
Abstract
Mental health disorders are widespread, affecting millions of people globally, creating a significant disease burden and leading to premature mortality. Stigma, discrimination, and social exclusion remain key barriers to mental healthcare, often preventing individuals from seeking help. Cultural differences shape the experience of stigma. To reduce stigma, three main intervention strategies are commonly used: education, social contact, and activism. Educational initiatives aim to replace harmful stereotypes with facts, while social contact programs, such as the ‘Human Library’, facilitate direct interactions between individuals drawn from stigmatised groups to improve understanding, reduce stigma, and discrimination. In the ‘Human Library’, people from marginalised groups, known as ‘Books’ share personal experiences with small groups of ‘Readers’. These interactions foster empathy and reduce prejudice. In this case study, we describe how we integrated the ‘Human Library’ into the curriculum of a postgraduate programme. Feedback across two consecutive cohorts of students indicated that the event was highly informative and encouraged students to challenge their own biases. The project’s success has led to plans for its continued use, with hopes to further assess its impact on mental health literacy and prejudice as well adapting it for our online distance learning students.
Introduction
Mental health disorders are prevalent and are in the top ten leading causes of the global burden of disease (GBD 2019 Mental Disorders Collaborators, 2022). In 2019, it was estimated that 970 million people were living with a mental health disorder (World Health Organization [WHO], 2024) and that in over half of cases, the average age of onset is under 25 (Solmi et al., 2022). In the student population, mental health problems appear to be increasing. Globally, a recent meta-analysis including over 100,000 students reported a pooled prevalence of 33.6% for depressive symptoms and 39.0% for anxiety symptoms amongst college students (Li et al., 2022). Poor mental health in students is associated with lower educational achievements (Patel et al., 2007). Anxiety and depression are the leading causes of disability-adjusted life years (DALYS) for young adults (Mokdad et al., 2016).
Furthermore, while life expectancy has improved for the general population over the last 60 years (World Bank, n.d), men and women with any mental health disorder die around ten years earlier than those living without one (Erlangsen et al., 2017). During the COVID-19 pandemic, the mortality rate for people with mental health disorders remained elevated, with deaths at least double the population average (Das-Munshi et al., 2021). While many factors contribute to this mortality gap, stigma, discrimination, and social exclusion are recognised as having an important impact (O’Connor et al., 2023; Thornicroft et al., 2022). Stigma, discrimination, and social exclusion are among the greatest barriers to achieving equitable healthcare worldwide and are important social determinants of health (Liamputtong and Rice, 2022).
Stigma, discrimination, and social exclusion
Stigma, first described by Goffman (1963), is a social construct strongly influenced by cultural and contextual factors which vary over time. Key components of stigma, such as labelling and stereotyping, lead to rejection, prejudice, discrimination, social isolation, and marginalisation (Subu et al., 2021). Stigma may occur due to health factors (such as a diagnosis of cancer, HIV, and mental health disorder), and non-health factors (such as age, gender identity, and sexuality). Discrimination, sometimes described as the endpoint of stigmatisation (Link and Phelan, 2001), is defined by the Joint United Nations (UN) Program on HIV/AIDS (UNAIDS) as ‘any form of distinction, exclusion, or restriction affecting a person, usually, but not only, by virtue of an inherent personal characteristic, irrespective of whether or not there is any justification for these measures’ (UNAIDS, 2000: 7). Although no widely recognised definition of social exclusion is found, the UN consider social exclusion to be ‘a state in which individuals are unable to participate fully in economic, social, political, and cultural life, as well as the process of leading to and sustaining such a state’ (UN, 2016: 18).
Within the context of mental healthcare and service provision, stigma remains particularly problematic, affecting all aspects of care and treatment (Sartorius, 2007). Mental health stigma is a global phenomenon with a report suggesting that ‘stigma is universal’ (Rössler, 2016: 1251). Stigma and its consequences can lead to delays in diagnosis and treatment, reduced quality of life, and increased mortality (Ahad et al., 2023). Commonly held stigmatising views towards people with mental illness include that they are ‘dangerous’, ‘unpredictable’, and ‘aggressive’ (Crisp et al., 2000). Furthermore, the deficit-based framing of mental illness and disability may worsen stigma (Cuttler and Ryckman, 2019).
Stigma is a multi-faceted concept. Self-stigma (or internalised stigma) refers to the negative attitudes an individual may have towards their own mental illness (Corrigan, Powell, and Rüsch, 2012b), as well as concerns about being exposed to stigmatising attitudes held by others (Valery and Prouteau, 2020). High levels of self-stigma can lead to negative health outcomes such as reduced quality of life (Corrigan et al., 2014) and increased suicidal ideation (Oexle et al., 2017). The negative attitudes of the public towards people with mental illness, known as public stigma (Corrigan, Morris et al., 2012a), can have wide-reaching discriminatory effects, negatively affecting employment, income, and housing (Valery and Prouteau, 2020), and increasing the potential for experiencing social exclusion. Structural (or institutional) stigma refers to organisational cultures and policies that reinforce negative and stigmatising attitudes towards people with mental illness (Broham and Thornicroft, 2010; Livingston, 2013). One example is laws that criminalise suicide and suicidal behaviour (Thornicroft et al., 2022). Structural stigma can have significant economic implications including impacts on healthcare resource allocation (Sharac et al., 2010).
