
Abstract
Introduction
Creative and performing artists are often confronted with precarious employment and insufficient healthcare coverage. A clinic in Canada that provides specialized healthcare to artists offers eligible artists subsidized health services. We aim to compare the use of health services, demographics and health conditions between subsidy artist recipients (SAs) and non-subsidy artists (NSAs).
Methods
We accessed existing data from 265 SAs and 711 NSAs and applied descriptive and inferential statistics to address our research questions.
Results
Musculoskeletal issues, stress, anxiety disorders, and depressive disorders are the most common health problems faced by SAs. Compared to NSAs, SAs were more likely to seek treatment for stress, but less likely to seek treatment for anxiety disorders, depressive disorders, chronic problems, and upper extremity problems.
Discussion
Future research may investigate the enduring effects of subsidized health services on SAs’ health outcomes. Sustained positive outcomes are crucial for maintaining an artist’s career and well-being.
Introduction
Easy and timely access to healthcare services is crucial for the health of Canadian artists. An artist is defined as an individual with specialized training in the artistic field, recognized as a professional by their peers, committed to devoting more time to artistic activities, and having a history of public presentation or publication. 1 Difficulty accessing healthcare is associated with delayed treatment, potentially poorer health outcomes, and increased costs to the healthcare system or patient.2,3 This is particularly true for artists who face unique health risks and occupational injuries as a result of their working conditions. Both visual artists and performing artists are often required to perform highly repetitive movements and sustain postures that can lead to musculoskeletal disorders, which can negatively impact their ability to produce art.4–6 For instance, a study by Kenny & Ackerman (2015) reported that 84% of musicians working at a premier opera orchestra in Australia suffered from performance-related musculoskeletal disorders that interfered with their work. 5 Additionally, visual artists who use pigments may suffer from toxicity due to heavy metals (e.g., lead, cadmium, etc.) and organic solvents. 7
Canada has a publicly-funded healthcare system that provides universal coverage for medically necessary health services. However, certain health services (e.g., physiotherapy and occupational therapy) that are essential for the treatment of artists’ health issues are only covered under specific conditions. For instance, the Ontario government funds physiotherapy for individuals who meet one of the following criteria: (a) 19 years or under, (b) 65 years or older, (c) receive income from Ontario Works or the Ontario Disability Support Program, or (d) stayed overnight at a hospital (within the last 12 months) for a condition requiring physiotherapy. 8 Artists who do not meet any of the criteria must pay out-of-pocket or through private health insurance for physiotherapy and other similar services. This can make treating health conditions very challenging for artists as they tend to have low income4,9 and lack private health insurance.4,10 Thus, subsidized health services can be essential for artists who do not meet the eligibility requirements for publicly-funded care.
The Kaiser Permanente Medical Financial Assistance (KPMFA) program is an example of a subsidized health service program that has provided significant benefits to patients. The KPMFA program provides support to patients, including artists, whose family income is at or below 400% of the United States’ Federal Poverty guidelines by covering up to 100% of their medical fees. 11 A study by Adams et al. (2022) 12 demonstrated that the KPMFA program increased the diagnosis rate for health conditions, medication use, and visits to the inpatient, ambulatory, and emergency departments. Similarly, a systematic review by Hung et al. (2021) 13 found that patients with financial medical assistance (FMA) had earlier prescription pick-ups and were more likely to start and less likely to discontinue using their medication compared to patients without FMA.
The Al and Malka Green Artists’ Health Centre (AHC) is a health clinic in a large, metropolitan city in Ontario, Canada that provides specialized health services to artists. The AHC also provides financial assistance to qualifying artists through the Joysanne Sidimus Fund (JSF). The JSF subsidizes 75% of an artist’s visit at the AHC up to a maximum of $760 annually. Li & Donn (2022) 14 reported that JSF recipients viewed the financial assistance as essential as it enabled easier access to health services and improved their short-term health outcomes. Thus, subsidized health services can help artists treat health conditions that impact their ability to engage in their practice.
This article builds upon Li & Donn’s (2022)
14
study by: (1) quantifying the use of subsidized health services, and (2) exploring how the demographic attributes of subsidy artist recipients relate to their health conditions. We will also compare subsidy artist recipients (SAs) and non-subsidy artists (NSAs) to identify similarities and differences in the health services accessed between both groups. Health-seeking behaviour is defined as the actions or decisions made by individuals to treat any health concern.
15
Understanding health-seeking behaviour is important because various factors that affect health-seeking behaviour can lead to disparities in access and utilization of health services within and between groups.
16
In particular, we seek to answer the following questions: 1. For which health conditions do SAs tend to more likely seek treatment for when compared to NSAs? 2. Is there a relationship between arts discipline and the health conditions SAs seek treatment for? 3. How do health conditions impact the daily lives of SAs?
Understanding these factors can help policymakers and health service providers take action to implement better subsidized health services for artists, and improve health promotion strategies and healthcare delivery.
Methods
Data collection
We accessed de-identified data of 265 SAs who filled out the JSF application form between January 2019 and December 2021. The JSF application form includes a combination of single-choice, multiple-choice, and open-ended items. It assesses an artist’s eligibility for financial assistance based on their residency status in Canada, income, time dedicated to practicing, teaching or learning art, and details of their health condition(s). One item assessed the impact of SAs’ health conditions on their daily lives by asking SAs to rate five 11-point scale items (scales A to E). Artists have access to the JSF form once they have had an initial intake appointment with a nurse practitioner, who provides an initial clinical assessment and asks questions pertaining to their plan for accessing treatment (e.g., how they may pay for uninsured healthcare expenses). At this point, the nurse practitioner informs the artist about the JSF and provides the application form to those who may be interested in applying. The JSF applications were received electronically.
