
Abstract
Aim
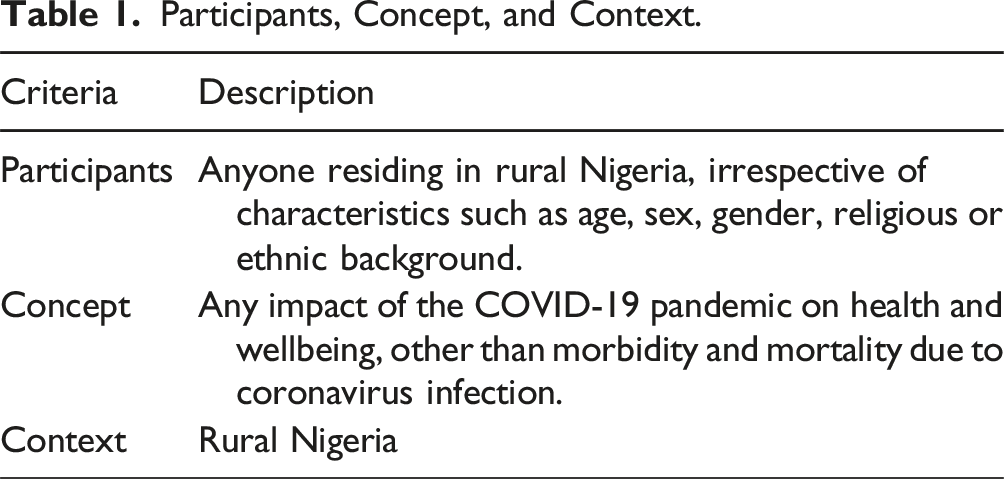
Collate and summarise published evidence of the non-clinical effects of the COVID-19 pandemic in rural Nigeria and compare the findings with community stakeholder experiences.
Methods
We searched PubMed, Scopus, and Cumulative Index to Nursing and Allied Health Literature (CINAHL) for peer-reviewed papers published up to January 2024. Included studies used quantitative, qualitative, or mixed methods to examine the influence of the COVID-19 pandemic on the lives of rural Nigerians. Two reviewers conducted title, abstract, and full-text screening independently. We used narrative descriptions and fuzzy cognitive maps to summarise the findings of the review and compared the maps with those previously created by stakeholders in rural communities in Bauchi State, rural Nigeria.
Results
Poverty, hunger and lack of food, and stress and mental health problems were leading themes in both the literature and stakeholder maps. Stakeholder maps highlighted job loss and household conflicts. These topics were rarely explored in the literature, which emphasized reduced health services.
Conclusion
This review and stakeholder perspectives confirm the importance of non-clinical impacts of the COVID-19 pandemic in rural Nigeria. Some issues highlighted by local community stakeholders were absent in the literature. Contextualizing published research with local experience provides specific insights to inform recovery policies.
Keywords
Introduction
The impact of the COVID-19 pandemic on sub-Saharan Africa has been far-reaching and complex. 1 Focusing solely on health impacts of the infection provides an incomplete picture. Secondary effects of the pandemic bring long-term challenges for individuals and communities. The United Nations emphasized the need to study the indirect impacts of the pandemic to inform comprehensive and equitable recovery strategies. 2 The pandemic’s disruptions to economic activities, education, food systems, and healthcare services exacerbated pre-existing vulnerabilities, particularly in low-resource settings.3,4 Stringent lockdown and social distancing measures contributed to market closures, job losses, and weakened local economies.1,3 These changes led to steep increases in the prices of food and goods, increasing poverty and food insecurity. 5 Pre-existing structural and socio-economic inequalities exacerbated these challenges, disproportionately affecting marginalized populations and further widening inequalities. 6 This review examines the pandemic’s secondary effects on rural Nigerian populations to gain insights that may inform ongoing COVID-19 recovery strategies in Nigeria and other low-income countries.
Nigeria is Africa’s largest economy, yet nearly 40% of its population live in poverty; national statistics mask marked regional health and socioeconomic inequalities. 7 Access to resources and health outcomes are worse in rural settings. Rural Nigeria has poor infrastructure, fragile healthcare systems, and relies on informal economies.7,8
There were relatively few deaths from COVID-19 in Nigeria during the pandemic, even allowing for serious under-reporting of cases: in January 2023, Nigeria (with a population of over 218 million) reported 266,207 COVID-19 cumulative cases and 3155 deaths. 9 But pre-existing inequalities were exacerbated by market closures, job losses, and mobility restrictions, which weakened local economies and restricted access to basic needs.1,3,10,11 The shift in healthcare resources toward COVID responses disrupted services such as antenatal care and immunizations. 12 School closures reduced access of millions of children and adolescents to education, extra-curricular activities, and social interaction.13,14 Lockdown and social distancing disrupted social networks, contributing to stress and mental health problems. 15 Many small studies have reported on impacts of the pandemic on specific, usually researcher-defined, outcomes in rural Nigeria.
Our scoping review collates the published evidence about these impacts. It is part of a larger project examining the impact of the COVID-19 pandemic in rural Bauchi State, Nigeria, and supporting community co-design of recovery strategies. We used fuzzy cognitive mapping (FCM) to compare the evidence from the scoping review with community stakeholder perspectives about the factors that worsened their experience of the COVID-19 pandemic. FCM depicts perceived causal relationships. 16 It provides a common format for juxtaposition of different knowledge sources. 17 The maps can depict relationships reported in the literature, associations identified through survey data, or causes perceived by stakeholders. 17 Dion and colleagues developed the Weight of Evidence approach using fuzzy cognitive mapping to update and contextualise literature reviews with knowledge and perceptions of stakeholders.18,19 The approach was useful for contextualising the literature about the role of traditional midwives for maternal health in Indigenous communities in Mexico. 20 We created cognitive maps of the factors related to the experience of the COVID-19 pandemic identified in the scoping review and compared them with community stakeholder maps of perceived causes of a bad experience of the pandemic in Bauchi State, northern Nigeria. 21
Methods
Overview
Participants, Concept, and Context.
