
Abstract
Background
Racial/ethnic disparities in maternal and infant morbidity and mortality (MIM&M) is a wicked problem that is reinforced and perpetuated by our system[s] of care. Life Course Theory (LCT) helps to explain drivers of health disparities, but its application is challenged. An upstream approach that promotes systemic change requires the implementation of an expanded prevention framework that includes primordial and quaternary prevention.
Research Design
We developed an innovative expanded Whole System Prevention Framework (WSPF) that incorporates LCT, prevention (including primordial and quaternary prevention) and systems thinking.
Study Sample
We implemented this new conceptual Framework with two Healthy Start community partnerships through training, service mapping, and strategic planning to address upstream drivers of MIM&M.
Data Collection and Analysis
Service mapping revealed few Healthy Start upstream activities/services with the predominance being delivered downstream at the program (microsystem) level.
Results
Service mapping provided a snapshot of the current service distribution of services across the systems. The preponderance were primary, secondary and tertiary prevention activities (75.5% and 65.6%) delivered at the program level (58.2% and 68%), revealing opportunities for upstream strategies to promote equity. The implementation process provided a new way to frame strategic planning and develop upstream strategies to promote health equity and reduce MIM&M.
Conclusion
The Whole System Prevention Framework and its implementation methodology could be applied to address other wicked problems.
Keywords
Introduction
Maternal i and infant morbidity and mortality (MIM&M) is a “wicked” problem. As such, its etiology is socially or culturally entrenched and its solution escapes us - a single solution is insufficient and the effectiveness of multiple solutions in concert is unknown. A wicked problem is characterized by the enmeshment in other social and cultural problems, and the significant economic burden it poses. 1 These factors, in addition to complexity and long-time horizons for intervention outcomes, pose barriers to addressing wicked problems. The current system often reinforces and perpetuates contributing factors – or root causes – resulting in continued and sometimes growing racial/ethnic disparity gaps in MIM&M.
Disparities in Maternal and Infant Mortality and Morbidity in the United States.
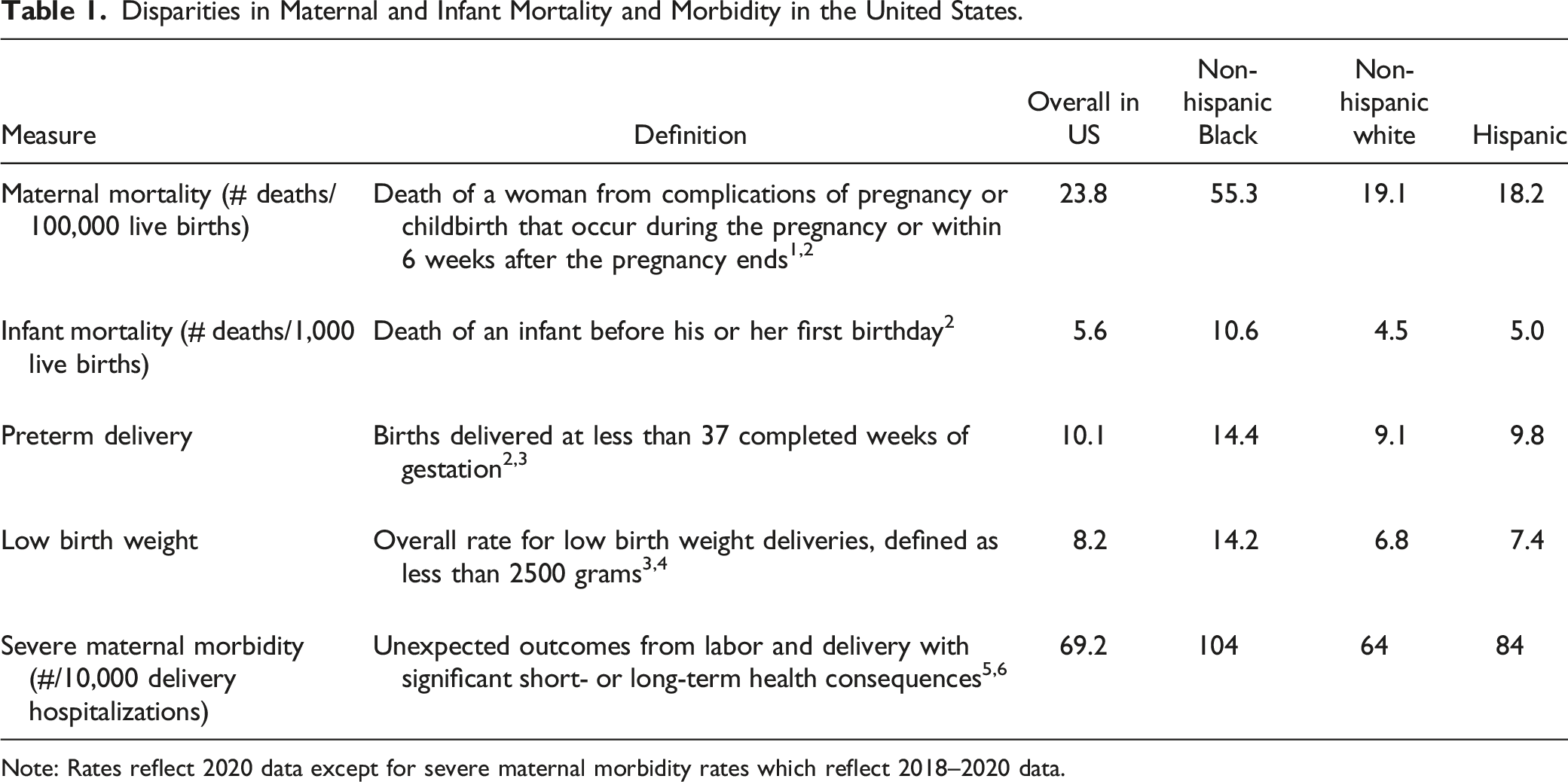
Note: Rates reflect 2020 data except for severe maternal morbidity rates which reflect 2018–2020 data.
Drivers of MIM&M include a myriad of social and structural determinants rooted in “systemic racism that perpetuate inequities in the health care system” and manifesting as, for example, barriers to care and chronic health conditions 6,p. 2, to name but a few. Social determinants of health are the conditions in which people are born, grow, live, work and age. 7 Addressing social determinants is essential to promoting health equity as social context affects delivery of services and related outcomes. However, while addressing social determinants is essential, it alone is not adequate. Structural determinants - cultural norms, policies, institutions and practices that drive the distribution of social determinants and shape the distribution of power and resources – must also be addressed. 8 Persistent health inequities along racial, gender and class lines are rooted in these structural determinants; eradication of inequity requires addressing historical, systemic forces that generate and sustain risk factors that manifest as health inequities. Such an approach appropriately shifts accountability for health inequities from the individual to the system.
Despite this appropriate shift, and ample data demonstrating persistent racial/ethnic inequities in MIM&M outcomes, public health continues to predominantly develop and promote interventions targeting downstream individual behaviors. 9 A framework that enables analysis of the whole system, identifying where types of interventions are implemented within each system level and how they complement each other, is not being applied in the field.
Application of a Whole System Prevention Framework
In 2021, the federal Health Resources and Service Administration (HRSA) funded twenty-one Healthy Start programs to work with their Community Action Networks (CAN) iii to develop strategic plans to address upstream drivers of MIM&M to reduce racial/ethnic disparities in perinatal health. 10 The purpose of the Healthy Start program is to reduce disparities in infant mortality and adverse perinatal outcomes in communities with infant mortality rates at least 1.5 times the U.S. national average and high rates of other adverse perinatal outcomes (e.g., low birthweight, preterm birth, maternal morbidity and mortality). 10 Healthy Start works to reduce the disparity in health status between the general population and individuals who are members of minoritized racial or ethnic populations, through a life course approach that emphasizes women’s health, family health and wellness, and community/population health.11,12
A recent evaluation of the Healthy Start program which included data from 32,233 participants found that participants were primarily below the age of 35 years old (87.6%), identified as Black or African-American (60%), had a high school degree/GED or less (69.4%), and health insurance coverage through public insurance, such as Medicaid (89.2%). The majority live below the federal poverty level (56.1%), and 45% have an annual income of less than $10,000. Most participants (51.6%) are prenatal. 13
Healthy Start programs operate at the individual and community levels within urban and rural areas. At the individual level, programs provide a range of direct services (e.g., home visits, reproductive life planning, and care coordination/case management). At the community level, programs work with multi-sector partnerships (Community Action Networks) as an approach to systems change. 10 The Community Action Networks (CANs) help fulfill one of the program’s core elements to promote systems change: activities to maximize opportunities for community action to address social determinants of health (SDOH), including systems coordination and integration among health and social services, other providers, and key leaders in the community and their states. 10 These multi-sector partnerships are essential to an expansive approach to identifying upstream drivers and responding with multifaceted strategies/solutions. 9 Understanding and ameliorating the causes, persistence, and temporal aspects of racial/ethnic disparities in MIM&M calls for a comprehensive approach incorporating multidisciplinary integrative strategies, complementary methods, quality population-level data, longitudinal cohort studies and intensive resources.9,14,15 It is an approach that is equal to the complexity of this wicked problem.