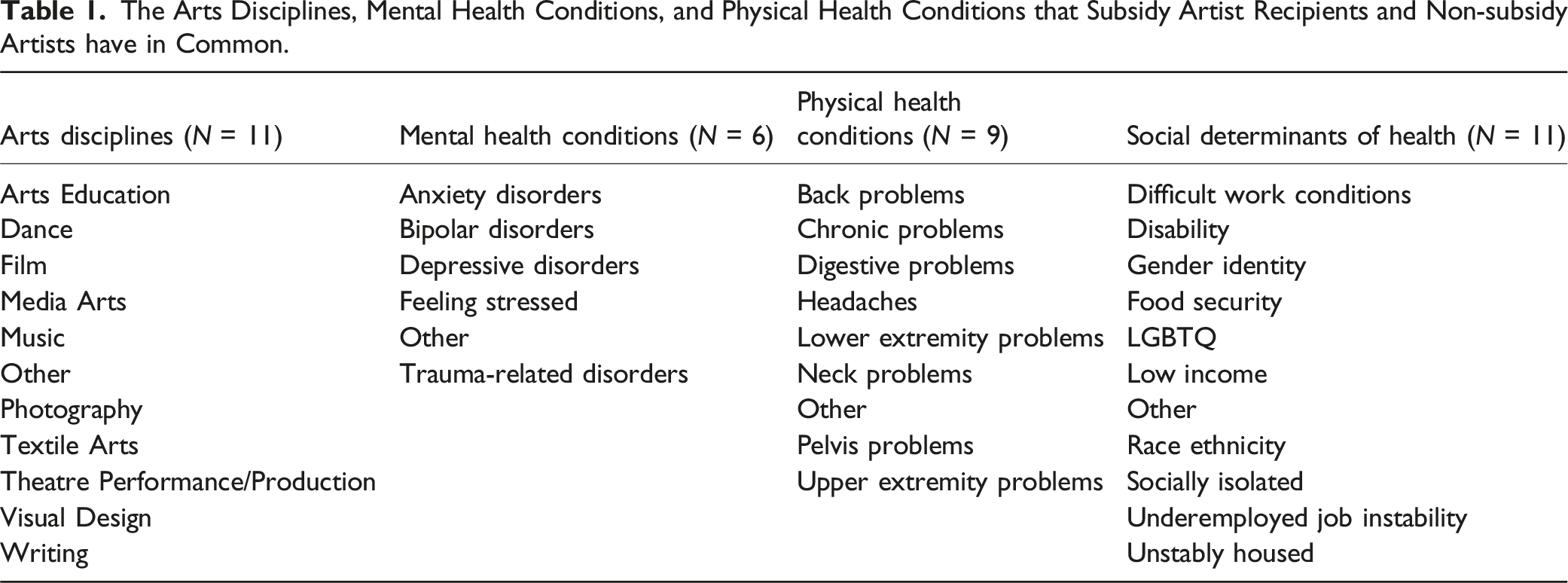
We accessed de-identified data of 711 NSAs who completed the AHC Health Statistics Form between January 2018 and February 2019. The is an 8-item multiple-choice questionnaire that is filled out during a 15-min patient intake interview conducted by a nurse practitioner. Seven of the eight items have an open-ended option (“Other” or “Group physiotherapy [Specify]”) in which a more precise response could be provided. The items ask information about arts discipline, type of clinic visit (e.g., in-person, phone, videoconference), type of mental or physical health condition, type of health service (e.g., physiotherapy, psychotherapy, etc.), internal or external referrals, and social determinants of health (e.g., disability, race, etc.).
We extracted all SA and NSA data from de-identified databases containing the responses for the JSF and AHC Health Statistics forms, respectively, including age and gender demographics. We received a waiver from the Research Ethics Board at University Health Network because it was deemed a quality improvement study.
Data analysis
Descriptive statistics (e.g., mean, standard deviation, etc.) were calculated for age and income, and gender was summarized using frequencies and percentages. Ordinal scale items were summarized using quartiles and mode, and analyzed using Mann-Whitney U and Kruskal-Wallis H tests. The Mann-Whitney U test was performed to determine if: (1) subsidy status was related to or independent of age or gender, and (2) gender was related to or independent of each of the five scales. The Kruskal-Wallis H test was performed to determine if arts discipline was related to or independent of each of the five scales.
The Arts Disciplines, Mental Health Conditions, and Physical Health Conditions that Subsidy Artist Recipients and Non-subsidy Artists have in Common.
The strength of associations for the chi-square test was measured using Cramer’s V (V) or the phi correlation (ϕ) coefficient. In cases where at least one expected cell count was less than five, fisher’s exact test was used. Pairwise comparisons were performed for statistically significant tests.
Multivariable logistic regression was performed to explore whether subsidy status was related to or independent of the likelihood of seeking treatment for a physical health condition versus a mental health condition, while controlling for age, gender, and arts discipline. Odds ratios (OR) and 95% confidence intervals (95% CI) were used to express the strength of the factors influencing the outcome. The Hosmer-Lemeshow test was applied to measure goodness of fit of the regression model. Artists who selected only one arts discipline, and one mental or physical health condition were included in the analysis. Of the selected artists, those missing values for gender or age were also excluded. As a result of the selection criteria, the “other” arts discipline was excluded from the logistic regression due to having no variation in response.
All statistical tests were two-sided and p < .05 was considered significant. IBM SPSS Statistics 26 was used to perform the Mann-Whitney U and Kruskal-Wallis H tests, while R version 4.1.3 was used for all other analyses.
Results
Demographics
Demographics of Subsidy Artist Recipients and Non-subsidy Artists.
