
Abstract
Introduction
Parents of children with cancer need a diverse and complex range of knowledge and skills. In the beginning, parents are in an unfamiliar and frightening situation and need to support their children in new ways. They have to monitor the children, observe them, ask healthcare professionals (HCPs) questions, and handle and search for information needed to manage their children's care (Carlsson et al., 2019). The consequences of childhood cancer on parental stress, anxiety, and depression are well-described in a multitude of studies (van Warmerdam et al., 2019). Further, when parents of ill children report low knowledge about their child's disease, they also experience higher levels of distress (Hames et al., 2021; Kelada et al., 2021; Othman et al., 2011) and higher levels of psychosomatic symptoms (Sloper, 1996).
Alleviating the strain on parents of children with cancer is thus a key task in pediatric oncology nursing. This paper reports initial findings from an intervention aiming at reducing parental stress through person-centered information.
Conveying information to parents should be a natural and integrated part of a child's cancer treatment. However, parents describe obtaining information as difficult, and the frustration they experience from their unmet informational needs only worsens as the treatment progresses (Lövgren et al., 2020; Ringnér et al., 2011a; Rodgers, Stegenga et al., 2016). HCPs report giving parents most of the necessary information at the time of diagnosis, but parents often are unable at that time to process such information while coming to terms with their child's illness. Furthermore, because the child's health can change swiftly, the information provided to their parents also needs to change constantly. Highly stressed parents thus often need repeated and updated information and will have new questions that need to be answered along the treatment trajectory (Baenziger et al., 2020). There are North American clinical recommendations concerning content (Haugen et al., 2016; Rodgers et al., 2018) and process (Rodgers, Laing et al., 2016) for information delivery. As for content, two Delphi studies have presented ranked lists of topics suggested for initial education, either according to a suitable point in time (Rodgers et al., 2018) or by diagnosis cluster (Haugen et al., 2016). As for the process, parents should be provided with information when they have had time to process the diagnosis. The information could be given in verbal discussions and written form, while allowing time to answer questions. Preferably the same HCP should meet with the parents. Over time, the content focus should shift from checklist-based essential topics at diagnosis to topics driven by the families’ specific information needs in a later stage of treatment (Landier et al., 2016; Rodgers, Laing et al., 2016).
Most studies on interventions aimed to decrease parental distress focus on psychoeducational methods for psychological coping (Hyewon et al., 2020; Koumarianou et al., 2020; Ogez et al., 2019; Sánchez-Egea et al., 2019). Fewer studies (e.g., De la Maza et al., 2020), however, focus on the core nursing intervention of providing information to parents and supporting them in managing the child's disease practically, emotionally, and socially.
The Person-centered Information to Parents in Pediatric Oncology study (PIFBO, acronym for Swedish Personcentrerad information till föräldrar inom barnonkologin) used a person-centered information approach, recognizing each parent's individual needs and preferences for information. Parents’ information needs differ from the ones of the child, and parents of the same child may also have different individual information needs (Zwaanswijk et al., 2010). A person-centered approach encourages parents to tell their own stories, provides information tailored to their unique needs, and involves them in a caring partnership with HCPs. This has been shown to improve people's satisfaction with care (Morgan & Yoder, 2012). In this paper, we conceptualize person-centered information as information about social, emotional, existential, and medical topics related to ill health and disease that is grounded in the person's present knowledge, preferences, and needs and that seeks to empower parents to participate in the care of their sick child (Ringnér, Björk et al., 2015).
To provide person-centered information to parents, we used the representational approach to patient education developed by Donovan and coworkers (Donovan & Ward, 2001; Donovan et al., 2007). This approach is based on two theories. First, the common-sense model of illness representations (Diefenbach & Leventhal, 1996) guided the nurses in assessing parents’ preexisting understandings. These assessments became the basis for planning individual education for each parent, informed by the second theory of conceptual change (Posner et al., 1982), which emphasizes the consequences of existing knowledge gaps or confusion before the education. The approach consists of five key elements: (a) representational assessment, (b) exploring misconceptions, (c) creating conditions for conceptual change, (d) introducing replacement information, and (e) making a summary (Donovan & Ward, 2001; Donovan et al., 2007). The representational approach has been used successfully with both patients and family members in areas such as cancer symptom management, brain tumors, and cardiac rehabilitation (Arida et al., 2016). The intervention was also pilot tested on eight parents of children with cancer ahead of this randomized controlled trial (RCT) study (Ringnér, Karlsson, et al., 2015). In that study, parents were satisfied with the intervention and the nurses perceived it as doable. However, we found no measurable effect on their perceived stress.
The aim of this paper is to report a multicenter RCT of person-centered information for parents of children with cancer. Our research questions were:
To what extent were each of the key elements in the representational approach used by the intervention nurses (INs)? What were the INs’ perceptions of the intervention method? What overall topics were raised by parents in the intervention? What was the parents’ perception of the HCPs in general and with the INs? What effects did person-centered information have on illness-related parenting stress, posttraumatic symptoms, depression, anxiety, received knowledge, and satisfaction with information?
Methods
The study was a multicenter RCT with two parallel arms and a 1:1 allocation ratio. The intervention arm received the intervention plus standard care, and the control arm received standard care only according to local routines at each ward. The Consolidated Standards of Reporting Trials (CONSORT) checklist for RCT studies was used (Figure 1; Schulz et al., 2010).