This manuscript describes the efforts of two Healthy Start programs and their collaborators to accomplish this specific task, and provides a larger framework for other community-based initiatives addressing MIM&M and potentially other wicked problems. Specifically, this paper first introduces a new combined theoretical framework, the Whole System Prevention Framework (WSPF), underpinned by three integrated frameworks: Life Course Theory,14,16–23 prevention thinking,24–33 and systems thinking.34–39 Then, it describes the application of the WSPF within the two local Healthy Start communities, focusing on systems mapping and strategic planning. And finally, it suggests policy and practice implications for the broad field of public health including maternal and child health.
Conceptual Frameworks
The following section presents Life Course Theory, prevention thinking and systems thinking. Combined, the three conceptual frameworks contribute to the development of a new integrated framework, the Whole System Prevention Framework (WSPF). WSPF takes into account the dynamics of a complex world and the need to address upstream drivers of disparities to achieve health equity.
Life Course Theory
Life Course Theory (LCT) is concerned with the cumulative impact of exposure to social and structural determinants of health (SSDoH) over one’s life span.19,23 Exposures (or experiences) occurring over time chart pathways/trajectories that become key contributors to health outcomes - both positive and negative - as protective factors and adversities. LCT answers two questions: (1) Why do racial/ethnic disparities persist across population groups? And (2) What factors influence the capacity of individuals or populations to reach their full health potential? These equity-based questions focus the inquiry on social and structural factors as determinants enabling or inhibiting health rather than misplacing accountability for disparate health outcomes on individual choice or behavior.
Organizing Principles of Life Course Theory, Description, and Examples.
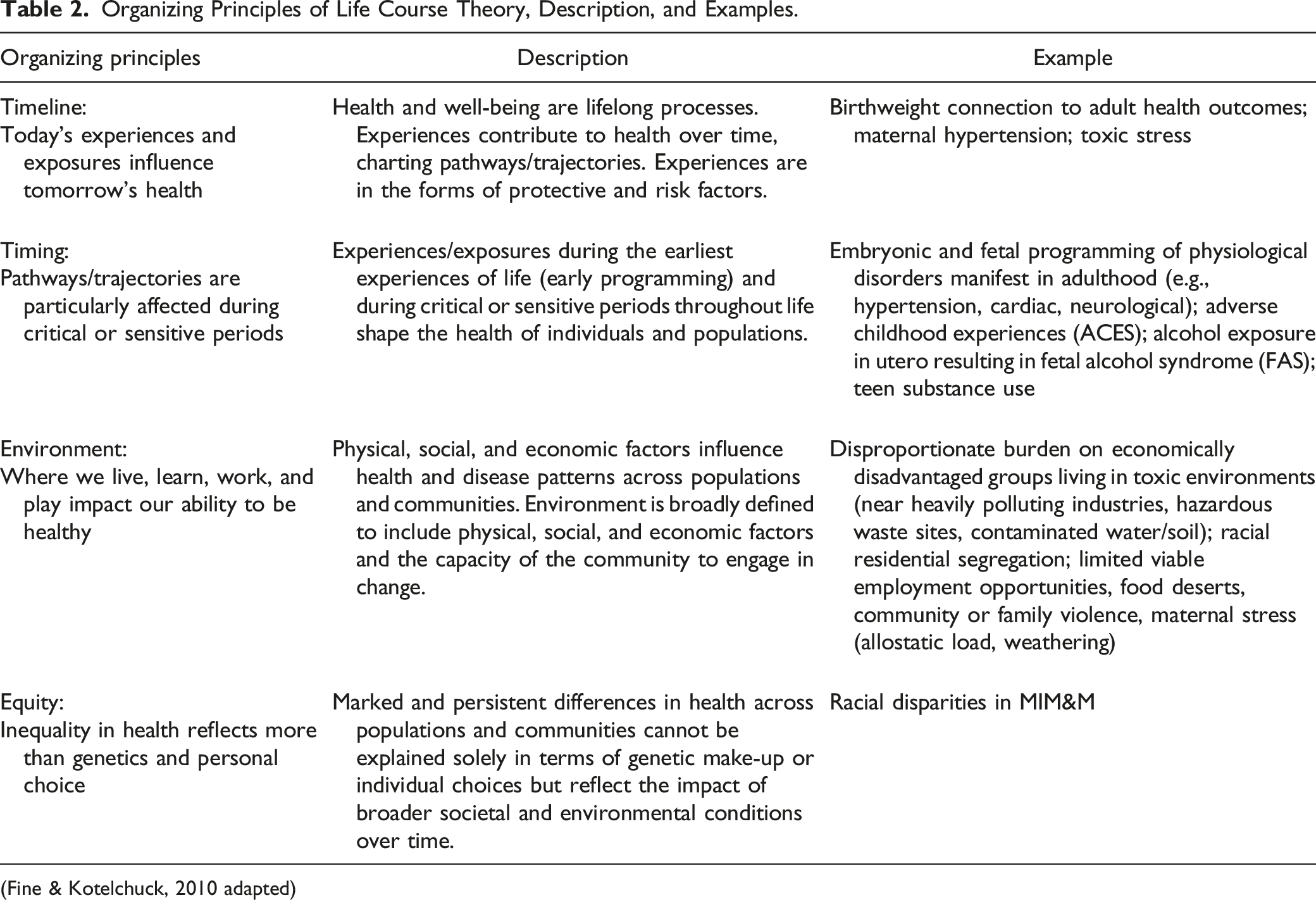
(Fine & Kotelchuck, 2010 adapted)
LCT has been used to examine several wicked public health issues, including chronic disease, 16 injury prevention, 20 nutrition, 22 substance use, 40 maternal health, 17 and birth outcomes.23,41,42 Although LCT provides explanation for how a wicked problem(s) exists and persists, LCT remains primarily an epidemiological and conceptual theory, challenged by limited feasible applications. 16 Its application is hindered by entrenched approaches to research siloed by discipline and funding, health system fragmentation, lack of integrated medical and public health approaches, and the complex challenges of linking social constructs to biological manifestations.14,18
While public health recognizes that adversities experienced over a lifetime (and even generations prior) accumulate to impact health outcomes, most strategies and interventions continue to limit their focus on ages and stages - specific periods such as pregnancy, infancy or early childhood development. In 2010, Fine and Kotelchuck issued a call to the maternal and child health community to not let LCT lay fallow, but to “realize LCT’s promise”,19,p.15 through dialogue to translate this not-so-simple theory into new and innovative practices, programs and policies.