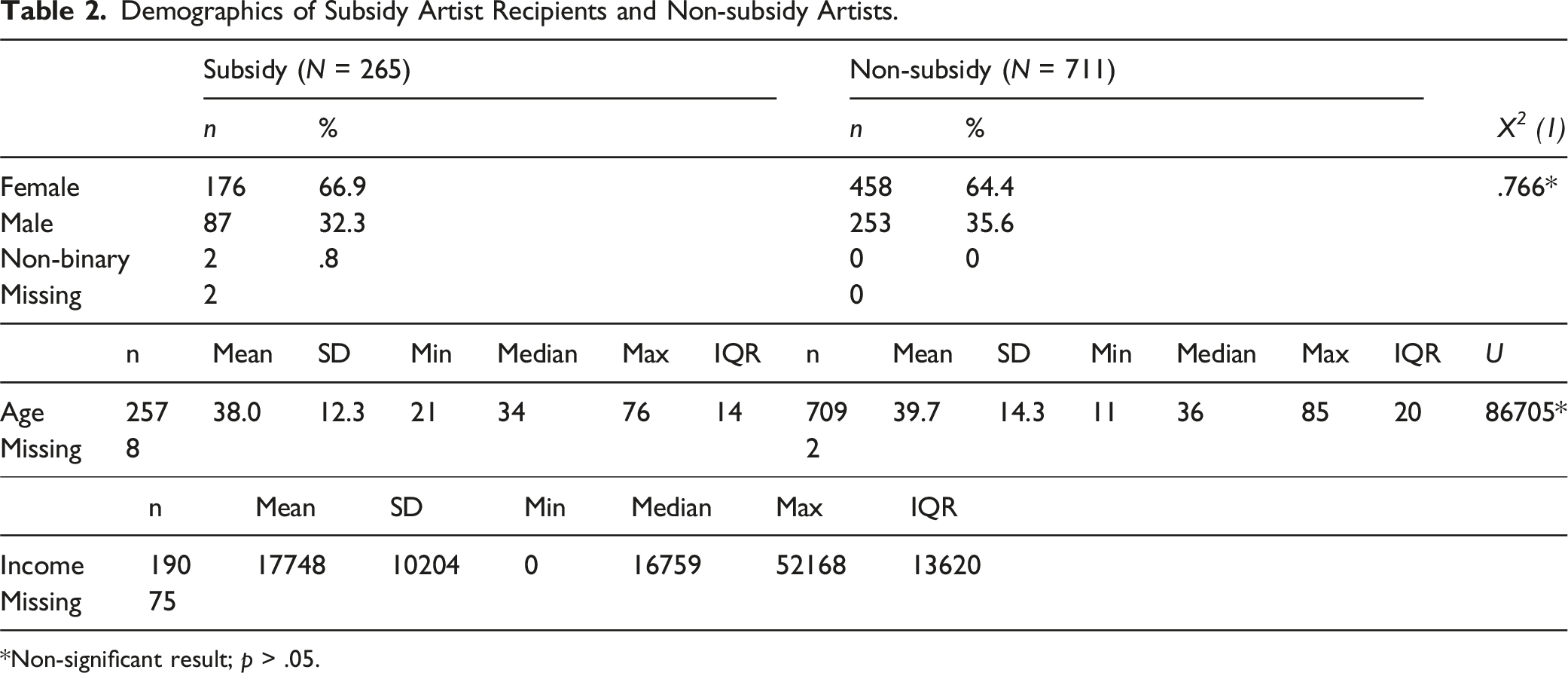
*Non-significant result; p > .05.
Subsidy status and arts discipline and social determinants of health
Frequencies and Percentages of Each Arts Discipline by Subsidy Status, and Chi-Square Test of Independence Between Subsidy Status and Arts Discipline.
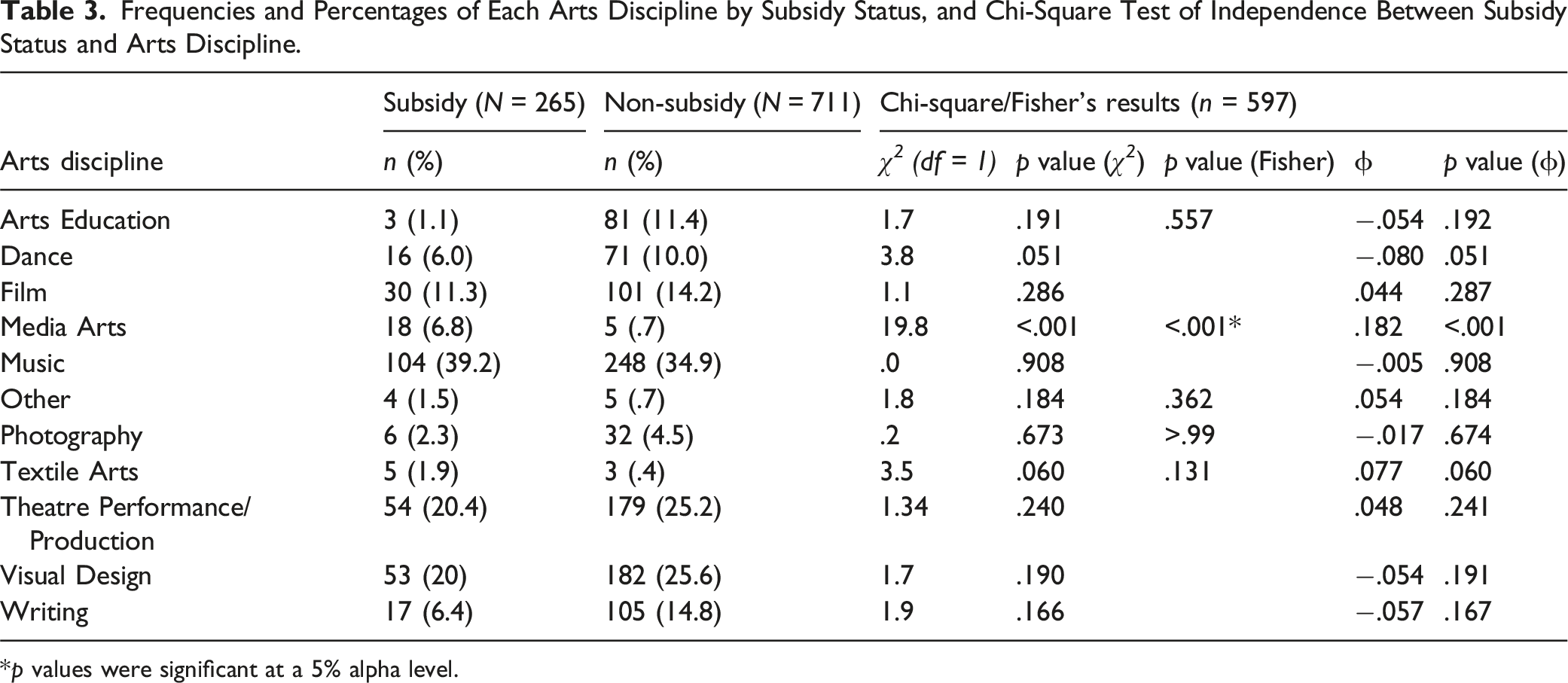
*p values were significant at a 5% alpha level.
