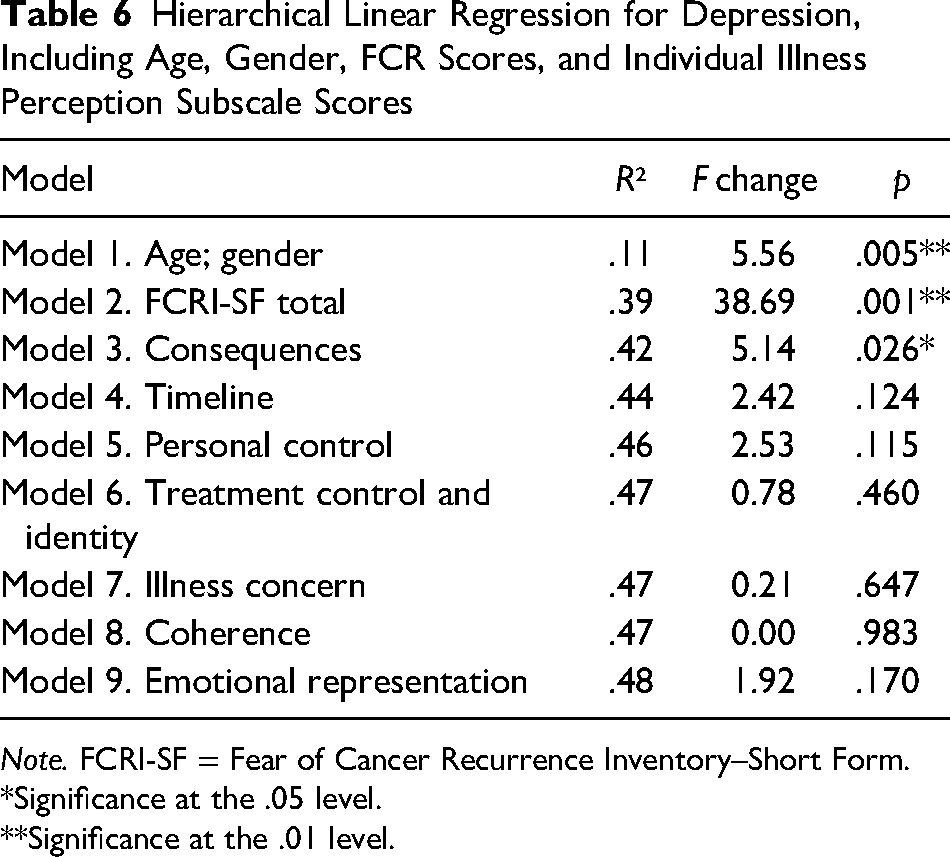
Note. FCRI-SF = Fear of Cancer Recurrence Inventory–Short Form.
*Significance at the .05 level.
**Significance at the .01 level.
Model 9 (which included the eight individual BIPQ subscales scores, total FCRI scores, age, and gender) was a significant predictor of depression scores, F(11, 78) = 6.56, p = .000. However, within this, only FCR had a significant main effect (β = 0.31, p = .021), with no significant effects for gender, age, or any of the BIPQ subscales. Thus, indicating that none of the specific illness perception domains, predicted the relationship between FCR–depression.
Question 2: Do Illness Perceptions Mediate the Association Between High FCR and Poorer Mental Health?
Anxiety
A mediation analysis was completed to investigate whether there was an indirect effect of illness perception scores, within the total effect seen between FCRI scores and GAD-7 scores (Figure 1).