Prevention Thinking
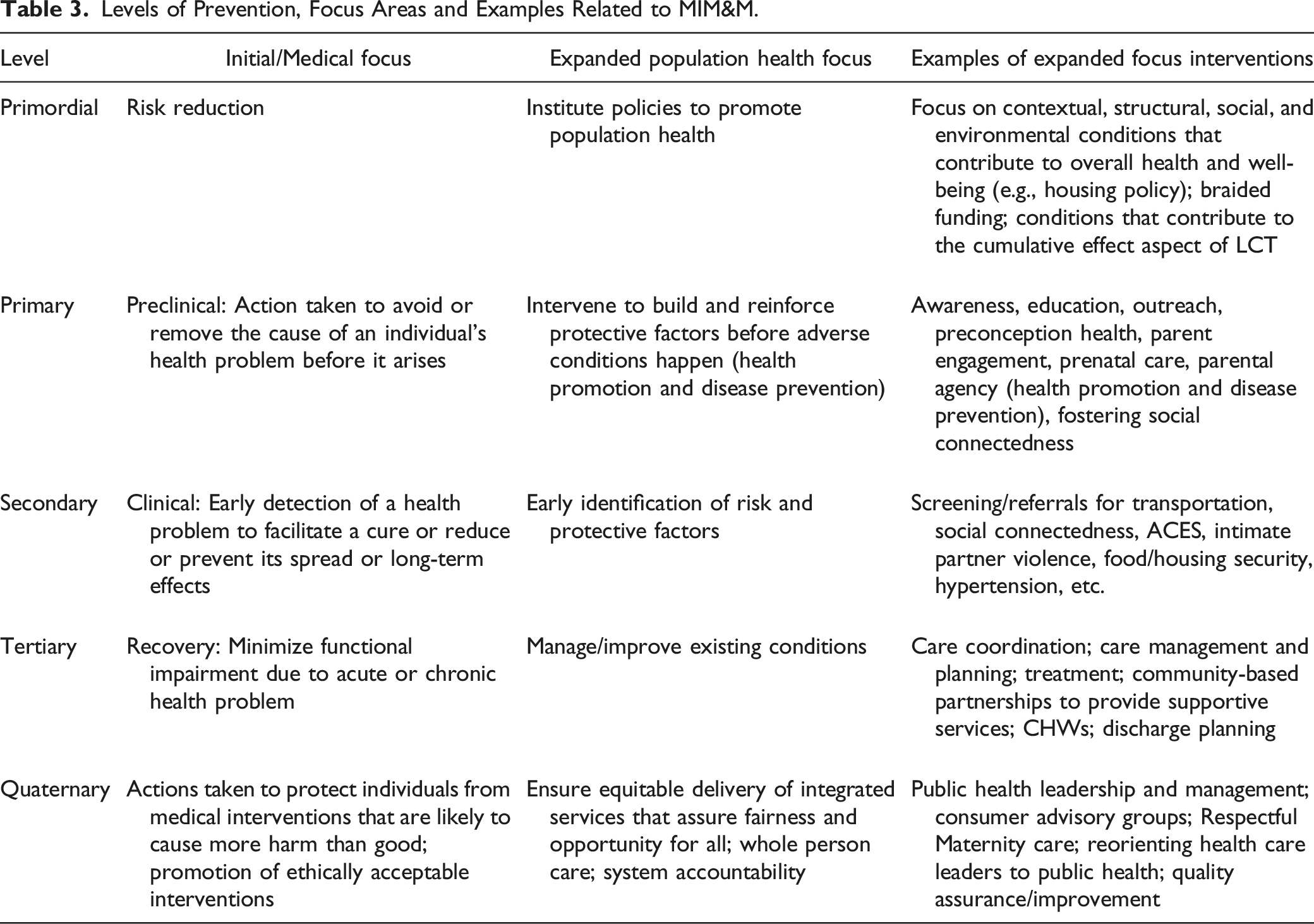
Traditional prevention levels organize primary, secondary, and tertiary prevention activities sequentially according to disease phases - preclinical, clinical, and recovery - focusing respectively on increasing awareness and prevention of disease before it occurs, early identification of disease, and prevention of further harm when disease is identified. 32 The levels of prevention have been expanded more recently to include primordial and quaternary levels,27,28 addressing limitations in the traditional medical-focused prevention model.
A primordial level was initially introduced in the context of preventing cardiovascular disease through interventions that prevent the penetration of risk factors into the population. 30 This expanded focus recognized the role of SSDoH in exposure to adversities that generate, perpetuate and compound health inequities. 33 Such factors include health-damaging exposures, susceptibilities, and limited health protective resources among the population. Primordial factors also encompass the effects of intergenerational trauma and “fetal programming of chronic diseases” - or changes in patterns of fetal development resulting from maternal exposures, such as malnutrition - that are linked to later development of cardiovascular, endocrine, and neurological effects in the child. Primordial prevention targets “upstream” SSDoH to reduce risk exposure, often through policy, expanding the individual-focused disease-based perspective to encompass a multifaceted population prevention focus. 43 Primordial factors provide the underpinning for LCT - establishing the context that generates societal protective factors and adversities that set the stage for an individual’s life trajectory.
The quaternary level is a relatively new concept in prevention, and a paradigm shift from a chronological pattern of medical care (primary, secondary, tertiary), to a relationship-based pattern of care.24,25 Initially conceived in the context of medicine, specifically the doctor-patient relationship, it is grounded in the concept “First, do no harm”. 31 In its initial conceptualization, quaternary relates to patient protection and the prevention of overtreatment or over-medicalization, in other words, harm to individuals resulting from their interface with the healthcare system. Quaternary prevention represents a shift in two dimensions. The first dimension shifts from a chronologic disease-oriented concept to one that is contextually based and grounded in LCT - a whole person approach. The second dimension transcends accountability beyond the individual relationship between provider and patient to include the system at large.
Quaternary prevention incorporates an additional layer of preventive intervention that touches each other level. 26 For example, the 2017 World Health Organization (WHO) standards for “quality of maternal and newborn care” elucidated the concept of Respectful Maternity Care by ensuring that several of the standards underscored “respect, dignity, emotional support, and a systemic commitment to a patient-led, informed decision-making process”. 29 In this example, “listen[ing] to the patients”, and applying “narrative-based medicine” to adapt medical intervention to the needs and wants of the individual. 28 Additionally, providers have both a professional and moral obligation to practice evidence-based medicine that ensures informed decisions and best practice. Quaternary prevention blends and balances each of these dimensions to assure that the best knowledge is applied, which aligns with whole person care. From our expanded perspective, quaternary prevention is concerned with mitigating or avoiding adverse outcomes resulting from an individual’s interface with the system of health care and social services, such as from obstetric racism resulting in inequities in birth and birthing person outcomes.44,45
Quaternary prevention activities directly address the issue of equity, viewing the role of the system of care itself as causative in reinforcing or mitigating adversities and introducing protective factors. Health equity “... is achieved when every person has the opportunity to attain [their] health potential, and no one is disadvantaged from achieving this potential because of social position or other socially determined circumstances”. 46 Public health surveillance, implementation of contextually and structurally relevant strategies, and quality improvement and assurance facilitate quaternary prevention efforts to achieve health equity. 47 The sum of these strategies is quaternary prevention’s function; to hold the system accountable for providing equitable services. Quaternary is the system’s conscience.
Levels of Prevention, Focus Areas and Examples Related to MIM&M.
Systems Thinking
Systems thinking applies systems principles to understand the way the world works and fits conceptually with LCT as a way to understand how life experiences produce context-dependent health outcomes. Systems thinking examines the dynamic interactions between parts of the system of care, including how consumers interact with and are impacted by it.39,48,49 And like LCT, systems thinking recognizes that causal linkages between events and outcomes may not be apparent because of long time horizons. Systems thinking accounts for complexity and offers a strategy to address wicked problems.34,48,50
Systems exist as a set of embedded and hierarchical, dynamical, and living networks. One way to conceptualize a “system of care” is considering the level at which direct care or services are provided, the level at which various community-based organizations or programs work together to provide coordinated services, and the level at which policies determine the allocation of resources and the administration of regulations related to services. These can be viewed as corresponding to the micro-, meso- and macrosystem levels describing the health care system. These levels operate interactively through vertical connections; each level with a specific role that contributes to the function of the whole system. 39 The application described here expands this model beyond the health care system to incorporate a broader context that includes the SSDoH. Multiple microsystems are embedded in a mesosystem, and multiple mesosystems are embedded in a macrosystem.39,48 Examining systems structures and functions, and the relationships between various components, provides an approach to identify where interventions are occurring or can occur. Each of these systems levels, and their functions are described below.
Macrosystem Level
At the macrosystem level, policy decisions are made38,39,48,50 that directly impact social and structural determinants, including access to healthcare and medicines; access to safe and affordable housing; economic opportunities; quality education; reliable public transportation; and availability of healthy, affordable food. Governmental agencies and institutions develop and administer policies and resources that impact meso- and microsystems, by establishing (among other things) funding priorities, determining performance measures for funding, and regulating adherence to policies. Professional associations establish guidelines, and promote evidence-based practices, which in turn drive licensing requirements, and training needs of service providers.