Furthermore, healthcare systems and healthcare professionals can also be sources of stigma and discrimination towards people with mental illness (Mestdagh and Hansen, 2014; Sartorius, 2007). In the United Kingdom, the General Medical Council (2024) has produced the ‘Good Medical Practice’ document, which outlines the principles, values, and responsibilities of all registered medical professionals. It states that all professionals should ‘respect every patient’s dignity and treat them as an individual’ and ‘never unfairly discriminate against patients or colleagues’ (General Medical Council, 2024: 7). However, sometimes healthcare professionals may not fully uphold these values and responsibilities. For example, Ross and Goldner (2009) reviewed the literature on mental health stigma and discrimination in the nursing profession and found stigmatising views towards people with mental illness within the general hospital setting, as well as towards psychiatric nurses (Ross and Goldner, 2009). Furthermore, Van Boekel and colleagues (2013) reported generally negative attitudes towards patients with substance use disorders amongst health professionals. Stigmatising and discriminatory views amongst health professionals are particularly problematic, as they may discourage help-seeking, impede patients’ access to appropriate and high standards of care, contribute to self-stigma, ultimately preventing a person from recovering (Nyblade et al., 2019). Thus, mitigating strategies are needed.
Culture influences how mental illness presents, and the types of services people will engage with (Ahad et al., 2023). Different cultural understandings of mental illness can lead to stigma and its consequences manifesting differently across the world. For example, in some cultures, mental illness is considered a sign of personal weakness (Chen and Mack, 2008). Any associated stigma may become internalised, leading to a reluctance to seek help. By comparison, other cultures may view mental illness through a supernatural lens (Girma et al., 2013), and the associated mental health stigma reflects issues around one’s spirituality. These cultural differences are reflected within student populations, where research has highlighted inequalities between different geographical settings. Gallego and colleagues (2020) observed higher rates of stigma in Spanish university students compared to Russian and Canadian university students.
Despite the increased prevalence of mental health problems in the student population (Kings College London, 2023) and the negative impact this can have on academic performance (Bruffaerts et al., 2018), only around a third of students seek help (Eisenberg et al., 2011). Reasons for this are unclear and multifactorial, but it is likely that personal and public stigma are important contributors (Wada et al., 2019). University teaching staff have a duty of care towards students, are potential gatekeepers, and should ensure that they have adequate mental health literacy and non-discriminatory views to support and signpost students to the relevant services if needed (Gulliver et al., 2017). However, teaching staff often do not receive formal training on how to respond to student mental health problems. Many staff lack confidence when talking about mental health issues with students, particularly those with suicidal thoughts, and feel they are not sufficiently informed to respond appropriately (Gulliver et al., 2018; Kalkbrenner et al., 2019). Reports have also documented a lack or low awareness of mental health policies and strategies to guide the actions of staff (Gulliver et al., 2018; Orygen, 2017).
Raising awareness and improving attitudes towards mental illness and other stigmatised groups in the student population is of great importance, due to both the current elevated rates of mental health problems reported in the student population globally (Li et al., 2022) and the future role students will have in their employment. According to a recent job market report, analytic and creative thinking remain the most important skills for workers, followed by resilience, flexibility, and agility, with empathy and active listening also reported in the top ten core skills (World Economic Forum, 2023). With more emphasis being placed on diversity within the workforce, interventions to improve mental health literacy and reduce stigma are recognised as important to embrace equity and inclusion.
Strategies to address stigma and discrimination
Many studies have explored interventions to reduce stigma. In general, three types of approaches may be engaged, these being educational, interpersonal, and activism. An educational approach challenges harmful, inaccurate stereotypes and replaces these with facts (Corrigan and Penn, 1999). Educational strategies can be carried out at a local or a national level, for example, the Scotland-wide education-focused anti-stigma campaign ‘See Me’ (See Me, n.d; Robertson, 2017) and Show Racism the Red Card (n.d). In general, public education-focused anti-stigma interventions reduce stigma in the short term (Griffiths et al., 2014), but evidence for sustained long-term change is lacking (Thornicroft et al., 2016).
Educational strategies targeting stigma related to mental illness usually rely on improving Mental Health Literacy (MHL). MHL is an evolving term, initially conceptualised as ‘the knowledge and beliefs about mental disorders which aid their recognition and management’ (Jorm et al., 1997: 182). However, it has been further developed to include additional aspects such as knowledge about mental illness prevention, early intervention, self-help strategies for mild illness, mental health first aid skills to support people in a mental health crisis (Jorm, 2012), and strategies to reduce mental health stigma and discrimination within society (Wei et al., 2015). Improved MHL at an individual and wider societal level aims to enhance mental health outcomes through earlier recognition of mental health problems and increased access to mental health services (Wei et al., 2015). In general, higher levels of MHL are associated with more positive attitudes towards people with mental illness (Svensson and Hansson, 2016).
An interpersonal approach involves providing people with opportunities to meet people who may be associated with the stigmatised group in a safe setting (Corrigan, 2005). This aligns with Allport’s (1945) Intergroup Contact Theory, which proposed that supportive and collaborative contact between different social groups could reduce prejudice. This type of intervention has been shown to reduce public stigma, as well as self-stigma (Corrigan et al., 2012a). In some cases, social contact interventions may be combined with educational interventions. For example, facts about a mental illness may be presented, and then a person with lived experience may contextualise the information. From evidence collated from over 70 studies exploring mental health-related stigma, Corrigan and colleagues (2012a) found that, for adults, social contact was more effective than education, but in adolescents, education was more effective than social contact. A systematic review of interventions to reduce mental health-related stigma in higher education students included and synthesised evidence from 35 studies (Yamaguchi et al., 2013). The review concluded that social contact and video-mediated social contact interventions led to improved attitudes towards those living with mental illness and reduced a stated desire for social distance (Yamaguchi et al., 2013). This was replicated by Amsalem and colleagues who found that a 90 second video intervention reduced stigma amongst nearly 2000 young adults aged 18–35 (Amsalem et al., 2022). Corrigan and colleagues (2012a) noted that, in their study, face-to-face contact was determined to be more effective in reducing stigma than video contact.
