
Abstract
Background
Turkish-, Moroccan-, and potentially Syrian-Dutch women in the Netherlands are disproportionately affected by cervical cancer (CC), yet participate less in CC screening and Human papilloma virus (HPV) vaccination program compared to other ethnic minorities and native Dutch women. Existing informational materials insufficiently address their practical, emotional, cultural, and religious concerns. Our aim was to investigate the information seeking behavior and the information needs regarding CC screening and HPV vaccination among Turkish-, Moroccan-, and Syrian-Dutch women.
Methods
Semi-structured interviews were held with 51 Turkish-, Moroccan-, and Syrian-Dutch women (n = 20, n = 19, and n = 12, respectively). The interview guide was based on the Health Belief Model, the Reasoned Action Approach, and Betancourt’s Model of Culture and Behavior. Interviews were transcribed verbatim and thematically analyzed.
Findings
This study identified language barriers and cultural factors related to virginity, fertility, and sexual activity as key influences on decision-making. Most participants reported not actively seeking information and expressed a need for tailored content delivered through trusted and recognizable key community figures and accessible channels, both online and offline. Comparison with CC prevention measures in their countries of origin may facilitate information processing and understanding.
Discussion
These findings underscore the importance of culturally sensitive materials and outreach to support informed decision-making and improve participation in cervical cancer prevention. These results provided concrete guidance for the development of targeted policies and communication strategies that better address the specific needs and barriers regarding CC prevention faced by Turkish-, Moroccan-, and Syrian-Dutch women.
Keywords
Introduction
In 2020, cervical cancer (CC) is the fourth most frequently diagnosed cancer and the fourth leading cause of cancer deaths in women globally. 1 The primary cause of CC is the Human Papilloma Virus (HPV). 2 HPV types 16 and 18 are responsible for roughly 70% of all CC cases worldwide. These are caused by a long-term (10-15 years) infection of HPV. More than 80% of sexually active individuals will be infected with HPV at least once by the age of 45 years. 2 Each year, approximately 800 women in the Netherlands are diagnosed with CC, of whom about 200 die as a result of the disease. 3 To reduce these numbers, the Dutch government introduced two prevention programs: CC screening and HPV vaccination. The CC screening program was implemented in 1996 and is aimed at women between 30 and 60 years old. 1 In 2010, the HPV vaccination was introduced in the Netherlands, initially targeting only 13-year-old girls. However, as of 2022, the target population has been expanded to include both girls and boys, and the age of invitation has been lowered from 13 to 10 years. 2 Although participating in these programs is free of charge, participation rates remains suboptimal, particularly among women with a migration background.4,5
Compared to native Dutch women, Turkish- and Moroccan-Dutch women, who account for the two largest immigrant population groups in the Netherlands, participate less in CC screening (79% vs 64% and 53%, respectively).5,6 This is especially worrisome, as more than half of the diagnosed CC cases occur in women who have not participated in CC screening before.7,8 A recent study in Scotland showed that no cases of invasive cancer were recorded in 25-year old women, who are vaccinated at 12 or 13 years of age, irrespective of the number of doses. 9 This highlights the effectiveness of HPV vaccination in children. However, HPV vaccination uptake is also found to be lower among Turkish- and Moroccan-Dutch immigrants, compared to those without a migration background and compared to those with another immigration background. 3 A study conducted in 2017 found that HPV vaccination uptake rates among Turkish- and Moroccan-Dutch girls with one parent being born in Turkey or Morocco were 26.1% and 18.7%, respectively. Among Turkish- and Moroccan-Dutch girls with both parents being born in their country of origin, the uptake was even lower, namely 20.5% and 16.5%, respectively. This HPV vaccination uptake rates are considerably lower compared to native Dutch girls (49.4%). 3
Multiple studies investigated the barriers and facilitators for participation in CC screening and HPV vaccination uptake. The most important reason for non-participation in these programs was a lack of awareness and knowledge. For example, a qualitative study among Turkish- and Moroccan-Dutch women indicated little knowledge on how to access the available information materials. 10 Another study among Syrian refugees in Greece also showed that there is limited knowledge on CC risk factors and symptoms among this population. 11 A longitudinal study assessed the determinants of HPV vaccination intention and uptake among parents/guardians from different ethnic backgrounds in Amsterdam, the Netherlands. 6 Among the Middle Eastern and North African (MENA) group, which includes Turkish-, and Moroccan-Dutch women, risk perception when deciding not to vaccinate (ß = 0.11; 95% CI = 0.01,0.21), and descriptive norms (ß = 0.12; 95% CI = 0.02,0.23) were identified as significant determinants of HPV vaccination intention. Descriptive norms in this context refer to individuals’ beliefs and expectations regarding the vaccination behaviors of others within their own community. 12
For CC screening and HPV vaccination, informed decision-making for participation is important, since both programs come with benefits and disadvantages. In this context, informed decision-making allows individuals to decide using the maximum available information and rationally weighing all aspects (both pros and cons) involved. To improve immigrant women’s informed decision-making, information materials regarding these programs should be tailored to the information needs and preferences of these women. In the Netherlands, the current information materials are mainly factual medical oriented, whereas a previous study indicated that Turkish- and Moroccan-Dutch women have a need for more information about the practical, emotional, cultural, and religious factors of CC screening. 10 A literature review indicated that the information needs of Turkish- and Moroccan-Dutch women regarding HPV vaccination and CC screening are similar 13 . No studies have been conducted among Syrian-Dutch women, which is a growing immigrant population group in the Netherlands. Since they share similar cultural and religious norms as Turkish- and Moroccan-Dutch women, it would be of great value to investigate whether they have similar information needs regarding CC screening and HPV vaccination or not. If their needs and preferences regarding information materials for CC prevention programs are similar, future interventions could use similar communication strategies. Therefore, this study aims to explore the current information seeking behavior and the information needs and preferences regarding CC screening and HPV vaccination among Turkish-, Moroccan-, and Syrian-Dutch women.