Search Strategy
We searched for peer-reviewed articles in PubMed, Scopus, Cumulative Index to Nursing and Allied Health Literature (CINAHL) published before January 2024. The search matrix included a combination of keywords to represent the rural Nigerian population and search terms related to the COVID-19 pandemic. Supplemental Material presents the search matrices we used.
Eligibility Criteria
We included studies about the impact of COVID-19 in rural Nigerian populations. We excluded papers reporting exclusively on morbidity or mortality due to coronavirus infection. The review included articles published in English peer-reviewed journals at any time up to January 2024. Eligible articles presented empirical evidence from qualitative, quantitative, or mixed methods studies. We considered multinational studies but excluded articles that did not present disaggregated data from rural Nigerian settings. We excluded reviews, editorial pieces, and grey literature, such as reports, conference proceedings, or other non-peer-reviewed documents.
Study Selection
Two reviewers (MZG and NRC) independently screened titles and abstracts. They resolved disagreements through discussion. They screened the full text of potentially eligible articles according to the agreed eligibility criteria, recording why they excluded articles and resolving disagreements through discussion, involving a third reviewer (IS) if necessary.
Data Extraction
MZG and NRC independently extracted data from included articles, involving a third reviewer (IS) if necessary to resolve disagreements. They created a data extraction template in Airtable (airtable.com), piloted it with five randomly chosen studies, and made modifications.
The template recorded study characteristics (authors, year of data collection, study design, data collection methods, research setting) and participant demographics (gender, age, occupation). It also recorded the reported impacts of the COVID-19 pandemic in a form to support creation of fuzzy cognitive maps from the review. The guidelines for identifying and justifying relationships extracted from the literature are shown in Supplemental Material. We specifically trained reviewers for the task. Two reviewers undertook the task separately and resolved conflicts by discussion with a third reviewer. For each identified relationship, the reviewers recorded the supporting data from the paper. For quantitative studies, they included all relationships significant at the 5% level in univariate analysis or in multivariate analysis if available. For qualitative studies, they recorded quotes describing the relationships. They did not include relationships based on assumptions or hypothesized explanations reported in the papers. They included second order relationships when these were reported. For example, a paper might report that lockdown caused market closures, which caused food insecurity.
From the extracted data on relationships, the reviewers created a list of reported relationships (an edge list). Edge lists are tabular formats of the elements of fuzzy cognitive maps. The first column contains the factors originating relationships (causes), the second column contains the landing factors (outcomes), and the third column indicates the relationship weights and signs. 20 Positive signs indicate that an increment of the cause leads to an increment in the outcome, while negative signs indicate that an increment of the cause leads to a decrease in the outcome. For the literature maps, any reported relationship received a weight of (meaning it was present in the study). For example, a qualitative study might report that market closure (cause) resulted in food insecurity (outcome). The relationship sign is positive because more markets closure leads to more food insecurity.
Data Analysis and Mapping
The research team standardized the names of the factors reported across the studies, ensuring factors with effectively the same meaning had the same name. On the standardized maps, we applied fuzzy transitive closure (available in CIETmap 2.2). 24 This mathematical model translates the map of individual associations into a knowledge network by identifying all the direct and indirect connections between factors and all possible ways a factor on the map can influence others. 24 Transitive closure adjusts the map by down-weighting direct arrows it adds between nodes (factors) that previously only had indirect connections.
To weight each relationship in the literature map, we calculated its relative frequency across the studies in the review. Inspired by Harris’ original discourse analysis, the more articles that identify the same relationship, the more likely the causal meaning of the relationship within the “universe” of the literature. 25 This weighting process is operator-independent: it does not rely on researcher interpretation to assign weights to relationships. 26
To simplify interpretation, four of the authors (MZG, IS, NRC, and AC) condensed the aggregate literature map into a category map, grouping factors with similar implications for action. We categorized using a digital version of the physical grouping of factor labels on a large whiteboard used for community stakeholder categorization in Nigeria. Considering factors one by one, the authors placed related factors together while constantly reviewing the emerging categories. We first used categories developed from community stakeholder FCM in Bauchi State. 21 We created additional categories for factors that did not fit into any of these categories.
We used social network analysis to compute indegree and outdegree centrality for each category in the map. 27 Outdegree centrality is the sum of absolute values of the weights of outgoing arrows; higher values indicate more important causes in the network. Indegree centrality is the sum of absolute values of the weights of incoming arrows; higher values indicate important outcomes in the network.
Comparing the Scoping Review with Local Knowledge Using FCM
We created pattern-matching tables contrasting outdegree and indegree centrality measures between the literature and stakeholder category maps. This highlighted the similarities and differences in the most important causes and outcomes between the two knowledge sources. We also compared the narrative content of categories in the literature and stakeholder maps.