Finally, social activism or protest can be used to reduce stigma. Here, negative representations of a stigmatised group are challenged by objecting to instances where this occurs (Arboleda-Flórez and Stuart, 2012). However, the evidence for social activism being effective is mixed, with some studies suggesting it can help reduce stereotypes (Eiroa-Orosa and Rovira-Gimó, 2024; Sawaf, 2022; Wahl, 1995), and others suggesting it worsens stereotypes (Macrae et al., 1994).
The ‘Human Library’
The concept of a ‘library’ has expanded from a traditional physical space with collections of books (Bonnand and Donahue, 2010) to any space (including virtual spaces) in which collections of images, videos, audio files, and even real people exist. The first ‘Human Library’ was established in 2000 in Denmark when the group ‘Stop the Violence’ hosted a series of ‘Human Book’ events as part of the Roskilde Festival (Sung et al., 2017). These events aimed to educate and encourage young people to become active in violence prevention. During sessions, people with lived experience acted as ‘Books’. They shared their experiences with attendees, termed ‘Readers’. Instead of reading, attendees engaged in direct conversations with the human ‘Books’, gaining insights into their lives, cultures, and perspectives with the aim of reducing stigma through social contact. After the festival, the ‘Stop the Violence’ group set up the ‘Living Library’ organisation, which became the ‘Human Library’ in 2010 (Little et al., 2011).
The ‘Human Library’ enables safe and confidential dialogue between volunteers drawn from a stigmatised group (the ‘Books’) and learners (the ‘Readers’). A human ‘Book’ is ‘a person that volunteered to represent a stigmatised group in the community and based on their personal experiences can answer questions from Readers to help challenge what is being said/told/understood about a given topic. To help shed light on the facts as you know them. Books are not political or on a mission when with us, but rather able to surrender to the agenda of the Reader and allow them control of the conversation’ (Human Library, n.d., a).
The ‘Human Library’ continues to evolve its language and, just like a library, tries to be neutral, apolitical, and non-activistic. It uses language that encourages engagement rather than taking an ideological or agenda-driven stance. For example, they would describe volunteer ‘Books’ as ‘drawn from’ rather than ‘representing’ groups in society, as the volunteers only represent themselves. This gives agency, autonomy, and authenticity to how ‘Books’ respond, allowing them to answer questions directly referring to their own experience, not with textbook replies and definitions, nor from activistic viewpoints. Similarly, the language of ‘counter’, ‘combat’, or ‘challenge’ has been dropped in favour of ‘explore’, ‘discover’, and ‘encounter’, as this is more conducive to constructive dialogue as opposed to debate or lecturing methodologies.
‘Books’, therefore, draw upon their personal experience, not professional expertise, to answer questions asked by small groups of ‘Readers’, typically three to five people. They are not paid for their time. To help facilitate the ‘Readings’ and ensure a safe space, one or more ‘Librarians’ and a facilitator from the ‘Human Library’ are present. ‘Librarians’ are also volunteers whose roles can include sourcing new ‘Books’, liaising with them, coordinating travel and arrangements, and providing ‘Books’ with debriefings and support following ‘Readings’.
Sessions encourage attendees to ‘unjudge someone’ (Human Library, 2024). The ‘Human Library’ facilitators emphasise that ‘unjudging someone’ starts with the self, including their opinions and prior judgements held and their fear about asking the necessary questions to elicit the information needed to modify existing assumptions. Participants are encouraged to ‘unjudge’ their colleagues’ and classmates’ questions and not make assumptions about where they came from, or what they say about the questioner’s views or experiences. As the sessions are not directive or orientated around an objective, the option to ‘unjudge someone’ is a choice, not a requirement. Through the dialogue created during the ‘Reading’, the ‘Human Library’ aims to promote understanding, which helps challenge stereotypes and stigmatising beliefs (Johannsen, 2015).
‘Books’ are similarly encouraged to ‘unjudge’ their ‘Readers’ and to ask questions such as ‘what do you already know about my Topic?’ or ‘have you previously encountered people like me?’ This stimulates conversation and demonstrates the unjudgement and openness they hope to receive. This approach draws from Iacoboni’s (2008) psychological mirroring effect where imitation is used to establish rapport and empathy, through mirroring physical body language, attitude and acceptance, humour, and warmth.
Humility and humbleness underpin the ‘Human Library’. Event facilitators and Library ‘rules’ often use gentle humour to encourage ‘Readers’ to relax into reading; commonly used phrases associated with physical libraries are used. For example, ‘Readers’ are asked to ‘avoid writing on the Books’ or ‘make sure the Books are returned on time’. This extends to ‘Books’, who will encourage questions from ‘Readers’ by putting them at ease through jokes such as saying they will ‘answer anything but [Readers] may regret that!’
Within the ‘Human Library’ event space, safety and bravery to ask any question without offence is encouraged. Participants are reminded that this is a consensually created space, not the outside or online world, and others may not respond so openly to the curious and courageous questions encouraged during the ‘Human Library’ sessions. The ‘Human Library’ ‘Books’ receive many hours of training to preserve personal boundaries, feel safe, know how to access support, not take offence at unintentional language differences or lack of knowledge about insensitivities, and be able to recognise that although they speak only to their personal lived experience, they also bear a responsibility to inform ‘Readers’ that others seen as part of the same group, belief, identity, diagnosis, or difference may hold different views. While a safe space is created, it is recognised that environments can never be entirely controlled and that, ‘Security is mostly a superstition. It does not exist in nature, nor do the children of men as a whole experience it. Avoiding danger is no safer in the long run than outright exposure. Life is either a daring adventure, or nothing’ (Keller, 1957: 50–51). It is important to acknowledge that some interactions taking place as part of a ‘Human Library’ session can lead to ‘Books’ feeling emotionally vulnerable (Kwan, 2020). On the other hand, interactions can also provide ‘Books’ with new perspectives or prompt self-reflection and opportunities for growth (Kwan, 2020). The concept of a ‘Human Library’ is therefore complex and requires careful consideration and coordination to mitigate any risk of harm to ‘Books’.