Examining existing services provides an understanding of which services are funded, and the nature of funding: siloed, braided, or blended. Siloed funding at the macro level does not allow for or accommodate the need for connected and coordinated services at the meso level to deliver whole person care that addresses a range of social and health needs at the micro level. Braided funding strategies allow for the joint utilization and coordination of funds from various sources and allocate them together for services, but maintaining specific tracking and accountability for each source. Blended funding strategies merge dollars from various sources into one pooled funding stream, from which funds are then allocated for needed services.51,52
Mesosystem Level
The mesosystem, comprised of multiple microsystems,39,48,50 functions to ensure that social determinants are addressed across the continuum of care and services within a community. At this level, organizations across the community that provide services establish relationships with one another through horizontal connections between community organizations to ensure that referral pathways are in place to meet the needs of their clients, and to communicate the needs of their clientele to community partners. The mesosystem level achieves its goals by building an effective, responsive continuum of care and services that adapts to the community’s changing needs. It contributes to community assessments to ensure that equitable reproductive health is identified and maintained as a community priority, and advocates for reproductive justice.
Vertical connections that facilitate bidirectional data utilization between the microsystem level (service delivery, quality and access) and the mesosystem level (surveillance of population needs and racial/ethnic disparities) should inform policy decisions and shape a political agenda at the macrosystem level for a whole system approach. Effective organizations identify, recruit, and support the development of individuals representative of the population to meaningfully participate in the continuous quality improvement of a program or an organization through consumer advisory boards, focus groups and/or more informal feedback opportunities. An effective mesosystem depends upon diverse multidisciplinary partnerships that represent a broad array of services that meet the unique needs of the community.
Microsystem Level
The microsystem level is where the rubber meets the road. It is the point of intersection between a system and individual,39,48–50 where direct service providers establish relationships and assess, educate, and provide trauma-informed, culturally competent, and person-centered preventive services. Organizations and programs ensure adequate staffing levels, with staff who have the training and resources needed to provide whole person, trauma-informed care through the implementation of care models that recognize and address racial/ethnic disparities. 53 Changes at the micro level include providing technical assistance to enhance staff capacity and ensuring that mechanisms are in place to refer clients, as appropriate, to community partners. Microsystems are well positioned to implement and test small scale system interventions, challenge how services are delivered, and gauge responsiveness and effectiveness. The microsystem is best positioned to gauge the effectiveness of large order system change through its person-level interaction with the system on a daily basis. The next section presents an example of putting the WSPF into action to understand and address racial/ethnic inequities in MIM&M.
Development of the Whole System Prevention Framework
The HRSA funding underlying this manuscript required a focus on upstream drivers of racial/ethnic disparities in MIM&M, and served as a catalyst to developing a new model that the CANs could and would use. The WSPF (Figure 1) emerged through this process, and incorporates and crystallizes its three critical components - life course, prevention thinking, and systems thinking. Whole System Prevention Framework.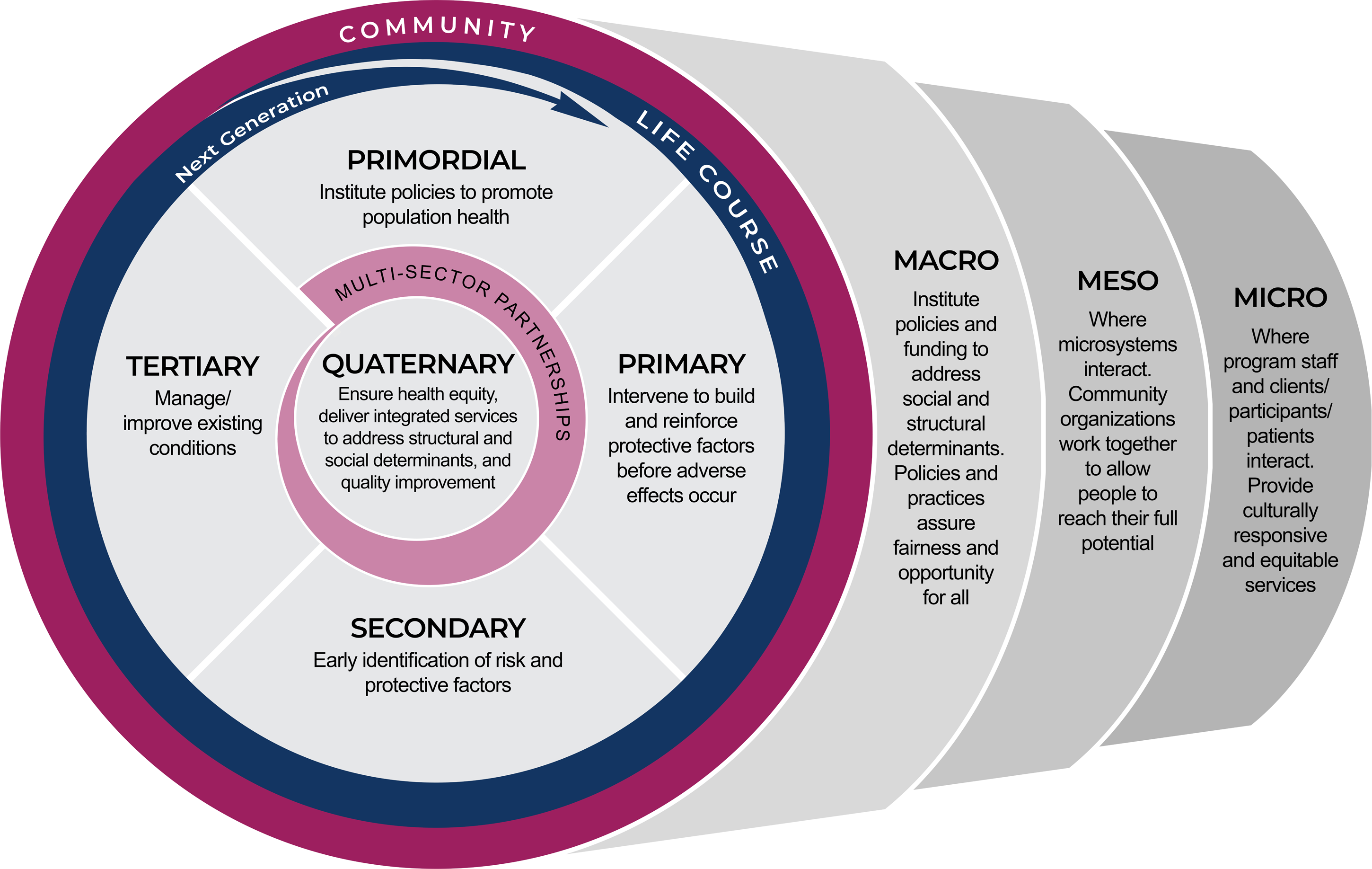
The WSPF is predicated on the principles of LCT; ongoing non-linear, dynamic experiences occur over time, and include interrelated protective factors and adversities which impact individuals, families and future generations. Life course occurs within the context of community – where inequities manifest as a result of the dynamic interactions and experiences with SSDoH - and where contextually-relevant solutions can be applied.
The framework depicts the context as the outer “Community” band. The placement of the “Life Course/Next Generation”, the circular arrow-headed band, is situated immediately inside the “Community” band to communicate the ongoing, cumulative experiences of individuals and families occur over time within the context of the community. The arrow represents the long-term, cumulative life course influences over time and across generations - for example, the reinforcing and amplifying effects of generational poverty. Both bands theoretically encapsulate all public health interventions organized by level of prevention, populating the center of the sphere.
The WSPF incorporates the expanded levels of prevention – beyond primary, secondary and tertiary, to include primordial and quaternary. Primordial and quaternary prevention are important additions to prevention thinking, each with a specific function in addressing upstream factors, introduces a new way to actualize population health equity.
The “Multi-Sector Partnerships” band encapsulates the quaternary prevention component at the center of the framework. Preventive interventions that touch all points along the life course are identified and informed through ongoing community engagement, thereby ensuring implementation within the community context that is tailored to the unique needs of its population. The tapered width of the “Multi-Sector Partnerships” band indicates that primordial (environmental/policy) and primary (awareness/education) level interventions target a broader segment of the population, while secondary and tertiary interventions target individuals or a more narrow, segment of the population experiencing greater health complications.
The multidimensional systems components, macro-, meso-, and microsystem levels, complete the framework. Systems thinking is a huge body of knowledge with many conceptual models; the traditional model described here, incorporating macro-, meso- and micro systems levels, enables a practical application that enabled the CANs to grasp and apply the critical concepts, generating a shared understanding of their system of care and services.