Subsidy status and health conditions
Frequencies and Percentages of Each Mental Health Condition by Subsidy Status, and Chi-Square Test of Independence Between Subsidy Status and Mental Health Condition.
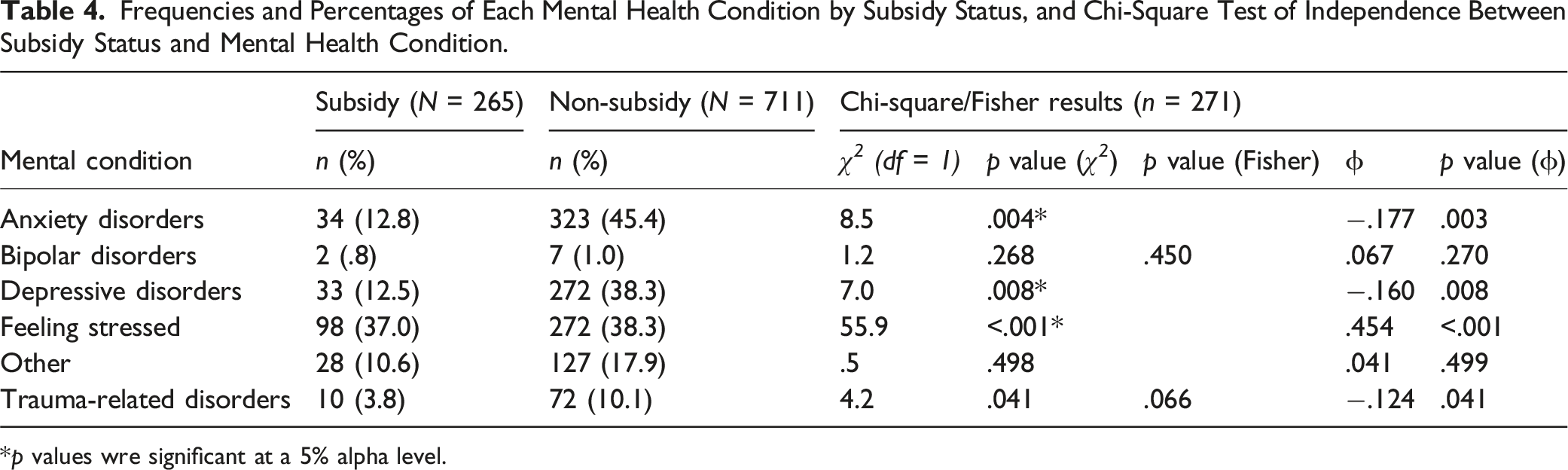
*p values wre significant at a 5% alpha level.
Frequencies and Percentages of Each Physical Health Condition by Subsidy Status, and Chi-Square Test of Independence Between Subsidy Status and Physical Health Condition.