Methods
Study Design
Between April to July 2023, 51 semi-structured interviews were conducted with Turkish-, Moroccan-, and Syrian-Dutch women. The aim was to gain insight into their current information seeking behavior and information needs regarding their (intended) participation or non-participation in CC screening and HPV vaccination uptake for their children. The reporting of this study is in adherence to the Conciliated criteria for Reporting Qualitative research (COREQ) checklist (see Appendix 1). 14
Study Population and Sampling
The study population consisted of first- and second-generation Turkish-, Moroccan-, and Syrian-Dutch immigrant women in the Netherlands. Following the definition of Statistics Netherlands, 15 first-generation immigrant women are defined as women born in Turkey, Morocco, or Syria, and are currently living in the Netherlands. Second-generation immigrant women are defined as born and currently living in the Netherlands, with at least one parent being born in Turkey, Morocco, or Syria. Inclusion criteria for these women were being aged 30-60 years old, and/or having a daughter aged 9-26 years old. These criteria were chosen because these women are eligible to participate in the CC screening program. Additionally, their daughters have been invited for the HPV vaccination. Participants were recruited using snowball sampling via flyers on social media platforms (Facebook, Instagram, and LinkedIn). We also contacted community centers, mosques, social and professional networks of the interviewers, and Turkish- and Moroccan-Dutch women who participated in a previous research project via email and telephone. 10 Potential interviewees meeting the inclusion criteria were invited and informed about the study via an (digital) information letter. Recruitment for the interviews went on until data saturation (i.e. no new (sub)themes being generated during the analysis of the latest interview) was reached for all three immigrant groups (Turkish-, Moroccan-, and Syrian-Dutch women), and the sample being diverse in terms of the following socio-demographic characteristics: first- or second-generation, migration background (Turkish, Moroccan, Syrian), age, educational level, and geographical orientation in the Netherlands.
Data Collection
Prior to the interviews, participants were asked to fill out a short questionnaire regarding several socio-demographic characteristics (age, digits of the postal code (a proxy for geographical distribution), marital status, educational level, spoken languages, self-reported proficiency in Dutch language (speaking and reading), country of birth, year of migration (if applicable), previous participation in CC screening, their own HPV vaccination status, number of children, children’s age, and children’s HPV vaccination status). This was to monitor whether we recruited a diverse sample of individuals. The interviews were conducted by bilingual female interviewers (TV, NHS, and NBA), in Dutch, English, Moroccan-Berber, Arabic, or Turkish, as preferred by the participants. This questionnaire also included the informed consent form. On average, the interviews lasted approximately 1 hour and took place face-to-face or with video conferencing via MS Teams (as preferred by the participants). Participants received a gift voucher (€18,- value) as a token of our appreciation for participating in this study.
Pre-defined Interview guide
All interviewers used a pre-defined interview guide, which was based on the Health Belief Model (HBM), the Reasoned Action Approach (RAA), and the Betancourt’s Model of Culture and Behavior (BMCB) (see Appendix 2). These models contain constructs relevant to a wide variety of health behaviors, 16 and have already been successfully applied to the context of CC (and Hepatitis B) screening and HPV vaccination for the specific target population in this study at hand.10,17–19 Questions were formulated to explore the participants’ perspectives regarding the current information materials on CC screening and HPV vaccination, their current information seeking behavior, and their information needs and preferences. During the interview, we showed the participants the current information materials for CC screening and HPV vaccination. These materials consisted of an information letter and a brochure. We also showed the cultural-sensitive video regarding CC screening developed in a previous project among. 20
The interview guide consisted of four parts. Firstly, opening questions regarding CC were asked, concerning knowledge, awareness, and attitude about CC. Secondly, we asked questions about their perceptions, decision-making, information seeking behavior, and their information needs regarding CC screening. Thereafter, these questions were repeated for HPV vaccination for their daughters. If participants indicated also having a son eligible for the vaccination, we also asked them whether they made other decisions or not regarding HPV vaccination for their sons. In the last part of the interview, we asked questions about their preferences on how they want to receive the information (e.g. combined information for CC screening and HPV vaccination, digital, on paper, videos etc.). The interview guide was tested in four (video) pilot-interviews. As a result, minor adjustments to phrasing and order of questions were made. Not all questions formulated in the interview guide were discussed with every participant. The questions addressed depended on the responses provided by each participant. Follow-up questions were only posed when relevant within the context of the conversation.
Data Analysis
The interviews were audio-recorded and directly translated into Dutch during transcription. Translation into Dutch was performed by the bilingual female interviewers (NHS and NBA), who have a sufficient proficiency in both languages. This was done to ensure that the entire analysis team was able to participate in the coding process. The transcripts were supplemented with eventual field notes made by the interviewer. Interviews were analyzed inductively using the qualitative software program MAXQDA v.2022.05. A thematic analysis was conducted by three of the interviewers (TV, NHS, and NBA), who independently performed open coding for each of the three immigrant groups. 21 One third of the total amount of interviews were double coded by two researchers (TV and NH). Subsequently subthemes and themes were generated through systemic comparison of the coded text (i.e. axial and selective coding). After each step, interpretation of the subthemes and themes were discussed among the interviewers until consensus was reached. Hereby, extra attention was paid on differences in themes among the three immigrant groups. Data saturation was defined at the point that no new themes and subthemes were generated in each of the three immigrant groups.