Results
Included Articles and the Factors They Considered
Figure 1 presents the PRISMA flow diagram and outlines the selection process from 742 references to 33 studies for inclusion. Table 2 summarises the characteristics of the included articles. Seven described international studies that included disaggregated data for rural Nigeria.31,37,38,53,55,56,60 Most studies used quantitative methods, mainly cross-sectional designs (n = 23), seven used qualitative methods, and two applied mixed methods. The included studies collected data between 2020 and 2022; 14 studies looked at the pandemic’s early effects in 2020. PRISMA flow diagram of scoping review on the impact of the COVID pandemic in rural Nigeria. Characteristics of Included Studies.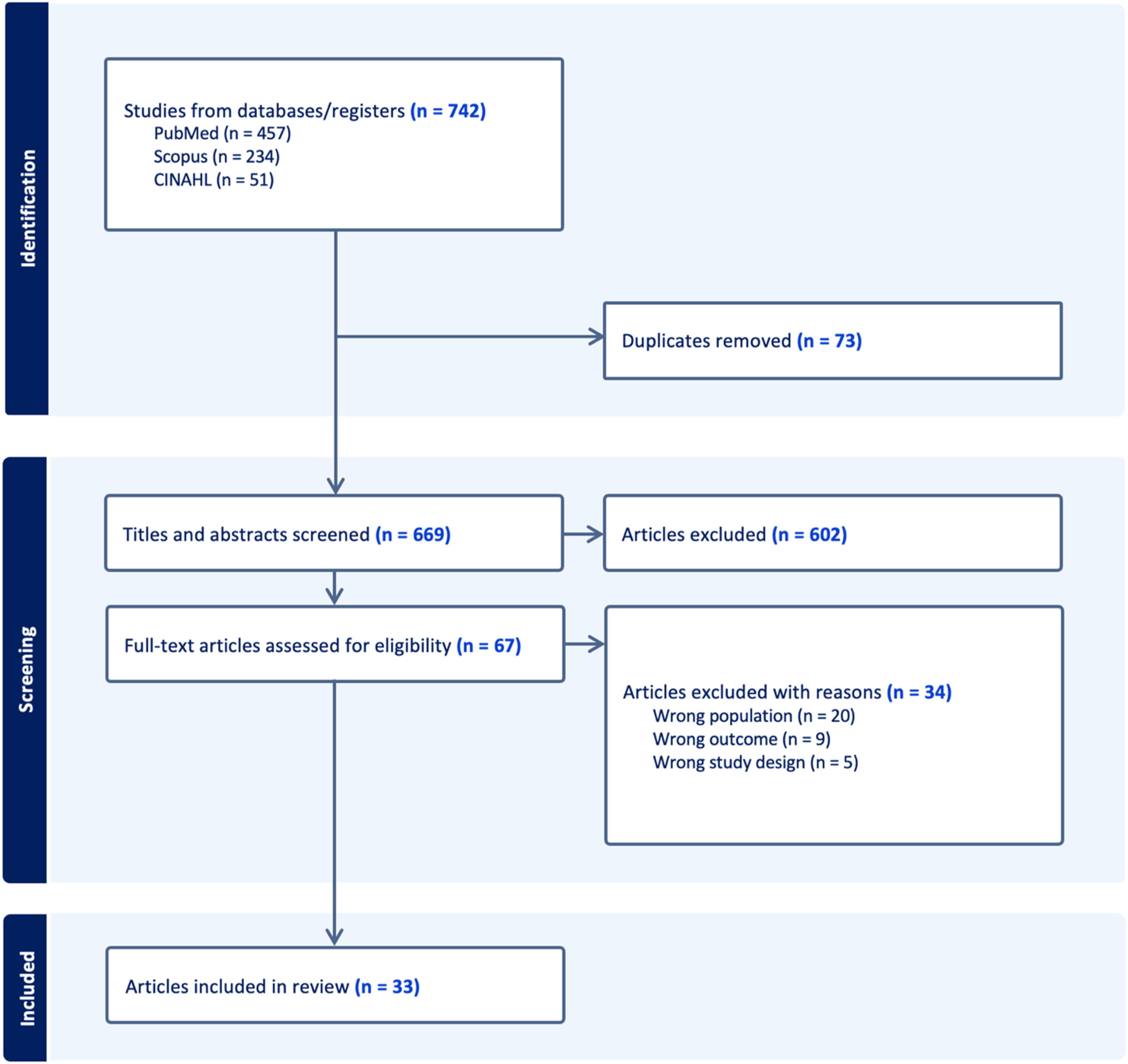
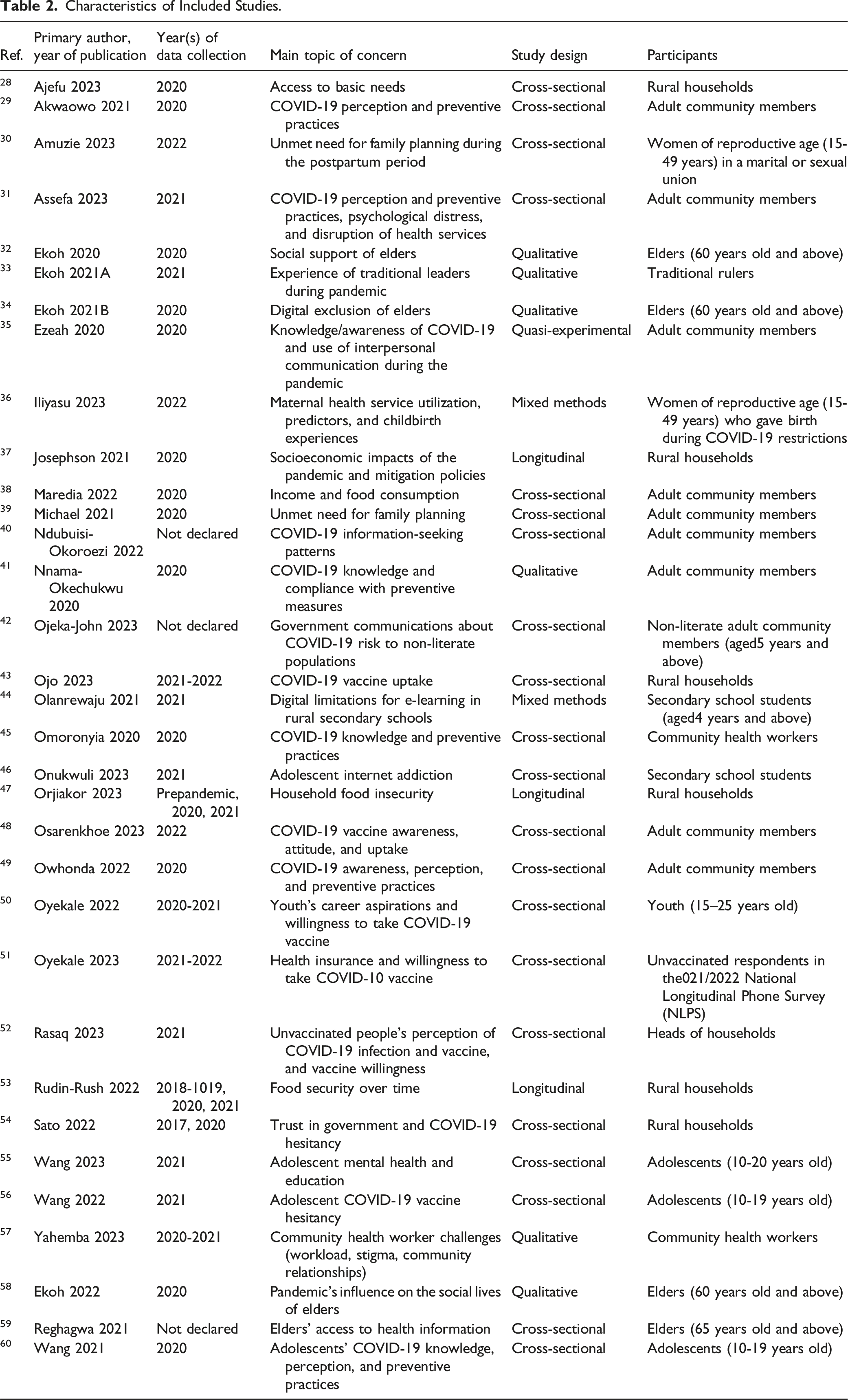
A common focus of the included articles was COVID-19 knowledge, perceptions, and preventive practices. Seven articles focused on individual experience of understanding and complying with public health measures and the influence of these measures on personal, economic, and community life.29,31,35,41,45,49,60 Five articles addressed vaccine hesitancy, including awareness about the vaccine, willingness to receive the vaccine, and trust in government communications.43,48,50,51,52,54,56 Four studies focussed on socioeconomic impacts of the pandemic, including food insecurity, income loss, and restricted access to basic needs.28,38,47,53 Three studies examined the challenges elders and adolescents faced in using digital technology to facilitate social contact, access information, and participate in e-learning platforms during the pandemic.34,44 Three studies focused on maternal and reproductive health, examining unmet family planning needs and barriers to accessing maternal health services.30,36,39 Other topics included adolescent mental health, community health worker challenges, and the social impacts on older adults.