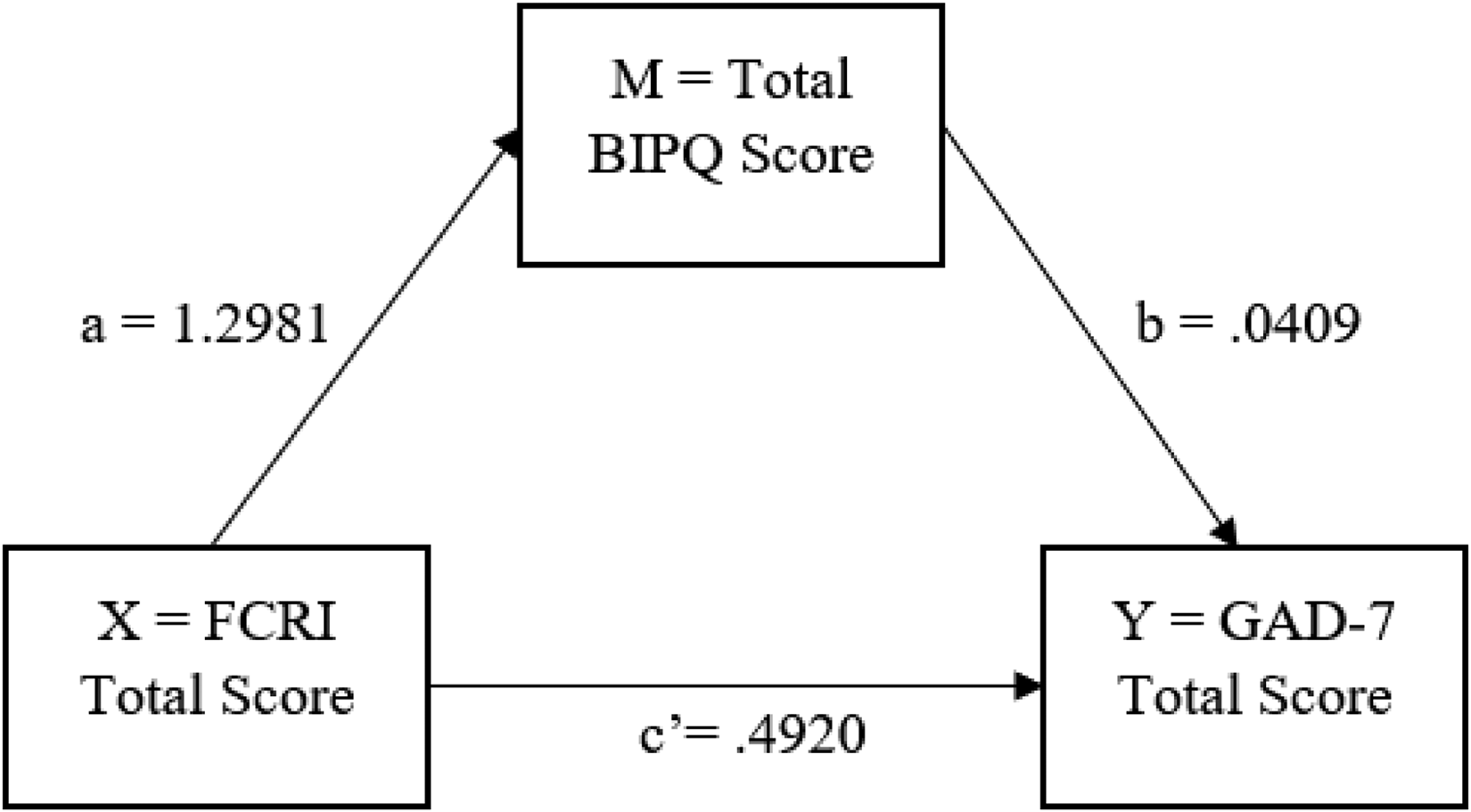
Illness Perceptions Mediation Model of FCR–anxiety. Note. The direct association between FCRI and GAD-7 scores is indicated by c′. The indirect association of FCRI and GAD-7 scores via BIPQ scores is indicated by the combination of a and b. This indirect association was not significant indicating that BIPQ scores do not mediate the relationship between FCRI and GAD-7 scores. BIPQ = Brief Illness Perception Questionnaire; FCRI = Fear of Cancer Recurrence Inventory; GAD-7 = Generalized Anxiety Disorder Scale.
The indirect effect of illness perceptions on the FCR–anxiety interaction was not significant, due to the bootstrap confidence intervals including 0 (effect = .05, 95% CI [−0.07, 0.19]). Illness perceptions, therefore, do not significantly mediate the total effect (β = 0.55) seen between FCRI total scores and GAD-7 total scores.
Depression
A mediation analysis was completed to investigate whether there was an indirect effect of illness perception scores, within the total effect seen between FCRI scores and PHQ-9 scores (Figure 2).