Ethical Considerations
Ethical clearance was obtained from the Medical Ethics Review Committee of University Medical Centre Utrecht (23-090/DB). Informed consent for participation and publication was obtained from all individual participants included in the study. The Committee confirmed that the Medical Research Involving Human Subjects Act (WMO) does not apply to this study. Participation was completely voluntary, and participants were allowed to withdraw from the study at any moment. Confidentiality was maintained by removing all reducible personal data from the transcripts during processing and storage.
Results
Socio-Demographics
Characteristics of the Participants (n = 51).
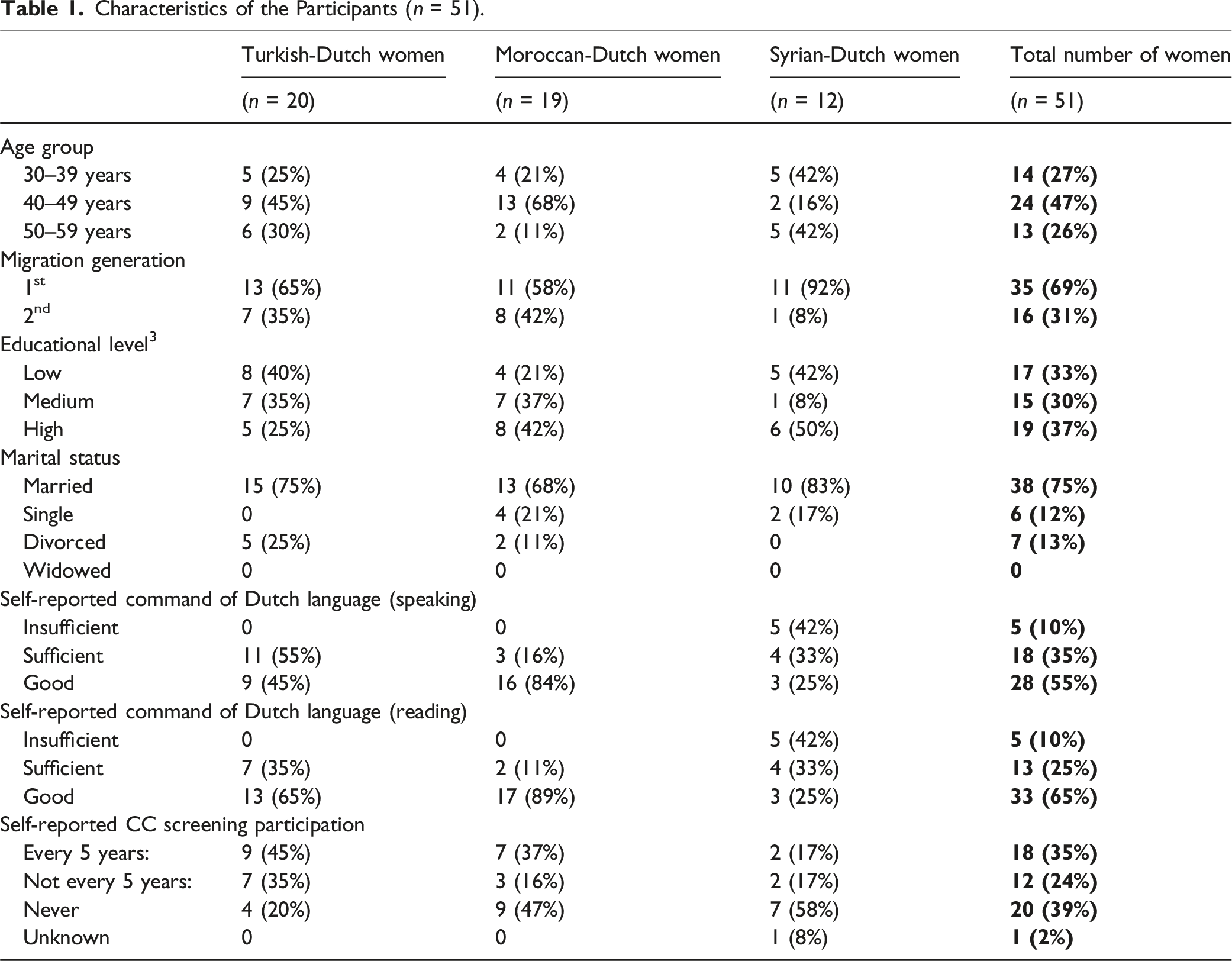
Most of the participants were aged 40 to 49 years (47%). In terms of geographical distribution, we included women living in different areas of the Netherlands, with a majority residing near big cities such as Amsterdam, Utrecht, or The Hague. Most participants self-reported to have sufficient to good command of the Dutch language in speaking and reading. Most of the Turkish- and Moroccan-Dutch women in this study participated in CC screening at least once before (80% for the Turkish-Dutch women and 53% for the Moroccan-Dutch women). However, only 7 out of the 12 Syrian-Dutch women (58%) reported to have never participated in CC screening. Five of them were between 30 and 39 years old, the other two were between 40 and 49 years old.
Self-Reported HPV Vaccination Uptake for Their Daughters and Sons.