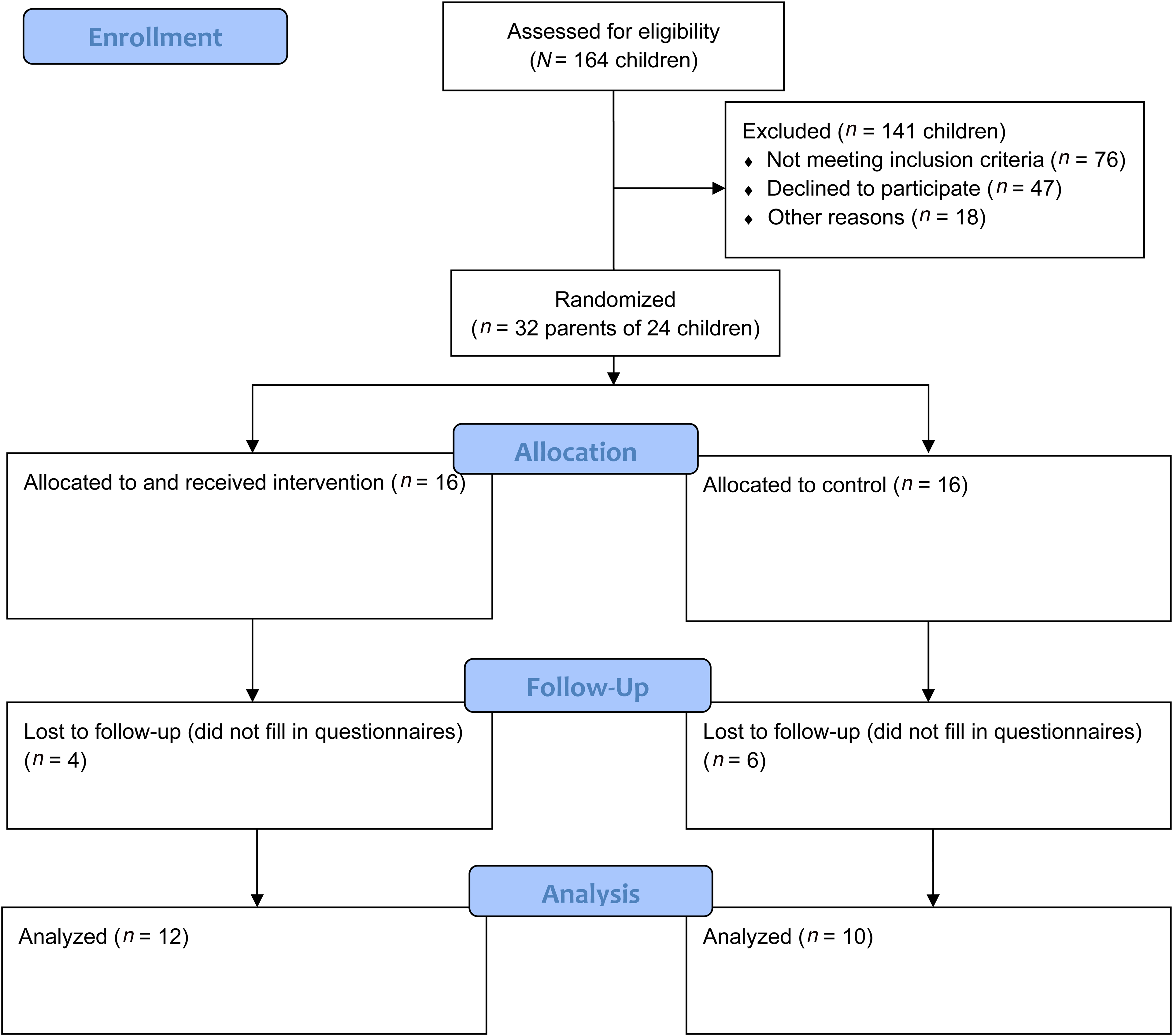
Consolidated Standards of Reporting Trials (CONSORT) flow diagram.
Participants
We recruited participants from two tertiary children's cancer centers in Sweden where children received their diagnoses and all major treatments. For distant patients, the centers cooperated with local hospitals to provide minor chemotherapy treatments and supportive care.
Eligible parents had a child diagnosed within the past two months with a first-time, curatively treated, malignancy and were able to participate without an interpreter.
A recruitment nurse at each site screened families for eligibility and provided information about the study in a two-step process beginning on the family level. First, if a child was excluded or both parents failed the inclusion criteria or declined to participate, no further data were recorded for that family. Next, parents agreeing to participate submitted their written informed consent and were given a baseline questionnaire. After baseline measurements, parents were randomized by a clerk not otherwise involved in the project, located at the department of nursing. Allocation sequences were obtained through www.randomization.com and sealed in opaque prenumbered envelopes. To avoid within-couple contamination, parents of the same child were randomized to the same arm. Randomization was performed in four strata, with the first division between the two sites and the next grouping of participants at each site by whether one or two parents per family participated. This grouping was aimed to balance the number of parents equally between sites and arms. All strata were randomized into blocks of two, four, or six units, blinded to the researchers and the clerk.
Intervention
The intervention was delivered by two pediatric nurses working part-time on the project at each site. All four had master's level specialist training in pediatric nursing and were experienced pediatric oncology nurses. As an introduction to the intervention, the nurses participated in a three-day workshop with both theoretical and practical training, including practicing the representational approach through role play.
The intervention started two months after diagnosis as previous studies indicated that by that time both parents and HCPs felt the intense stage of information-giving at diagnosis had passed (Björk, 2008; Ringnér et al., 2011a, 2011b). Each parent in the intervention arm met with the IN four times, at approximately 8, 11, 14, and 22 weeks postdiagnosis (Figure 2). Before each meeting, the parents were asked to choose a topic for which they required more information.
