
Abstract
The United States has made tremendous progress in delivering COVID-19 vaccines. As of January 2022, more than 79% of the eligible population had received ≥1 dose of the vaccine. 1 Encouragingly, the relative proportions of administered vaccines among Black and Latinx populations have increased compared with their population sizes. 2 As of late July 2021, among the 58% of people who had received ≥1 vaccine dose and for whom race and ethnicity were known, Latinx and Black people had begun to receive a larger share of recent vaccinations compared with their total population share (30% vs 17% and 13% vs 12%, respectively). 3 These recent trends provide reason for optimism. However, because vaccinations among Black and Latinx populations, who have been disproportionately impacted by COVID-19, have only just begun to match or exceed their population proportions, their overall vaccination rates continue to lag relative to White populations. While we lack vaccination data in more granular race and ethnicity categories, it seems likely that many other racial and ethnic groups, in addition to Black and Latinx populations, included under the broader term Black, Indigenous, and People of Color (BIPOC), are experiencing the same lag relative to White populations.
A New and Challenging Phase of the Vaccine Rollout
The vaccine rollout has been a massive undertaking, and pent-up demand far outpaced supply during the initial months of rollout. More recently, as expected, the pendulum has swung; we have entered a new phase in which demand has declined dramatically, and most people who wanted the vaccine and could easily access it have gotten vaccinated. In this new phase, public health officials and health care institutions, faith-based organizations and youth-led nonprofit organizations, small businesses and huge national companies, tech startups, and many more are getting the chance to apply well-established public health principles that we all (think we) know so well 4 : engage the community, understand their barriers, use trusted messengers to get the word out, and provide information using the channels that communities actually use, in the languages they actually speak. These principles, while not new, have never been more urgently needed, particularly given the explosion of misinformation and disinformation about COVID-19 vaccines. What is new is the unprecedented speed, scale, and complexity of what the nation is attempting to do: vaccinate as many people as possible in the shortest amount of time.
Barriers to Vaccination Access and Creative Strategies to Overcome Them
Across the country, hundreds of organizations at the federal, state, local, and hyperlocal levels are using promising strategies to overcome the many barriers that populations that have been historically marginalized—particularly those in BIPOC communities—confront in accessing COVID-19 vaccination (and health care more generally). The Rockefeller Foundation–funded Equity-First Vaccination Initiative is supporting more than 100 community-based organizations in 5 US cities to lead efforts to increase access to COVID-19 vaccines and accurate information about them. 5 As a learning partner for this initiative, focusing on access to and delivery of vaccines, our team conducted an environmental scan to identify promising practices for overcoming access barriers and promoting racial and ethnic equity in COVID-19 vaccination. Importantly, ensuring access to evidence-based information to build vaccine confidence and counter misinformation is outside our scope but is a crucial part of the overall initiative.
Starting in early April 2021, we conducted repeated online media searches to identify strategies being used across the United States to promote equity in COVID-19 vaccination. 6 We initially conducted these media scans 3 times per week and then decreased the frequency of our searches to weekly, then monthly, through June 14, 2021. We also monitored social media channels, including Twitter, Facebook, Instagram, and Google (through an automated alert), daily to identify additional promising practices. We screened 777 media articles, leading to a total of 228 included articles that (1) described approaches to overcoming access barriers to COVID-19 vaccination and/or (2) contained results of interventions to increase COVID-19 vaccination rates. We excluded articles that only identified barriers to vaccination access without discussing solutions to address them or focused exclusively on overcoming vaccine hesitancy. From those 228 included articles, we abstracted into a Microsoft Excel spreadsheet the following information: the organization(s) leading efforts to address vaccine equity, their location, the target population, the barriers to vaccine access the organization was tackling, interventions used to address those barriers, challenges encountered and solutions to those challenges, and measures of effectiveness, if any.