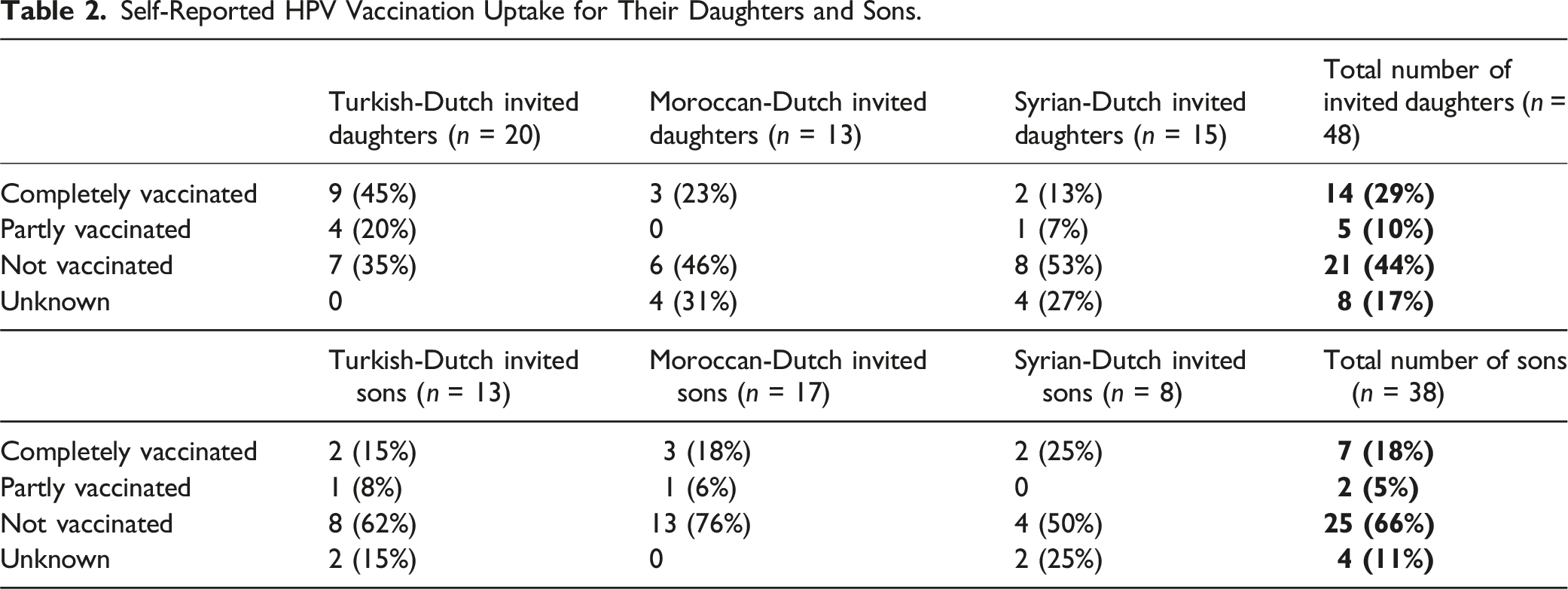
In total, 33% of the participants’ children was (completely/partly) vaccinated against HPV. For the daughters only, this percentage was 39% and for the sons only this was 23%. Among the Turkish-Dutch participants, most of their daughters had been vaccinated against HPV, namely 65% (completely/partly). For the Moroccan- and Syrian-Dutch participants, this percentage was found to be lower, namely 23% and 20%, respectively (completely/partly).
Thematic Analysis
The thematic analysis resulted in five themes, which were identical and representative for all three immigrant groups. Therefore, these results indicated that the needs and preferences for information materials regarding CC prevention programs are similar for Turkish-, Moroccan-, and Syrian-Dutch. We identified the following five themes: 1. Diverse attitudes towards preventive care in general, CC prevention programs, and its current information materials; 2. Current information seeking behavior and information sources for CC prevention programs; 3. Lack of awareness and knowledge regarding CC and its prevention programs; 4. Barriers and facilitators regarding obtaining, processing, and understanding information about CC and its prevention programs; 5. Information needs and preferences regarding CC and its prevention programs. In the following section, the main findings of these themes are described.
Diverse Attitudes Towards Preventive Care in General, CC Prevention Programs, and Its Current Information Materials
Overall, participants in all three immigrant groups had a positive attitude towards preventive care in general and the availability of CC screening. However, the attitude towards the HPV vaccination was mixed within all three immigrant groups. For example, participants indicated to be more likely to participate in CC screening rather than vaccinating their children against HPV. I do prefer prevention, but I am somewhat against those vaccinations. Because I do not know what the child is ingesting, and I am like: just let the body clean it up on its own. If there is something, it will be alright, hopefully. I am mainly against vaccinations. Especially after Covid, I also decided no more vaccinations, the body will solve it itself, hopefully. – Turkish participant, 40-49 y/o
Some participants indicated skepticism towards HPV vaccination. This was marked by an overall mistrust toward the government. They [referring to the government] are not transparent, they are not fair. – Moroccan participant, 40-49 y/o
In general, most participants were positive regarding the current information materials for CC screening and the HPV vaccination. These information materials were considered as comprehensive, understandable, and accessible. Some indicated the information materials as confusing. They attributed this to the elaborative texts and small font sizes that hindered the readability. The availability of translations and videos online were particularly appreciated by the participants, as they made the information easier to understand. However, some participants indicated that the online materials were not easy to access for individuals with a lack of digital skills (mostly among first-generation immigrants).
Current Information Seeking Behavior and Information Sources for CC Prevention Programs
Most participants, generally first-generation immigrants, mentioned that they have not actively sought for information about CC screening and/or HPV vaccination. This was consistent across all three immigrant groups, with avoidance and passiveness given as reasons for not fully reading the information. Not having any symptoms was also mentioned multiple times as a reason for not (fully) reading the information materials. We are too passive to do that. We are very good in social media, but not in seeking for the right things. – Moroccan participant, 40-49 y/o
Participants were also asked about their current sources of information. General practitioners (GPs) and the internet were identified as the primary sources of information regarding CC screening and HPV vaccination. However, participants acknowledged the presence of misinformation online. A few participants indicated that they were familiar with the Culturally Sensitive Educational Videos (CSEVs) developed in a prior project. 20 They came across these videos while seeking information on the website of the RIVM or had been informed about this by others. Women indicated that these videos supported their decision-making process and helped to overcome the language barrier. During the interviews, the videos were also introduced to participants who were not previously familiar with them. These women reported similar benefits when using these videos as a source of information.