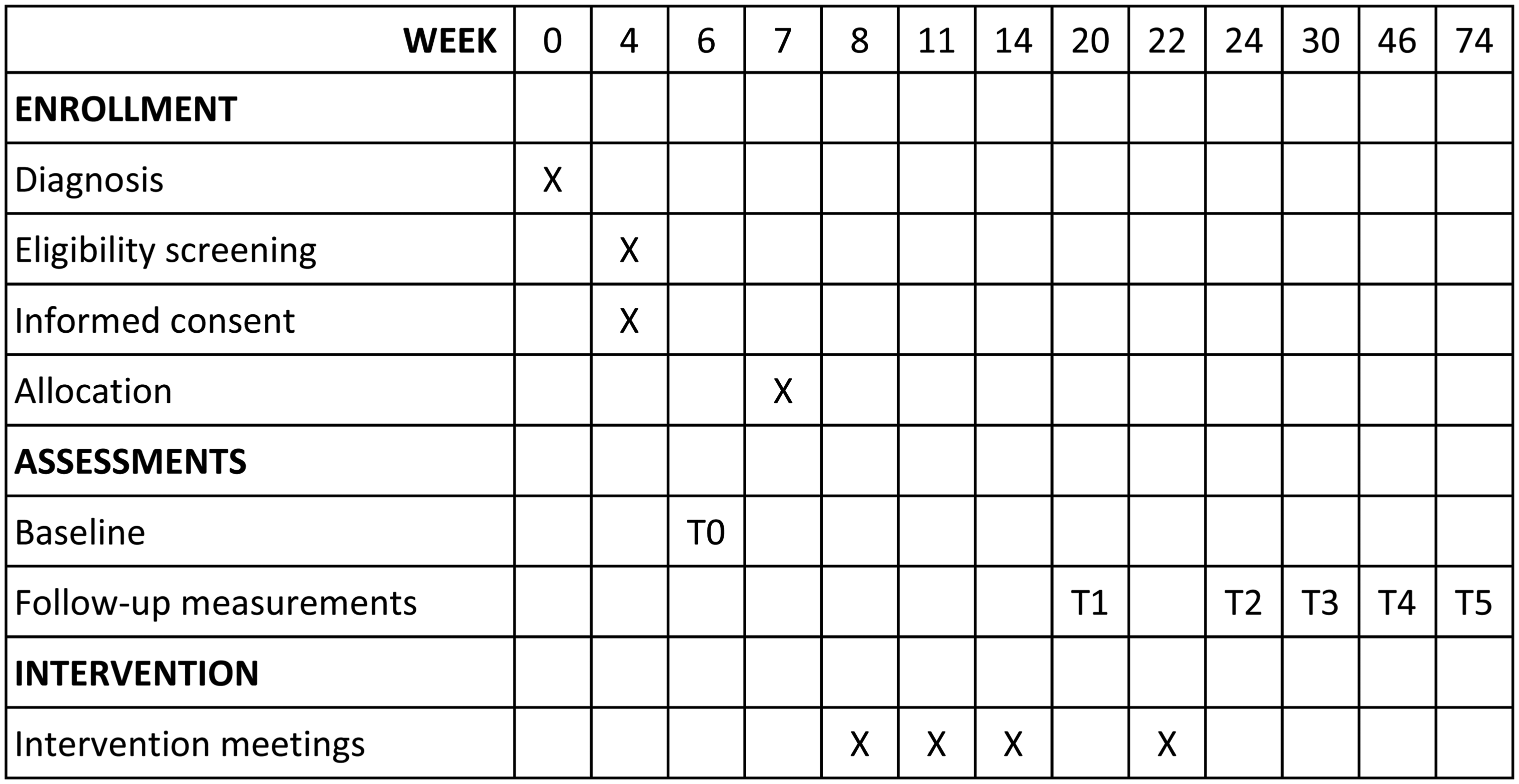
Flowchart of the study design.
The intervention meetings were conducted face-to-face or over the telephone. After identifying the topic for the meeting the IN guided the conversation using the five key elements in the representational approach (Donovan & Ward, 2001; Donovan et al., 2007). (a) The IN started with a representational assessment of the parent's current knowledge of the topic. This was done by asking questions according to the dimensions of the illness representation model (Diefenbach & Leventhal, 1996), that is, identity, cause, timeline, consequences, cure/control, and emotions. (b) Next, the IN explored possible misconceptions such as gaps, confusions, and/or misunderstandings in the parent's representations of the topic. This thorough assessment then helped the nurse to tailor the information given to the parent. (c) To create conditions for conceptual change of the representations, the consequences of knowledge gaps or misunderstandings were discussed with the parent (Posner et al., 1982). (d) Then, new information was introduced. (e) Finally, the IN summed up and discussed the benefits of the new information together with the parent. These key elements of the intervention were not necessarily performed stepwise, but rather as a process of flux between the elements (Donovan & Ward, 2001; Donovan et al., 2007).
Measures
The linking between intervention components and the measures in the study is visualized in Figure 3. The instruments will now be detailed below.