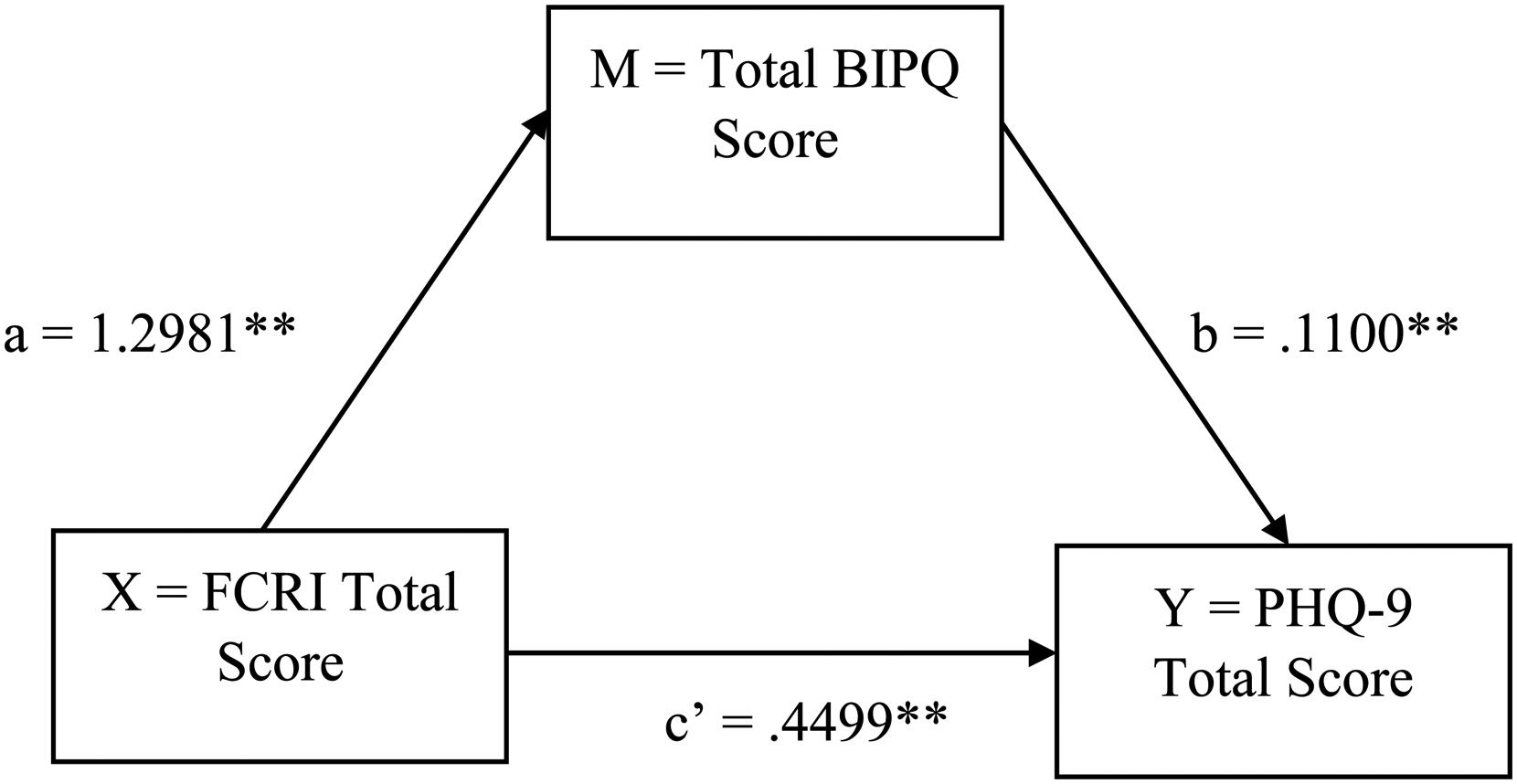
Illness Perceptions Mediation Model of FCR–depression. Note. The direct association between FCRI and PHQ-9 scores is indicated by c′. The indirect association of FCRI and PHQ-9 scores via BIPQ scores is indicated by the combination of a and b. This indirect association was significant at a p ≤ .01 level as indicated by **. This indicates that BIPQ scores mediate the relationship between FCRI and PHQ-9 scores. BIPQ = Brief Illness Perception Questionnaire; FCRI = Fear of Cancer Recurrence Inventory; PHQ-9 = Physical Health Questionnaire.
The indirect effect of illness perceptions on the FCR–depression interaction was significant, due to the bootstrap confidence intervals not including 0 (effect = .14, 95% CI [0.02, 0.28]). Illness perceptions therefore significantly mediate the total effect (β = 0.59) seen between FCRI total scores and PHQ-9 total scores. Specifically, FCRI scores account for 75.9% of PHQ-9 scores in AYA cancer survivors, but 24.1% is accounted for through the illness perceptions of these AYAs.
Discussion
In AYA cancer survivors, we found that more negative illness perceptions were associated with higher FCR and more severe anxiety and depression. Specifically, illness concern, consequences, and personal control were most strongly associated with all outcome variables. High FCR was predictive of worse mental health outcomes; total illness perceptions predicted and mediated the relationship between FCR and depression. Contrastingly, total illness perceptions did not predict the relationship between FCR–anxiety, but the specific illness perceptions of timeline, personal control, and emotional representation did.