Factors and Categories in the Literature Maps
Brief Description of Categories of Factors From the Literature.
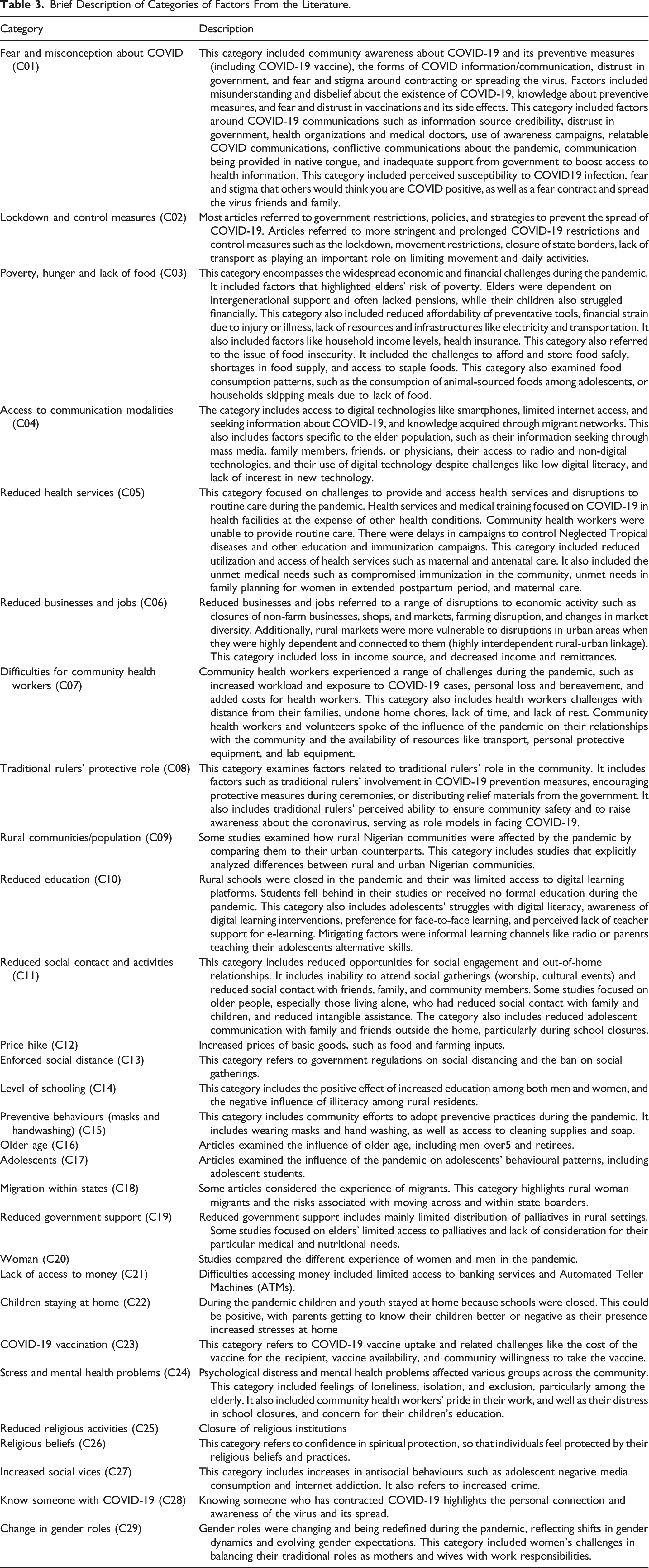
Figure depicts the relationships in the literature category map between categories with the highest indegree centrality (outcomes) and highest outdegree centrality (causes). Online Supplemental File shows the adjacency matrix for the final literature category map showing all relationships and their weights, and the calculated indegree and outdegree centrality of each category. Relationships among the categories with higher indegree and outdegree centrality. This