The lens through which the system is viewed is prevention. The telescoping represents the nested structure of systems, depicting each of the levels separately, and the whole system, at once. The size of each system level reflects its respective sphere of influence. The macro level has a broader sphere of influence, as it contains meso- and microsystem levels, while the micro level sphere of influence is the most narrow. The nested nature facilitates connection between each level to the other. System levels interact with each other and with prevention interventions. A whole system approach suggests that a range of preventive interventions occur at each system level, and across the life course to address current/existing population needs while laying the groundwork for the public health of future generations. The result is a whole system approach to developing an upstream plan for rewiring systems (through system alignment or integration) with deeply rooted inequities that perpetuate racial/ethnic disparities including MIM&M.
By tethering LCT to prevention thinking and systems thinking, the WSPF enhances LCT’s practical usability and provides focus for interventions to eradicate MIM&M racial/ethnic disparities through a whole system application of an expanded levels of prevention framework. The resulting WSPF suggests opportunities for influencing life course trajectories with interventions that span the entire system of care, thereby activating life course theory. The WSPF guided a whole system assessment that examined where and how adversities could present within each system and prevention level, and where opportunities for mitigation might exist. The next section presents two examples of putting the WSPF into action to understand and address racial/ethnic inequities in MIM&M.
Application Methodology
In response to the HRSA Eliminating Disparities in Perinatal Health funding opportunity, the Southern New Jersey Perinatal Cooperative (SNJPC) Healthy Start program and The Foundation for Delaware County (TFDC) Healthy Start program engaged JSI Research and Training Institute, Inc. (JSI) to provide training and technical assistance (T/TA) to their respective CANs to support their upstream community-based MIM&M strategic planning. The process described in this manuscript exemplifies the standard of community engagement - widely recognized as an essential factor in promoting health equity.9,14,54,55 The process used the new Whole System Prevention Framework to implement a fresh approach for understanding how an individual organization (a member of the CAN) fits into the larger system of care – in this case, community-based MIM&M reduction efforts - and generating a visual representation that highlights where coordinated efforts could strengthen the system of care’s upstream efforts to reduce racial/ethnic disparities in MIM&M.
Both Healthy Start communities, having worked with JSI in prior years on a leadership and system improvement initiative, recognized that a new systems approach was necessary to develop new upstream programmatic thinking and programming to address MIM&M. The two sites had previously engaged their CANs to address MIM&M; and they each had completed an environmental scan including focus groups and key informant interviews, which included review and interpretation of public health surveillance data. This initial work of the CAN provided the springboard for the iterative mapping and strategic planning process - the new work with JSI - and the focus of this paper. This process spanned the months of September 2021 to March 2022. The project was determined as exempt by the Institutional Review Board.
Shifting the Paradigm through Training
The two Healthy Start programs funded to address upstream MIM&M engaged JSI for T/TA in systems thinking and health equity. Building on previous systems thinking training with Healthy Start programs, JSI first developed an original iterative training approach that oriented CAN members to Life Course Theory (LCT) to understand racial/ethnic disparities, prevention thinking to guide the focus of public health interventions, and systems thinking to explain how system behaviors actually perpetuate adversities (SSDoH), and consequently health disparities. This training provided the necessary foundation for targeted upstream strategic planning, pivoting CAN members’ tendency to focus on direct service and individual behavior change, and cultivate a fuller contextual landscape that promotes optimal population health.
Training on the components of this new dynamic strategic framework (the WSPF), was provided through a sequence of meetings held with each Healthy Start CAN. Each CAN convened a subgroup of its members for this specific HRSA funded project that served as the project’s advisory group. Training content was shared with the advisory group prior to meeting with the larger CAN. Based on their feedback, adjustments were made regarding language and flow to increase accessibility to the information for each respective CAN. The iterative, collaborative learning that occurred allowed CAN members to shift their focus from their respective organization’s delivery of programs and services to their role within the larger system of care. What transpired was a greater depth of comprehension of dynamic relationships between system of care components and how each program (CAN member organization) might contribute to the perpetuation of adversities. The trainings delivered on the WSPF laid the groundwork for the system assessment to map the local system of care for MIM&M reduction.
Mapping the System of Care
As a part of the system assessment, JSI developed a WSPF worksheet (Identifying System Level Interventions through the Life Course Lens iv ) for individual members of each Healthy Start CAN to describe their program/organization and list specific activities/services that focus on promoting both infant and/or maternal health. Each CAN member organization was asked to complete the worksheet indicating prevention and system level for each identified service. JSI provided detailed instructions. Some organizations were able to identify prevention and/or system level(s) to correspond to each activity/service, some only listed their program or organization’s activities/services. Completed worksheets were submitted to JSI for analysis.
Each worksheet was then reviewed by two JSI team members for concurrence in prevention level and system level assignment based on the definitions outlined in the matrix (Figures 3 and 4), and coded by prevention and system level. For additional insight into program/organization missions, JSI staff reviewed CAN member organization websites and spoke with the CAN coordinator for confirmation. When activities/services fell into more than one level (e.g., Family planning clinic provides advice on sexual and reproductive health, prevention and options with unplanned pregnancy, and was categorized as primary, secondary and tertiary prevention services at the micro level) the activity/service was counted in all applicable cells. Variances were discussed to reach consensus. When applicable, JSI noted suggestions for how activities could be expanded to other system levels, thus providing another level of T/TA.
JSI then returned the coded worksheets to the CAN Coordinator who distributed them back to their appropriate programs. Each program completed a final review to ensure accuracy as well as understanding of the system and prevention levels that JSI had assigned to their respective program activities and services. This step also served as another CAN training activity (e.g., consensus and final approval by each CAN member organization of the joint worksheet), and it served as the data points for the JSI summary of their collective efforts. Interventions were then aggregated, mapped to a matrix (Figures 3 and 4), and shared with the CANs. Analysis ultimately yielded a depiction of whole system prevention services for each CAN.
After the mapping exercise, JSI co-facilitated with the Healthy Start project directors a group reflection process for all CAN members, generating discussion around CAN member contributions (i.e., programs, services, activities, and policies) to the system of care. This enabled the CANs to understand where and how resources are (and are not) currently directed and allowed for the emergence of a whole system action plan targeting coordinated upstream CAN efforts to address MIM&M racial/ethnic disparities. Discussion generated a shared understanding of how multisector partnerships within each community shape and inform the development of the existing system of care, both perpetuating adversities as well as protective factors. This understanding provided the foundation for developing a new strategic plan to create a whole system approach to addressing MIM&M.