Our novel finding that high FCR was associated with more negative illness perceptions in AYA cancer survivors (hypothesis 1 supported) fits with similar findings in adult populations (e.g., Kaptein et al., 2015; Phillips et al., 2013). This is perhaps unsurprising given the shared theoretical underpinning of CSM for both illness perceptions and FCR. We found significant positive correlations between individual illness perceptions and FCR scores, suggesting that the cognitive representations underpinning FCR (e.g., around cancer timeline or perceived control) might conceptually overlap with those underpinning illness perceptions (e.g., around illness timeline or personal control).
Expanding on the existing evidence (Sun et al., 2019; Thong et al., 2018; Wroot et al., 2020), we found that both illness perceptions and RCT are important contributory factors in the mental health of AYA cancer survivors (second and third hypotheses supported). This is particularly important considering the increased vulnerability AYAs have for mental health difficulties following cancer treatment (Kosir et al., 2019; Moss et al., 2021), at a time when they are also undergoing distinct psychoemotional changes (Abrams et al., 2007; Blakemore & Choudhury, 2006). It is unsurprising that anxiety was associated with FCR, given that FCR is fear or worry that cancer will return (Vickberg, 2003), while general anxiety is defined as the experience of persistent, excessive, and unfocused worry and anxiety (NICE, 2011; Tyrer and Baldwin, 2006). However, FCR and anxiety need exploring further to understand how these constructs interact: Do AYAs who are anxious fear most things, including cancer recurrence? Or is the experience of anxiety related to FCR different and so needs specific understanding and informed care?
While overall illness perceptions did not predict the relationship between FCR–anxiety, the individual illness perceptions of timeline, personal control, and emotional representation, were shown to be predictive (more negative perceptions predicting a more negative interaction). The CSM suggests that someone's cognitive and emotional representations of their illness precede and influence their physical and emotional coping responses (McAndrew et al., 2019). It is therefore possible that these individual cognitive and emotional illness perceptions (i.e., thinking you have no control; thinking that cancer will last for longer; experiencing a greater emotional impact due to having cancer), maybe more directly associated with the emotional response of experiencing anxiety and uncertainty. However, while these individual perceptions may play a predictive role and could be used to predict AYA FCR–anxiety levels, overall illness perceptions did not significantly mediate the total effect seen between FCR and anxiety. This suggests that while a potential clinical marker, targeting overall illness perceptions may not reduce FCR and anxiety, and these may need more direct targeting, through evidence-based approaches, such as cognitive-behavioral therapy (CBT; NICE, 2014).
Contrastingly, we found that more negative overall illness perceptions were predictive of the association between high FCR–depression, mediating the relationship seen between FCR and depression, and accounting for 24.1% of the variance. It may be that more negative illness perceptions associate directly with factors associated with depression. For example, more negative cognitive and emotional perceptions may contribute to a negative thinking bias or a feeling of hopelessness—common symptoms and perpetuating factors of depression (Beck, 1979). The CSM would suggest that more negative illness perceptions and higher FCR (both underpinned by negative cognitive and emotional representations of cancer), influence depressive thinking styles and feelings to predict depression (i.e., they influence worse emotional coping responses). However, the reverse interaction could be true—a negative thinking bias could influence the development of more negative illness perceptions, or the interaction might be bidirectional. Overall illness perceptions might be important in the association between FCR and depression, acting as a potentially modifiable treatment target, reducing FCR, and improving depression. However, further longitudinal research is needed to develop a causal understanding.
Strengths and Limitations
A preregistered data analysis plan increased replicability of findings and prevented ad hoc decisions, minimizing risk of bias or false positives (Moore, 2016). Important covariates (gender and age) were controlled for, decided a priori, to further minimize risk of bias. The potential conceptual overlap of worry/fear was considered across all three constructs of anxiety, FCR, and emotional representations (within illness perceptions), and tests were conducted for multicollinearity to increase reliability of analyses. The data did not show multicollinearity, suggesting distinct functions in each construct. However, future research might explore the conceptual similarities and differences of these constructs. The use of the CHERRIES checklist (Eysenbach, 2004) additionally improved the quality of the web-based survey.
The cross-sectional nature of the research makes causality and direction of relationships difficult to establish (Fiedler et al., 2011). While illness perceptions were found to mediate the relationship between FCR–depression, which variable precedes another is unclear (e.g., negative illness perceptions preceding FCR). Mediation analysis did allow inferences to be made about potential dual roles of illness perceptions, as both a potential cause and effect of high FCR and lower mood. The lack of prior research on how illness perceptions, FCR, and mental health interact in TYA cancer survivors means this initial investigation provides useful information to inform future longitudinal research.