fuzzy cognitive map includes the five categories with the highest indegree and outdegree centrality, representing the main outcomes and causes in the literature map. The complete set of relationships is provided in Online Supplemental File 4. Line thickness is proportional to the cumulative influence of one category on another, with values of ±1 indicating the strongest influences.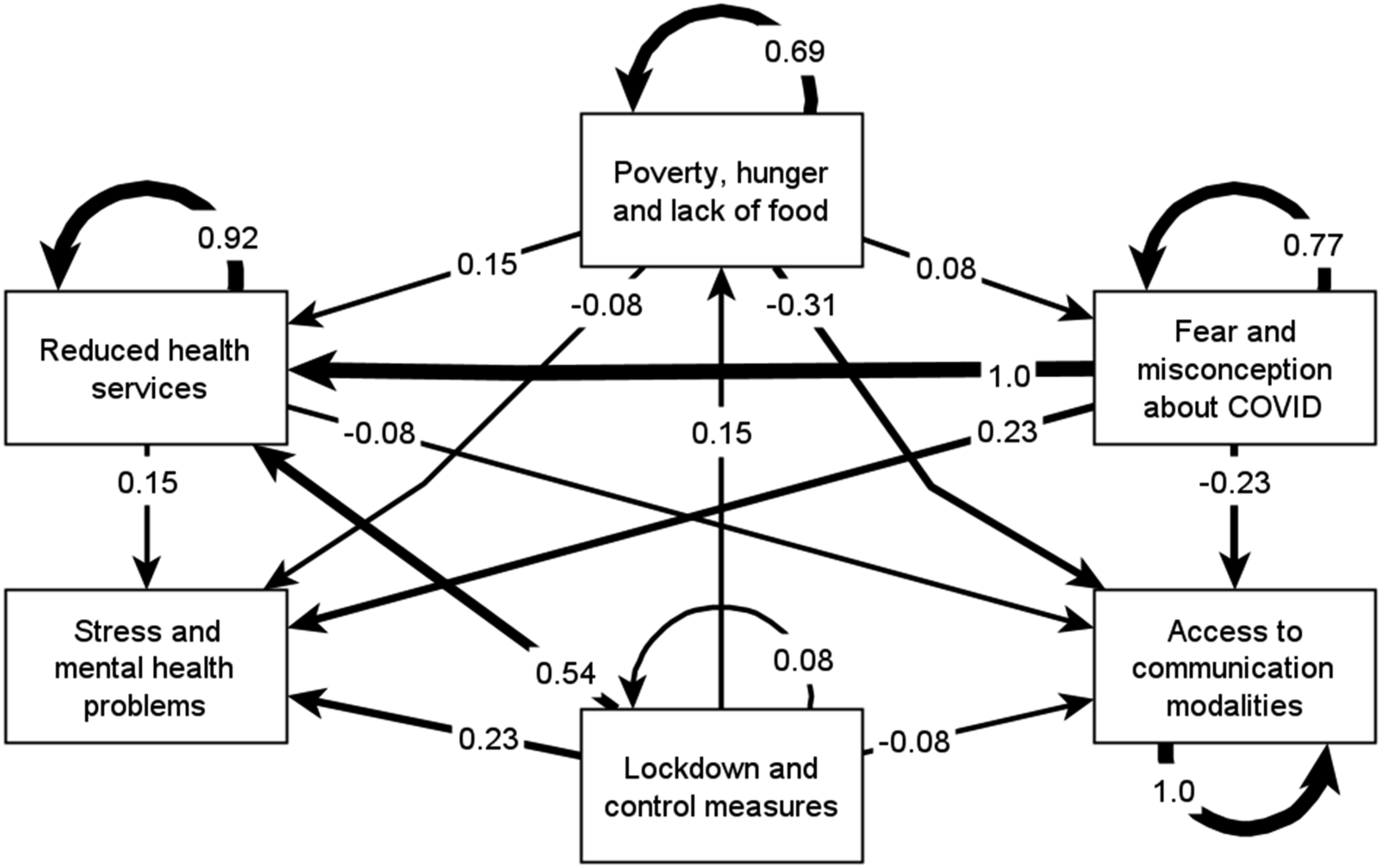
Main Outcomes in the Literature Map
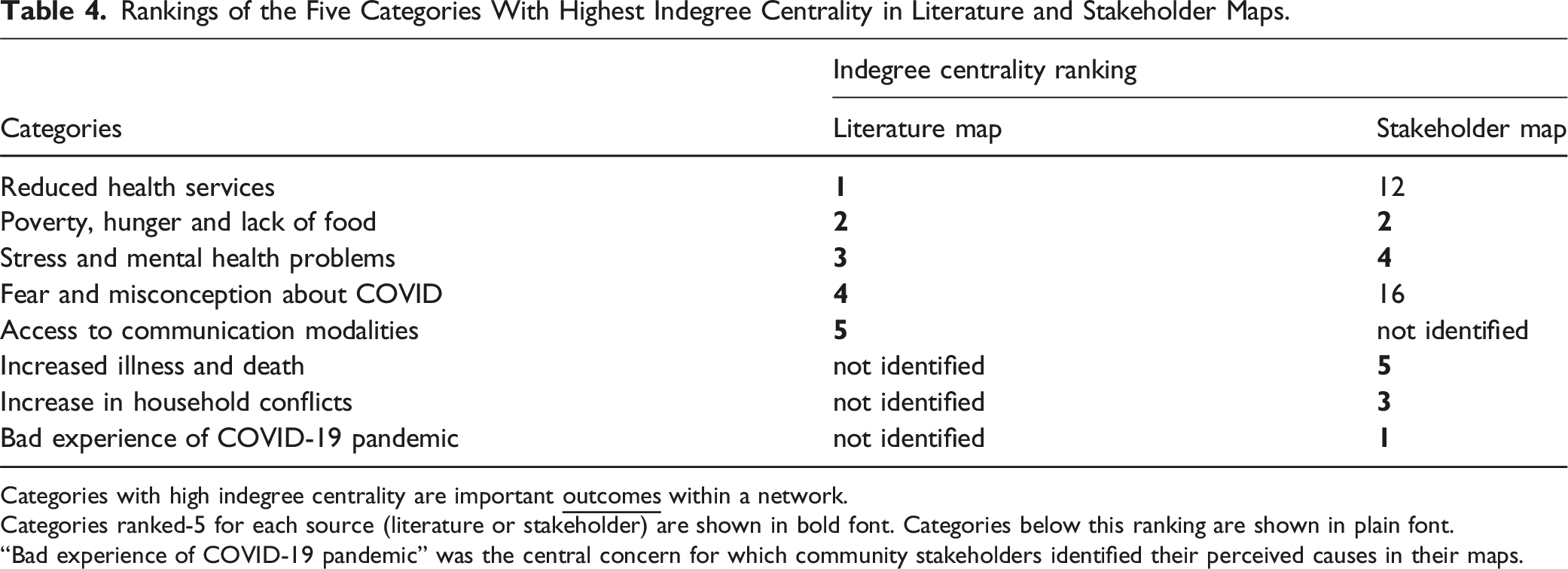
Rankings of the Five Categories With Highest Indegree Centrality in Literature and Stakeholder Maps.