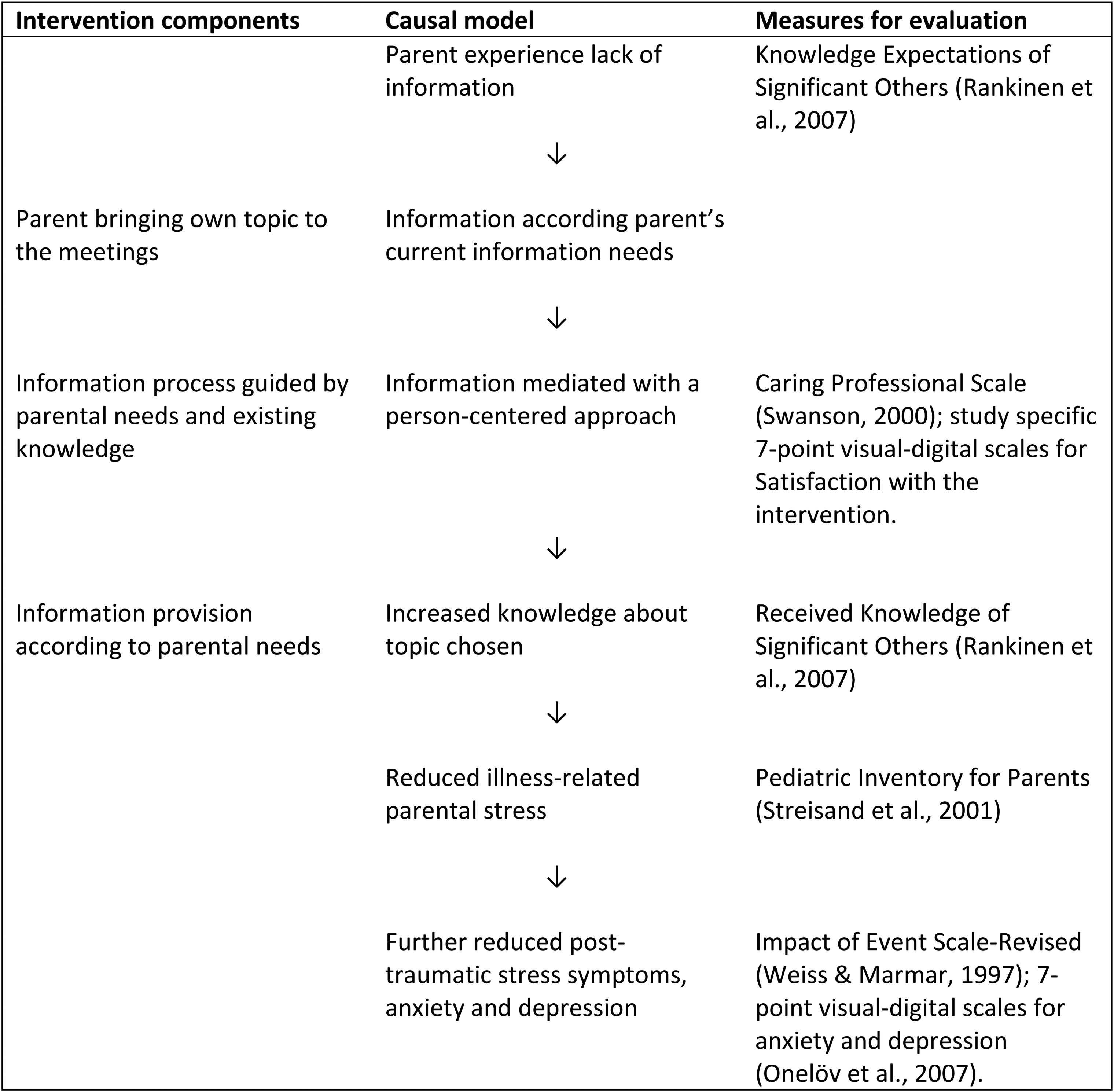
Mapping of intervention components and measures.
Expected and Received Knowledge
Knowledge Expectations of Significant Others (KEso) and Received Knowledge of Significant Others (RKso) (Rankinen et al., 2007) are paired instruments, measuring expected and received knowledge, respectively, in six dimensions: biophysiological, functional, experiential, ethical, social, and financial. Each of the 40 items is scored on a 4-point Likert-type scale. Low scores indicate high expectations for, or satisfaction with, knowledge. Cronbach's α was .82 for KEso and .98 for RKso in this sample.
Experiences With Healthcare Providers
These were measured using the Caring Professional Scale (CPS). This instrument has 15 items and was developed from Swanson's theory of caring (Swanson, 2000). Low scores indicate high caring behavior from the healthcare provider. For the intervention arm, this instrument was used also to assess parents’ experience of the IN. In this study, Cronbach's α was .97.
Satisfaction With Information
Two study-specific 7-point visual digital scales (VDS) assessed satisfaction with information in general about the child's illness, and satisfaction with information from the intervention (1 = very dissatisfied to 7 = very satisfied for both).
Illness-Related Parental Stress
The Pediatric Inventory for Parents (PIP) (Streisand et al., 2001) was the primary outcome of this study and has been used extensively in different pediatric settings. The instrument has been translated into Swedish (Olsson et al., 2018) and measures the frequency and difficulty of 42 items in four domains of stress: communication, emotional functioning, medical care, and role functioning. Typical items are “watching my child having trouble eating,” “feeling numb inside,” and “speaking to my child about his/her illness.” Each item is answered twice on a 5-point Likert-type scale, and total scores are calculated for frequency and difficulty. Higher values indicate higher frequency/difficulty. Cronbach's α was .94 for frequency and .92 for difficulty in this sample.
Posttraumatic Stress Symptoms
These were measured using a Swedish translation of the Impact of Event Scale-Revised (IES-R) (Weiss & Marmar, 1997). Three dimensions (intrusion, avoidance, and hyperarousal) are measured using 22 items answered on a 5-point Likert-type scale. Higher scores indicate more symptoms. In this study, Cronbach's α was .91.
Anxiety and Depression
Seven-point VDSs assessed anxiety (1 = never anxious to 7 = always anxious) and depression (1 = never depressed to 7 = always depressed). These were considered as individual, separate items. Using VDSs for assessing anxiety and depression agrees well with established instruments for these constructs (Onelöv et al., 2007).
We also collected background demographic data such as parents’ age, occupation, sex, and education and children's age, sex, and diagnosis.
All data were collected using online or paper questionnaires according to parental preference. Measurements were made at baseline, and then at weeks 20, 24, 30, 46, and 74 postdiagnosis to capture the long-time effect of the intervention.
After each meeting, the INs reported what topics they discussed, the duration of the meeting, the elements of the representational approach they used, and their satisfaction and difficulty with various aspects of the meeting (measured on a 7-point scale ranging 1 = very easy to 7 = very difficult).
Analysis
For missing values in all instruments, we imputed the mean value for the remaining items in that specific subscale for that individual when <10% of the items were missing. The intention was to recruit 130 parents in total, expecting a moderate Cohen effect size (0.5) corresponding to a 13 points difference in the total score of the PIP, α = .05, and power = .8 (Ringnér, Björk, et al., 2015).
Baseline continuous variables were reported as the arithmetic mean ± standard deviation, and categorical variables were reported as frequencies. Baseline characteristics for the two intervention arms were compared using the Mann–Whitney U-test for continuous variables and Fisher's exact test for categorical variables. Because of a relatively large number of drop-outs in follow-up measurements, we calculated each participant's mean ratings at available time points during follow-up for comparisons. Differences between the trial arms were then evaluated using the Mann–Whitney U-test for each outcome variable (Field, 2009). The intention-to-treat principle guided the comparisons, and two-tailed p-values ≤.05 were considered statistically significant.