The ‘Human Library’ has an international presence, with events being held across six continents in over 80 countries including Japan (Kudo et al., 2011), Poland (Groyecka et al., 2019), and Hong Kong (Chung and Tse, 2022). Unlike educational interventions, which are often pre-prepared and pre-planned, the events held by the ‘Human Library’ allow the development of spontaneous and organic conversations between ‘Books’ and ’Readers’ (Abergel et al., 2005). This social contact is thought to be a powerful tool to help challenge negative stereotypes (Garbutt, 2008). The ‘Human Library’ aims to ‘rid discrimination, prevent conflicts and contribute to greater human cohesion across social, religious and ethnic divisions’ (Human Library, n.d., b).
Context
The on-campus Global Mental Health (GMH) Master of Science (MSc) Programme is based within the School of Health and Wellbeing (SHW), which sits in the College of Medical, Veterinary and Life Sciences (MVLS) at the University of Glasgow, Scotland. The SHW holds an Athena Swan Gold Award and, as such, equality, diversity, and inclusion are central values embedded through all aspects of teaching and research activity. The GMH MSc was launched in the 2012–13 academic year and as an online distance learning (ODL) Programme in 2016–17. The Programme attracts a diverse cohort of students from various disciplines, including clinical and other professional backgrounds. In the 2023–24 academic year, the Programme had 48 registered on-campus students, of whom 39 were international (81%), and an additional 34 ODL students. The international students come from countries including (but not limited to) Brazil, Canada, China, India, Kenya, Lebanon, Nigeria, Ukraine, and the United States. With this diversity, a range of cultural, societal, religious, and legal perspectives, schemas, and stigmatisations can arise that have relevance when exploring the causes, experiences of, and management of mental health.
Informed by pedagogical literature focused on blended learning (Alammary et al.,. 2014; Cooner, 2010) and student feedback collected across the programme (Sharp et al., 2018), the online materials have been curated over the past eight years and consist of a range of asynchronous learning activities with informative text, key readings, case studies, videos, quizzes, assessment tips, self-care activities, employability insights, and note-taking activities. The online materials, prepared using Articulate Rise 360, are hosted on Moodle and are available to both the on-campus and ODL students. This allows a ‘flipped classroom’ approach, whereby the on-campus students engage with and independently progress through the online core learning materials, and time in the classroom is used for active learning (McNaughton and Bhardwaj, 2022). Learning materials have been reviewed to ensure they are accessible, diverse, and inclusive. For example, a diversity review of the curriculum was undertaken using the Open University, 2022 Whose W.O.R.D.D. counts? tool (Foley et al., in press) and, most recently, the process of decolonising the curriculum has commenced (Sharp et al., 2025). Assessments have also been reviewed and redesigned to be authentic to provide students opportunities to apply their learning to real-world scenarios (Karadzhov et al., 2021).
While stigma and discrimination are central themes throughout the Programme, one of the core courses, Mental Health and Disability: International Law and Policy, explores these issues and strategies to address them in depth. The course focuses on mental health legislation and policies through a human rights lens and is grounded in core equality and inclusivity principles. Efforts have been made to include videos of people from a range of racial, cultural, and geographical, backgrounds describing their lived experience of mental illness. However, the course team believed that the opportunity to engage on a personal level with individuals who have experienced stigma and discrimination would be a powerful learning experience. The ‘Human Library’ provided a service that could offer this experience in a safe environment for all those participating.
Graduates of the Programme seek to apply the knowledge, skills, and attributes established in the MSc to develop and deliver mental health services and systems around the globe. The field of GMH is professionally diverse, and many graduates gain roles in clinical settings and third-sector organisations, as well as pursue further doctoral-level study. To gain the skills needed to work across a variety of settings and to be empathetic, responsive, and aware of broader socio-political factors that influence a person’s mental health, GMH graduates must be aware of the stigma and biases they hold and be able to ‘unjudge' someone in order to provide a high standard of care. Aligned to the University of Glasgow’s Graduate Attributes (University of Glasgow, 2024a) and the MVLS Education Strategy (University of Glasgow, 2024b), which is underpinned by the core values of equality, diversity, inclusion, integrity, and respect, we aim to ensure our potential graduates are ‘ethically and socially aware’. A recent job market analysis undertaken by a member of the Programme team led to the development of a multi-sectorial, multi-professional GMH competency framework (Karadzhov et al., 2024). This analysis found that values such as: humility, empathy, and compassion; respect for diversity, fairness, and inclusion; a commitment to social justice; integrity; and honesty were highly sought skills (Karadzhov et al., 2024). These values are targeted throughout the course.
Pedagogical underpinnings: Contact-based education, critical pedagogy, and experiential learning
The integration of the ‘Human Library’ project into the GMH curriculum draws on several pedagogical methodologies. The project has taken inspiration from contact-based education, critical pedagogy, and experiential learning which have each been engaged across health education contexts to break down barriers between practitioners and patients, reduce stigma, promote critical consciousness, and challenge dominant knowledge schemas. Contact-based methodologies draw from Intergroup Contact Theory (Allport, 1945), offering structured interactions between learners and stigmatised groups to improve the attitudes, beliefs, and behaviours of students and future practitioners (Al-Ma and Hamdan-Mansour, 2020; Bakos-Block, 2020; Tucker et al., 2020). Intergroup Contact Theory recognises the power of interactions in forming attitudes and beliefs (Tucker et al., 2020). Facilitating interactions with stigmatised groups can encourage positive attitudes and critical self-reflection, challenge power dynamics, and decrease feelings of discomfort when engaging with patients (Tucker et al., 2020).