Strategic Planning
Each CAN member was asked to consider how their respective organizations mitigate and contribute to adversities and protective factors for mothers and for infants, at which level of prevention, and at which system level. CAN member organizations identified priority areas and corresponding strategies which JSI then analyzed for system and level of prevention distribution using the WSPF. An iterative process followed (Figure 2), encouraging CAN members to pivot from micro-level interventions to meso- and macrosystem level strategies to develop a whole system approach that also included primordial and quaternary prevention strategies. Process utilized to apply the Whole System Prevention Framework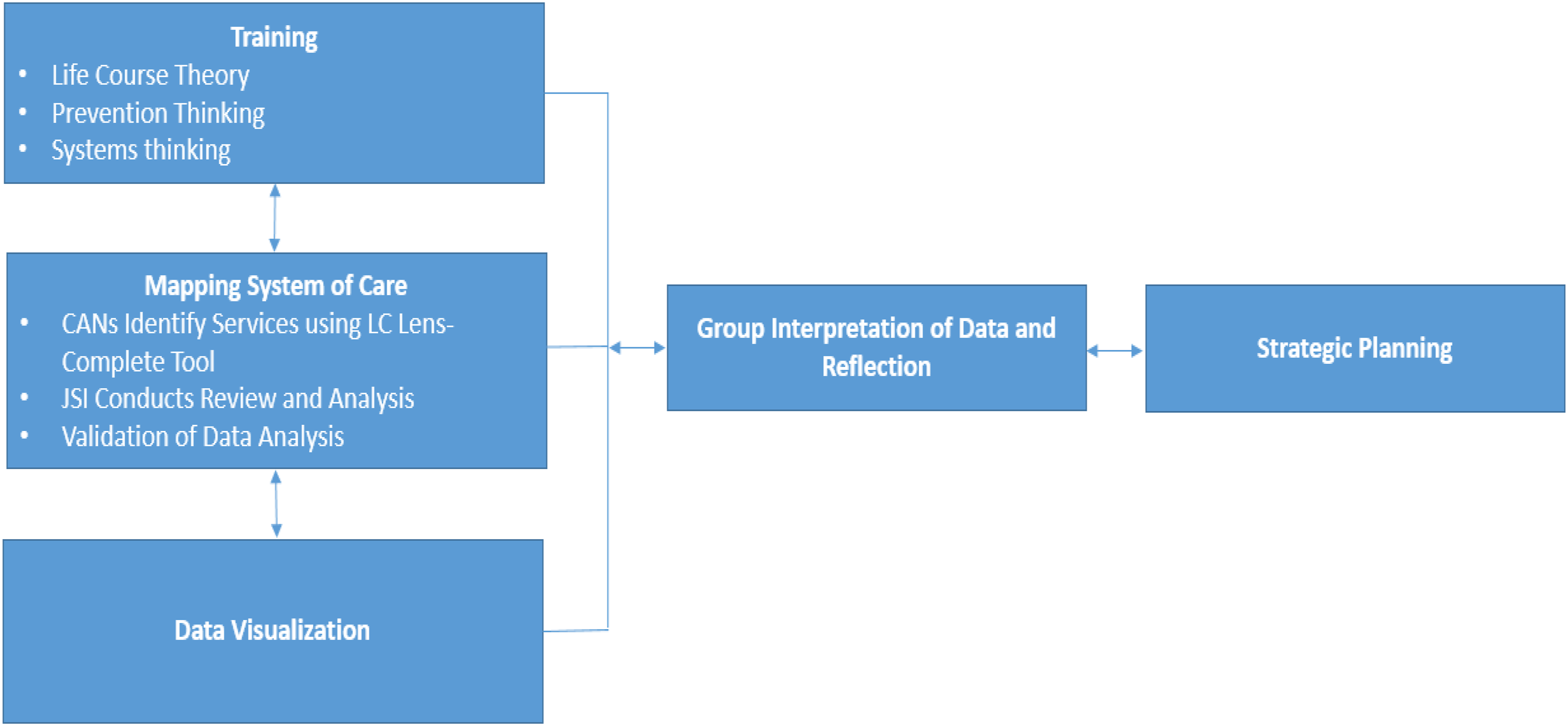
Findings
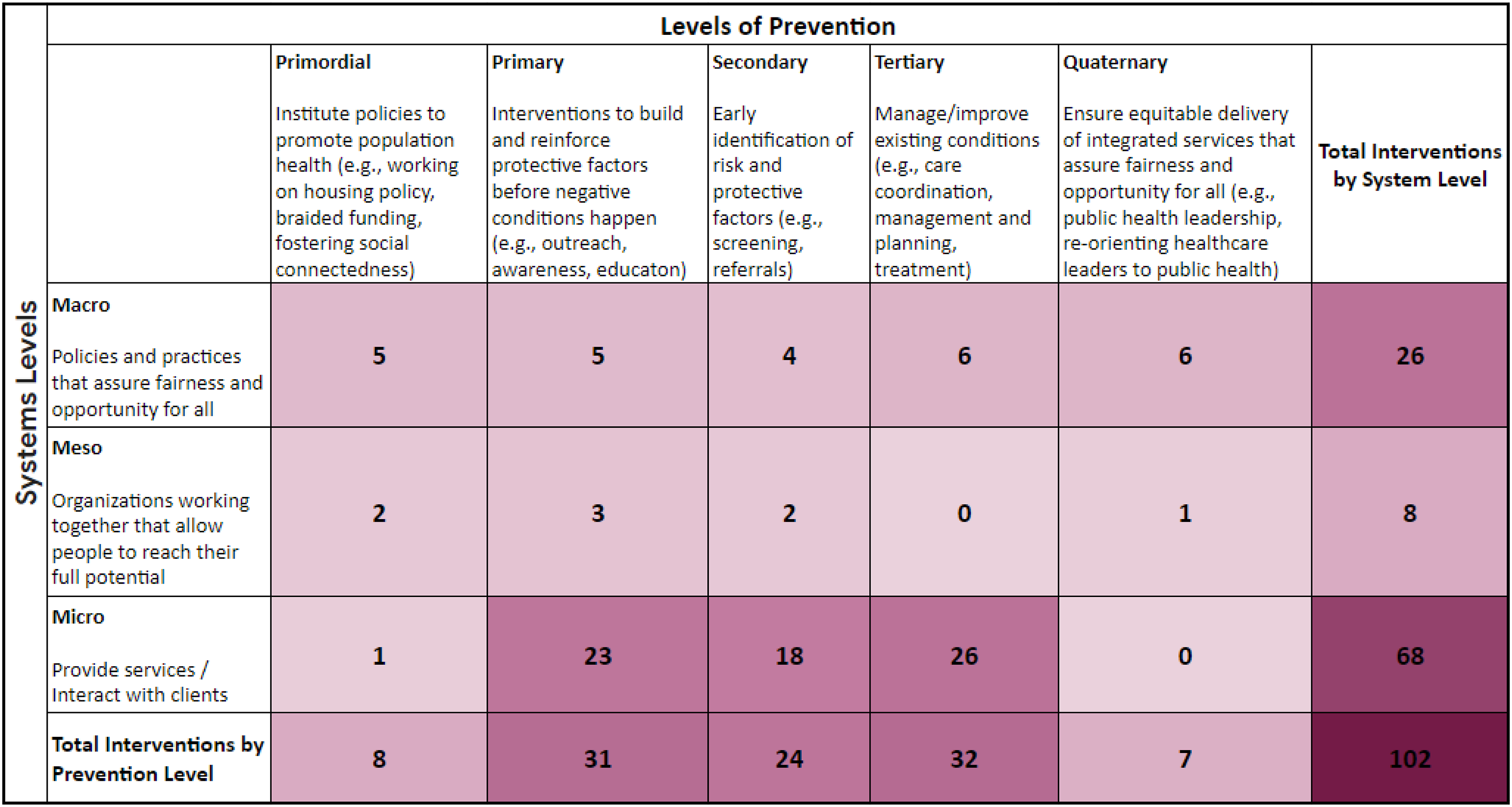
The results of the systems mapping exercises are detailed below for each Healthy Start program. Figures 3 and 4 illustrate the distribution of each CAN’s local efforts, with the shading reflecting concentration of services. That is, the most darkly shaded cells reflect cells with the greatest number of services identified within the community; cells with lighter shading indicate fewer services. Distribution of Services Provided (n = 98) by SNJPC Healthy Start CAN Member Organizations (n = 12) by System Level and Prevention Level [Shading intensity reflects concentration of services]. Distribution of Services Provided (n = 102) by TFDC Healthy Start CAN Member Organizations (n = 13) by System Level and Prevention Level [Shading intensity reflects concentration of services].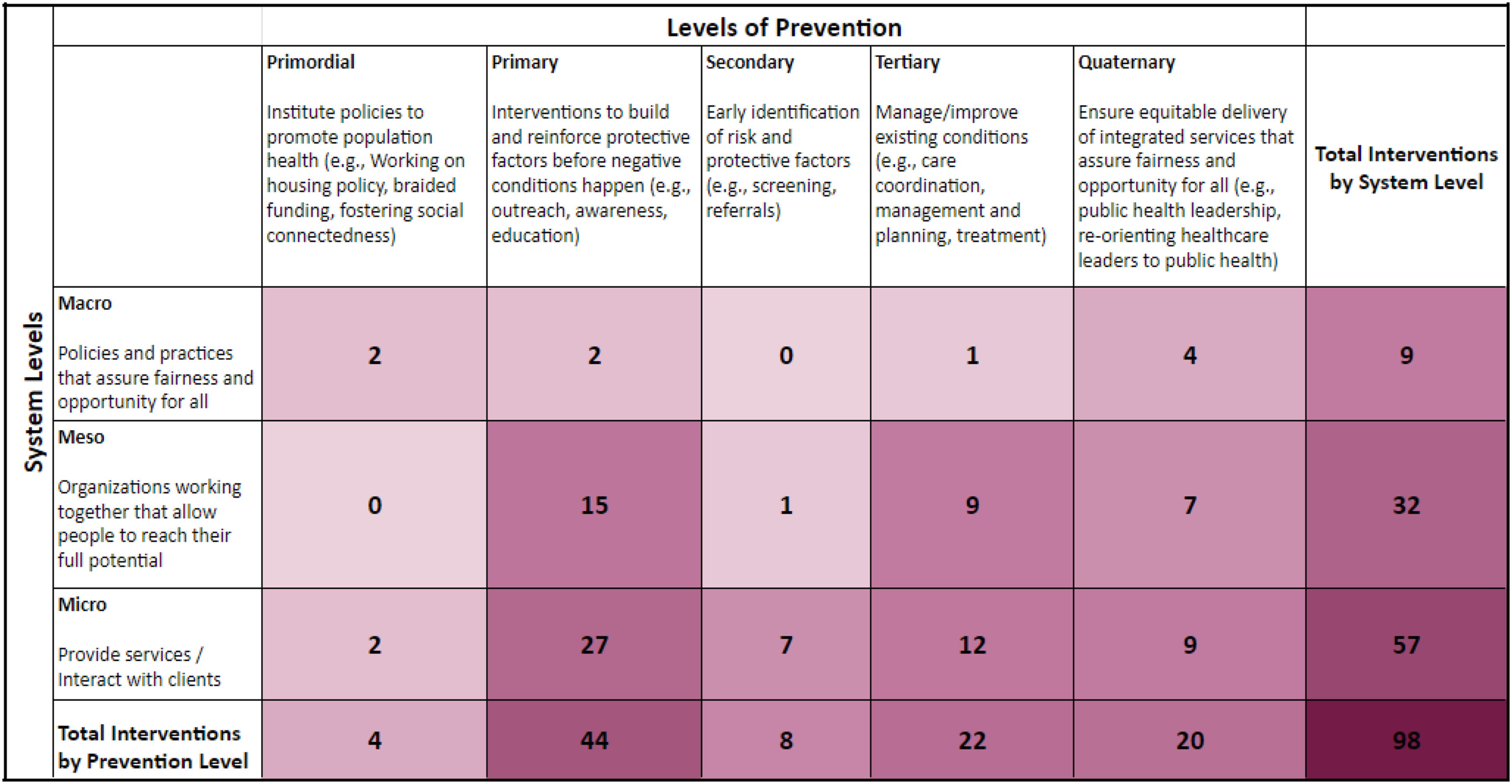
Southern New Jersey Perinatal Cooperative Healthy Start
Twelve SNJPC Healthy Start CAN members provided descriptions of 80 programs and services that their organizations deliver that they believed contributed to reducing MIM&M racial/ethnic disparities in their community. A total of 98 services were identified when services that fell into more than one system or prevention level were counted.