The INs’ short reports of the meeting topics were analyzed using deductive qualitative content analysis (Graneheim & Lundman, 2004; Hsieh & Shannon, 2005) and predetermined categories from a previous study (Ringnér, Karlsson, et al., 2015).
Ethical Considerations
Written informed consent was obtained from all participating parents. Participants had the option to withdraw from the study at any time. No adverse effects were reported by the participants. The study was approved by the Ethical Review Board in Umeå (Dnr 2014-167-31 M) and is registered at Clinicaltrials.gov (NCT02332226, December 11, 2014).
Results
Participant Characteristics
Parents of 164 children were eligible for the initial recruitment step. A total of 32 parents filled in the baseline questionnaires and were randomized into the study (Figure 1).
Participants’ mean age was 39 years. The two groups were equal on most baseline characteristics, but a greater proportion of the intervention group lived in larger cities. Of the participants, 66% (n = 21) were mothers and 34% (n = 11) were fathers. They were parents of 24 children with cancer. Demographics and equivalency statistics are displayed in Table 1. There were 16 participants from each of the two study sites.
Demographics of Participating Parents and Their Children at Baseline
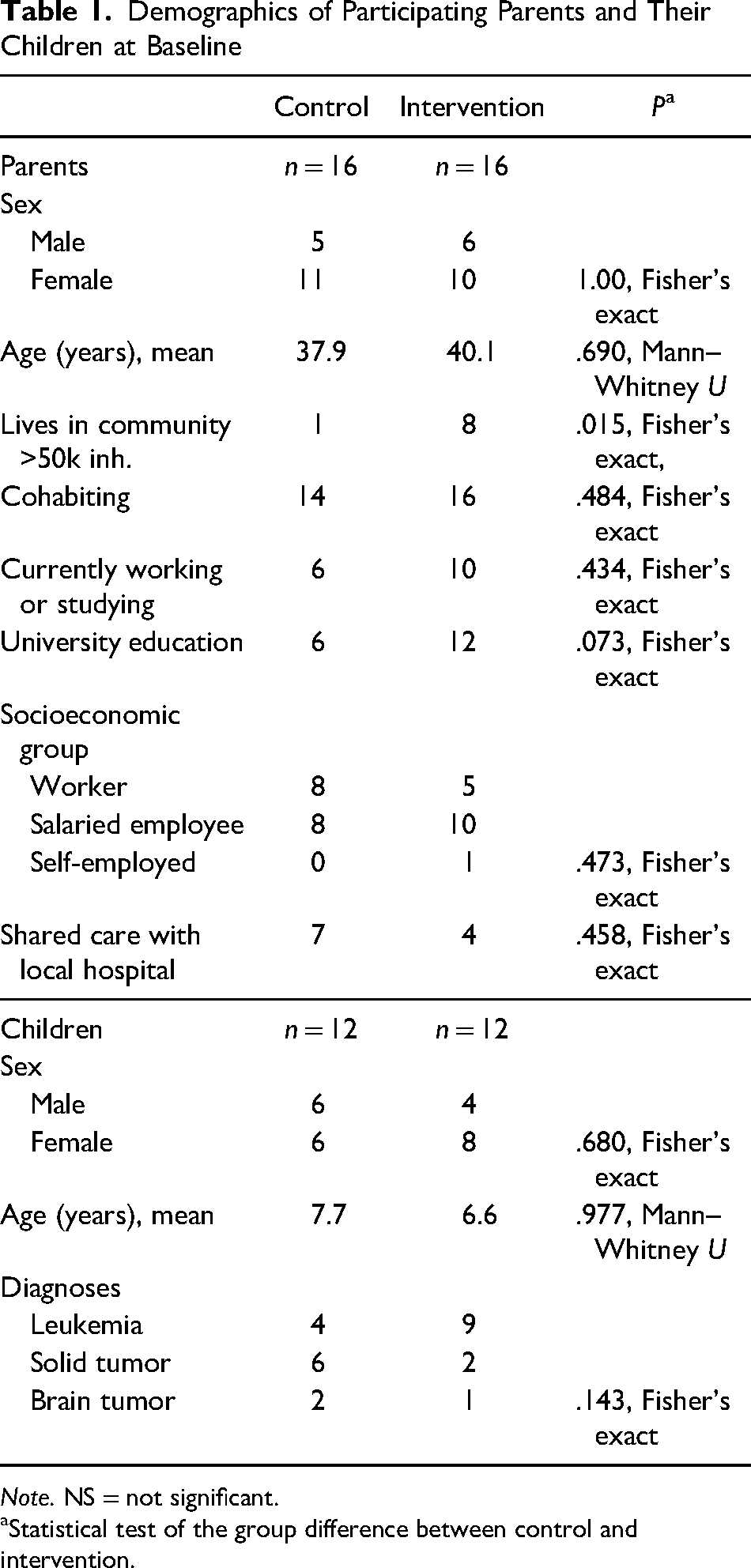
Note. NS = not significant.
Statistical test of the group difference between control and intervention.
Effects of the Intervention
No between-group differences were seen in the measures for illness-related parenting stress, posttraumatic symptoms, depression, or anxiety (Table 2). Parents in the intervention group, however, rated their knowledge expectations of the biophysiological and functional aspects of their child's illness, including topics such as symptoms, investigations, treatment, and self-care, better met than parents in the control group. In the intervention group, parents’ general satisfaction with the information provided increased over the time of the intervention, whereas satisfaction remained stable in the control group.