Lack of Awareness and Knowledge regarding CC and Its Prevention Programs
Participants had a lack of knowledge regarding the cause of the disease and its related symptoms. For example, some participants identified food as a main cause for developing cancer. They [referring to the government] have to do something about the food. The food is full of carcinogenic substances. – Turkish participant, 40-49 y/o
Most participants had heard of the CC screening and were familiar with its steps. However, a few, mainly first-generation immigrant women, were not familiar with the CC screening program. Thereby, the self-sampling kit was new for many of them as well. Furthermore, the purpose of the screening was not always clear. Many participants knew that the HPV vaccination is for primary protection against an infection with certain types of HPV. However, not everyone knew that, in the Netherlands, HPV vaccination is also available for boys since 2022. But how does it work with boys? Why are only girls invited for the HPV vaccination? – Syrian participant, 40-49 y/o
Barriers and Facilitators for Obtaining, Processing, and Understanding Information about CC and Its Prevention Programs
Health Literacy
Mainly first-generation immigrant women mentioned the language barrier as the biggest barrier for obtaining, processing, and understanding the information. Participants also spoke about a generation gap; first-generation women experienced many difficulties when it comes to the accessibility of digital information materials. This resulted from a lack of digital skills (e.g. the use of QR codes), and limiting them to receive all the information available. Audiovisual information was considered as highly beneficial, but should also be made easier to access for individuals with limited digital skills. Participants in this study indicated to prefer a phone call from their GP, rather than receiving written information. Simultaneously, participants also mentioned that this approach will facilitate the opportunity to address initial inquiries with a GP assistant. Multiple Turkish-, Moroccan-, and Syrian-Dutch women indicated receiving information from individuals with a similar cultural or religious background as an additional benefit. Such individuals are perceived to have a better understanding of their perspectives, due to shared norms and values concerning virginity, fertility, and sexual activity. ‘They [referring to first-generation immigrant women] think like: ‘you have a similar background, you have a similar culture, so you will understand me better and might be willing to do more for me as well.’ – Moroccan participant, 30-39 y/o
Fear for Seeking Information
Participants also mentioned fear as a barrier for seeking information, because it would evoke negative thoughts. That is why many individuals indicated that they did not want to talk or think about CC, and everything that comes with it, in their daily life. This was illustrated by the following quote: This topic in particular scares me a lot, which is why I would generally not go into the details. – Syrian participant, 50-60 y/o
Country of Origin and Islam as Their Religion
Many Turkish participants reported that they still go to Turkey regularly for general health checkups, which also include CC screening. Some participants cited this as a reason for non-participation in CC screening in the Netherlands. Consequently, several participants suggested that providing a comparison of the available preventive measures in their country of origin could facilitate the processing and understanding of information. This suggestion was attributed to their strong attachment to their country of origin. If you compare it with the possibilities in their country of origin, sometimes they are more open to it, this is especially true for the elderly [referring to first-generation immigrants]. – Turkish participant, 40-49 y/o
In general, according to the Islam, it is considered very important, especially for a woman, to take good care of your health. Since the Islam plays an important role in these population groups, many participants also indicated that this could be seen as a facilitator for seeking information regarding CC prevention programs. The Turkish community is largely Muslim. It [referring to the Islamic religion] actually supports taking care for yourself and for your body. It [referring to the body] is given by Allah, you are the caretaker and you must take good care of your body. So, the Islam is actually encouraging rather than hindering. – Turkish participant, 40-49 y/o
Social Network
Participants indicated that Turkish-, Moroccan-, and Syrian-Dutch women highly rely on their social network when it comes to receiving information adequately. Since some (mostly first-generation immigrant) women do not have sufficient proficiency in the Dutch language, they are highly dependent on information obtained from others. Accordingly, many participants identified their social network as a facilitator for obtaining, processing and understanding the information. They indicated that this support was particularly relevant for translating information, as well as for inquiring about the decisions made so by their friends and family members. You ask your social network. You ask those around you: did you also receive that letter? Have you already done this? – Moroccan participant, 40-49 y/o
Although most participants indicated that the topic can be openly discussed, they also mentioned that this is usually done very superficially. As they explain, people only say that they have cancer, but do not get into detail about which form of cancer they have. Participants indicated to experience a barrier to discuss their decisions for (non) participation due to varying reactions within their social network, both for and against participation in CC screening and HPV vaccination. Participants noted that participation in CC screening could be perceived as an indication that one considers oneself at risk for developing CC. Consequently, others might infer, for example, that you are not monogamous. Conversely, participants also indicated that non-participation in CC screening or HPV vaccination could be interpreted by others as a lack of attention to one’s health.