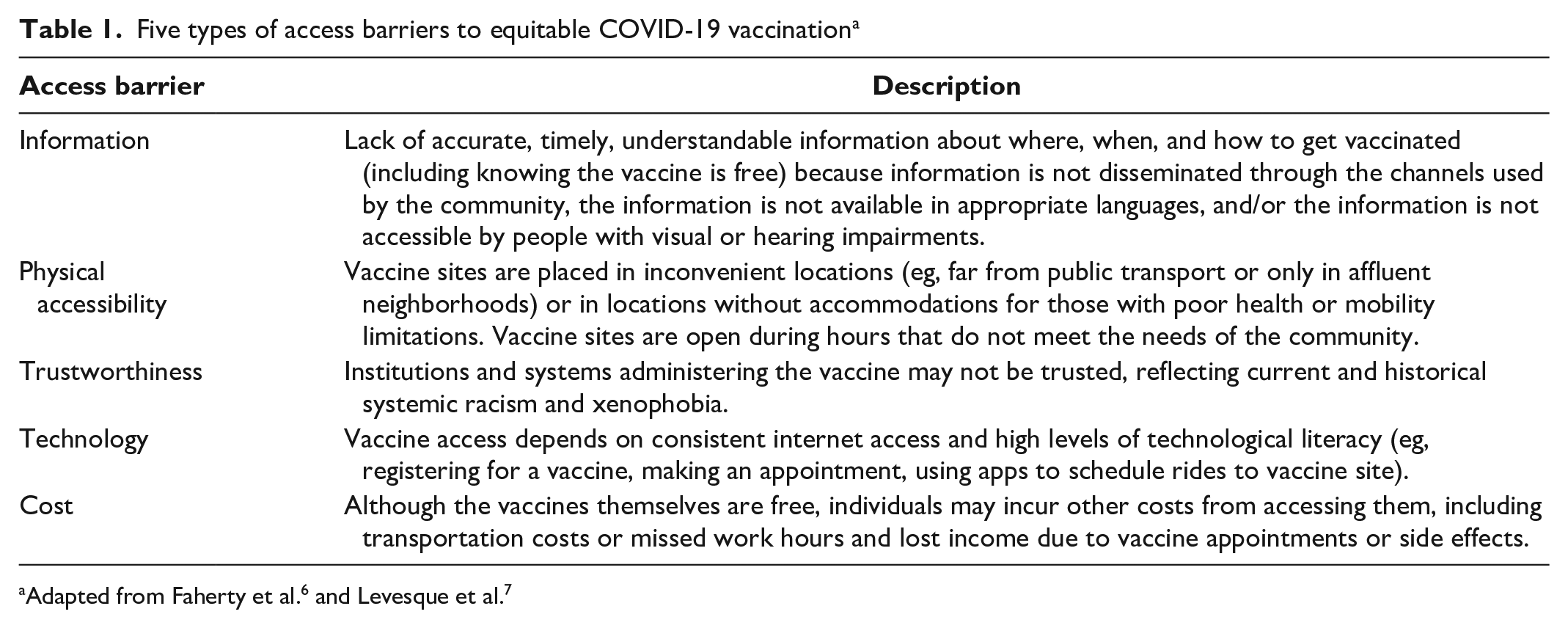
Using a qualitative descriptive approach, in which we sorted the data to identify patterns and synthesized findings into meaningful groups, we organized the most common access barriers into 5 broad categories: information, physical accessibility, trustworthiness, technology, and cost. To do so, we drew on an existing conceptual model of health care access 7 that integrates the supply side (accessibility of services) with the demand side (the person’s ability to access those services), adapting the model to the unique COVID-19 context (Table 1).
Five types of access barriers to equitable COVID-19 vaccination a
Similarly, the strategies organizations are using to address barriers to access and promote COVID-19 vaccine equity can be organized into 5 categories:
We illustrate examples of efforts in each type of strategy (Table 2). For example, the United Way of Cincinnati used a 2-1-1 line to arrange transportation to vaccination appointments. 12 Additionally, growers, agricultural producers, and county farm bureaus throughout California have hosted clinics at local farms and processing plants for agricultural employees during their regular work hours. 22
Equity-focused strategies to promote COVID-19 vaccination a
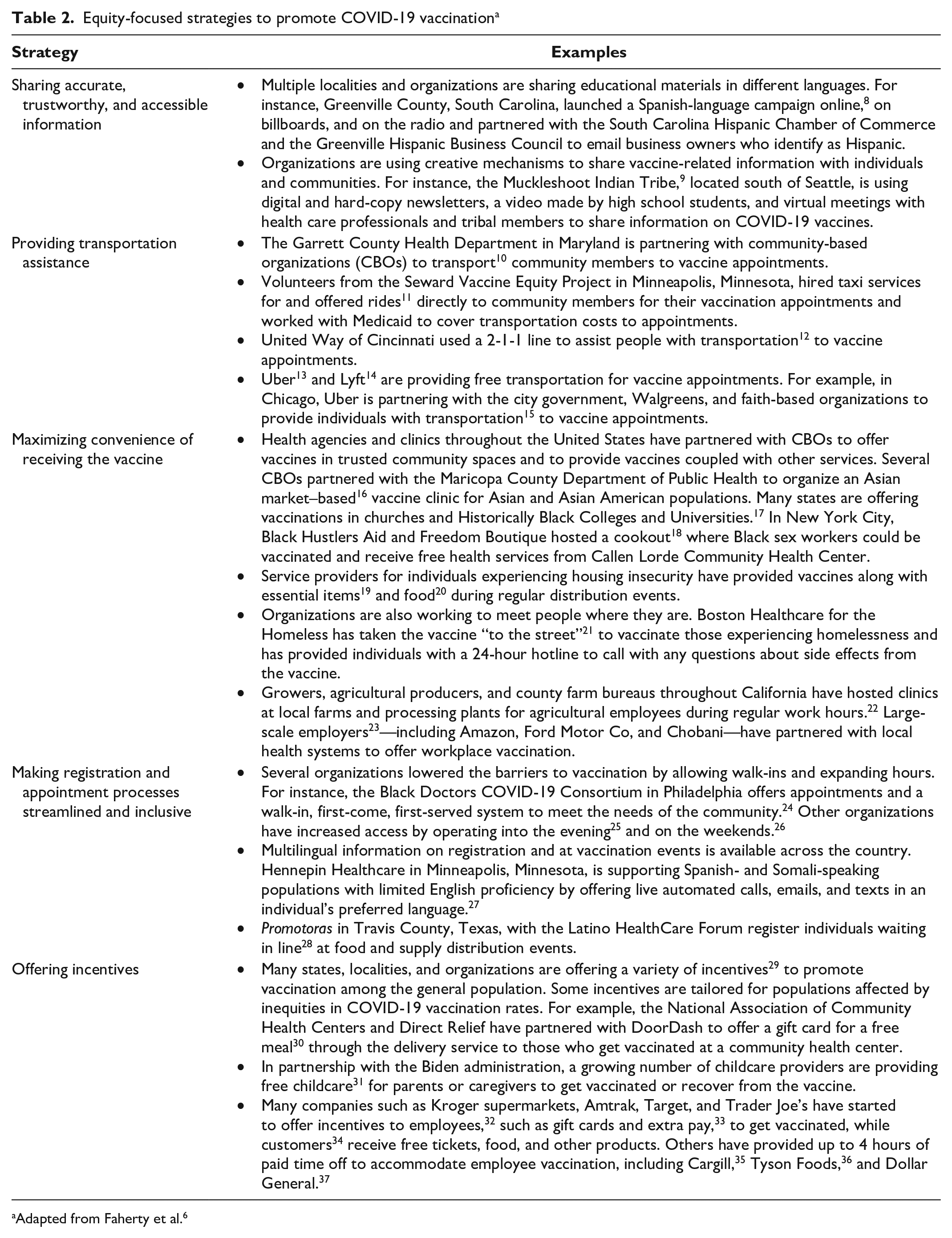
Adapted from Faherty et al. 6
Potential Pitfalls and Missteps in the Implementation of These Strategies