An online UK-wide survey was used as a convenient and cost-effective way of reaching young populations from a broad range of regions—intended to increase generalizability. However, online surveys are at greater risk of self-selection bias (Bethlehem, 2010), and our sample predominantly identified as British (91.1%)—somewhat higher than the national figure, according to Census Data (2011). Recruiting only in the UK meant a Western, educated, industrialized, rich, and democratic cultural sample (WEIRD; Henrich et al., 2010). As such, if illness perceptions are culturally and contextually specific, we cannot necessarily generalize to other cultures.
Implications for Research and Clinical Practice
Our findings suggest that interventions targeted at improving illness perceptions may be a way to target both FCR and depression in AYAs, in line with previous literature in other populations (e.g., diabetes; Keogh et al., 2007; myocardial infarction; Petrie et al., 2002). Discovering effective and efficacious ways of improving illness perceptions, while also improving FCR levels and mental health for young people with cancer, would be clinically important and time and cost-effective.
Our findings highlight the importance of all health professionals holding FCR and illness perceptions in mind when working with AYA cancer survivors. Illness perceptions and FCR can help clinicians understand and formulate AYAs’ experiences of anxiety and depressive symptomatology. For young people who are anxious, the illness perceptions around cancer timeline, personal control, and emotional representation might be prioritized. For young people who are depressed, it may be helpful to explore overall illness perceptions. Clinicians routinely measuring FCR (using the FCRI-SF) and illness perceptions (using the BIPQ), could aid in assessment, formulation, and intervention related to illness perceptions, FCR, and mental health. For example, nursing staff could use measures to discuss with AYA cancer survivors how they perceive their cancer and the impact it is having on their mood. This initial exploration could inform appropriate stepped-care interventions—from basic psychoeducation and support to signposting/referral for targeted additional support (e.g., psychology). It appears to be important that high FCR and poor mental health be taken into account when planning service delivery. For example, in considering that when AYAs enter remission, the frequency of clinical contact significantly reduces, minimizing their access to support with these ongoing challenges.
Future longitudinal research should explore the direction of the associations between FCR and illness perceptions and their effect on mental health. Building an understanding of the processes of influence will help inform both where and when clinical intervention should be targeted.
Longitudinal research could explore and further conceptualize FCR and its relationship to mental health outcomes. A low level of anxiety around recurrence might help AYAs make helpful health-related decisions (e.g., attend check-ups). However, questions remain as to whether there is a point at which FCR transitions from adaptive to maladaptive, when it begins to predict poor mental or physical health outcomes. Understanding these processes could inform future clinical practice as to when additional support is helpful.
Conclusion
The findings indicate that illness perceptions and FCR are significantly associated, and both predict mental health outcomes. Overall illness perceptions predict depression, while the specific illness perceptions of timeline, personal control, and emotional representation predict anxiety. Additionally, overall illness perceptions mediate the relationship between FCR and depression, but do not mediate the relationship between FCR and anxiety. This suggests that FCR and illness perceptions are important in the experience of AYA cancer survivors, could help explain vulnerability to mental health difficulties, and should be considered within clinical interventions and services. Further longitudinal and cross-cultural research into these relationships could improve our understanding and inform future clinical practice, policy, and guidelines.
Supplemental Material
sj-docx-1-jpo-10.1177_27527530231190378 - Supplemental material for Illness Perceptions, Fear of Cancer Recurrence, and Mental Health in Teenage and Young Adult Cancer Survivors
Supplemental material, sj-docx-1-jpo-10.1177_27527530231190378 for Illness Perceptions, Fear of Cancer Recurrence, and Mental Health in Teenage and Young Adult Cancer Survivors by Michael Horwood, Maria Elizabeth Loades, Urska Kosir and Cara Davis in Journal of Pediatric Hematology/Oncology Nursing
Footnotes
Acknowledgments
The views expressed in this publication are those of the authors and not necessarily those of the NIHR, NHS, or the UK Department of Health and Social Care. I would like to thank all people with personal experience of cancer who inputted to the development of and supported in the recruitment for this research. Similarly, I would like to thank all the charities and organizations which supported the recruitment of this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Authors disclose the following financial support: National Institute for Health Research (NIHR Doctoral Research Fellowship, DRF-2016-09-021; Development and Skills Enhancement Award, 302367).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.