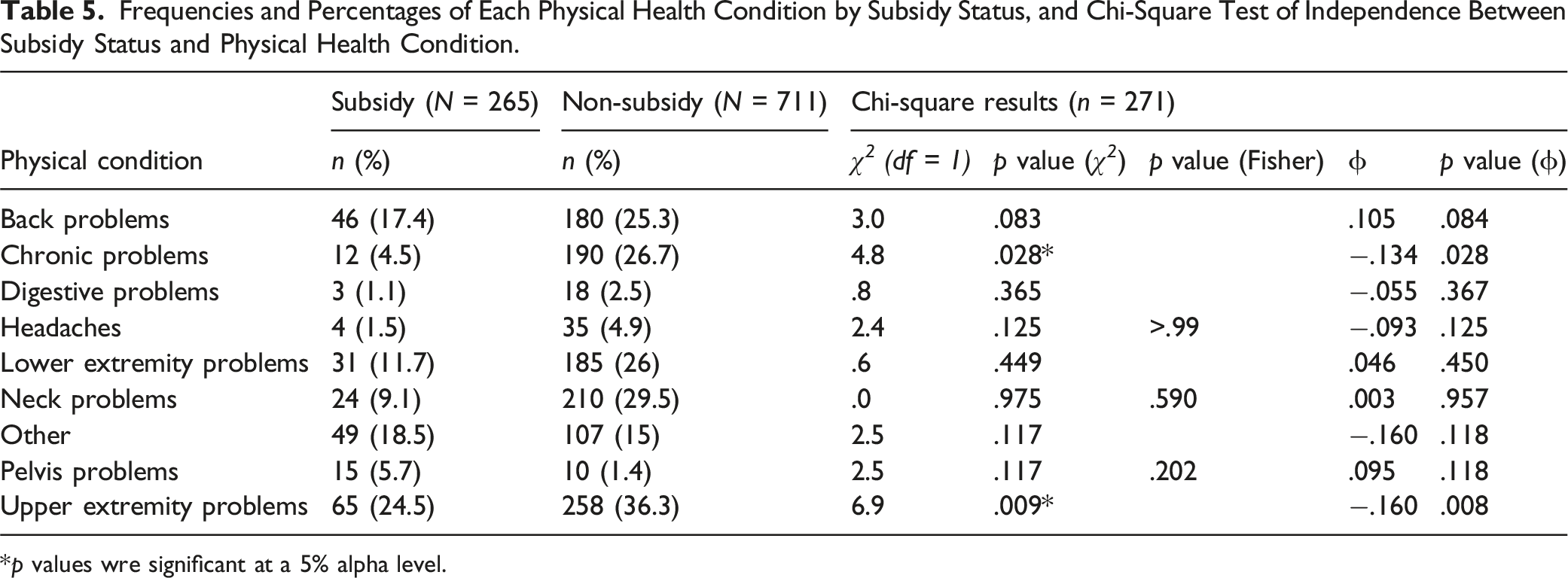
*p values wre significant at a 5% alpha level.
Multivariable Logistic Regression on the Influence of Subsidy Status on Type of Health Condition (Mental or Physical) After Controlling for Age, Gender, and arts Discipline (n = 175).
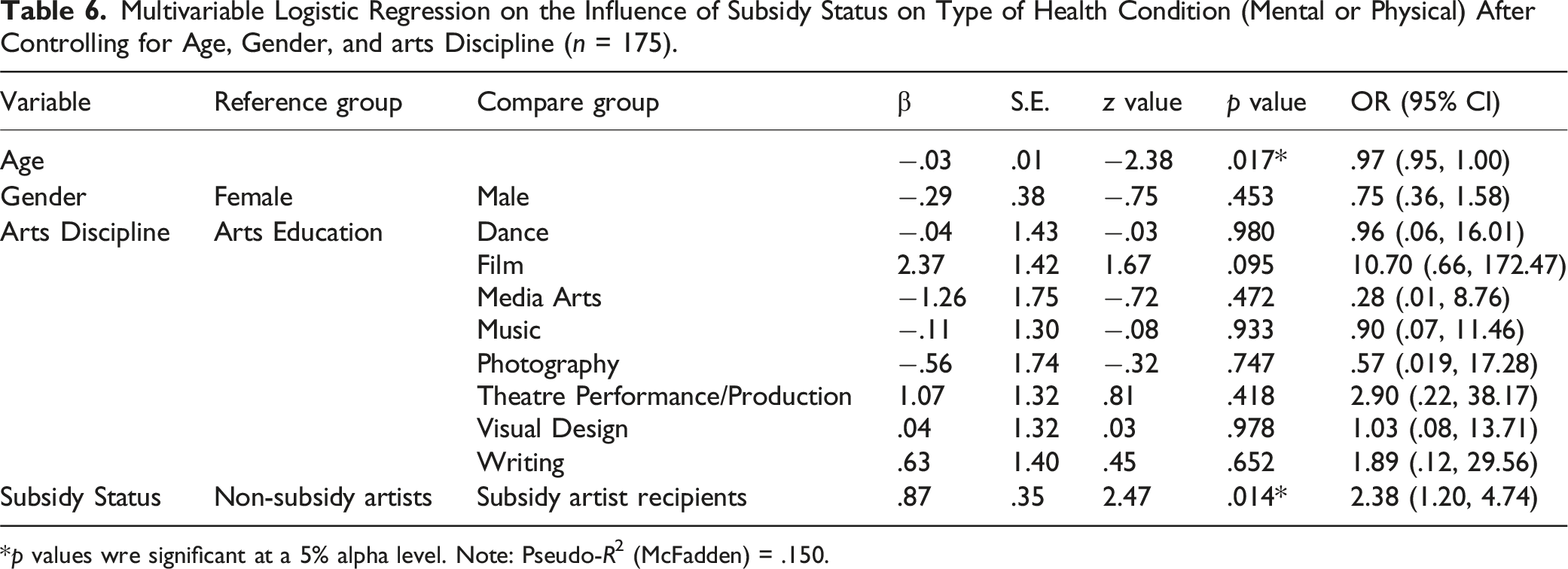
*p values wre significant at a 5% alpha level. Note: Pseudo-R2 (McFadden) = .150.
Subsidy status was moderately but significantly (p < .05; .30 ≤ |ϕ| < .50) associated with feeling stressed, and modestly but significantly (p < .05; 0 ≤ |ϕ| < .20) associated with anxiety disorders, depressive disorders, chronic problems, and upper extremity problems. SAs were more likely to seek treatment for stress, but less likely to seek treatment for anxiety disorders, depressive disorders, chronic problems, and upper extremity problems compared to NSAs. We observed a modest but significant (8.8 < χ 2 1 < 27.1, n = 786, p < .05; 0 ≤ |ϕ| < .20) association in the subsidy status and the number of health conditions sought for treatment. Compared to NSAs, SAs were more likely to seek treatment for one or two health conditions, and less likely to seek treatment for three or four health conditions.