Although these vaccination strategies are inspiring and represent just a sampling of the work that is occurring every day around the country, it was clear from this national scan that in some situations, even the most well-intentioned strategies for equitable vaccine distribution encountered challenges as they were implemented in the real world of a vast, complicated, and urgent vaccine rollout (Table 2). Organizations discovered that even small missteps were thwarting their efforts. Here are just a few examples, organized by the 5 types of strategies:
As these unintended consequences show, the devil is truly in the details when it comes to equitably delivering COVID-19 vaccines in the context of historic and current structural racism, xenophobia, worsening politicization, and declining trust in institutions. 38 In other words, a strategy that seems reasonable and sounds like it should succeed may not be effective if policy makers and implementers do not have the full, detailed picture of the local context in which the strategy is being deployed.
Summary and Policy Implications
Based on the experiences of exemplary organizations at various levels, the first few months of the COVID-19 vaccination rollout showed us that even as we celebrate our progress, public health officials and other policy makers at the federal, state, local, and hyperlocal levels must recommit to closing persistent equity gaps, learning from these early missteps, and sustaining progress toward health equity beyond the pandemic. To do so, structural changes are needed to maximize the chances that the strategies we described will be successful. Specifically, policy makers may consider several actions as they seek to address inequities in COVID-19 vaccination (Table 3).