Information Needs and preferences regarding CC and Its Prevention Programs
Most of the participants indicated that there is still a need for medical information, such as the cause and severity of the disease, and the related symptoms. Some participants also expressed a need for information on the available options to participate in CC screening, such as the self-sampling kit and the possibility to ask for a female health practitioner. These options were described as lowering their barriers for participation. Also, more specified information on the practical steps of CC screening was considered helpful. Women also indicated a need for more relevant information that is adjusted to their cultural and religious norms and values, for example regarding virginity, fertility, and sexual activity. Specific examples of information needs mentioned by participants were: more information on how to request the self-test, whether it is useful or not to get vaccinated against HPV at an older age (and how does this impact your fertility?), and if you should participate in CC screening if you are not sexually active yet. I think it is important that people who are not sexually active also participate. I am not married myself and as a Muslim you are not sexually active before marriage, and I adhere to that. The CC screening program actually ignores that. The practical aspect of a smear test for someone who has never been sexually active also raises concerns. I think there is a large group of women who are over 30, not married, and Muslim, who must deal with this. – Moroccan participant, 30-39 y/o
Informational Meetings
Participants mentioned organizing informational meetings as their most favorable source of information. This was indicated by women across all three immigrant groups and varying age categories. Participants stated that it facilitates women to pose questions and start the conversation. Schools and mosques were most frequently mentioned as potential locations for such meetings. Besides informational meetings, audiovisual information materials were also mentioned as a preferable source of information. Stories of experts-by-experiences who had undergone CC (screening) and/or HPV vaccination should also be included in the information materials. Participants indicated that it is recommended to collaborate with key community figures or other relatives from the community while organizing informational meetings and developing audiovisual information materials. To tailor the information materials to the needs of Moroccan-Dutch women, you should collaborate with women who have experienced it [referring to CC] themselves and collaborate with a gynecologist or a GP. – Moroccan participant, 40-49 y/o
GP as Main Source of Information
Participants indicated that they would prefer to receive information regarding both CC screening and the HPV vaccination from their GP. The main reason for this was that the GP knows individuals’ personal situation and it is therefore easier to ask questions. The GP is the most important and reliable source of information. He is the closest to his patients. – Syrian participant, 50-60 y/o
Integrated Information
The CC screening and the HPV vaccination have similar goals, namely lowering CC-related morbidity and mortality. However, integrating the information of both programs is not favored according to the immigrant women included in this study. The main reason for this was that the programs have different target populations; whereas the HPV vaccination is aimed 9/10 years old children, CC screening is for women aged 30 to 60 years old. Participants indicated that integrated information would be confusing and overwhelming. I would be confused. I would doubt whether the information is about the screening or the vaccination. I would recommend keeping it separated, so that everyone knows to which program it belongs, and for whom it is intended. – Moroccan participant, 50-60 y/o
Practical Preferences
Besides suggestions for the information materials regarding CC screening and HPV vaccination, participants also shared their view on practical applications of these programs. For example, some participants suggested that CC screening should begin at an earlier age than 30, as sexual activity is now commencing at younger ages. Another recommendation was regarding home- and/or community visits, which was suggested multiple times for both conducting the CC screening and the HPV vaccination. This could lower the barrier for women who are hesitating or not able to go to their GP and/or the vaccination location. It would be so much better if someone can visit me at home to conduct the screening. This would be very helpful, especially for women who do not have a car. – Syrian participant, 50-60 y/o
Discussion
Main Findings
This study explored the current information seeking behavior and information needs of Turkish-, Moroccan-, and Syrian-Dutch women in relation to informed decision-making regarding participation in CC screening and HPV vaccination uptake. The development of the interview guide was informed by the HBM, RAA, and BMCB, ensuring that questions addressed individual health beliefs, behavioral intentions, and relevant cultural norms and values. Findings derived from HBM-based questions revealed that many women expressed skepticism toward (HPV) vaccination. Participants also reported low perceived susceptibility to CC and expected limited benefits of participating in CC screening, while concerns regarding pain, embarrassment, and lack of trust in information sources emerged as significant perceived barriers. Following the RAA, the study demonstrated negative attitudes towards (HPV) vaccinations, which could lead to a lower intention for HPV vaccination uptake. By integrating BMCB, the interviews further highlighted how cultural values, particularly regarding virginity, fertility, and sexuality, influence both risk perception and trust in existing information. As a result, participants expressed a clear need for more targeted information that explicitly incorporates these cultural and religious norms and values. Furthermore, the opportunity to compare CC prevention strategies with those implemented in their countries of origin was perceived as a facilitator for information processing and understanding among immigrant women.
These findings also highlight the importance of recognizing the substantial cultural and religious diversity among Turkish-, Moroccan-, and Syrian-Dutch women. For instance, norms and values related to virginity, fertility, and sexuality varied widely within and between these groups. Such diversity may consequently also influence individual’s risk perceptions, trust in effectiveness and safety of the prevention programs, and informed decision-making regarding CC screening and HPV vaccination uptake. Therefore, addressing these nuances through culturally sensitive and contextually relevant communication strategies is essential to improve access to information regarding CC screening and HPV vaccination.