Studies assessing the impact of contact-based methodologies have reported improvements in attitudes towards patients, including reduced anxiety during interactions, less desire to socially distance, and more interest in patients and their histories (Al-Ma and Hamdan-Mansour, 2020; Bakos-Block, 2022; Tucker et al., 2020). However, within contact-based methodologies, there is significant variation in the type of contact (face-face, virtual, or impact statements), the length of contact, and the extent to which students are encouraged to ask questions. Contact-based methodologies often feature a presentation from a person with lived experience (Al-Ma and Hamdan-Mansour, 2020; Bakos-Block, 2022; Tucker et al., 2020), healthcare providers (Al-Ma and Hamdan-Mansour, 2020; Tucker et al., 2020), and/or family members (Al-Ma and Hamdan-Mansour, 2020; Tucker et al., 2020). In these interactions people share their experiences of receiving care and treatment, and recovery in lecture based (Al-Ma and Hamdan-Mansour, 2020; Bakos-Block et al., 2022; Tucker et al., 2020), small group (Tucker et al., 2020), and/or clinical formats (Tucker et al., 2020). There is a lesser emphasis on the role of student questions, and the level of interaction between students and the person from a stigmatised group.
The ‘Human Library’ approach to social contact brings in additional dimensions of critical pedagogies and experiential learning. Paulo Freire’s critical pedagogy is an approach grounded in critical theory where education is seen as a tool to dismantle oppressive systems (Freire, 1970). Knowledge is considered socially constructed. As David Didau states ‘learning is fundamentally social. We don’t just learn facts, we learn from the context in which we encounter those facts’ (Didau, 2012: n.p.). In the ‘Human Library’ learners are encouraged to deconstruct and actively rebuild their knowledge through dialogue and problem-solving, fostering an awareness of dominant schemas and power dynamics within and outside the classroom (Matthews, 2014; Uddin, 2019). In the ‘Human Library’, students control the dialogue. ‘Readers’ can critically question health information through the ‘Readings’, engage with people from marginalised and stigmatised groups, and learn from their stories in ways that may challenge dominant narratives. This immersive approach draws on experiential learning methodologies where learners are provided with chosen experiences, and encouraged to critically reflect, analyse, and synthesise learning with previous knowledge (Thomas et al., 2024). During experiential activities, learners are expected to take initiative and ask questions, adopting a stance of curiosity to construct new meaning (Varker and Small, 2021).
Vaker and Small (2021) highlight the importance of discomfort in experiential learning. The ‘Human Library’ provides an environment where participants are encouraged to move beyond normal conversation, where people are bound by notions of politeness, to ask questions that may provoke discomfort. This pushes them into spaces of learning where they can engage directly with the knowledge that has informed any stigma or biases held. When critical pedagogies and experiential learning are combined, it leads to activities that expose students to diverse demographics, facilitating empathy and understanding through direct interaction and reflective practices (Varker and Small, 2021).
Project approach and aims
The project aimed to introduce a novel and innovative learning session to the GMH Programme to further embed core values of equality, diversity, inclusion, integrity, and respect into the curriculum. Furthermore, the session aimed to encourage students to learn about, recognise, and challenge their own stereotypes, which may contribute to stigma and discrimination. With initial funding from the MVLS College Equality, Diversity, and Inclusion Committee (CEDIC), the first learning event facilitated by the ‘Human Library’ was organised for the 2022–23 cohort of Mental Health and Disability: International Law and Policy on-campus students. A second ‘Human Library’ event was delivered to the 2023–24 cohort of on-campus students taking the same course. There was no option for the ODL students to attend remotely.
Summary of ‘human library reading hall’ event structure.
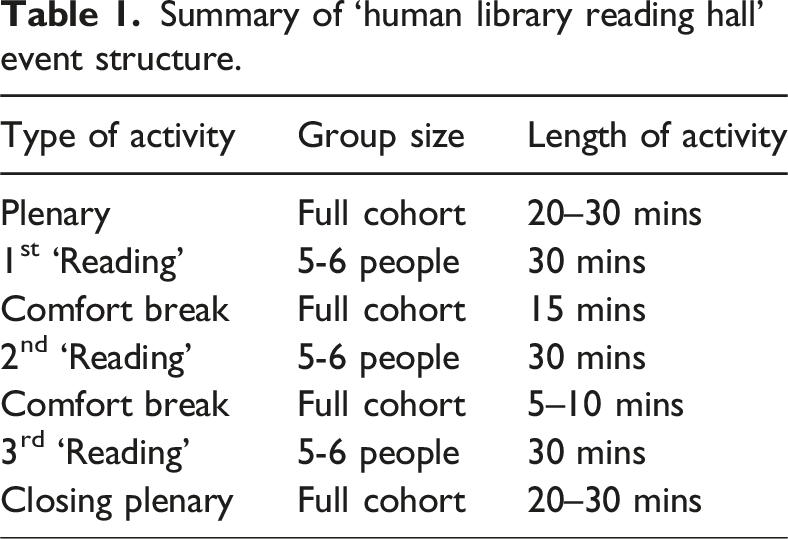
The ‘Human Library’ session was embedded in the weekly timetable for the on-campus students across both academic years from the start of the semester and so was an expected learning event as part of their timetabled teaching. Attendance at teaching events is not compulsory but is strongly encouraged. Funding from the CEIDC allowed students who attended to be given a catering card to purchase refreshments from university vendors. This feature was retained for the 2022–23 cohort of students. At the start of each event, time was spent by the ‘Human Library’ facilitator explaining the format, purpose, and establishing the ‘Reading Hall’ as a safe and brave space to ask questions and ‘be curious’. Content advisory warnings for potentially distressing topics that may be discussed by a ‘Book’ were given at the outset and within the conversations, with varied options on navigating any potential discomfort.