As shown in Figure 3, the greatest number of preventive services, and those with the darkest shading, were delivered at the microsystem level (e.g., not upstream, but downstream), and clustered at primary and tertiary prevention levels. The greatest percentage of services are primary prevention services (44.9%, n = 44), followed by tertiary prevention services (22.4%, n = 22). 20% of services (n = 20) fell into the quaternary level. Primordial and secondary prevention services each comprised less than 10% (4.1%, n = 4 and 8.2%, n = 8, respectively), as indicated by the lighter shade of cells in Figure 3. Greater than half (58.2%, n = 57) of prevention services are delivered at the individual/program (microsystem) level, which also reflect each prevention level. A third (32.7%, n = 32) of services are provided through community programs working together (mesosystem level). No primordial activities were reported at the mesosystem level. Fewer than 10% (9.2%, n = 9) of activities focused on upstream, policy/funding/regulation-type activities (macrosystem level). No secondary prevention level activities were reported at the macrosystem level.
The Foundation for Delaware County Healthy Start
Thirteen TFDC Healthy Start CAN members provided descriptions of 70 programs and services that their organization delivers that they believed contributed to reducing MIM&M racial/ethnic disparities in their community. A total of 102 services were identified when services that fell into more than one system or prevention level were counted.
As shown in Figure 4, the greatest number of services and those with the darkest shading, were delivered at the microsystem level [e.g., not upstream, but downstream], and clustered at primary, secondary and tertiary prevention levels. Primary and tertiary services comprise the greatest percentage of preventive services (22.5%, n = 23 and 25.5%, n = 26), followed by secondary prevention activities (17.6%, n = 18).
Primordial and quaternary prevention activities each comprised less than 10% (7.9%, n = 8 and 6.9%, n = 7, respectively), as indicated by the lighter shade of cells in Figure 4. The majority (66.7%, n = 68) of activities are provided at the individual/program (microsystem) level. Less than 1% (n = 1) of these are primordial; no quaternary activities were noted at the microsystem level. Services provided through community programs working together (meso level) reflected the lowest number (7.9%, n = 8). Most of these were primary prevention activities (2.9%, n = 3). No tertiary activities were reported. A quarter of services (25.5%) represent upstream activities (e.g., policy, funding, regulation) occurring at the macro level, fairly evenly distributed across prevention levels.
Through their strategic planning processes, the SNJPC CAN identified affordable, adequate, and safe housing as the priority determinant; they then drafted strategies to address altering policies and practices that pose barriers/limit access. TFDC identified community-centered access to resources and economic supports as the priority determinant; they then drafted strategies to focus on quality improvement, standardizing data collection, and engaging policy makers in the CAN.
Discussion
Overall, the mapping process provided a visual distribution of the existing prevention intervention landscape of the two Healthy Start communities related to maternal and child health. For each, the mapping revealed that most services are provided at the downstream micro level, and the majority of these are primary prevention (e.g., increasing awareness, education, outreach, parent engagement, and prenatal care) and tertiary prevention (e.g., case management and treatment). Fewer prevention services target primordial or quaternary prevention. There were virtually no (less than 10%) pre-existing upstream MCH/MIM&M activities.
Although there is an emphasis by the HRSA funders for Healthy Start programs and initiatives to address SSDoH, focusing efforts upstream, the mapping suggests possible system inertia as public health efforts continue to focus on downstream interventions. In addition to identifying opportunities for greater primordial (upstream) and quaternary prevention, the mapping indicated significant opportunities to address these issues at the macro level, and for cultivating horizontal connections at the community (meso) level. The authors believe that the most important outcome of the Healthy Start CAN strategic planning process is the enhanced understanding of what is needed to create a whole system prevention framework, with now a higher proportion of upstream approaches, to address the wicked problem of racial/ethnic MIM&M disparities.
The WSPF facilitated a process that enabled communities to understand how resources need to be redistributed to include primordial and quaternary at the macro- and mesosystem levels. The two exemplar Healthy Start CANs are in the process of refining and prioritizing which strategies to implement first. JSI continues to support them in refining their strategies, including revisiting the composition of their CANs and enhancing them through the provision of training and technical assistance.
The value of multi-sector partnerships (such as the CAN) lies in their potential to bring diversity of perspectives, strategies and interventions reflecting components of a whole system.9,14,15 While primary, secondary and tertiary prevention efforts are critical to addressing immediate needs of individuals in the short-term, addressing “Wicked Problems” requires robust prevention efforts across all prevention levels, including primordial and quaternary. At the same time, it requires addressing wicked problems at each system level simultaneously. Mapping existing interventions by level of prevention at each system level provides a way to visualize the current state of the system of care. It provides a snapshot of the distribution of prevention activities across the system of care, potentially revealing gaps and therefore needed sector partners for developing and implementing a whole system strategic plan to address, in particular, MIM&M. The WSPF guided this process.
MIM&M is a “wicked” problem. Its etiology is socially or culturally entrenched and perpetuated through built-in system structures and processes, 1 thus reinforcing adversities that manifest as racial/ethnic disparities. Systems have a history. Current behavior is influenced by the past, i.e., previous activities or actions, 35 current status or conditions result from previous activities or actions [path dependency]. 36 In the absence of whole system interventions that take into account primordial and quaternary prevention, society will continue to reinforce its dysfunctional systems that serve the already harmed women and infants, resulting in continued adverse health outcomes (disparities).
The WSPF provides an enhanced approach to address MIM&M and other wicked problems. It integrates and activates LCT with expanded levels of prevention, required to balance addressing the immediate needs of individuals, families, and communities through primary, secondary, and tertiary prevention activities, while simultaneously transforming the context (primordial) for the next generation and beyond. 56 LCT helps to understand disparities and why health equity is challenging to achieve.
While inherent complexities challenge development of empirical evidence supporting LCT, the current approach offers a path to action that is based upon the growing body of science, without waiting for the science to catch up. The expanded levels of prevention are critical for progress: primordial prevention addresses life course and SSDOH, and quaternary allows for a targeted addressing of the perpetuation of inequities by the existing system of health care and social support. Primordial factors, the long game issues that explain generational effects, provide the underpinning for LCT - establishing the context of societal protective and risk factors that set the stage for individual life trajectories.