Differences Between Baseline and Mean Follow-Up Values
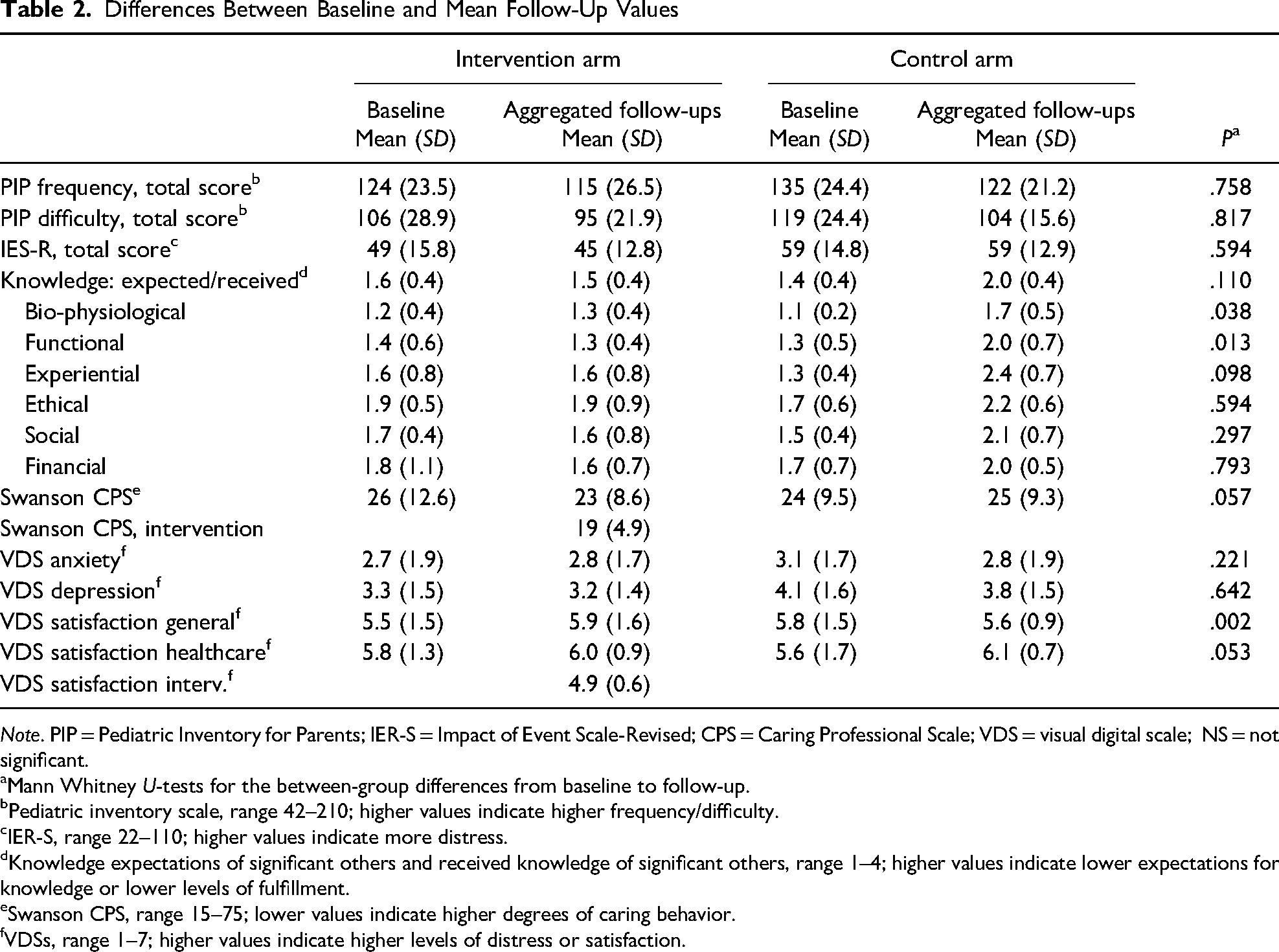
Note. PIP = Pediatric Inventory for Parents; IER-S = Impact of Event Scale-Revised; CPS = Caring Professional Scale; VDS = visual digital scale; NS = not significant.
Mann Whitney U-tests for the between-group differences from baseline to follow-up.
Pediatric inventory scale, range 42–210; higher values indicate higher frequency/difficulty.
IER-S, range 22–110; higher values indicate more distress.
Knowledge expectations of significant others and received knowledge of significant others, range 1–4; higher values indicate lower expectations for knowledge or lower levels of fulfillment.
Swanson CPS, range 15–75; lower values indicate higher degrees of caring behavior.
VDSs, range 1–7; higher values indicate higher levels of distress or satisfaction.
Using the Representational Approach
Parents attended an average of 3.5 meetings (range: 2–5) lasting on average 51 min (range: 15–105 min); two-thirds of the meetings were performed face-to-face and one-third over the phone. Other means such as video calls were not used. Technical problems were reported in only one meeting.
Before each meeting, parents were asked to identify a topic for which they needed more information or had questions. In 21 of the 56 meetings parents had identified a topic. When they had not, the INs often started by recapitulating the previous meeting or asking about their current situation as a way to identify topics.
The INs’ use of the elements in the representational approach (Table 3) varied between 100% (assessing representations) and 66% (giving feedback). In 14 of the 56 meetings (25%) the IN needed to refer the patient to another HCP on the team, such as the responsible physician, head nurse, social worker, or other support person.