In the multivariable logistic regression, subsidy status was the only factor significantly (OR 2.38, 95% CI 1.20–4.74, p < .05) associated with increasing the likelihood of seeking treatment for a mental health condition versus a physical health condition (Table 6). SAs are predicted on average to have 2.38 times the odds of seeking treatment for a mental health condition versus a physical health condition compared to NSAs, controlling for all other independent variables. The logistic regression model was statistically significant (χ 2 11 = 38.6, p < .05) and, based on the Hosmer-Lemeshow test, the model fits the data well (χ 2 11 = 6.2, p > .05).
Subsidy artist recipients: arts discipline and health conditions
Chi-Square Test of Independence Between Arts Discipline and Physical Health Condition for Subsidy Artist Recipients Only.
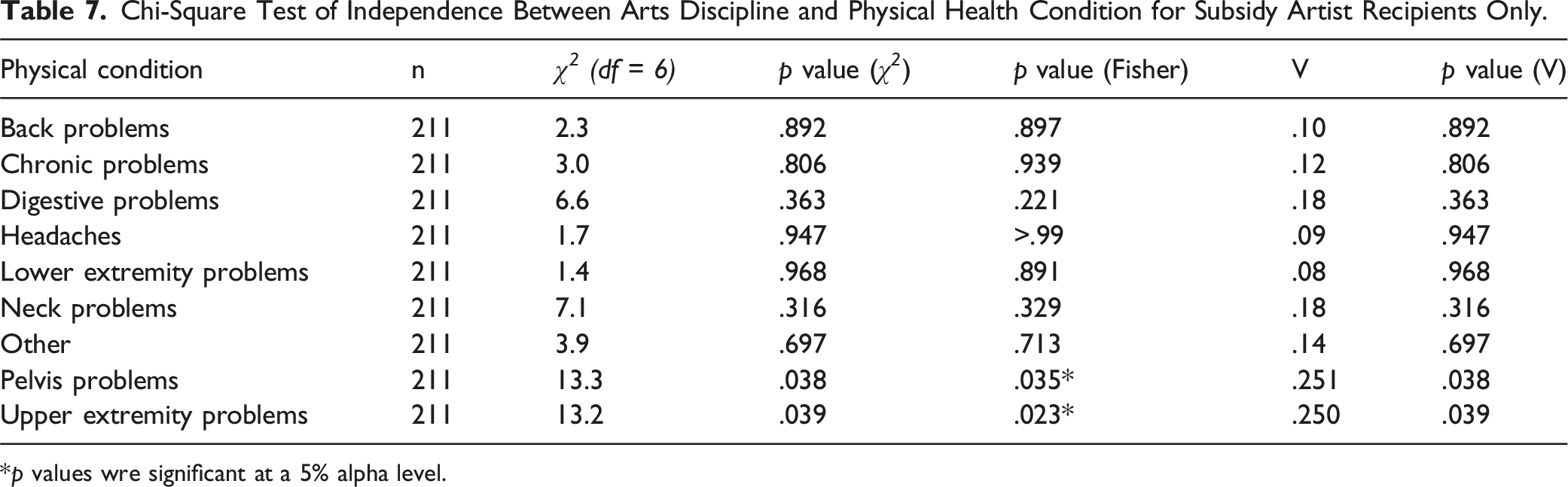
*p values wre significant at a 5% alpha level.
Subsidy artists recipients: impact of health conditions on daily functioning
Figure 1 shows the five scale items (scales A to E) used to evaluate the impact of health conditions on artists’ daily life. Of the 265 SAs, 215 responded; 1 recipient completed scales A to D and 214 recipients completed scales A to E. See Appendix 1 for the distribution of scores for each scale item and the domain represented by each scale. JSF ordinal scale item - Impact of injury on daily life.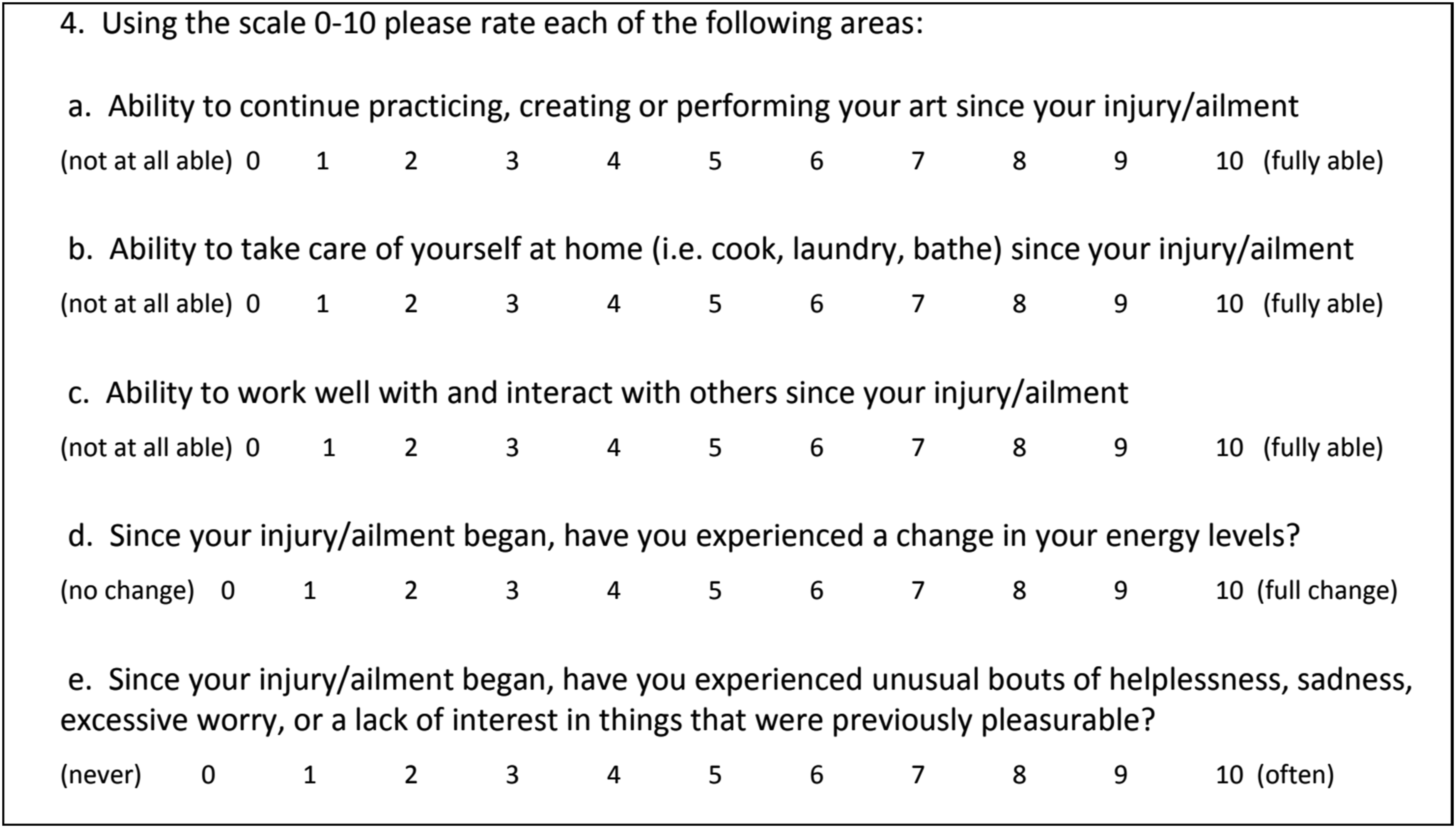
Self-identified gender, arts discipline, and score distribution
For all scales, there was no statistically significant difference in scores between art disciplines (2.8 < H < 11.4; na,b,c,d = 181; ne = 180; p > .05), and between males and females (4764.5 < U < 5669.5, na,b,c,d = 213, ne = 212, p > .05). Non-binary gender was excluded due to having only two observations that could lead to spurious results.
Scales A to C: ability
Half of the SAs selected a score of =<5 for A, =<7 for B, and =<6 for C. The median score of 5 for A suggests that SAs’ injuries impacted their ability to practice their art to some degree, and the median scores of 7 and 6 for B and C, respectively, suggest that SAs' health condition(s) had less impact on self-care activities (e.g., bathing, cooking, and laundry) and interaction with others.
Scales D and E: energy levels and negative mental state
Half of SAs selected a score of ≥7 for D and ≥8 for E. This suggests that a substantial portion of SAs experienced a considerable change in energy levels and an increase in negative thoughts towards activities that were previously pleasurable due to health concerns.
Discussion
Findings from this study suggest that: (1) musculoskeletal problems (back, upper extremities, lower extremities, etc.), stress, anxiety disorders, and depressive disorders are the most common health problems faced by SAs, which is consistent with other studies on artists4,17,18; (2) compared to NSAs, SAs are more likely to report feeling stressed and are predicted to be twice as likely to seek treatment for mental health versus physical health conditions; and (3) the injuries sustained by SAs tended to negatively impact their ability to perform daily life functions, with the largest negative impacts being an increase in negative thoughts about previously enjoyable activities, changes in energy levels, and less capacity to practice their art.