Policy actions to support hyperlocal efforts to promote equitable COVID-19 vaccination
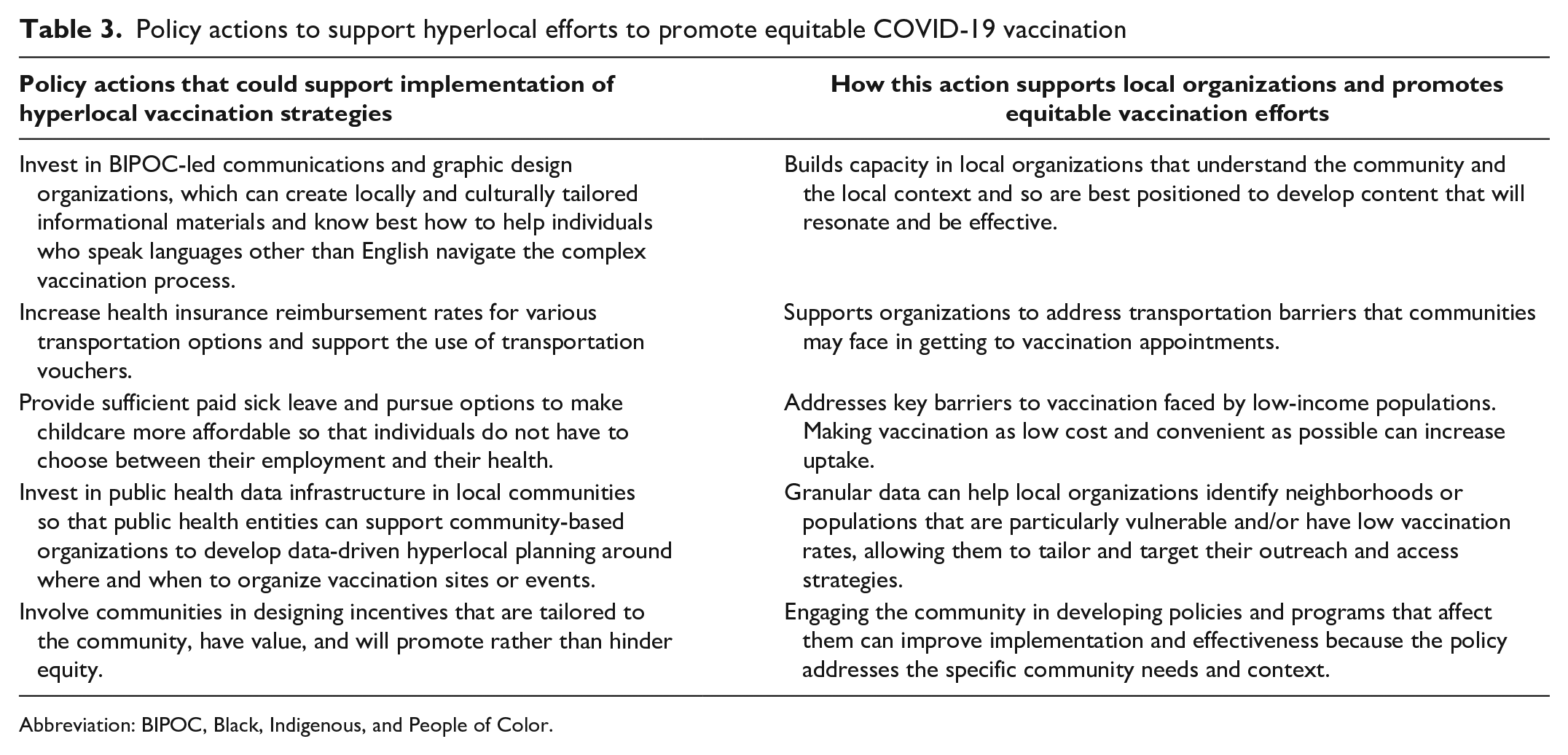
Abbreviation: BIPOC, Black, Indigenous, and People of Color.
As we put our public health principles into practice, we need to continuously and critically examine proposed solutions to overcoming access barriers. These solutions should be designed by members of historically marginalized communities, and their input should be put front and center when implemented and adapted to local contexts. If we fail to do this, our “solutions” at best will not help those they are intended to reach and, at worst, will exacerbate existing inequities in COVID-19 vaccination.
Footnotes
Acknowledgements
The authors thank their RAND colleagues, Kiera Addair, Paul Koegel, and Ninna Gudgell, for their contributions to this work. The authors also thank Boston Medical Center, Del Valle Community Coalition, Growing Coachella Valley, iFoster, Neighborhood Outreach Access to Health, the Rhode Island Department of Health, Sandhills Pediatrics Inc, the San Diego Unified School District, the Seward Vaccine Equity Project, and the University of Pennsylvania Health System, who agreed to be interviewed for this project and provided invaluable insights that informed this work.
Authors’ Note
The findings and conclusions contained in this article are those of the authors and do not necessarily reflect positions or policies of The Rockefeller Foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Rockefeller Foundation.