Nurses’ Use of Elements in the Intervention Method
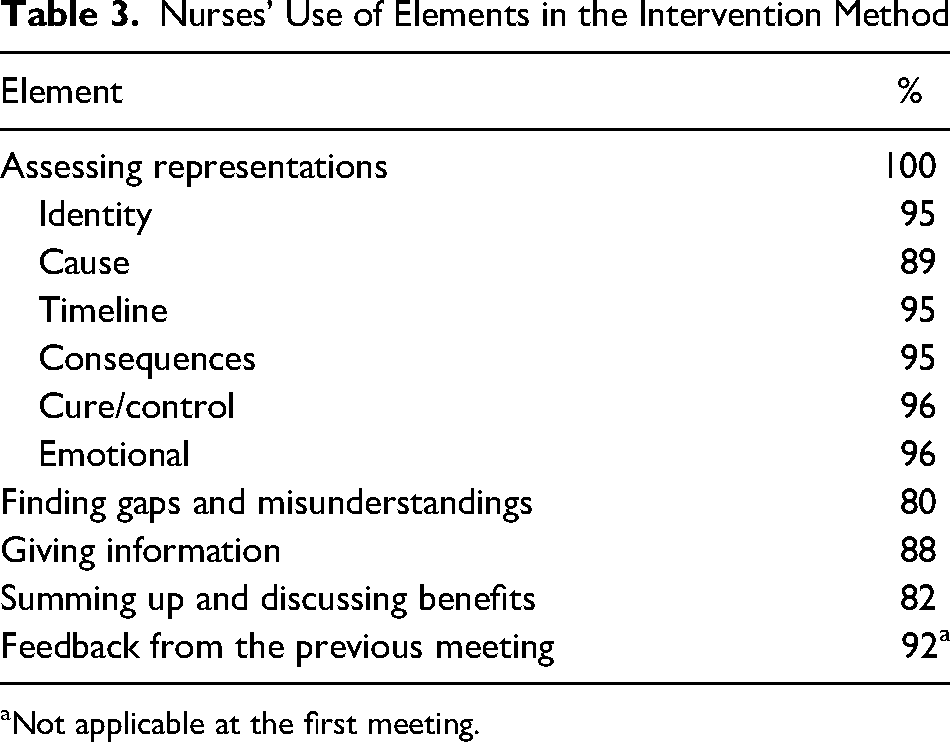
Not applicable at the first meeting.
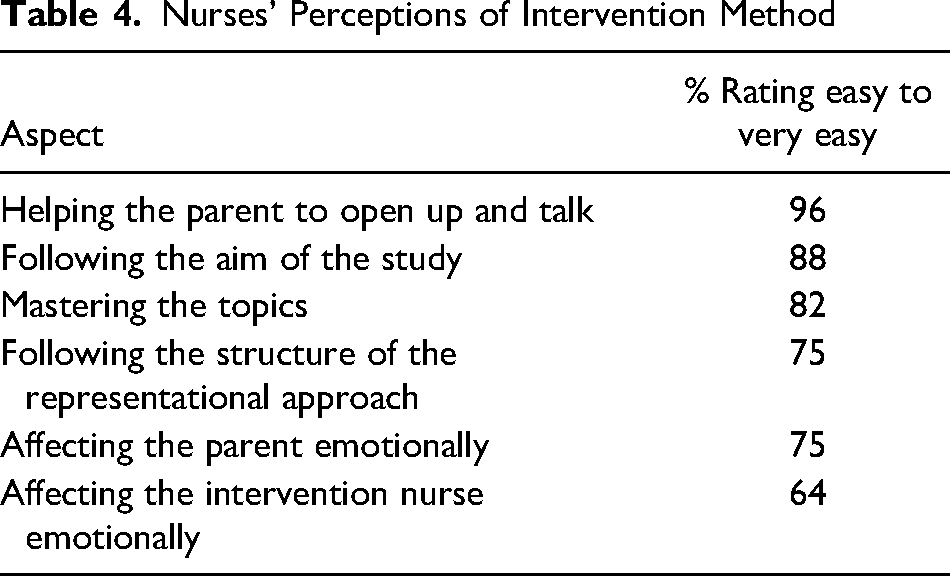
The INs reported feeling satisfied to very satisfied in 93% of the meetings. They rated “helping parents to open up” the easiest element and “being emotionally affected oneself” the least easy (Table 4).
Nurses’ Perceptions of Intervention Method
A wide variety of topics were brought up in the meetings, and many meetings focused on more than one topic. Emotional issues were most common (Table 5).
Topics Raised in the Meetings
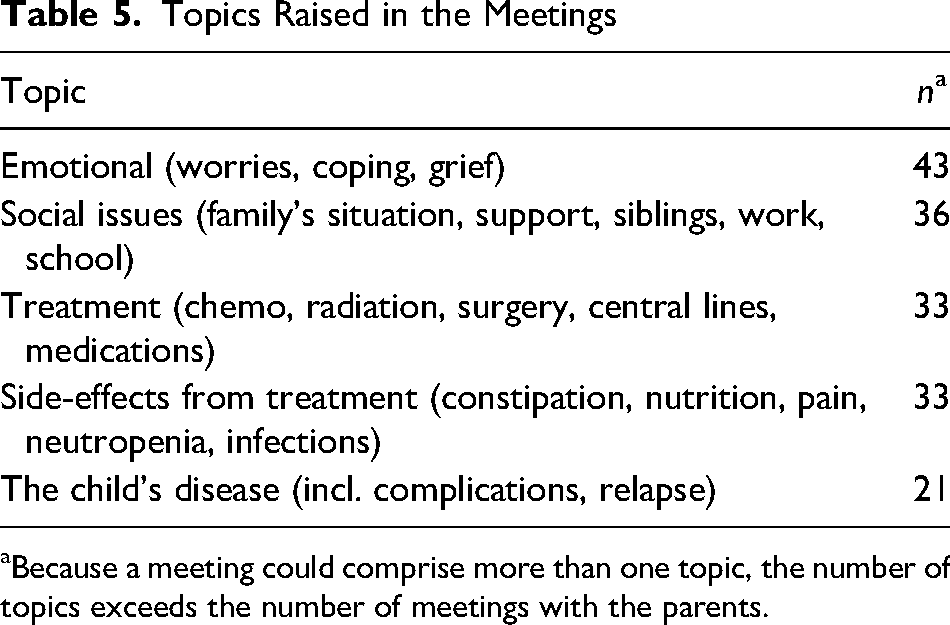
Because a meeting could comprise more than one topic, the number of topics exceeds the number of meetings with the parents.
Discussion
The aim of this study was to evaluate a multicenter RCT of a person-centered informational intervention for parents of children with cancer. Although the final sample size was too small to draw definite conclusions concerning the effect of the intervention, some interesting results need to be discussed. We found no differences between the intervention and control groups in psychosocial distress outcomes. The intervention group had their knowledge needs about biophysiological and functional aspects met to a larger degree than the control group. Parents in the intervention group were significantly more satisfied with the overall information they had received about their child's disease. The topics chosen by parents in the intervention ranged widely from medical issues to social and emotional concerns.