Comparison with Previous Literature
A recent study conducted among Syrian refugee women in Turkey (n = 409) investigated CC awareness and the influence of socio-cultural factors on healthcare utilization. 22 Among the participants, 307 (75%) reported never having undergone CC screening. Reasons for non-participation in CC screening included embarrassment or hesitancy to visit a doctor, concerns about pain, skepticism regarding the benefits of the test, and difficulties in accessing health facilities. These findings are in line with a previous study among Turkish-, and Moroccan-Dutch women in the Netherlands, which identified similar barriers and facilitators for participation in CC screening. 10 Notably, the most frequently reported reason for non-participation in CC screening among Syrian refugee women in Turkey was a low perceived risk of developing CC, as indicated by 30% of those who had never been screened. 22 Furthermore, 24.4% of non-participating women attributed this to a lack of information regarding CC screening. Especially, these latter two reasons closely align with the findings of the present study, in which lack of awareness and knowledge regarding CC and its prevention programs emerged as a theme (see Theme 3 in Results). Participants in a qualitative interview study among Syrian migrant women in Turkey also indicated a lack of knowledge regarding the CC (and breast) screening program. 23 The findings of these studies also align with prior research emphasizing that future intervention studies for CC prevention should prioritize cultural appropriateness and address the health behaviors and information needs of immigrant women.10,24,25
A meta-analysis of RAA-based studies demonstrated that several aspects of attitude are moderately to strongly associated with individuals’ intentions toward specific behaviors such as participation in health prevention programs (such as screening and vaccination). 26 In our study, this was reflected by the fact that women showed a more positive attitude towards CC screening rather than towards the HPV vaccination. Therefore, it could be said that women were more likely to participate in CC screening rather than to have their children vaccinated against HPV. We also found that participants showed more negative attitudes towards vaccines in general. These attitudes were shaped by skepticism toward the government and pharmaceutical industry, who were responsible for the supply of other vaccines as well. Participants often linked this skepticism to the COVID-19 pandemic. A recent study by Hajissa et al. also indicated hesitancy for COVID-19 vaccination among immigrants, refugees, and foreign workers due to a lack of trust in both the vaccine and the government. 27 The lack of trust regarding the HPV vaccination may be partly due to the COVID-pandemic, but also pre-COVID studies identified similar barriers for HPV vaccination.28,29
Previous research already indicated that Turkish- and Moroccan-Dutch women have a need for information about the cultural, religious, practical, and emotional aspects of CC screening, besides the factual medical information. 10 For example, they indicated that shame and taboo play an important role in this population group. This current study provided more in-depth insights on how to apply these aspects to better reach and inform Turkish-, Moroccan-, and Syrian-Dutch women for CC prevention programs. When it comes to receiving the information, participants indicated to highly rely on their social network. This is in line with a previous study that indicated that second-generation immigrants often act as translators for their family members who have little to no command of the local language. 30 For the content of the information, participants of this current study further specified the information needs regarding cultural, religious, practical, and emotional aspects of CC screening. Namely, they expressed a need for more information on the relevance of participation in CC screening if you are a virgin, what the impact is on your fertility, to what extent the result of CC screening is related to your sexual activity. Furthermore, referring to the religious responsibility to take good care of their health could work as a facilitator to support information seeking behavior. Accordingly, comparing CC prevention measures with those in their countries of origin may also enhance the processing and understanding of information. Therefore, participants suggested to address these aspects during informational meetings at mosques and community centers and develop audiovisual materials that are relevant and recognizable for this specific target population (e.g. videos).
Furthermore, it is important to realize that the highest influx of Syrian immigrants started in 2015, due to the ongoing war. 31 The influx of Turkish- and Moroccan immigrants in the Netherlands emerged longer ago, namely around the ‘60s and ‘70s. 32 Therefore, in general, Turkish- and Moroccan-Dutch women are more familiar with the Dutch healthcare system (including CC screening and HPV vaccination) than Syrian-Dutch women. Relatively, we included more first-generation Syrian-Dutch women with a lower proficiency of the Dutch language. However, this study indicated that the information needs of these Syrian-Dutch women are in line with those of the Turkish- and Moroccan-Dutch women included in this study. Therefore, interventions addressing these needs could be targeted at all three immigrant populations.
Recommendations for Practice and Future Research
Besides factual medical information, we identified relevant cultural and religious norms and values regarding virginity, fertility, and sexual activity that are not discussed in the currently available information materials for CC prevention. Therefore, newly developed information materials should incorporate the relevance of participation in CC screening if you are a virgin, what the impact is on your fertility, and what participation and the result of CC screening is related to your sexual activity. It is also recommended that information materials include a comparison of the CC prevention measures from immigrants’ countries of origin. Furthermore, we should make good use of immigrants’ trusted and preferred sources of information. During the interviews, many women emphasized their GP as most reliable source of information. This was especially the case for CC screening, as GPs and GP assistants are the ones who carry out the screening procedure (except for self-sampling).
However, participants also indicated their GP as a highly valued and trusted source of information for HPV vaccination. Previous studies indicated that healthcare providers’ recommendations have a positive effect on HPV vaccination uptake among immigrant women.33,34 This is also in line with the findings described in a meeting rapport of the HPV Prevention and Control Board. 35 Experts from this international board recommended to also stimulate healthcare professionals to get vaccinated against HPV themselves. Since they are often seen as trusted role models for their patients, refusal of HPV vaccination by healthcare professionals may lead to lower HPV vaccination uptake in the general population. Therefore, the board suggested to increase education, emphasize the norms of HPV vaccination, and make it easier for healthcare professionals to get the HPV vaccination. 35
Multiple studies also investigated the role of GPs in cancer screening.36,37 In these studies, GPs expressed a willingness to empower their patients in cancer screening, but also have to deal with insufficient resources to do this. Besides GP’s, collaboration with experts-by-experience and key community figures was also frequently mentioned for both CC screening and HPV vaccination. An intervention study applied this in a randomized controlled trial among women who have recently screened for CC. 38 The intervention consisted of seven workshops in which women discussed their fears for CC and decision-making for screening, but also paid attention to healthy living in general and how to start conversations on sensitive topics like this. The intervention was found to be highly effective in increasing the CC screening uptake among social network members. In the intervention group, 67% of the participants indicated to be likely to participate in CC screening, compared to only 16% of the control group. 38
Future Steps
Besides improving the role of GPs in CC screening and HPV vaccination, it was also recommended to collaborate with key community figures in developing and implementing interventions. Based on the results of this study, we have investigated the role of different stakeholders (e.g. key community figures, healthcare professionals, communication experts, policy makers, and program managers) in supporting informed decision-making regarding participation in CC screening and HPV vaccination among immigrant women. Therefore, we conducted multiple focus group discussions with several stakeholders (key community figures, healthcare professionals, communication experts, policy makers, and program managers). The results and analysis of this study will follow in due course and will also be incorporated in the development of our future intervention studies; a training program for key community figures in providing informational meetings (mainly targeted at the first generation), and audiovisual materials for social media including a bicultural GP and experts-by-experience from the target population (mainly targeted at the second generation). Both interventions will focus on cultural, religious, practical, and emotional aspects regarding virginity, fertility, and sexual activity described in this study that affect decision-making for participation in CC screening, next to the factual medical information which is also still needed. The audiovisual materials will be evaluated in a mixed-method study.