In 2022–23, six ‘Books’, three ‘Librarians’, and a ‘Human Library’ coordinator delivered the session. ‘Books’ drew on experience across various intersections of marginalisation and mental health, including religion, physical impairments, gender identity, eating disorders, gang membership, and abuse. Some ‘Books’ represented overlapping and intersecting experiences, reflecting the diversity and intersectionality inherent in society; as the facilitator summarised in the feedback session using Lorde’s words, ‘There is no such thing as a single-issue struggle because we do not live single-issue lives’ (Lorde, 1984: 138).
The 2023–24 session drew on eight ‘Books’ with additional marginalisation experiences, bringing insights from people with experience of migration, domestic violence, and undertaking sex work, as well as those who had been diagnosed with anorexia, bipolar disorder, and complex post-traumatic stress disorder (cPTSD). The ‘Library’ also included ‘Books’ with experience of living with autism, being a carer, and from diverse sexualities and gender identities. Intersectionality was again observed within the ‘Books.’
Methods
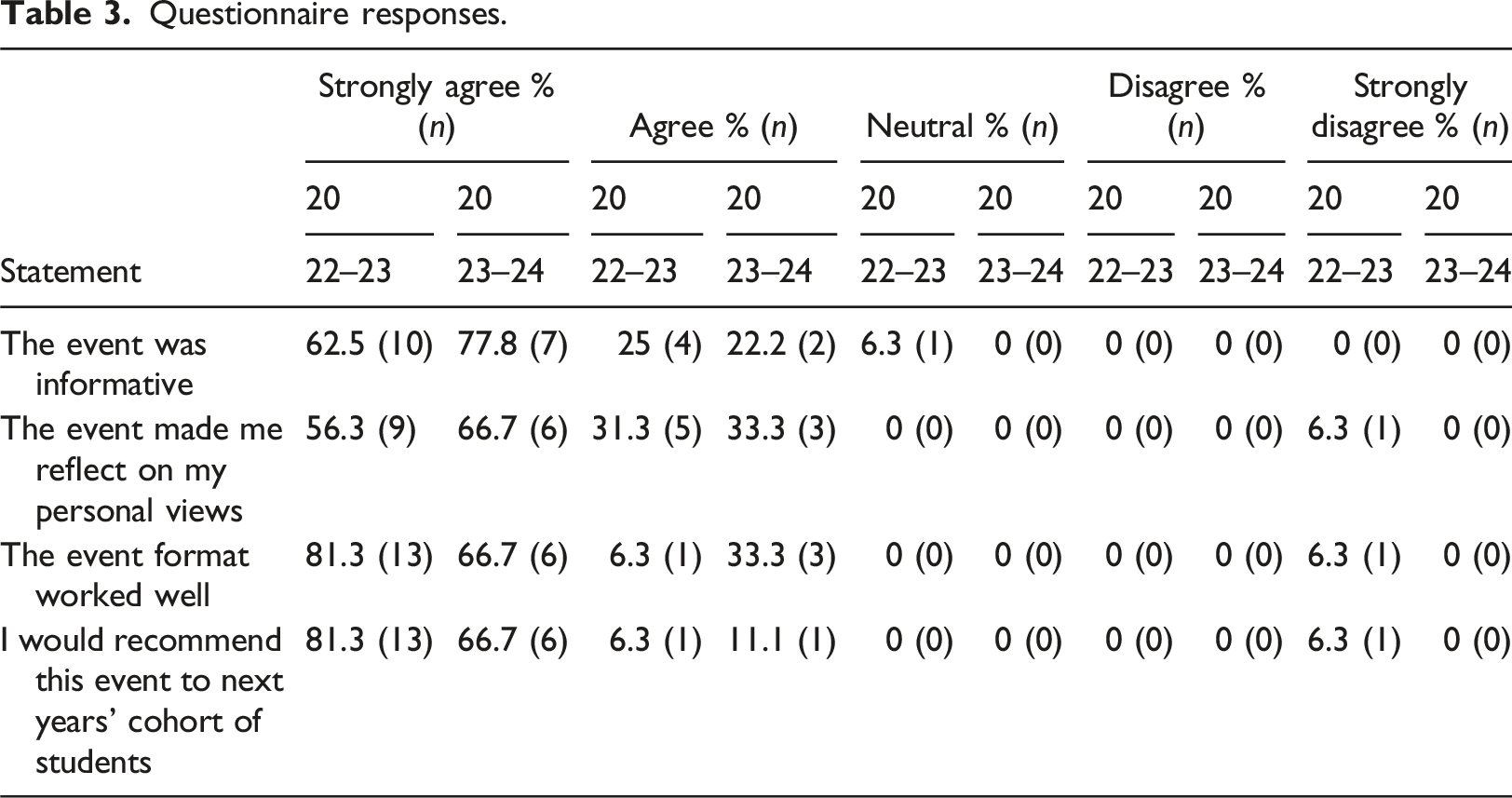
At the end of the event, students were invited to complete a short, online anonymised questionnaire. This included four questions that adopted a five-point Likert scale (strongly agree to strongly disagree) requiring participants to determine the extent to which they felt the event was informative, worked well, encouraged reflection on their personal views, and their likelihood of recommending the event to future cohorts of students. The final question was open-ended and free text, enquiring about how they felt the event could be improved. Data for the Likert scale questions were analysed using descriptive statistics, while free-text responses were analysed using principles of content analysis (Neuendorf, 2017).