This intervention gave parents person-centered information about their child's disease and its consequences on the family's daily life. Other studies have evaluated educational interventions aimed at parents with cancer, and a recent meta-analysis reports small effect sizes for psychoeducational programs in reducing posttraumatic stress symptoms and improving mood (Tang et al., 2020). These studies taught coping strategies such as problem-solving and stress management. The intervention in the present study provided person-centered information about the child's disease, but failed to demonstrate any improvements in stress or symptoms of posttraumatic stress. Participants in the intervention did, however, demonstrate higher levels of knowledge in certain domains (biophysiological and functional) than the control group. This is also mirrored in the separate qualitative evaluation of this study, where parents in the intervention arm reported a deeper understanding of their entire situation (Ringnér et al., 2021).
Having a child diagnosed with cancer creates many information needs in parents. In the present study, the topics raised in the intervention varied from consequences of the disease and treatment on the child's health to emotional aspects of the parents’ situation. Encouraging parents to choose topics according to their own specific wishes and needs and arranging for them to discuss these with a competent and compassionate IN (Ringnér et al., 2021) reflect core components of person-centered care that aims to offer a respectful and individualized holistic nursing approach based on the person's choice (Morgan & Yoder, 2012). This is further in correspondence with recommendations about giving parents an opportunity to “dig deeper” into specific topics later in the treatment trajectory (Landier et al., 2016). Deeper insight into parents’ everyday concerns about their ill children could guide future interventions and provide pediatric oncology nurses with a better understanding of parents’ needs for information and support.
Treatment fidelity is a crucial factor for a successful intervention (Hasson, 2015). We used INs’ self-assessments to measure the components of the representational approach used and the difficulties encountered in the meetings (Tables 3 and 4). In general, the INs reported high adherence to the method, with each of the components used in at least 80% of the meetings. Nurses were also generally confident about mastering the topics and adhering to the aim of the study. As these were self-assessments, however, there is a risk of recall bias; the study might have benefited from observations or recordings of the meetings. Still, we believe that the nurses adhered closely to the representational approach in this study.
Methodological Considerations
The difficulty of recruiting parents into research studies during the first phase of their child's cancer is well-known (Stehl et al., 2009) and reflected in this study. The power analysis performed ahead of this study required 130 participants for a moderate effect size and a statistical power of p = .8 (Ringnér, Björk, et al., 2015). Our low recruitment rates could have had several reasons: organizational, parental preferences, and parental stress.
Our original plan was to recruit at four sites, however, staffing shortages in the prospective wards, likely a consequence of high nursing turnover in pediatric oncology in Sweden, made this impossible. At one site, one IN quit after about one year and was not replaced. Problems in accessing sites and losses of key people have been previously described as barriers to successful nursing research (Haugen et al., 2020; Lewis et al., 2014). With one intervention site partially unstaffed and a generally slow rate inclusion, we felt forced to stop recruitment prematurely.
We foresaw that the INs might have difficulty performing the intervention as part of their regular duties, with which the intervention might conflict. For this reason, the university hired the INs by the hour rather than compensating the hospitals for the time they put into the study. This worked well and the INs usually planned the intervention meetings right after or before their shifts on the ward. However, we should probably also have compensated the recruiting nurses to encourage recruitment to the study. Offering more directed guidance on how to approach eligible parents could also have been beneficial, as could intensifying the personal day-to-day contact with the remote site (Ringnér & Olsson, 2021). Furthermore, the study competed with several others running simultaneously on the same sites which may have distracted recruitment to this study.
Another general problem was that parents are introduced to several different clinical studies, not only about their child's disease and treatment, but also about their own situation, straight from the moment of diagnosis. Deciding whether or not to take part is known to create stress in some parents (Shilling & Young, 2009). Although Swedish ethical legislation does not allow researchers to ask why parents decline to participate in a study, the strain of being invited to yet another study might have contributed to parents’ unwillingness to join this one, especially as the PIFBO study was introduced a few weeks after diagnosis. Considering the difficult situation parents face, it is understandable that filling in questionnaires for a study has lower priority than their other more urgent chores.
We employed several strategies to improve data collection during follow-up. In a previous study, all participating parents chose to answer their questionnaires online after an email invitation (Ringnér, Karlsson, et al., 2015). However, in this study with the same population, many chose the paper questionnaires instead. Thus, questionnaires were first distributed by email, but parents also had the opportunity to request paper questionnaires, which were then sent out with a prestamped envelope. At a later stage of the trial, after email reminders, a research assistant also telephoned parents to politely remind them to return the questionnaires which increased the response rate in that stage.
Conclusions
This person-centered information intervention for parents of children with cancer addressed a broad variety of topics. The intervention increased parents’ received knowledge about biophysiological and functional aspects of their child's illness, but showed no effect on their psychosocial distress. Although the INs fidelity to the intervention protocol was sufficient, the study was flawed by recruitment difficulties, primarily due to organizational factors, which may have prevented us from observing more effects.
Supplemental Material
sj-doc-1-jpo-10.1177_27527530221115860 - Supplemental material for Effects of Person-Centered Information for Parents of Children With Cancer (the PIFBO Study): A Randomized Controlled Trial
Supplemental material, sj-doc-1-jpo-10.1177_27527530221115860 for Effects of Person-Centered Information for Parents of Children With Cancer (the PIFBO Study): A Randomized Controlled Trial by Anders Ringnér, Maria Björk and Cecilia Olsson in Journal of Pediatric Hematology/Oncology Nursing
Footnotes
Acknowledgments
We would like to express our sincere gratitude to the participating parents, to the INs, and to Ms. Benedicte Stendal Hansen, RN, MsN, for her diligent work in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Swedish Childhood Cancer Fund (Barncancerfonden; grant number: PR20130086).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.