Categories with high indegree centrality are important
Categories ranked-5 for each source (literature or stakeholder) are shown in bold font. Categories below this ranking are shown in plain font.
“Bad experience of COVID-19 pandemic” was the central concern for which community stakeholders identified their perceived causes in their maps.
The second most prominent outcome (Table 4) was poverty, hunger, and lack of food. This category included increased poverty specifically among elderly people who depended on intergenerational support but whose children were also struggling financially. Food insecurity was prominent, with households skipping meals, unable to buy and store food, and facing staple food supply shortages.
Stress and mental health problems were ranked third among outcomes (Table 4). This category included feelings of loneliness, isolation, and exclusion, particularly among the elderly.
Fear and misconceptions of COVID (Table 4) ranked fourth as an outcome. This broad category included misconceptions about the existence of COVID-19 and fear and distrust around vaccination. Fear and misconceptions were reduced by effective awareness campaigns, and the protective role of traditional rulers. Fear and stigma concerned contracting COVID and spreading infection to friends and family.
Access to communication modalities (Table 4) was the fifth most prominent outcome. This outcome mitigated against adverse effects of other categories. Among older people, the category included actively seeking information, access to radio and non-digital technologies, and use of digital technology.
Leading Causes in the Literature Map
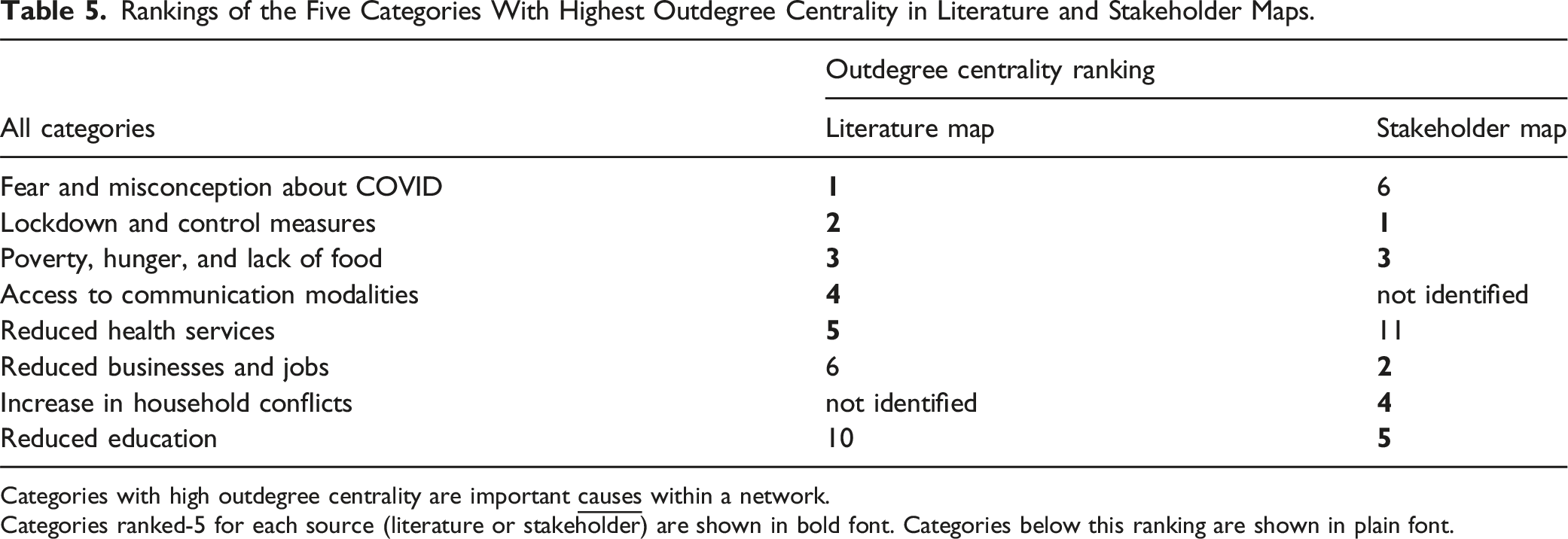
Rankings of the Five Categories With Highest Outdegree Centrality in Literature and Stakeholder Maps.
Categories with high outdegree centrality are important
Categories ranked-5 for each source (literature or stakeholder) are shown in bold font. Categories below this ranking are shown in plain font.
The close second ranked cause on the map was lockdown and control measures. The main associated outcomes were reduced health services and lack of social contact and activities. Lockdown and control measures contributed importantly to stress and mental health problems.
Poverty, hunger and lack of food ranked third as a cause (Table 5), linked with outcomes such as stress and mental health problems. The fourth-ranked cause was access to communication. This category reduced the outcome of reduced education, through improved internet connectivity.
Reduced health services was the fifth strongest causal category. The inability of community health workers to provide routine care compromised immunization efforts, and the focus on COVID-19 in health facilities significantly impacted healthcare services. Fear of harassment during childbirth, overcrowding in clinics, and unclean examination areas deterred individuals from seeking medical attention. Non-availability of health workers and maternal health services led to unmet needs for family planning.
Reduced businesses and jobs was the sixth strongest cause. This included disruption from closure of businesses, shops, and markets, and farming disruption. Loss of sources of income included loss of remittances from family members working away from home.