Quaternary prevention applies an equity lens, viewing the role of the system of care itself in introducing and reinforcing protective factors and mitigating adversities. Quaternary prevention touches each other prevention level. An equitable whole system approach would include quaternary prevention at each system level, holding the system accountable for providing equitable services, utilizing quality improvement, and serving as the system’s conscience.
Systems thinking provides a framework for applying LCT. Systems thinking that facilitates system change/improvement starts through a process of collective analysis and synthesis. First, “breaking the whole into its parts” yields knowledge of the system: where and how stakeholders contribute to life course adversities, and where it might be promoting protective factors. Synthesizing this knowledge provides an understanding of the “whole”, revealing gaps, untapped potential, and alternatives. 57 The WSPF ensures that all stakeholders see themselves as a part of the system - the engine - that has the potential to drive the change necessary to address wicked problems because of their subject matter and context expertise. The result is a whole system approach to developing an upstream plan for rewiring systems with deeply rooted issues, drivers of racial/ethnic disparities in MIM&M. The work sets the stage for system alignment, or rather, re-alignment.
CAN members found it difficult to make the shift in thinking. They found this shift to systems thinking “hard” and were surprised that their programs were heavily weighted toward primary and microsystem level prevention. However, the visual representation through the mapping process helped them to conceptualize their systems of service and care, and their respective organizations’ contributions and role within it. For both Healthy Start CANs, these striking comparisons generated rich discussion among CAN members during their group’s post-numeric mapping summary reflection activity. Incorporating the systems’ dimension allowed them to step back to see the system in its entirety, including the deprivation of protective factors and the perpetuation of adversities by the system that inhibit one’s ability to reach their full potential.
Across both Healthy Start communities, prevention interventions (i.e., activities, services and programs) distribution is weighted at the micro level and the preponderance are primary and tertiary prevention. These distributions indicate gaps in primordial prevention activities that target upstream health determinants, and quaternary prevention activities, thus suggesting opportunities for systemic interventions. Such interventions create the optimal conditions for positive community health outcomes and ensure equitable access to services across the whole system of care. Visualizing the whole system – with its strengths and gaps – illuminated the whole system approach, and the WSPF specifically, as a way to address wicked problems. It gave both communities ideas for addressing the wicked problem at meso- and macrosystem levels and reinforced the value of systems thinking as a way to activate LCT.
The WSPF provides a mechanism for addressing upstream drivers of the wicked problem of MIM&M racial/ethnic disparities. The process is doable, and its community-level analysis can help programs such as Healthy Start shape, direct and better utilize resources and community assets to strategically address MIM&M, especially its upstream roots, as well as other wicked problems. Regardless of the determinant, the process of mapping the current system of care using the WSPF was transformative and could be for other wicked problems.
These local analyses can inform a local or state policy and program agenda for social and political action. It allows for immediate enhancements at the micro level, a partial blueprint for mesosystem level initiatives, and an agenda for macro level efforts. However, political will creates political agendas and through regulation and funding, sets the parameters for other system dimensions and opportunities to either perpetuate disparities or mitigate them. Recent restrictions to access to sexual and reproductive health services58,59 underscore the urgency of primordial and quaternary prevention.
Macrosystem level policy and corresponding funding streams could prioritize braided or blended funding to support primordial initiatives. Primordial initiatives are essential to creating the optimal conditions for individuals to reach their full potential by promoting protective factors and doggedly mitigating adversities that drive disparities. Funding streams supporting primordial prevention would in turn catalyze interactions between multi-sector partners and focus of their efforts, effectively steering public health programs and practice upstream, towards equity. Consequently, performance measurement would no longer be limited to the number of individuals served (or services provided) but more so on how the system is performing - or behaving - as evidenced by, for example, diminishment of racial/ethnic disparities that manifest as wicked problems.
Public health plays an essential role as convener and coordinator of a whole system approach to establish a new and equitable context for all. In order to capture the full array of services and supports, multi-sector partnerships, like the CAN, need to diversify representation, strategies, and interventions in the context of systems levels and expanded levels of prevention. Furthermore, funders need to revisit their funding priorities and interventions and assess for distribution across system and prevention levels to effectively address wicked problems, like racial/ethnic disparities in MIM&M, that burden generation. 9
Limitations and Further Development Needs
There are some limitations to our work. Most CAN member organizations provide direct services; and the CAN may not include all community organizations or programs that provide prevention interventions that address the broad set of factors that contribute to MIM&M. 4 v However, taking into account that the focus of a Healthy Start CAN is to improve the health and health care systems of infants, mothers and families, the authors believe this multi-sector partnership provides a valid and valuable perspective and representation of the foundational system of care within these communities. The value of the visual produced by the mapping process helps multi-sector partners consider other community partners to engage in the work of addressing SSDoH at system levels and levels of prevention.
As a newly developed framework and applied methodology, the WSPF could still and likely will be further operationally developed with its usage in practice. The authors acknowledge LCT is not explicitly named/identified in the Distribution of Services provided by System Level and Prevention Level matrices (Figures 3 and 4) because all the services pertain to life course for this population. For the WSPF, life course is not limited to discrete ages and stages, but is recognized as a dynamic, emergent development across the full life course and into future generations. Future applications of the WSPF will likely encourage prevention thinking and systems thinking to additionally consider and incorporate the implications of life course within their respective spheres, by potentially better articulated life course time specifications. However, implementation of programmatic interventions can generally only address a specific time period. Application of prevention thinking will likely help to develop greater detailed primordial conceptual markers with maturity over time, thereby adding the needed specificity for the WSPF to evolve. The WSPF utilizes a traditional micro, meso, macro system conception; however, a growing sophistication in systems thinking may subsequently get incorporated into a yet further enhanced WSPF.
This paper also debuted the first effort to utilize the WSPF as an applied methodology to guide new upstream strategic planning. While this process successfully engaged HS CAN members and served as an excellent T/TA approach, the tools and methods used were initial practical T/TA efforts. There is no doubt with time these tools and methods for upstream strategic planning will evolve. This initial effort with two Healthy Start CANs established a Proof of Concept for our “implementation” methodology. Whether this methodology works for other groups/participants beyond Healthy Start CANs, who are generally already very life course and upstream savvy, needs to be established – and the tools and methods – especially in the initial training – will need to be adapted to other groups – and also explored for other wicked problems. But this project did make substantial progress for Healthy Start and the larger maternal and child health (MCH) community in thinking practically and addressing programmatically the upstream/SSDoH roots of the wicked problem of MIM&M racial disparities.
Conclusion
This paper presents both a new framework and a new methodology for practical application of the Whole System Prevention Framework, and describes the implementation of this methodology within two Healthy Start communities. The WSPF is an enhanced way to begin to conceptualize and address wicked problems, like MIM&M. It offers a “community up” approach starting with context (primordial prevention) and guided by the system’s conscience (quaternary prevention), while interfacing with all other traditional system levels. Fine and Kotelchuck identified the need to reframe and reorganize systems and services to emphasize prevention and called for increased integration across systems of care and across the lifespan.24,26 This mapping methodology can further enhance and strengthen the upstream efforts of Healthy Start (and other place-based and systems initiatives) through intentional efforts; and it makes for fertile ground to respond to Fine and Kotelchuck’s call to activate LCT in public health practice. The Whole System Prevention Framework is a call to action for funders, policymakers, and the MCH community to not lose sight of the long game - the next generation - where the change/improvement will be evident in the wicked problems, like MIM&M, and their racial/ethnic disparities that haunt us today.
Footnotes
Acknowledgements
Many thanks to Rachael Meyer, JSI Graphic Designer, and the Community Action Networks of Southern New Jersey Perinatal Collaborative. Milton Kotelchuck, a member of the Maternal and Child Health - Measurement Research Network, was supported for this research by the Health Resources Services Administration (HRSA) award No. U3DMC32755-01-00.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Health Resources and Services Administration, Maternal and Child Health Bureau’s, Division of Healthy Start and Perinatal Services (HRSA\MCHB\DHSPS) (3 H49MC30725‐06‐01) and Health Resources and Services Administration, Maternal and Child Health Bureau’s, Division of Healthy Start and Perinatal Services (HRSA\MCHB\DHSPS) (H4900142).