In our comparison between SAs and NSAs, SAs were more likely to seek treatment for mental stress, but less likely to seek treatment for anxiety disorders, depressive disorders, chronic problems, and upper extremity problems compared to NSAs. Gender and age are unlikely to be the reasons for this difference, since there was no significant difference in gender and age distribution between SAs and NSAs. Art discipline is also unlikely to be the cause, since both groups were highly similar in their distribution of arts discipline. Finally, it is unlikely that the detected difference in the media arts discipline played a part due to the small sample of participants in media arts discipline (n = 23, 2.4%).
Although our analysis indicates that there is no relationship between subsidy status and social determinants of health, this warrants further investigation due to our limited sample size for SAs (n = 20) versus NSAs (n = 151). Thus, we believe that social determinants of health having a larger effect on SAs’ ability to access treatment could possibly explain why SAs were more likely to seek treatment for stress compared to NSAs. Social determinants of health are social, economic, and physical factors that may affect an individual’s health, such as employment, education, income, housing, community, and race.19,20 Lower income,21–23 difficult working conditions,24,25 and precarious employment26–28 are all determinants that have been shown to be associated with increased mental stress. The aforementioned negative impacts of social determinants of health also tend to be associated with the artist population.4,9,29 Importantly, data for SAs were collected during the recent coronavirus disease 2019 (COVID-19) pandemic, while the data for NSAs were collected pre-pandemic. It is possible that the COVID-19 pandemic increased stress levels nationwide, amplifying the negative effects of these determinants. 30
It is also possible that social determinants of health still play a part in why SAs were less likely to seek treatment for anxiety disorders, depressive disorders, chronic problems, and upper extremity problems compared to NSAs. SDHs, such as race, 31 housing, income, and education, 32 have been shown to negatively impact healthcare use. In particular, lower income has consistently been shown to be associated with underuse of healthcare, typically through earlier discontinuation of treatment,33–35 and less monitoring or treatment visits.31,32 This underuse of healthcare can persist even in the presence of subsidized health services. 35 Additionally, comorbidities—various health conditions that are present at the same time—have been shown to increase out-of-pocket expenses for patients,36–38 strengthening the negative association between income and underuse of healthcare.