Risk of harm to ‘Books’ was mitigated by identifying appropriate ratios of ‘Readers’ to ‘Books’, limiting the number of ‘Readings’ for any given ‘Book’, ensuring adequacy of breaks between ‘Readings’, as well as the need for a separate and confidential physical space for ‘Books’ to debrief during and after sessions. The extensive ‘Human Library’ training to be a ‘Book’ also includes continuous consent and the right to respectfully not answer a question that may breach boundaries or wellbeing. The role of the ‘Librarian’ was essential to help safeguard the ‘Books.’ For students, the course coordinator and programme lead were available for a debrief if required. Ethical approval to undertake this evaluation was granted by the MVLS Ethics Committee prior to data collection (Project Number: 200170142).
Results
Summary of attendee and questionnaire responses.

Questionnaire responses.
Although the free-text question requested suggestions for improvement, most responses provided reflections on how the event positively impacted on them:
‘I thoroughly enjoyed this event. I had never heard of this organisation before and I think that it is an incredible concept. This was easily one of my favorite class days. I can’t think of anything in particular that could’ve been done better.’ (2022–23
respondent)
‘The event was amazing. I didn’t even know such [a] thing existed. Thank you for exposing these things to me.’ (2023–24
respondent)
Across both cohorts, students highlighted that they would have liked to have had more time and opportunity to engage with all of the ‘Books’: ‘We were able to talk to only three people in the allocated time, it would have been better if opportunity was provided to have a conversation with all of the ‘Books’, just to have an insight about their stories and perception.’ (2022–23 respondent) ‘More time so we could listen to the other ‘Books’’ (2022–23 respondent)
‘I think a lot of us expected to be able to chat with all of the ‘Books’…If we had experienced all 8 that would have been fantastic, would happily have stayed for hours more’
(2023–24
respondent)
In the 2023–24 cohort only, students highlighted that they would like the ability to choose the ‘Books’ they ‘read’: ‘It would be great if we could choose the ‘Books’’ (2023–24 respondent).
‘I understand why they [the Librarians] chose the ‘Books’ for us beforehand, but I also wish that we could have chosen which ‘Books’ we wanted to read.’
(2023–24
respondent).
One student response summarised the intended impact of the event, commenting that the event ‘made me feel more confident to go with the flow of life and not judge myself, as well as not judging others’ (2023–24 respondent). This comment aligned with the principles embedded in the session of ‘unjudge someone’, including yourself.
Of note, one respondent in the 2022–23 cohort ‘strongly disagreed’ that the event made them reflect on their personal views. They reported that the format worked well and that they would recommend the event to the next cohort of students but stated that ‘It was a very interesting experience but I’m unsure in what way it connects to the module. That could be made clearer’ (2022–23 respondent).
Discussion
From the data gathered across both academic years, the vast majority of students reported that the ‘Human Library’ event was informative and made them reflect on their own personal views. The only negative comment was in regard to how the session connected to the module being studied. A key tenent of critical pedagogies and experiential learning is the deconstruction and reconstruction of knowledge, and the alignment of new experiences with theory and prior learning (Matthews, 2014; Varker and Small, 2021). Although an isolated comment, it is concerning that one student was unable to correlate the ‘Human Library’ event with the module Mental Health and Disability: International Law and Policy where there is a strong focus on the role of legislatory and policy reform in reducing discriminatory and harmful practices towards people living with mental illness. However, if one student was unable to connect the event with the module, it is likely that future students may have the same issue. Future directions could consider the integration of a student debrief session, a formative reflective summary of the experience, or integrating a discussion of the ‘Human Library’ event into the module itself.
Across both years, almost all students who responded to the questionnaire would recommend the event to other cohorts of students. Similar positive feedback has been reported in other ‘Human Library’ events held in higher education settings, for example, in Japan where 86.9% (n = 20) reported that they would recommend others to join the ‘Library’ (Kudo et al., 2011). This demonstrates the potential cross-cultural application of this approach in challenging stigma associated with mental health within higher education settings.
The social contact provided through the ‘Human Library’ event has been shown to be an effective tool to reduce discrimination and negative attitudes towards different stigmatised groups and improve MHL. It also acts to challenge the deficit-based framing of mental illness whereby the initial presentation of ‘Books’ by their reductive ‘Title’ are soon dismantled in dialogue. A ‘Human Library’ event in Hungary which focused on addressing prejudice towards the Roma and Lesbian, Gay, Bisexual and Transgender (LGBT) communities found that the ‘Human Library’ intervention reduced participants’ scores on multiple measures of prejudice (Orsoz et al., 2016). In Hong Kong, a ‘Human Library’ Reading event improved MHL and reduced stigma and preferred social distance among those attending the event compared to two other groups, one who attended a didactic education session and the other who had no intervention (Chung and Tse, 2022). This is consistent with evidence from a systematic review which reported that social contact interventions were most effective in improving attitudes and reducing desire for social distance in University and College students (Yamaguchi et al., 2013).
However, one study in Poland that explored the influence of a ‘Human Library’ event on attitudes towards LGBT, Muslim, and Roma communities had more mixed findings. A reduction in social distance was reported towards the Muslim communities only, with no difference reported in social distance towards Roma and transgender people (Groyecka et al., 2019).