Comparison of the Scoping Review Findings with Stakeholder Knowledge
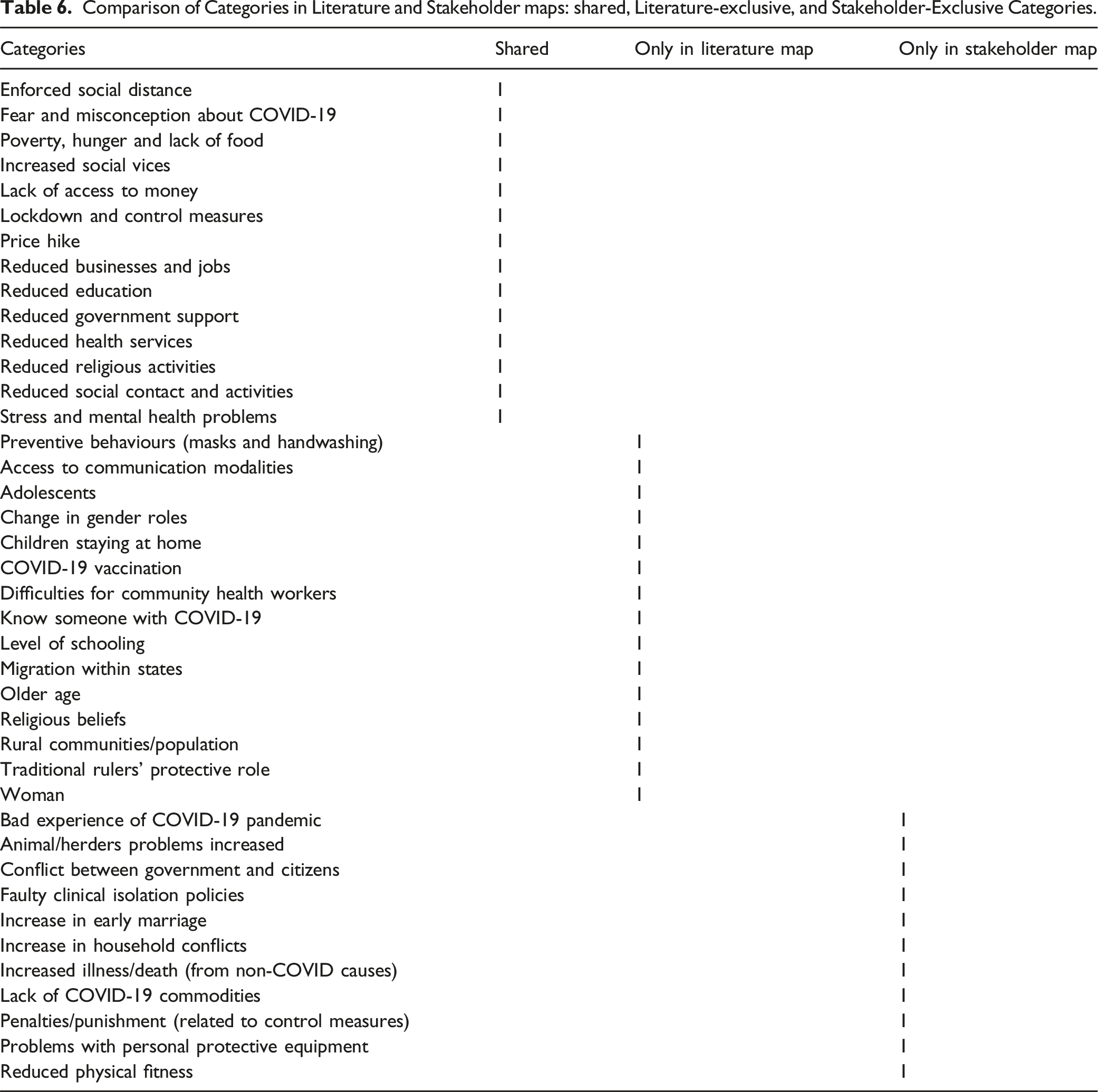
Comparison of Categories in Literature and Stakeholder maps: shared, Literature-exclusive, and Stakeholder-Exclusive Categories.
Bad experience during the COVID-19 pandemic was the most important outcome for stakeholders (Table 4) because this category was the central outcome for their mapping sessions. This outcome did not appear in the map from the literature; rather the articles examined outcomes and potential causes identified by researchers. Both sources of knowledge identified poverty, hunger and lack of food and Stress and mental health problems as prominent outcomes of the pandemic. However, the main outcome reported in the literature, reduced health services, was much less prominent in the community maps, ranking only 12th for indegree centrality. Other important outcomes from the literature, fear and misconception about COVID and access to communication modalities, were less important or absent in stakeholder maps. On the other hand, increased household conflicts, identified as the third most prominent outcome category by Bauchi community stakeholders, was not reported at all as an outcome in the studies included in the scoping review.
Table 5 compares literature and stakeholder rankings of outdegree centrality, as an indicator of the importance of categories as causes in the maps. Both the literature and stakeholders identified lockdown and control measures and poverty, hunger, and lack of food as prominent causes of other categories. However, fear and misconception about COVID was a much stronger cause in research studies than among community members. Access to communication modalities, prominent as a mitigation of problems in the literature, was not mentioned at all by community stakeholders. Increased household conflicts and reduced education were much more important causes of problems for community stakeholders than in the literature.
We compared the factors within each of the top five indegree and outdegree centrality categories between the literature and stakeholder maps (see Supplemental Material 7). For most categories, the factors were quite similar between the literature and stakeholder maps. For example, in the category reduced businesses and jobs, the common factors included market closures, job and income loss, farm and non-farm closures. The individual factors in the literature tended to be broader than those identified by community stakeholders. Stakeholder maps included factors specific to their context, such as challenges with religious schooling, household conflicts, loss of Hajj deposits, and limited access to farm tools. The literature maps also included some highly specific factors described in studies of particular population groups, such as community health workers, elders, and adolescent students.