In Canada, the Ontario Health Insurance Plan covers appointment costs of family physicians who practice psychotherapy. Most patients who have at least one clinical psychiatric diagnosis are eligible. Therefore, this may explain the reason as to why more NSAs seek help for their clinical diagnoses (e.g., depressive disorder, anxiety disorder) compared to SAs. We also found that SAs were more likely to treat one or two health conditions, while NSAs were more likely to treat three or more health conditions. Because the JSF subsidy has a maximum of $760 for 12 months, it is possible that SAs prioritize their health conditions based on urgency and severity for treatment. This would correspond to Li & Donn’s (2022) 14 finding that the SAs’ need for consistency in treating their mental and physical health conditions, and their fear about running out of subsidies when they are making progress.
More research is needed to identify and address any additional disparities in health-seeking behaviors between SAs and NSAs. To effectively address the complexity of interactions between various social determinants of health and other influencing factors, such as workplace stigma and perceptions of biases or fears, and employment stability; it is essential to conduct future studies that specifically explore these areas. Qualitative research methods may provide a deeper and richer understanding of the artists’ perspectives on how the various social determinants of health may impact on their health-seeking behaviours. Qualitative studies could include in-depth interviews, focus groups, and case studies to explore the personal experiences of artists. These methods would allow researchers to capture nuanced insights into how artists navigate their health-seeking behaviors amidst challenges such as financial instability, lack of health insurance, and professional uncertainties.
Future research should also investigate the enduring effects of subsidized health services on SAs’ health outcomes. Sustained positive outcomes are crucial for maintaining an artist’s career and well-being, making this area of study particularly important. Longitudinal studies could track health outcomes over time, examining how continuous access to subsidized health services impacts physical and mental health, productivity, and career longevity. This would provide a comprehensive picture of the long-term benefits and any potential areas for improvement in the subsidy program. Additionally, researchers should assess the disparity in median income levels between SAs and NSAs, providing valuable insights for administrators and policymakers. By pinpointing a potential ‘trigger point’ where artists may struggle to afford health services out of pocket, we can better understand the financial thresholds that necessitate support. Quantitative data on income levels, combined with qualitative insights on financial stress and coping strategies, would inform the design of more effective subsidy programs.
Understanding this income threshold is essential for designing effective subsidy programs and drafting policies that support artists in maintaining access to necessary health services. Policymakers can use this information to ensure that subsidies are targeted to those most in need, thereby maximizing the impact of limited resources. Additionally, this knowledge can guide advocacy efforts to secure more comprehensive health coverage for artists, addressing systemic issues that contribute to their precarious employment and healthcare access.
By addressing these research areas, we can gain a better understanding of the long-term impacts and effectiveness of subsidized health services for artists. This knowledge will ultimately improve their access to healthcare and enhance their overall well-being.
Limitations
This study has potential limitations. The data collection instruments used to collect data from SAs and NSAs were different and not validated, and, as previously mentioned, data for SAs were collected during the COVID-19 pandemic, while the data for NSAs were collected pre-pandemic. Therefore, it is possible that the results are subject to measurement and response biases. The sample sizes between these two groups are also different, which may also lead to potential biases. The issue arises because statistical tests like chi-square and logistic regression consider the overall proportions or effects. As a result, small but practically meaningful differences in the smaller sample may be statistically nonsignificant, even if they have importance. In contrast, the larger sample sizes may lead to the detection of even the smallest difference by the chi-square test. Finally, the sample was drawn from a single medical facility in one geographic location. Findings may not be representative of the overall artist population.
Conclusion
As demonstrated by Li & Donn (2022), 14 the subsidy removes barriers to accessing paid health services that are otherwise unattainable among artists who demonstrate a financial need. The findings presented in this study further contribute by providing a contemporary view of the most utilized health services by SAs (and NSAs). This can be useful to policymakers and health service providers in determining which health services to prioritize to ensure that more artists are receiving the care they need for their conditions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Subsidy artist recipients: ability to function due to health condition.
A – Ability to continue practicing, creating or performing your art since your injury/ailment B – Ability to take care of yourself at home (i.e. cook, laundry, bathe) since your injury/ailment C – Ability to work well with and interact with others since your injury/ailment D – Since your injury/ailment began, have you experienced a change in your energy levels? E – Since your injury/ailment began, have you experienced unusual bouts of helplessness, sadness, excessive worry, or a lack of interest in things that were previously pleasurable? a/b – “Not at all able”/“Fully able” (scales A to C), “No change”/“Full Change” (scale D), or “Never”/ “Often” (scale E).
Scale A (n = 215)1
Scale B (n = 215)2
Scale C (n = 215)3
Scale D (n = 215)4
Scale E (n = 214)5
Rating
Freq
% Total
Freq
% Total
Freq
% Total
Freq
% Total
Freq
% Total
0a
10
4.7
0
.0
0
.0
2
.9
1
.5
1
9
4.2
5
2.3
3
1.4
8
3.7
6
2.8
2
17
7.9
9
4.2
10
4.7
9
4.2
12
5.6
3
27
12.6
13
6.0
23
10.7
11
5.1
8
3.7
4
36
16.7
24
11.2
19
8.8
20
9.3
9
4.2
5
34
15.8
21
9.8
36
16.7
25
11.6
20
9.3
6
28
13
32
14.9
46
21.4
24
11.2
17
7.9
7
28
13
37
17.2
34
15.8
32
14.9
27
12.6
8
17
7.9
17
7.9
12
5.6
39
18.1
29
13.6
9
5
2.3
13
6.0
12
5.6
22
10.2
19
8.9
10b
4
1.9
44
20.5
20
9.3
23
10.7
66
30.8
Missing
50
50
50
50
51
Total
265
100
265
100
265
100
265
100
265
100