In addition to improved MHL (Chung and Tse, 2022) and reduced prejudice (Orsoz et al., 2016), there is some evidence to suggest that the ‘Human Library’ intervention can improve students’ cultural awareness and sensitivity (Pope et al., 2023). In a study carried out in Australia, participation in the ‘Human Library’ improved cultural competence and awareness in a group of occupational therapy students and was reported as a cost-effective intervention (Pope et al., 2023). Furthermore, in a study in China, the ‘Human Library’ was found to facilitate social inclusion and promote recovery (Kwan, 2020).
The lack of choice regarding which ‘Books’ to engage with was highlighted by several students in the 2023–24 cohort. The authors are unsure of the reasons why students appeared to wish to choose what ‘Books’ to engage with. This presents interesting challenges and opportunities. It is possible that the students experienced emotional distress in response to the topics covered by the ‘Books’ selected for them and would, therefore, have liked more choice regarding the materials they engaged with. With that said, navigating the discomfort of engaging with potentially overwhelming topics such as abuse, and PTSD was transparently handled by the ‘Librarians’ and the ‘Books’ by asking for ‘consent to continue’ or if ‘Readers’ would prefer to ‘fast forward past the details’ when more graphic or emotional ‘chapters’ were triggered by questions.
The ‘Human Library’ argues from experience that choice-based conversations naturally feed the curious and open-minded who want to deepen understanding but may not reach those whose views may be more deeply held due to non-exposure or varied cultural or ideological differences. People have self-protective tendencies to ‘play safe' and choose a comfortable conversation topic. Thus, it is possible that some students might have preferred to choose ‘Books’ on topics they already felt an affinity to and that did not provoke a strong response. In order to create braver dialogues and reflect real life when encountering strangers - or indeed patients, classmates, and colleagues, whom we do not choose, the ‘Reading Hall’ format creates ‘a safe space for risk, not from it’. In this way, allocating ‘Books’ to ‘Readers’ aligns with experiential learning as it presents curated experiences that encourages participants to engage with potentially unfamiliar topics (Varker and Small, 2021). What is meant by this is a ‘safer braver space’ to risk questions, to risk the uncomfortable and awkward, to reveal ignorance or prior assumptions, without the fear of being wrong, shut down, shamed, or embarrassed. The ‘Human Library’ event space is designed to balance psychological safety with psychological bravery, as well as the engagement fears of both ‘Books’ and ‘Readers’ alike. The length of the conversations at 30 minutes is also optimum to reach a point of rapport and trust between all parties and yet finish leaving ‘Readers’ wanting more, not less, of each encounter. A common response is ‘I wanted more time’, despite the length of the event. This idea of ‘wanting more’ was reported by both cohorts who expressed a desire to speak to all the ‘Books.’
The ‘Human Library’ has an expanding range of formats online and in-person, some offering people the choice to choose the ‘Books’ they want to engage with. Both have their advantages and disadvantages. One option is an In-Person Book Cafe where students can choose topics that align with their learning interests for one-to-one conversations. Another is an ‘Human Library’ web-based App experience that allows groups of two to five ‘Readers’ to choose a 30 minute scheduled reading from the nearly 300 available ‘Book’ topics across 15 diverse categories, subject to availability. The Yale School of Nursing is currently trialling the latter among students (Human Library, 2023). Other collaborations include with University College Copenhagen’s Institute of Social Work where all future social workers become ‘Readers’ of the ‘Human Library’ (Human Library, 2018) and with Human Resources (HR) in Ontario Health (Human Library, 2024).
Our case study exploring the role of a ‘Human Library’ event to raise awareness of and sensitivity to stigma and discrimination in a cohort of postgraduate masters students has several limitations. Firstly, attendance at the session and completion of the online questionnaire was not compulsory and thus the findings are only reflective of a small proportion of the total class. It was also not clear why the response rate to the questionnaire was much lower in the 2023–24 cohort compared to the 2022–23 cohort. Additionally, it may be the case that students who chose not to attend the session may have benefitted most from this type of event. Evaluation methods were pragmatic and, as such, only limited feedback was collected; the analysis presented here reflects this. A more detailed in-depth evaluation of the event using objective measures of MHL and prejudice will be planned for future iterations of the course. Additionally, we were unable to determine if there were any lasting impacts on stigma for the student attendees. Longer-term evaluations of the impact of the ‘Human Library’ event are challenging due to the one-year nature of the masters degree. Finally, consideration as to how best to adapt this event for our smaller online cohort of students is needed, to ensure that they are able to access this important learning opportunity. Drawing from lessons from the University of Glasgow medical student undergraduates who engage in this learning opportunity exclusively online with much larger numbers of students will be helpful. However, ‘Human Library’ representatives advise that ‘Readers’ typically prefer in-person over online after experiencing both but find either experience memorable and impactful.
Conclusion
Feedback across two iterations of the ‘Human Library’ event indicates that the sessions are informative and encourage self-reflection. Given this positive feedback, the GMH team have taken the decision to embed the ‘Human Library’ event into the Mental Health and Disability: International Law and Policy course for all future cohorts of on-campus students. Based on feedback, students will be supported with drawing the links between the event and the wider learning objectives of the course, something we would recommend others considering this approach to embed during development. The ‘Human Library’ event offers our students authentic learning opportunities, supporting their understanding within the course of the environmental challenges and stigma individuals face. The event also supports programmatic level skill transferability, addressing wider learning outcomes related to social and cultural factors in the manifestation of mental health difficulties to reflect on appropriate strategies for developing, delivering and improving interventions.
Footnotes
Acknowledgements
We would like to thank the ‘Human Library’ ‘Books’, and ‘Librarians’ who delivered the sessions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: With initial funding from the MVLS College Equality, Diversity and Inclusion Committee (CEIDC), the first learning event facilitated by the Human Library was organised for the 2022/23 cohort of students.
Correction (March 2025):
Article updated to correct the Special issue title.
Ethical statement
Data availability statement
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.