Strengths and Limitations
One of the strengths of this study was that we succeeded in including a diverse sample of participants, in terms of migration background, age, and educational level. Another strength of this study was that all interviews were conducted at a location preferred by the participants. This could be either at their homes, community centers, or online via MS Teams. This provided comfortable settings for the participants. Another notable strength of this study is its theory-informed design, as the interview guide was based on a combination of three complementary theoretical models, the HBM, the RAA, and the BMCB. This enabled a more comprehensive and systematic exploration of the information seeking behavior and the relevant information needs.
Participants in this study reported difficulty recalling how they previously obtained information and made decisions regarding CC prevention. This represents a potential limitation of the study, as questions concerning prior decision-making processes and information seeking behavior may be subject to recall bias and self-reporting bias. Another point is that most participants chose to participate in online interviews, which may have resulted in less natural conversations compared to face-to-face interviews. However this mode of data collection was based on the participants’ own preferences. To enable coding for the entire analyze-team, all transcripts were translated into Dutch. This could have created a limitation, since nuances in meaning and context could have been lost or altered during the translation. However, interviews being conducted by bilingual researchers (TV, NHS, and, NBA), enabled participants to speak in their preferred language, which facilitated them to speak more fluently about their experiences and emotions. Furthermore, this study exclusively included women who provided informed consent, which potentially introduced a context-specific selection bias,. Nevertheless, we also observed the presence of both positive and negative attitudes toward CC screening and/or HPV vaccination. The fact that this study is led by the Dutch National Institute for Public Health and Environment (RIVM), could have contributed to a response bias, potentially leading to more socially desirable answers. However, during the interviews some women also criticized RIVM. These limitations should be taken into account when interpreting the results, as they may restrict the generalizability of the findings.
The richness of the data collected during study could also serve for a deep exploration of cultural nuances. However, this was not undertaken, as it is beyond the scope of this present study. Instead, the aim was to investigate the information seeking behavior and the information needs specifically, rather than providing an in-depth cultural analysis in general.
Conclusion
Overall, this study yielded valuable insights into the current information seeking behavior and the information needs and preferences regarding CC screening and HPV vaccination among Turkish-, Moroccan-, and Syrian-Dutch women. While the current study offers valuable insights, it underscores the need for further efforts to reach and inform immigrant women about CC prevention programs. Comparison with CC prevention measures in their countries of origin may facilitate information processing and understanding. It is necessary to address the practical, emotional, cultural, and religious aspects regarding virginity, fertility, and sexual activity. These aspects should be incorporated into informational meetings and audiovisual materials to support Turkish-, Moroccan-, and Syrian-Dutch women in their informed decision-making regarding CC screening and HPV vaccination.
Supplemental Material
Supplemental material - Supporting Informed Decision-Making Regarding Participation in Cervical Cancer Prevention Programs: A Qualitative Study Among Turkish-, Moroccan-, and Syrian-Dutch Women
Supplemental material for Supporting Informed Decision-Making Regarding Participation in Cervical Cancer Prevention Programs: A Qualitative Study Among Turkish-, Moroccan-, and Syrian-Dutch women by Tharsini Veeravagu, Nora Hamdiui, Mart L. Stein, Nadien Al-Rubaie, Josien van Wijk, Narjiss Ben Ali, Rik Crutzen and Aura Timen in Community Health Equity Research & Policy.
Footnotes
Acknowledgements
The authors would like to thank all participants for their contributions in the interviews and for inviting others to participate as well. The authors thank Berfin Duman (BD) for conducting, translating, and transcribing a subset of the Turkish interviews. The authors would like to thank their own network, influencers, key community figures, Facebook groups, mosques, community centers, and foundations that helped with the recruitment of Turkish-, Moroccan-, and Syrian-Dutch women. The authors are thankful to the Foundation Al Amal for their support in the recruitment of Turkish-, Moroccan-, and Syrian-Dutch women.
Ethical Considerations
Ethical clearance was obtained from the Medical Ethics Review Committee of the University Medical Centre Utrecht (23-090/DB). The Committee confirmed that the Medical Research Involving Human Subjects Act (WMO) does not apply to this study. Participation was completely voluntary, and participants were allowed to withdraw from the study at any moment. Confidentiality was maintained by removing all reducible personal data from the transcripts during processing and storage.
Consent to Participate
Informed consent to participate was obtained from all individual participants included in the study.
Consent for Publication
Informed consent for publication was obtained from all individual participants included in the study.
Author Contributions
TV and NH conceived and designed the study. TV, NHS, NBA, BD and NH conducted the interviews, and TV, NHS, NBA and NH analyzed the interviews. TV wrote the first draft of the manuscript. All authors provided critical revisions on the interview guide and the manuscript. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by ZonMw under (grant number: 2477411).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data generated and/or analyzed during the current study are not publicly available due to privacy reasons, but are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.