Discussion
This scoping review identified factors associated with negative experiences of the COVID-19 pandemic in rural Nigeria in published literature and juxtaposed the results with stakeholder perspectives from one area of Bauchi State in Northern Nigeria. There was a large overlap in themes, such as poverty, hunger, and lack of food, fear and misconceptions of COVID, as well as the detrimental effects of lockdown and social distancing measures. Both the literature and stakeholders highlighted the critical role of food insecurity, exacerbated by market closures and price hikes. There were also important differences. The literature emphasised reduced health services as an important outcome, while stakeholders identified increased household conflicts as a key outcome. Access to communication modalities was identified as an important influence on pandemic impact in the literature, but did not feature in the stakeholder maps. Stress and mental health issues were important outcomes of the pandemic in both the literature and stakeholder maps; community stakeholders also saw them as causing other problems.
Studies in other countries reported that COVID-19 exacerbated existing challenges in rural communities, including poverty, isolation, socio-economic marginalization, and loss of livelihood and income, even in high income countries such as Canada, US and Australia. 61 A021 review reported that lockdown measures in six low- and middle-income countries (LMIC), including Nigeria, disproportionately impacted vulnerable populations, who were more at risk from domestic violence, school discontinuity, disruptions in the informal economic sector and limited health system capacity. 62
Stakeholder maps identified as important some factors that were rarely, if at all, reported in the literature, even though we deliberately restricted the scope of the review to the rural Nigerian setting. It was not that the studies in the review examined the influence of these factors and found them not to be important; rather they did not examine them at all. What gets studied often depends on the interests and biases of researchers, sometimes influenced by the interests and biases of funding bodies. This bias carries over into systematic and scoping reviews, which can only include what is “out there”, even if they attempt to include grey literature. Chackalackal and colleagues broadened the scope of their literature review of the effects of lockdown in LMIC by including mass media reports as well as journal articles. 62 Contextualising literature findings with local knowledge, as we did in this case, ensures inclusion of locally important causes of a problem and provides evidence to support codesign of locally appropriate solutions. Relying on literature reviews, without local contextualisation, to guide actions may miss important issues.
Our contextualised scoping review confirms the multifaceted impacts of the COVID-19 pandemic in rural Nigeria. By integrating published research with community knowledge, it provides a nuanced understanding of the pandemic’s challenges and opportunities for recovery. As pandemic recovery efforts continue, prioritizing local perspectives will be essential in fostering sustainable and resilient systems in vulnerable communities. This literature review, contextualised by local stakeholder perspectives, was part of a larger project that included a household survey about experiences before and during the pandemic, a process for sharing the findings with local communities, and support for community groups and service providers to plan and implement local actions to support pandemic recovery.
Limitations
The review was limited to English-language peer-reviewed articles, potentially excluding relevant data from unpublished studies or reports and non-English sources. Nigerian scientific literature is almost all in English, so we do not expect the language restriction introduced an important bias. Excluding grey literature may potentially have missed some relevant reports. Fuzzy cognitive mapping, while robust in integrating diverse data, may oversimplify complex causal relationships. The stakeholder maps were from communities in a single local government area of Bauchi State. The findings from the maps are likely relevant to other nearby states, but we do not suggest they are generalizable to other rural Nigerian contexts or rural contexts in other countries. The purpose of creating the stakeholder maps and using them to contextualise the literature review was to inform local action contextualizing the literature to other Nigerian settings would require additional local FCM exercises.
Conclusions
This scoping review describes important non-clinical impacts of the COVID-19 pandemic in rural Nigeria. Expressing the review findings in a fuzzy cognitive map allowed contextualization with local knowledge in stakeholder fuzzy cognitive maps. The contextualised review contributes to ongoing pandemic recovery efforts tailored to the needs and strengths of rural Nigerian communities.
Supplemental Material
Supplemental Material - Experience of the COVID-19 Pandemic in Rural Nigeria: A Scoping Review of the Literature Contextualized With Local Knowledge Using Fuzzy Cognitive Mapping
Supplemental Material for Experience of the COVID-19 Pandemic in Rural Nigeria: A Scoping Review of the Literature Contextualized With Local Knowledge Using Fuzzy Cognitive Mapping by Mona Z. Ghadirian, Ivan Sarmiento, Natalia Reinoso Chávez, Neil AnderssonAnne Cockcroft in Community Health Equity Research & Policy
Supplemental Material
Supplemental Material - Experience of the COVID-19 Pandemic in Rural Nigeria: A Scoping Review of the Literature Contextualized With Local Knowledge Using Fuzzy Cognitive Mapping
Supplemental Material for Experience of the COVID-19 Pandemic in Rural Nigeria: A Scoping Review of the Literature Contextualized With Local Knowledge Using Fuzzy Cognitive Mapping by Mona Z. Ghadirian, Ivan Sarmiento, Natalia Reinoso Chávez, Neil AnderssonAnne Cockcroft in Community Health Equity Research & Policy
Supplemental Material
Supplemental Material - Experience of the COVID-19 Pandemic in Rural Nigeria: A Scoping Review of the Literature Contextualized With Local Knowledge Using Fuzzy Cognitive Mapping
Supplemental Material for Experience of the COVID-19 Pandemic in Rural Nigeria: A Scoping Review of the Literature Contextualized With Local Knowledge Using Fuzzy Cognitive Mapping by Mona Z. Ghadirian, Ivan Sarmiento, Natalia Reinoso Chávez, Neil AnderssonAnne Cockcroft in Community Health Equity Research & Policy
Footnotes
Acknowledgements
We thank Genevieve Gore and Andrés Rojas-Cárdenas for their support in shaping the search strategies used in this review. We also acknowledge the use of grammar checkers (Grammarly and Copilot) powered by generative artificial intelligence.
Author Contributions
AC, MZG and NA conceived the study. IS supported the fuzzy cognitive mapping. MZG, NRC, and IS performed article screening, data extraction, analysis and synthesis. MZG, IS, NRC, and AC drafted the manuscript; all authors contributed to drafts and reviewed and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Canadian Government’s New Frontiers in Research Fund (grant number NFRFR-2022-00439) supported this work.
Ethical Considerations
This scoping review used published data and did not involve interactions with human subjects. It did not require ethical clearance. Ethical clearance for the fuzzy cognitive mapping by community members is detailed in a separate article describing the mapping.
Data Availability Statement
The data used in this study are included in the Supplemental Material.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.